Embed Size (px)
Citation preview

Carcinogenicity of acetaldehyde in alcoholic beverages:risk assessment outside ethanol metabolism
Dirk W. Lachenmeier1, Fotis Kanteres2 & Jürgen Rehm2–4
Chemisches und Veterinäruntersuchungsamt (CVUA) Karlsruhe, Karlsruhe, Germany,1 Centre for Addiction and Mental Health (CAMH),Toronto, Canada,2 DallaLana School of Public Health, University of Toronto,Toronto, Canada3 and Institute for Clinical Psychology and Psychotherapy,TU Dresden, Dresden, Germany4
ABSTRACT
Aims In addition to being produced in ethanol metabolism, acetaldehyde occurs naturally in alcoholic beverages.Limited epidemiological evidence points to acetaldehyde as an independent risk factor for cancer during alcoholconsumption, in addition to the effects of ethanol. This study aims to estimate human exposure to acetaldehyde fromalcoholic beverages and provide a quantitative risk assessment. Methods The human dietary intake of acetaldehydevia alcoholic beverages was estimated based on World Health Organization (WHO) consumption data and literature onthe acetaldehyde contents of different beverage groups (beer, wine, spirits and unrecorded alcohol). The risk assessmentwas conducted using the European Food Safety Authority’s margin of exposure (MOE) approach with benchmark dosesobtained from dose–response modelling of animal experiments. Life-time cancer risk was calculated using the T25 dosedescriptor. Results The average exposure to acetaldehyde from alcoholic beverages was estimated at 0.112 mg/kgbody weight/day. The MOE was calculated to be 498, and the life-time cancer risk at 7.6 in 10 000. Higher risk mayexist for people exposed to high acetaldehyde contaminations, as we have found in certain unrecorded alcohol bever-ages in Guatemala and Russia, for which we have demonstrated possible exposure scenarios, with risks in the range of1 in 1000. Conclusions The life-time cancer risks for acetaldehyde from alcoholic beverages greatly exceed the usuallimits for cancer risks from the environment set between 1 : 10 000 and 1 : 1 000 000. Alcohol consumption has thusbeen identified as a direct source of acetaldehyde exposure, which in conjunction with other sources (food flavourings,tobacco) results in a magnitude of risk requiring intervention. An initial public health measure could be to reduce theacetaldehyde content in alcoholic beverages as low as technologically possible, and to restrict its use as a food flavouradditive.
Keywords Acetaldehyde, alcohol, alcoholic beverages, cancer, ethanol, unrecorded alcohol.
Correspondence to: Dirk W. Lachenmeier, Chemisches und Veterinäruntersuchungsamt (CVUA) Karlsruhe, Weissenburger Strasse 3, D-76187 Karlsruhe,Germany. E-mail: [email protected] 30 September 2008; initial review completed 26 November 2008; final version accepted 15 December 2008
INTRODUCTION
Acetaldehyde (ethanal, CH3CHO, CAS # 75-07-0) is ametabolite of ethanol which occurs in the human bodyafter the consumption of alcoholic beverages; addition-ally, it is widely present in foods, beverages and industry,as well as in the environment [1]. It is also a known geno-toxic and carcinogenic substance, with recent evidenceindicating that exposure to acetaldehyde directly con-tained in alcoholic beverages may have detrimentaleffects above those of ethanol and metabolically formedacetaldehyde [2–4]. In our ongoing investigation aboutthe composition and global public health impact of
alcoholic beverages, including unrecorded alcohol [5–7],we have detected high acetaldehyde concentrations in anumber of products, including sugarcane spirits (cuxa)from Guatemala [8], agave spirits from Mexico [9], andcertain spirits from China [3], as well as fortified winesand fruit and marc spirits from Europe [3]. Otherresearchers have also detected similarly high levels in theFrench cider spirit calvados [2] and the Brazilian sugar-cane spirit cachaça [10,11]. The occurrence of acetalde-hyde, including contamination, in alcohol products maytherefore be a prevalent problem on a world-wide scale.
In contrast to other constituents of alcoholic bever-ages (e.g. methanol, higher alcohols or ethyl carbamate),
REVIEW doi:10.1111/j.1360-0443.2009.02516.x
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550

for which excellent risk assessments are available in theliterature [12–14], as well as regulatory limits havingbeen provided in many jurisdictions, we found a majorknowledge gap regarding information about the potentialpublic health impact of acetaldehyde, resulting in aninability to adequately ascertain the risk for the consum-ers of the alcoholic beverages researched. In this study,using the harmonized approach of the European FoodSafety Authority (EFSA) [15], we present for the first timea quantitative risk assessment for acetaldehyde in alco-holic beverages.
MATERIALS AND METHODS
Literature research
Data on the toxicity of acetaldehyde were obtained by acomputer-assisted literature search using the key words‘acetaldehyde’, ‘alcohol’, ‘consumption’ and ‘cancer’.Data on the exposure were searched using the key words‘acetaldehyde’, ‘exposure’ and ‘environment’. Searchesin both English and German were carried out in July2008, using the following databases: PubMed, Toxnetand ChemIDplus (US National Library of Medicine,Bethesda, MD, USA), Web of Science (Thomson Scientific,Philadelphia, PA, USA), IPCS/INCHEM [InternationalProgramme on Chemical Safety/Chemical Safety Infor-mation from Intergovernmental Organizations, WorldHealth Organization (WHO), Geneva, Switzerland], FoodScience and Technology Abstracts (International FoodInformation Service, Shinfield, UK) and Scopus (ElsevierBV, Amsterdam, the Netherlands). This was accompaniedby a hand search of the reference lists of all papers for anyrelevant studies not included in the databases. We specifi-cally aimed to identify long-term animal studies thatwould be usable for dose–response modelling, as well ashuman exposure data from large surveys. The references,including abstracts, were imported into ReferenceManager V.11 (Thomson ISI Research Soft, Carlsbad, CA,USA) and the relevant articles were identified manuallyand purchased in full text.
Approach for risk analysis and dose–response modelling
Analysis was conducted according to the harmonizedapproach of the EFSA for the risk assessment of sub-stances which are genotoxic and carcinogenic [15]. TheEFSA has developed and recommends an approachknown as the margin of exposure (MOE). This approachuses the doses of substances which have been observed tocause low but measurably harmful responses in animalsas reference point values and compares them with rel-evant substance specific dietary intake estimates inhumans, taking into account differences in consumptionpatterns. The benchmark dose (BMD), derived from the
animal data by mathematical modelling within theobserved range of experimental data, is recommended asa standardized reference point. To obtain the MOE, thebenchmark dose lower confidence limit (BMDL) of 10%was taken. The BMDL is an estimate of the lowest dosethat is 95% certain to cause no more than a 10% cancerincidence in rodents.
In cases where data is unsuitable for obtaining aBMDL the EFSA recommends using the T25 calculation,wherein the dose corresponding to a 25% incidence oftumours, after correction for spontaneous incidence, isrepresented. The basic difference between the determina-tion of the BMD and the T25 calculation is that the BMDis accomplished through dose–response modelling thatconsiders all available information on the dose–responsecurve, whereas the T25 is calculated from one data point[15]. For further details on the T25 calculation seeDybing et al. [16].
The BMD and BMDL values were calculated using theUS EPA’s BMDS version 2.0 software (available at the USEnvironmental Protection Agency website: http://www.epa.gov/ncea/bmds/index.html). The T25 valueswere calculated using the European Union (EU) methodas detailed by Van Landingham et al. [17]. MOEs werecalculated by dividing the reference point, i.e. the BMDL,by the estimated human intakes. We also used the T25method to calculate life-time cancer risk [18].
Dietary intake assessment
The EFSA harmonized approach was also used to conductthe dietary intake assessment [15]. Data on alcohol con-sumption for the groups beer, wine and spirits wasobtained from the Global Information System on Alcoholand Health [19] based on data from the Food and Agri-culture Organization as well as other sources [20,21] forthe year 2002 as averages for the years 2001–03 and forthe population older than 15 years. The data on unre-corded consumption were based on estimated volume forthe population older than 15 for the years after 1995[22].
The distribution of consumption in the spirits cat-egory was calculated based on data from the EuropeanSpirits Organization (CEPS) from 2005 [23]. The whiskeycategory includes Scotch, US, Canadian, Irish and otherwhisk(e)y. White spirits include gin, vodka, tequila andother white spirits. Flavoured spirits include liqueurs,bitters, aniseed-flavoured spirits and fruit spirits (eau-de-vie). Data on cuxa consumption in Guatemala are fromKanteres et al. [8].
The acetaldehyde content of alcoholic beverages wastaken mainly from our own data [3]. Special exposurescenarios were developed with acetaldehyde data in cuxa[8] and in homemade samogon from Russia [24].
534 Dirk W. Lachenmeier et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550

RESULTS
Hazard identification and characterization
Epidemiology
Epidemiological research has provided a great deal of evi-dence regarding alcohol as a major risk factor for a rangeof diseases, including certain cancers [25–32]. This,however, has not been the case with regard to mechanismsof this effect, which have not received the same level ofinvestigation. Acetaldehyde, which occurs not onlyduring ethanol metabolism, but also in smoking, food pro-duction and industry, has had its health effects investi-gated as early as the 1950s [33] and its relationship withcancer in the 1970s [34]. In 1965, acetaldehyde wasasserted a ‘generally recognized as safe’ (GRAS) status bythe Flavor and Extract Manufacturers Association (FEMA)[35]. This status was reconfirmed by the Joint FAO/WHOExpert Committee on Food Additives (JECFA) in 1998 [36].However, mounting evidence has contradicted this stanceas studies have found that acetaldehyde is mutagenic,genotoxic and plays a significant role in the developmentof certain types of cancer [1]. Only recently have therebeen studies involving human subjects and acetaldehyde;these have focused generally on genetic susceptibility[37–40], with relatively far fewer looking at the healtheffects on a population level [2].This is discussed in greaterdetail below. Most of these analyses concentrated onacetaldehyde within the ethanol metabolism. Notableexceptions include epidemiological research concerningthe French distilled cider spirit calvados. Studies research-ing the accumulation of squamous-cell cancer in Nor-mandy and Brittany (France) were able to prove asignificantly increased risk for cancer of the oesophaguscaused by chronic calvados consumption [41,42]. Con-sumption of hot calvados appeared to explain abouttwo-thirds of the inter-regional and urban and rural dif-ferences in incidence, compared with total alcohol con-sumption which explained less than one-fifth [41]. Thehigh concentration of acetaldehyde combined with thepossible effects of the high temperature at which calvadosis consumed could account for the increased risk ofcalvados-related oesophageal cancer [2]. Similarly, thehigher risk for oral cancer associated with shochu con-sumption in Japan [43] may also be explained by its rela-tively higher acetaldehyde concentration [4].
Animal studies
Results from animal studies on alcohol and cancerdepend on experimental design, carcinogen evaluated,time-frame of exposure and measurement and dosage,among other factors. Of the few studies on acetaldehydethat exist there have been significant results. Alcohol hasbeen shown to increase the occurrence of tumours when
applied locally to the oral or oesophageal mucosa;ethanol, with some exceptions, has been noted to have astimulating effect on chemically induced carcinogenesis[29,44]. Furthermore, animal studies using alcohol andprocarcinogens have reported stimulating hepatocar-cinogenesis [45]. Acetaldehyde, when inhaled, has beenobserved to cause nasopharyngeal and laryngeal carci-noma [46,47]. Although these studies are very limited interms of the number of animals and time-frame, they stillprovide evidence of the potential hazard of acetaldehyde-influenced carcinogenicity for humans.
As the focus on the specific effects of orally adminis-tered acetaldehyde is relatively new, there are few studies.The most notable and relevant include: Soffriti et al. [48],a long-term case–control study of rat groups exposed toacetaldehyde that resulted in a carcinogenic effect;Matysiak-Budnik [49], where exposure to an acetalde-hyde solution during a short period (11 weeks) resulted inliver inflammation; and Til et al. [50], an earlier workwhich observed hyperkeratosis of the forestomach in ratsgiven top doses of acetaldehyde. These studies are dis-cussed in more detail in the section ‘Dose–response analy-sis’. Another oral study of note is that of Homann et al.[51], in which Wistar rats were given acetaldehydeduring an 8-month period at a single concentration level(324 mg/kg body weight/day). Due to the single doselevel, this study was not included in our dose–response-modelling. However, it is important to mention thatalthough no tumours were observed, cell proliferation intongue, epiglottis and forestomach was significantlygreater in the acetaldehyde-treated animals than inthe control group. In addition, the epithelia fromacetaldehyde-treated rats were significantly thicker in allthree sites. The findings suggest that hyperplastic andhyperproliferative changes in epithelia of the upper gas-trointestinal tract may be early stages of carcinogenesis.Long-term or life-time studies are necessary for detectingtumours [48]. Indirect evidence on the carcinogenicity ofacetaldehyde in animal experiments is also provided byoral long-term studies on vinyl acetate and ethanol, bothof which form acetaldehyde as a metabolite [52–55].
The hazard of acetaldehyde has been confirmed bya number of evaluations by the International Agencyfor Research on Cancer (IARC) which, as early as 1985,found sufficient evidence for the carcinogenicity ofacetaldehyde with experimental animals [56]. In 1987,the IARC assigned acetaldehyde into group 2B as being‘possibly carcinogenic to humans’ [57]. The classificationof group 2B was confirmed in 1999 [58]. In a recentIARC meeting [32,59], acetaldehyde was discussed inthe context of the carcinogenicity of alcoholic beverages(see section ‘Genetic epidemiology’). No separate re-evaluation of acetaldehyde was conducted; however,the accumulating evidence about the genotoxicity and
Risk assessment of acetaldehyde 535
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550

carcinogenicity of acetaldehyde was again pointed out inthe resulting IARC monograph.
Genotoxicity and mechanistic data
Acetaldehyde has been shown to have mutagenic andcarcinogenic effects in several in-vitro and in-vivo experi-ments, including prokaryotic and eukaryotic cell culturesand animal models [45]. It has been found to cause pointmutations, including in human lymphocytes, as well asform DNA adducts (i.e. covalent bonds with DNA, leadingto carcinogenesis) [60–66], and induce sister chromatidexchanges and gross chromosomal aberrations [67,68].In addition, it has also been found to interfere withDNA repair mechanisms, inhibiting the enzymeO6-methylguanine transferase, important for the repairof damage caused by alkalizing agents [69], and toinduce mutations in the TP53 tumour suppressor gene,which is a common genetic alteration involved in humancancer, especially oesophageal [70]. Furthermore, themutagenic properties of acetaldehyde have also beenlinked to the promotion of breast cancer [71,72]. Recentexperimental evidence has shown that the mutagenicadducts formed from acetaldehyde can occur in cellularconcentrations of 100 mM and above [60]. The lowestconcentration of acetaldehyde that has induced sisterchromatid exchange in Chinese hamster ovary cells invitro was 3.9 mg/l (88 mM) [73].
Indirect evidence from in vivo findings obtained inhuman studies points to a similar concentration range.During alcohol consumption, an important mechanismis the local formation of acetaldehyde in the digestivesystem by microbes representing normal oral or gut flora[74–76]. Ethanol oxidation also occurs, to a limitedextent, in nearby tissues [77]. As ethanol is distributedevenly to the whole aqueous phase of the human body, itis metabolized continuously to acetaldehyde as long as itremains in the blood and saliva. This leads to accumula-tion of acetaldehyde in the saliva and intestinal contentsduring and after the consumption of alcohol [74,78].Thus, an important factor is the limited capacity of oralmicrobes and mucous membranes to detoxify acetalde-hyde [78]. Via swallowing, salivary acetaldehyde is trans-ported from the mouth to the mucous membranes of thepharynx, oesophagus and stomach [78].
Depending upon the quality of oral hygiene, alcoholconsumption has been found to result in salivary acetal-dehyde concentrations of 50–200 mM [79,80]. Aftersimilar doses of alcohol, salivary acetaldehyde levels ofaldehyde dehydrogenase 2 (ALDH2)-deficient subjectshave been found at levels two to three times higher thannormal [4,81]. Moreover, combination with smoking hasresulted in salivary acetaldehyde concentration of over250 mM [80]. Epidemiological studies have found that
increases in salivary acetaldehyde concentrations areassociated with linear or even multiplicatively increasedrisk for upper digestive tract cancer [32,59].
The combined evidence from in vitro experiments andhuman drinking and smoking studies points tomutagenic acetaldehyde concentrations in a range as lowas 50–150 mM. For our evaluation of acetaldehydeoutside ethanol metabolism it is interesting to note thatsome groups of alcoholic beverages may lead to short-term salivary acetaldehyde concentrations significantlyhigher than 150 mM [3]. This is exemplified by the firstexperimental evidence recently provided by Yokoyamaet al. [4], which demonstrated considerable differences insalivary acetaldehyde immediately after the consumptionof different alcoholic beverages. In the following period,between 30 and 180 minutes after drinking, the salivaryacetaldehyde concentrations were then unrelated to bev-erage type.
Genetic epidemiology
A number of genetic epidemiological studies provide evi-dence that the heterozygous genotype for the ALDH2gene, the enzyme primarily responsible for the oxidizationof acetaldehyde during alcohol metabolism, ALDH2*1/*2, contributes substantially to the development ofoesophageal cancer related to alcohol consumption[37,38,82]. This is due to that fact that carriers of thisgenotype process acetaldehyde at a much slower rate,which leads to higher levels of acetaldehyde in their blood[83] and saliva [81] after the consumption of alcohol.According to a recent study, these individuals also havehigher levels of acetaldehyde-related DNA adductsin their lymphocytes [84]. This has led to observationsthat include up to a 12-fold increase in risk for heavydrinkers in comparison to carriers of the homozygousALDH2*1/*1 genotype (which encodes the activeenzyme) [85]. Furthermore, even ingestion of moderatedoses of alcohol has been associated with a remarkablyincreased risk for digestive tract cancers, as salivaryacetaldehyde concentrations of ALDH2-carrier subjectshave been measured at two to three times higher thanthose with the normal ALDH2 enzyme [81,86]. Thisadditional acetaldehyde is due to the deficient ability ofsalivary gland and mucosal cells to remove acetaldehydeformed by their own alcohol dehydrogenase (ADH)[81,87]. The majority of studies into ALDH2*1/*2 havefocused primarily on Asian populations, which have beenfound to carry this allele in significant frequency.However, recent work by Zhang et al. [40] has identifiedanother allele of ALDH2, ALDH2 Ex1+82 G, investigatedin a Polish population, which they suggest may be func-tionally deficient in eliminating acetaldehyde. They alsostate that heavy drinkers who are genetically prone to
536 Dirk W. Lachenmeier et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550

accumulate acetaldehyde may face an increased risk ofstomach cancer. However, research into polymorphismsis not restricted to ALDH, as ADH1B*1/*1 (activity only1/40 of the normal), has also been reported to increaserelative risk for head and neck cancers [88]. In this case,the genotype results in a longer exposure time to themicrobially formed salivary acetaldehyde after alcoholconsumption [89]. Also the highly active ADH1C*1 allele(which metabolizes ethanol to acetaldehyde 2.5 timesfaster than the normal variant) has been associated withboth increased risk of head and neck cancers [90] andsignificantly elevated acetaldehyde concentration insaliva after alcohol consumption [91]. Furthermore, itshould be emphasized that the risk for cancer is multi-plied if both the ADH1B*1/*1 and ALHD2*1/*2 allelescoincide [92,93]. The IARC confirmed recently that thereis substantial mechanistic evidence that acetaldehydederived from the metabolism of ethanol in alcoholic bev-erages contributes to causing malignant oesophagealtumours in humans deficient in ALDH [32,59]. In ouropinion, an additional safety factor has to be used in therisk assessment of acetaldehyde taking these geneticpolymorphisms into consideration (see below).
Dose–response analysis
There is no adequate human study available for a dose–response analysis. From the animal experiments men-tioned above, three studies researching the oral route ofexposure to acetaldehyde appear to be suitable for dose–response modelling. In the study by Matysiak-Budniket al. [49], which focused on hepatotoxicity, acetaldehydewas administered to male rats at doses of 0, 120 and500 mg/kg body weight/day in drinking water for 11weeks and histopathological changes in the liver wereassessed morphometrically. The study indicated thatacetaldehyde delivered via the digestive tract could reachthe liver by the portal circulation and was able to produceliver injury (Table 1). Til et al. [50] studied the oral toxic-ity of acetaldehyde in rats in a 4-week drinking-waterstudy at dose levels of 25, 125 and 675 mg/kg bodyweight/day. Hyperkeratosis of the forestomach, observedin the top-dose rats, was the only adverse effect of acetal-dehyde detected (Table 2). In a more recent life-time study
of carcinogenicity by Soffritti et al. [48], male and femaleSprague–Dawley rats were given drinking water contain-ing acetaldehyde at concentrations of 0, 50, 250, 500,1500 or 2500 mg/l. Treatment with acetaldehyderesulted in an increase in total malignant tumours andshowed specific carcinogenic effects on various organsand tissues. A selection of results is presented in Table 3.
Due to the low number of animal subjects and theshort-term nature of their studies, Matysiak-Budnik et al.[49] and Til et al. [50] provide only limited applicable evi-dence for risk assessments, as the carcinogenic effectswere not evident during the study time. However, wemodelled the studies for comparison purposes, as hepato-toxicity is an especially intriguing area in the evaluationof acetaldehyde within the context of alcoholic bever-ages, and thus interactions with ethanol on hepatotoxic-ity cannot be excluded. It is also interesting to note thatneither hepatotoxicity nor hyperkeratosis of the fore-stomach were noted in the long-term study of Soffrittiet al. [48], possibly because both outcomes werethreshold-based, and the observed dose levels for hepato-toxicty and hyperkeratosis were more than double thoseused by Soffritti.
Soffritti et al. [48] is the only study designedadequately to be used for a risk assessment of carcinoge-nicity via the oral administration route. However, themodelling of the data is complicated, as the backgroundlevels were relatively high. In addition, the incidence ofcertain carcinomas was increased in the treated groups,but the statistical power was insufficient for allowingthe modelling of any specific cancer site (e.g. for the oral
Table 2 Histopathological changes in the stomach of rats givenacetaldehyde in drinking water for 4 weeks [50].
Acetaldehyde(mg/kg bodyweight/day)
Number ofanimals
End-point: focal hyperkeratosisof forestomach (incidence oflesions slight and moderate)
0 (control) M = 20, F = 20 M = 1 (5%), F = 025 M = 10, F = 10 M = 0, F = 0125 M = 10, F = 10 M = 0, F = 0675 M = 10, F = 10 M = 8 (80%), F = 8 (80%)
M: male; F: female.
Table 1 Hepatotoxicity study of male (M) rats exposed to acetaldehyde delivered in drinking water for 11 weeks [49].
Acetaldehyde (mg/kgbody weight/day)
Number ofanimals
End-point: hepatotoxicity(percentage of hepatocytes containingfat in the periportal area)
End-point: hepatotoxicity(percentage of hepatocytes containingfat in the pericentral area)
0 (control) M = 10 36 � 10 8 � 2120 M = 4 38 � 11 12 � 3500 M = 10 85 � 2 34 � 5
Risk assessment of acetaldehyde 537
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550
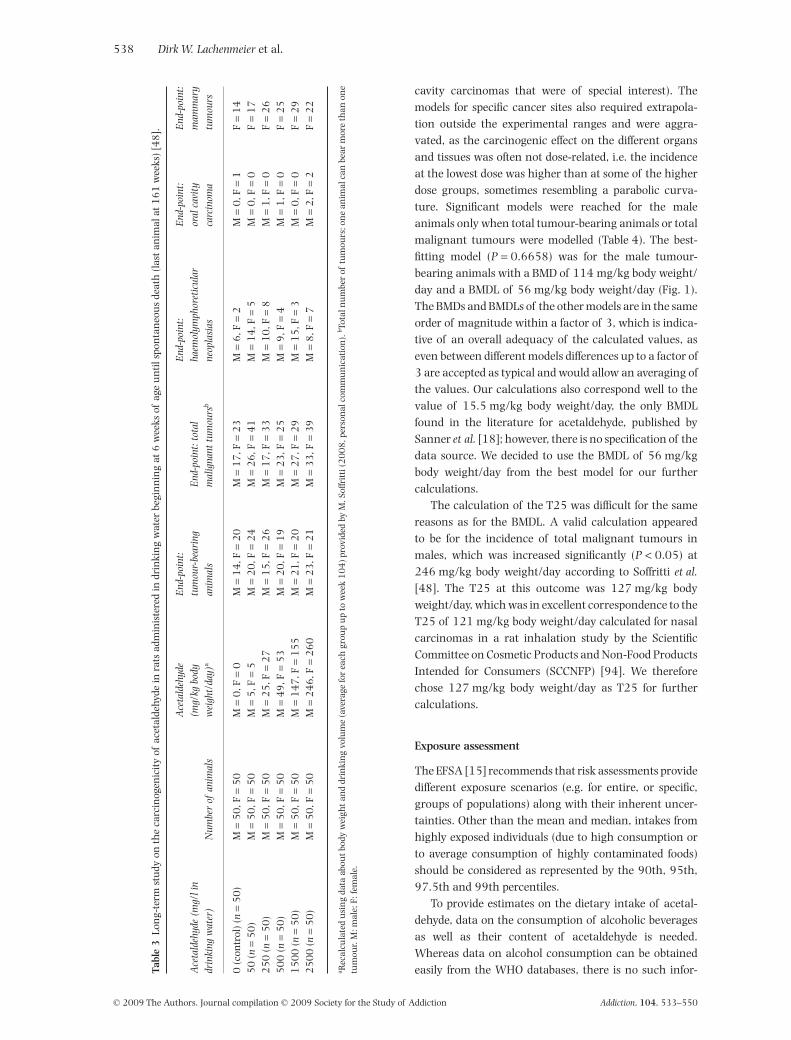
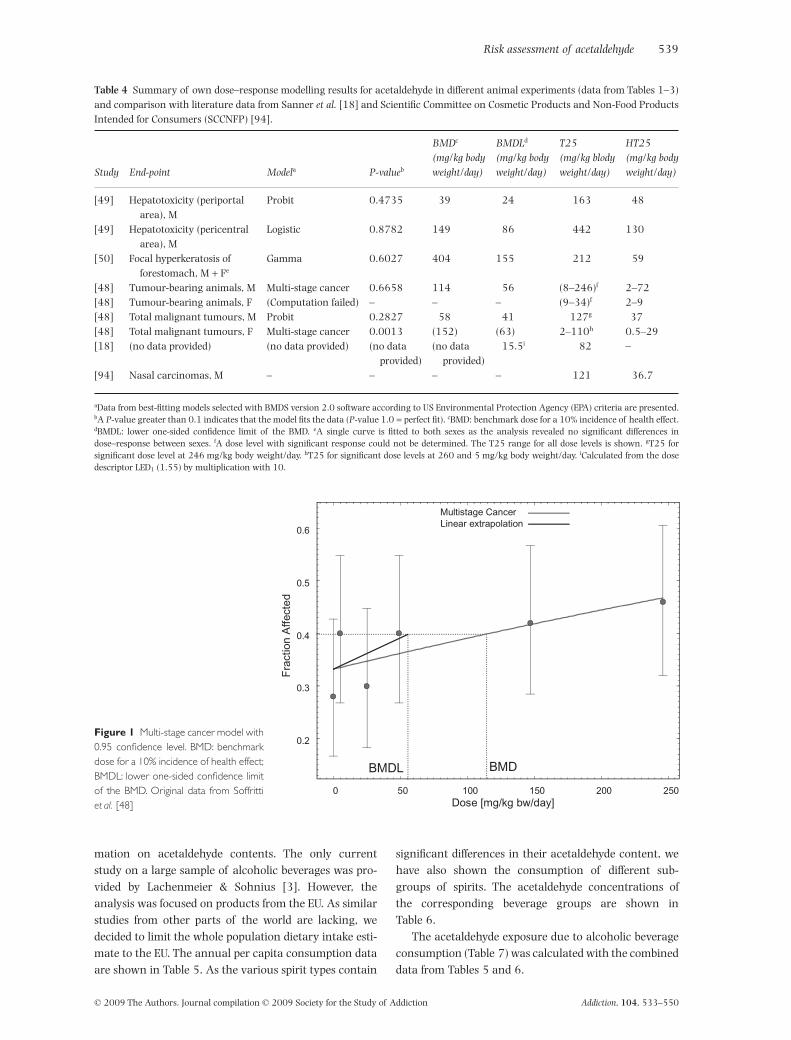
cavity carcinomas that were of special interest). Themodels for specific cancer sites also required extrapola-tion outside the experimental ranges and were aggra-vated, as the carcinogenic effect on the different organsand tissues was often not dose-related, i.e. the incidenceat the lowest dose was higher than at some of the higherdose groups, sometimes resembling a parabolic curva-ture. Significant models were reached for the maleanimals only when total tumour-bearing animals or totalmalignant tumours were modelled (Table 4). The best-fitting model (P = 0.6658) was for the male tumour-bearing animals with a BMD of 114 mg/kg body weight/day and a BMDL of 56 mg/kg body weight/day (Fig. 1).The BMDs and BMDLs of the other models are in the sameorder of magnitude within a factor of 3, which is indica-tive of an overall adequacy of the calculated values, aseven between different models differences up to a factor of3 are accepted as typical and would allow an averaging ofthe values. Our calculations also correspond well to thevalue of 15.5 mg/kg body weight/day, the only BMDLfound in the literature for acetaldehyde, published bySanner et al. [18]; however, there is no specification of thedata source. We decided to use the BMDL of 56 mg/kgbody weight/day from the best model for our furthercalculations.
The calculation of the T25 was difficult for the samereasons as for the BMDL. A valid calculation appearedto be for the incidence of total malignant tumours inmales, which was increased significantly (P < 0.05) at246 mg/kg body weight/day according to Soffritti et al.[48]. The T25 at this outcome was 127 mg/kg bodyweight/day, which was in excellent correspondence to theT25 of 121 mg/kg body weight/day calculated for nasalcarcinomas in a rat inhalation study by the ScientificCommittee on Cosmetic Products and Non-Food ProductsIntended for Consumers (SCCNFP) [94]. We thereforechose 127 mg/kg body weight/day as T25 for furthercalculations.
Exposure assessment
The EFSA [15] recommends that risk assessments providedifferent exposure scenarios (e.g. for entire, or specific,groups of populations) along with their inherent uncer-tainties. Other than the mean and median, intakes fromhighly exposed individuals (due to high consumption orto average consumption of highly contaminated foods)should be considered as represented by the 90th, 95th,97.5th and 99th percentiles.
To provide estimates on the dietary intake of acetal-dehyde, data on the consumption of alcoholic beveragesas well as their content of acetaldehyde is needed.Whereas data on alcohol consumption can be obtainedeasily from the WHO databases, there is no such infor-Ta
ble
3Lo
ng-
term
stu
dyon
the
carc
inog
enic
ity
ofac
etal
dehy
dein
rats
adm
inis
tere
din
drin
kin
gw
ater
begi
nn
ing
at6
wee
ksof
age
un
tils
pon
tan
eou
sde
ath
(las
tan
imal
at1
61
wee
ks)
[48
].
Ace
tald
ehyd
e(m
g/li
ndr
inki
ngw
ater
)N
umbe
rof
anim
als
Ace
tald
ehyd
e(m
g/kg
body
wei
ght/
day)
a
End
-poi
nt:
tum
our-
bear
ing
anim
als
End
-poi
nt:t
otal
mal
igna
nttu
mou
rsb
End
-poi
nt:
haem
olym
phor
etic
ular
neop
lasi
as
End
-poi
nt:
oral
cavi
tyca
rcin
oma
End
-poi
nt:
mam
mar
ytu
mou
rs
0(c
ontr
ol)
(n=
50
)M
=5
0,F
=5
0M
=0
,F=
0M
=1
4,F
=2
0M
=1
7,F
=2
3M
=6
,F=
2M
=0
,F=
1F
=1
45
0(n
=5
0)
M=
50
,F=
50
M=
5,F
=5
M=
20
,F=
24
M=
26
,F=
41
M=
14
,F=
5M
=0
,F=
0F
=1
72
50
(n=
50
)M
=5
0,F
=5
0M
=2
5,F
=2
7M
=1
5,F
=2
6M
=1
7,F
=3
3M
=1
0,F
=8
M=
1,F
=0
F=
26
50
0(n
=5
0)
M=
50
,F=
50
M=
49
,F=
53
M=
20
,F=
19
M=
23
,F=
25
M=
9,F
=4
M=
1,F
=0
F=
25
15
00
(n=
50
)M
=5
0,F
=5
0M
=1
47
,F=
15
5M
=2
1,F
=2
0M
=2
7,F
=2
9M
=1
5,F
=3
M=
0,F
=0
F=
29
25
00
(n=
50
)M
=5
0,F
=5
0M
=2
46
,F=
26
0M
=2
3,F
=2
1M
=3
3,F
=3
9M
=8
,F=
7M
=2
,F=
2F
=2
2
a Rec
alcu
late
du
sin
gda
taab
outb
ody
wei
ghta
nd
drin
kin
gvo
lum
e(a
vera
gefo
rea
chgr
oup
up
tow
eek
10
4)p
rovi
ded
byM
.Sof
frit
ti(2
00
8,p
erso
nal
com
mu
nic
atio
n).
b Tota
lnu
mbe
rof
tum
ours
;on
ean
imal
can
bear
mor
eth
anon
etu
mou
r.M
:mal
e;F:
fem
ale.
538 Dirk W. Lachenmeier et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550
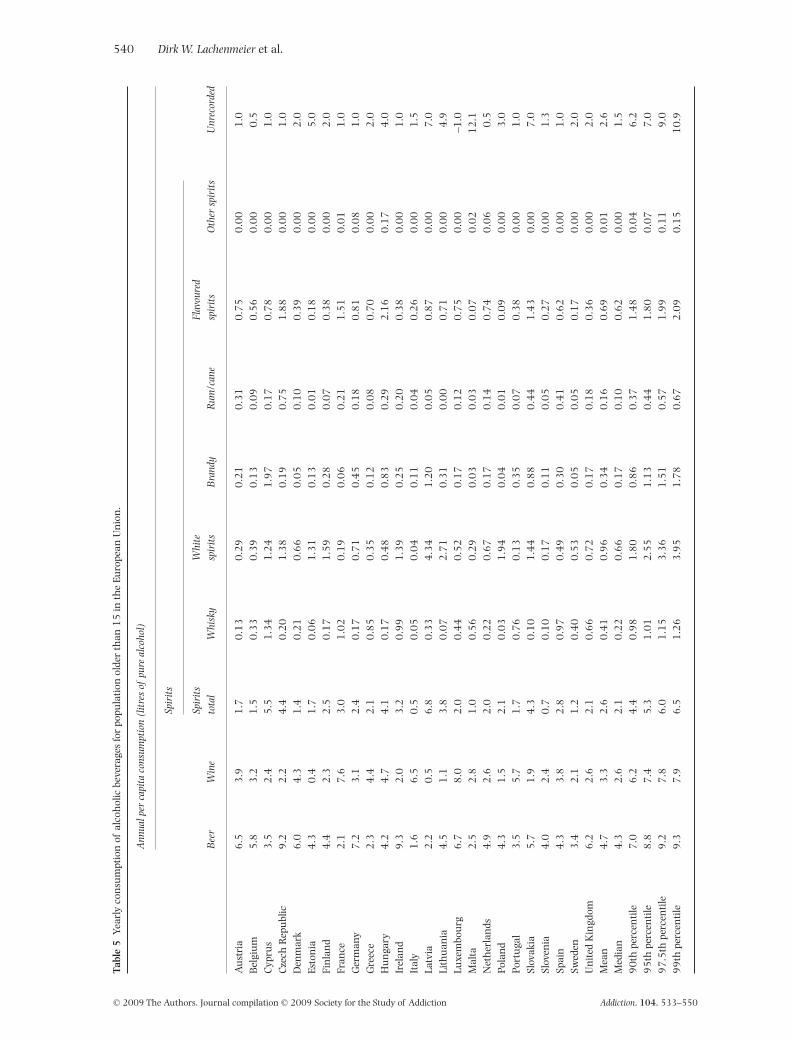
mation on acetaldehyde contents. The only currentstudy on a large sample of alcoholic beverages was pro-vided by Lachenmeier & Sohnius [3]. However, theanalysis was focused on products from the EU. As similarstudies from other parts of the world are lacking, wedecided to limit the whole population dietary intake esti-mate to the EU. The annual per capita consumption dataare shown in Table 5. As the various spirit types contain
significant differences in their acetaldehyde content, wehave also shown the consumption of different sub-groups of spirits. The acetaldehyde concentrations ofthe corresponding beverage groups are shown inTable 6.
The acetaldehyde exposure due to alcoholic beverageconsumption (Table 7) was calculated with the combineddata from Tables 5 and 6.
Table 4 Summary of own dose–response modelling results for acetaldehyde in different animal experiments (data from Tables 1–3)and comparison with literature data from Sanner et al. [18] and Scientific Committee on Cosmetic Products and Non-Food ProductsIntended for Consumers (SCCNFP) [94].
Study End-point Modela P-valueb
BMDc
(mg/kg bodyweight/day)
BMDLd
(mg/kg bodyweight/day)
T25(mg/kg blodyweight/day)
HT25(mg/kg bodyweight/day)
[49] Hepatotoxicity (periportalarea), M
Probit 0.4735 39 24 163 48
[49] Hepatotoxicity (pericentralarea), M
Logistic 0.8782 149 86 442 130
[50] Focal hyperkeratosis offorestomach, M + Fe
Gamma 0.6027 404 155 212 59
[48] Tumour-bearing animals, M Multi-stage cancer 0.6658 114 56 (8–246)f 2–72[48] Tumour-bearing animals, F (Computation failed) – – – (9–34)f 2–9[48] Total malignant tumours, M Probit 0.2827 58 41 127g 37[48] Total malignant tumours, F Multi-stage cancer 0.0013 (152) (63) 2–110h 0.5–29[18] (no data provided) (no data provided) (no data
provided)(no data
provided)15.5i 82 –
[94] Nasal carcinomas, M – – – – 121 36.7
aData from best-fitting models selected with BMDS version 2.0 software according to US Environmental Protection Agency (EPA) criteria are presented.bA P-value greater than 0.1 indicates that the model fits the data (P-value 1.0 = perfect fit). cBMD: benchmark dose for a 10% incidence of health effect.dBMDL: lower one-sided confidence limit of the BMD. eA single curve is fitted to both sexes as the analysis revealed no significant differences indose–response between sexes. fA dose level with significant response could not be determined. The T25 range for all dose levels is shown. gT25 forsignificant dose level at 246 mg/kg body weight/day. hT25 for significant dose levels at 260 and 5 mg/kg body weight/day. iCalculated from the dosedescriptor LED1 (1.55) by multiplication with 10.
0.2
0.3
0.4
0.5
0.6
0 50 100 150 200 250
Fra
ctio
n A
ffec
ted
Dose [mg/kg bw/day]
BMDBMDL
Multistage CancerLinear extrapolation
Figure 1 Multi-stage cancer model with0.95 confidence level. BMD: benchmarkdose for a 10% incidence of health effect;BMDL: lower one-sided confidence limitof the BMD. Original data from Soffrittiet al. [48]
Risk assessment of acetaldehyde 539
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550
Tabl
e5
Yea
rly
con
sum
ptio
nof
alco
hol
icbe
vera
ges
for
popu
lati
onol
der
than
15
inth
eEu
rope
anU
nio
n.
Ann
ualp
erca
pita
cons
umpt
ion
(lit
res
ofpu
real
coho
l)
Bee
rW
ine
Spir
its
Unr
ecor
ded
Spir
its
tota
lW
hisk
yW
hite
spir
its
Bra
ndy
Rum
/can
eFl
avou
red
spir
its
Oth
ersp
irit
s
Au
stri
a6
.53
.91
.70
.13
0.2
90
.21
0.3
10
.75
0.0
01
.0B
elgi
um
5.8
3.2
1.5
0.3
30
.39
0.1
30
.09
0.5
60
.00
0.5
Cyp
rus
3.5
2.4
5.5
1.3
41
.24
1.9
70
.17
0.7
80
.00
1.0
Cze
chR
epu
blic
9.2
2.2
4.4
0.2
01
.38
0.1
90
.75
1.8
80
.00
1.0
Den
mar
k6
.04
.31
.40
.21
0.6
60
.05
0.1
00
.39
0.0
02
.0Es
ton
ia4
.30
.41
.70
.06
1.3
10
.13
0.0
10
.18
0.0
05
.0Fi
nla
nd
4.4
2.3
2.5
0.1
71
.59
0.2
80
.07
0.3
80
.00
2.0
Fran
ce2
.17
.63
.01
.02
0.1
90
.06
0.2
11
.51
0.0
11
.0G
erm
any
7.2
3.1
2.4
0.1
70
.71
0.4
50
.18
0.8
10
.08
1.0
Gre
ece
2.3
4.4
2.1
0.8
50
.35
0.1
20
.08
0.7
00
.00
2.0
Hu
nga
ry4
.24
.74
.10
.17
0.4
80
.83
0.2
92
.16
0.1
74
.0Ir
elan
d9
.32
.03
.20
.99
1.3
90
.25
0.2
00
.38
0.0
01
.0It
aly
1.6
6.5
0.5
0.0
50
.04
0.1
10
.04
0.2
60
.00
1.5
Latv
ia2
.20
.56
.80
.33
4.3
41
.20
0.0
50
.87
0.0
07
.0Li
thu
ania
4.5
1.1
3.8
0.0
72
.71
0.3
10
.00
0.7
10
.00
4.9
Luxe
mbo
urg
6.7
8.0
2.0
0.4
40
.52
0.1
70
.12
0.7
50
.00
–1.0
Mal
ta2
.52
.81
.00
.56
0.2
90
.03
0.0
30
.07
0.0
21
2.1
Net
her
lan
ds4
.92
.62
.00
.22
0.6
70
.17
0.1
40
.74
0.0
60
.5Po
lan
d4
.31
.52
.10
.03
1.9
40
.04
0.0
10
.09
0.0
03
.0Po
rtu
gal
3.5
5.7
1.7
0.7
60
.13
0.3
50
.07
0.3
80
.00
1.0
Slov
akia
5.7
1.9
4.3
0.1
01
.44
0.8
80
.44
1.4
30
.00
7.0
Slov
enia
4.0
2.4
0.7
0.1
00
.17
0.1
10
.05
0.2
70
.00
1.3
Spai
n4
.33
.82
.80
.97
0.4
90
.30
0.4
10
.62
0.0
01
.0Sw
eden
3.4
2.1
1.2
0.4
00
.53
0.0
50
.05
0.1
70
.00
2.0
Un
ited
Kin
gdom
6.2
2.6
2.1
0.6
60
.72
0.1
70
.18
0.3
60
.00
2.0
Mea
n4
.73
.32
.60
.41
0.9
60
.34
0.1
60
.69
0.0
12
.6M
edia
n4
.32
.62
.10
.22
0.6
60
.17
0.1
00
.62
0.0
01
.59
0th
perc
enti
le7
.06
.24
.40
.98
1.8
00
.86
0.3
71
.48
0.0
46
.29
5th
perc
enti
le8
.87
.45
.31
.01
2.5
51
.13
0.4
41
.80
0.0
77
.09
7.5
thpe
rcen
tile
9.2
7.8
6.0
1.1
53
.36
1.5
10
.57
1.9
90
.11
9.0
99
thpe
rcen
tile
9.3
7.9
6.5
1.2
63
.95
1.7
80
.67
2.0
90
.15
10
.9
540 Dirk W. Lachenmeier et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550
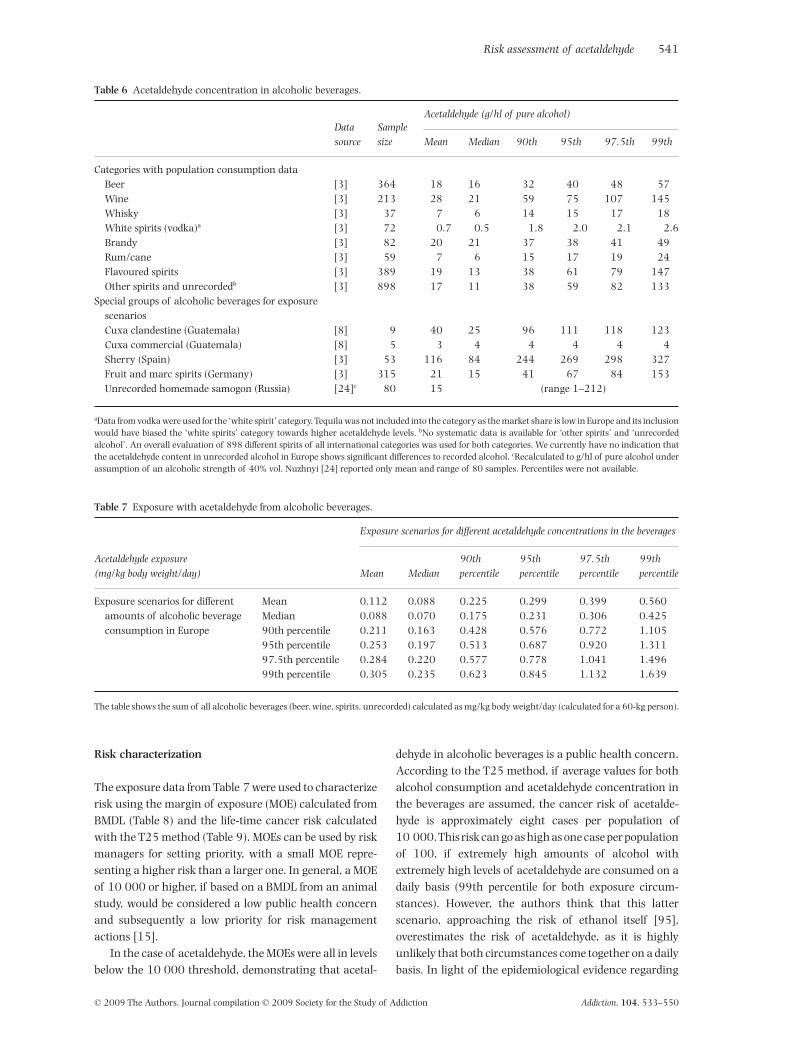
Risk characterization
The exposure data from Table 7 were used to characterizerisk using the margin of exposure (MOE) calculated fromBMDL (Table 8) and the life-time cancer risk calculatedwith the T25 method (Table 9). MOEs can be used by riskmanagers for setting priority, with a small MOE repre-senting a higher risk than a larger one. In general, a MOEof 10 000 or higher, if based on a BMDL from an animalstudy, would be considered a low public health concernand subsequently a low priority for risk managementactions [15].
In the case of acetaldehyde, the MOEs were all in levelsbelow the 10 000 threshold, demonstrating that acetal-
dehyde in alcoholic beverages is a public health concern.According to the T25 method, if average values for bothalcohol consumption and acetaldehyde concentration inthe beverages are assumed, the cancer risk of acetalde-hyde is approximately eight cases per population of10 000.This risk can go as high as one case per populationof 100, if extremely high amounts of alcohol withextremely high levels of acetaldehyde are consumed on adaily basis (99th percentile for both exposure circum-stances). However, the authors think that this latterscenario, approaching the risk of ethanol itself [95],overestimates the risk of acetaldehyde, as it is highlyunlikely that both circumstances come together on a dailybasis. In light of the epidemiological evidence regarding
Table 6 Acetaldehyde concentration in alcoholic beverages.
Datasource
Samplesize
Acetaldehyde (g/hl of pure alcohol)
Mean Median 90th 95th 97.5th 99th
Categories with population consumption dataBeer [3] 364 18 16 32 40 48 57Wine [3] 213 28 21 59 75 107 145Whisky [3] 37 7 6 14 15 17 18White spirits (vodka)a [3] 72 0.7 0.5 1.8 2.0 2.1 2.6Brandy [3] 82 20 21 37 38 41 49Rum/cane [3] 59 7 6 15 17 19 24Flavoured spirits [3] 389 19 13 38 61 79 147Other spirits and unrecordedb [3] 898 17 11 38 59 82 133
Special groups of alcoholic beverages for exposurescenariosCuxa clandestine (Guatemala) [8] 9 40 25 96 111 118 123Cuxa commercial (Guatemala) [8] 5 3 4 4 4 4 4Sherry (Spain) [3] 53 116 84 244 269 298 327Fruit and marc spirits (Germany) [3] 315 21 15 41 67 84 153Unrecorded homemade samogon (Russia) [24]c 80 15 (range 1–212)
aData from vodka were used for the ‘white spirit’ category. Tequila was not included into the category as the market share is low in Europe and its inclusionwould have biased the ‘white spirits’ category towards higher acetaldehyde levels. bNo systematic data is available for ‘other spirits’ and ‘unrecordedalcohol’. An overall evaluation of 898 different spirits of all international categories was used for both categories. We currently have no indication thatthe acetaldehyde content in unrecorded alcohol in Europe shows significant differences to recorded alcohol. cRecalculated to g/hl of pure alcohol underassumption of an alcoholic strength of 40% vol. Nuzhnyi [24] reported only mean and range of 80 samples. Percentiles were not available.
Table 7 Exposure with acetaldehyde from alcoholic beverages.
Acetaldehyde exposure(mg/kg body weight/day)
Exposure scenarios for different acetaldehyde concentrations in the beverages
Mean Median90thpercentile
95thpercentile
97.5thpercentile
99thpercentile
Exposure scenarios for differentamounts of alcoholic beverageconsumption in Europe
Mean 0.112 0.088 0.225 0.299 0.399 0.560Median 0.088 0.070 0.175 0.231 0.306 0.42590th percentile 0.211 0.163 0.428 0.576 0.772 1.10595th percentile 0.253 0.197 0.513 0.687 0.920 1.31197.5th percentile 0.284 0.220 0.577 0.778 1.041 1.49699th percentile 0.305 0.235 0.623 0.845 1.132 1.639
The table shows the sum of all alcoholic beverages (beer, wine, spirits, unrecorded) calculated as mg/kg body weight/day (calculated for a 60-kg person).
Risk assessment of acetaldehyde 541
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550
alcoholic beverages consumption, we think that anaverage risk in the range of 10-3 to 10-4 is probable. Ourreasoning here can only be indirect, as any higher riskshould be seen in more elevated cancer rates for countriesor regions with high acetaldehyde consumption com-pared to those with the same per capita consumption butlower acetaldehyde consumption.
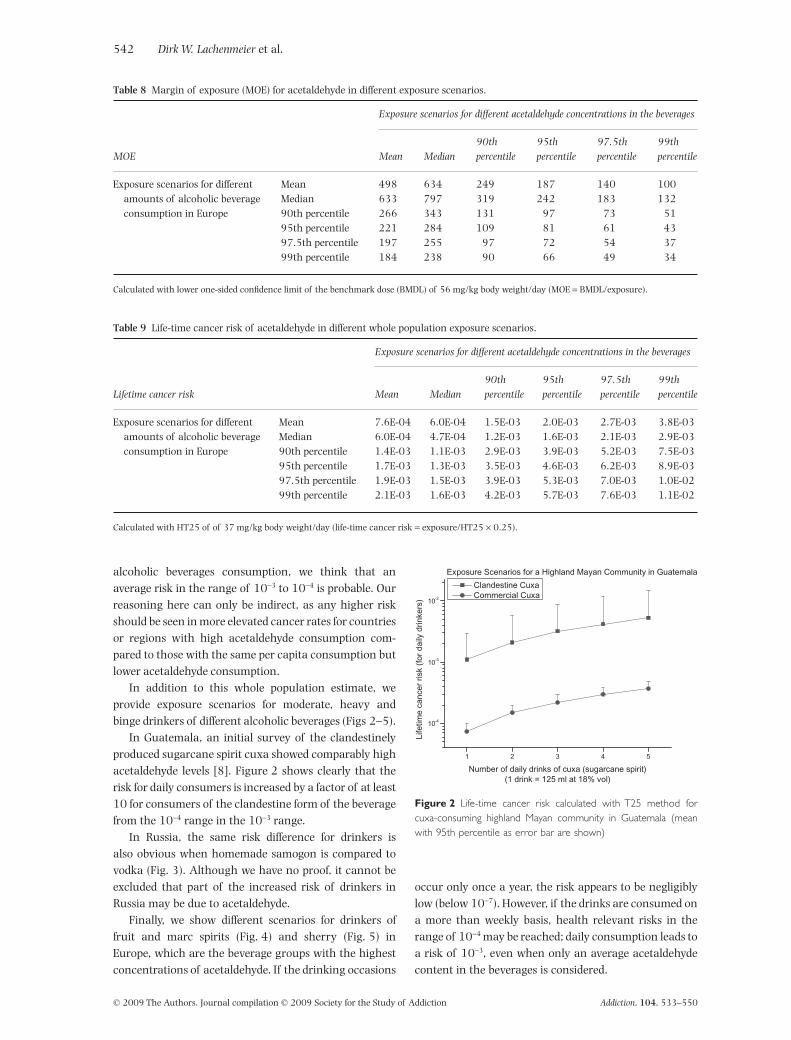
In addition to this whole population estimate, weprovide exposure scenarios for moderate, heavy andbinge drinkers of different alcoholic beverages (Figs 2–5).
In Guatemala, an initial survey of the clandestinelyproduced sugarcane spirit cuxa showed comparably highacetaldehyde levels [8]. Figure 2 shows clearly that therisk for daily consumers is increased by a factor of at least10 for consumers of the clandestine form of the beveragefrom the 10-4 range in the 10-3 range.
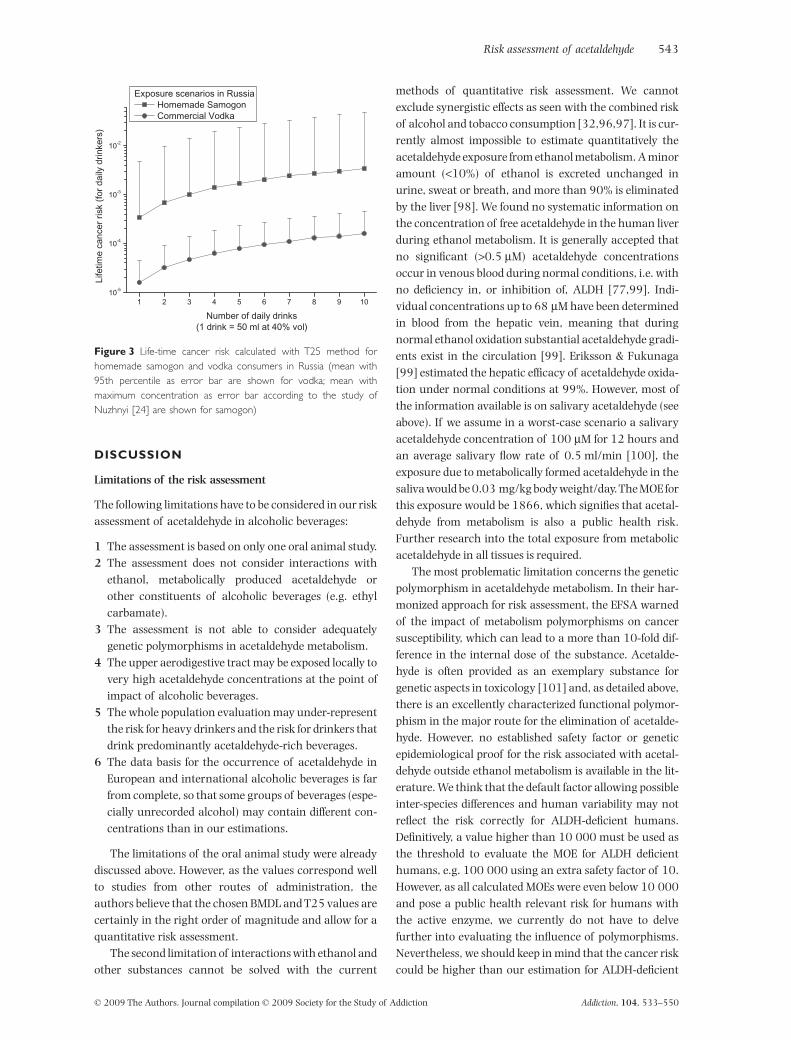
In Russia, the same risk difference for drinkers isalso obvious when homemade samogon is compared tovodka (Fig. 3). Although we have no proof, it cannot beexcluded that part of the increased risk of drinkers inRussia may be due to acetaldehyde.
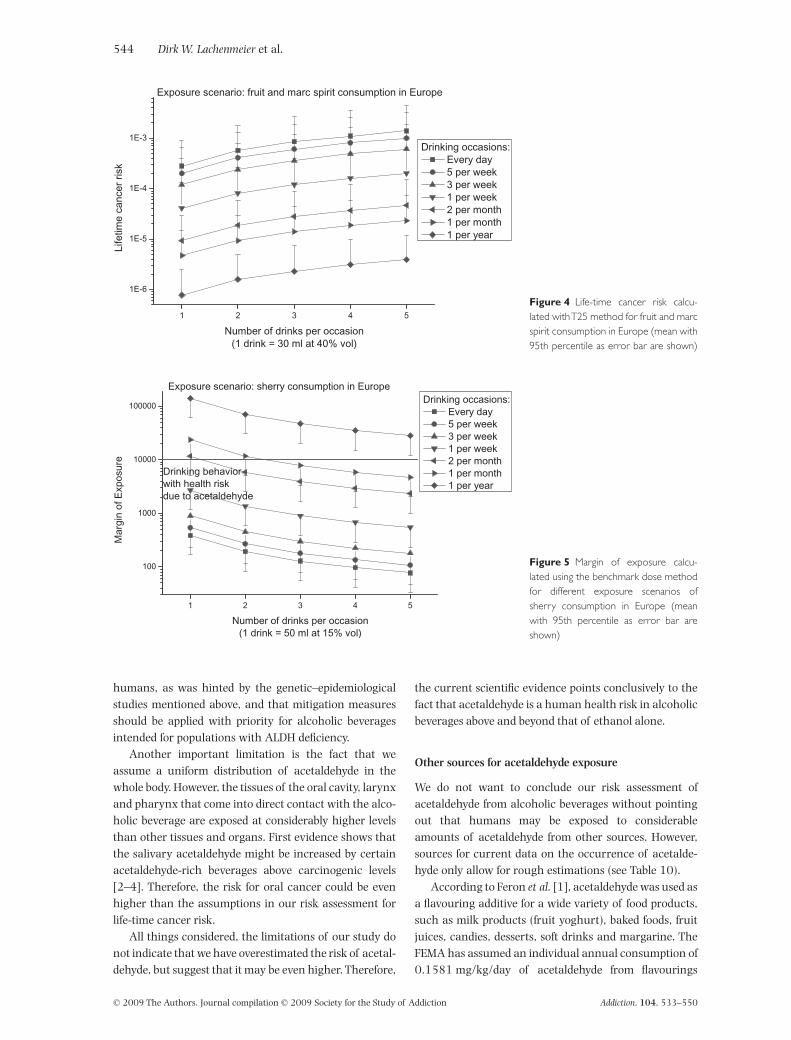
Finally, we show different scenarios for drinkers offruit and marc spirits (Fig. 4) and sherry (Fig. 5) inEurope, which are the beverage groups with the highestconcentrations of acetaldehyde. If the drinking occasions
occur only once a year, the risk appears to be negligiblylow (below 10-7). However, if the drinks are consumed ona more than weekly basis, health relevant risks in therange of 10-4 may be reached; daily consumption leads toa risk of 10-3, even when only an average acetaldehydecontent in the beverages is considered.
Table 8 Margin of exposure (MOE) for acetaldehyde in different exposure scenarios.
MOE
Exposure scenarios for different acetaldehyde concentrations in the beverages
Mean Median90thpercentile
95thpercentile
97.5thpercentile
99thpercentile
Exposure scenarios for differentamounts of alcoholic beverageconsumption in Europe
Mean 498 634 249 187 140 100Median 633 797 319 242 183 13290th percentile 266 343 131 97 73 5195th percentile 221 284 109 81 61 4397.5th percentile 197 255 97 72 54 3799th percentile 184 238 90 66 49 34
Calculated with lower one-sided confidence limit of the benchmark dose (BMDL) of 56 mg/kg body weight/day (MOE = BMDL/exposure).
Table 9 Life-time cancer risk of acetaldehyde in different whole population exposure scenarios.
Lifetime cancer risk
Exposure scenarios for different acetaldehyde concentrations in the beverages
Mean Median90thpercentile
95thpercentile
97.5thpercentile
99thpercentile
Exposure scenarios for differentamounts of alcoholic beverageconsumption in Europe
Mean 7.6E-04 6.0E-04 1.5E-03 2.0E-03 2.7E-03 3.8E-03Median 6.0E-04 4.7E-04 1.2E-03 1.6E-03 2.1E-03 2.9E-0390th percentile 1.4E-03 1.1E-03 2.9E-03 3.9E-03 5.2E-03 7.5E-0395th percentile 1.7E-03 1.3E-03 3.5E-03 4.6E-03 6.2E-03 8.9E-0397.5th percentile 1.9E-03 1.5E-03 3.9E-03 5.3E-03 7.0E-03 1.0E-0299th percentile 2.1E-03 1.6E-03 4.2E-03 5.7E-03 7.6E-03 1.1E-02
Calculated with HT25 of of 37 mg/kg body weight/day (life-time cancer risk = exposure/HT25 ¥ 0.25).
1 2 3 4 5
10-4
10-3
10-2
Exposure Scenarios for a Highland Mayan Community in Guatemala
Life
time
canc
er r
isk
(for
dai
ly d
rinke
rs)
Number of daily drinks of cuxa (sugarcane spirit)(1 drink = 125 ml at 18% vol)
Clandestine Cuxa Commercial Cuxa
Figure 2 Life-time cancer risk calculated with T25 method forcuxa-consuming highland Mayan community in Guatemala (meanwith 95th percentile as error bar are shown)
542 Dirk W. Lachenmeier et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550
DISCUSSION
Limitations of the risk assessment
The following limitations have to be considered in our riskassessment of acetaldehyde in alcoholic beverages:
1 The assessment is based on only one oral animal study.2 The assessment does not consider interactions with
ethanol, metabolically produced acetaldehyde orother constituents of alcoholic beverages (e.g. ethylcarbamate).
3 The assessment is not able to consider adequatelygenetic polymorphisms in acetaldehyde metabolism.
4 The upper aerodigestive tract may be exposed locally tovery high acetaldehyde concentrations at the point ofimpact of alcoholic beverages.
5 The whole population evaluation may under-representthe risk for heavy drinkers and the risk for drinkers thatdrink predominantly acetaldehyde-rich beverages.
6 The data basis for the occurrence of acetaldehyde inEuropean and international alcoholic beverages is farfrom complete, so that some groups of beverages (espe-cially unrecorded alcohol) may contain different con-centrations than in our estimations.
The limitations of the oral animal study were alreadydiscussed above. However, as the values correspond wellto studies from other routes of administration, theauthors believe that the chosen BMDL and T25 values arecertainly in the right order of magnitude and allow for aquantitative risk assessment.
The second limitation of interactions with ethanol andother substances cannot be solved with the current
methods of quantitative risk assessment. We cannotexclude synergistic effects as seen with the combined riskof alcohol and tobacco consumption [32,96,97]. It is cur-rently almost impossible to estimate quantitatively theacetaldehyde exposure from ethanol metabolism. A minoramount (<10%) of ethanol is excreted unchanged inurine, sweat or breath, and more than 90% is eliminatedby the liver [98]. We found no systematic information onthe concentration of free acetaldehyde in the human liverduring ethanol metabolism. It is generally accepted thatno significant (>0.5 mM) acetaldehyde concentrationsoccur in venous blood during normal conditions, i.e. withno deficiency in, or inhibition of, ALDH [77,99]. Indi-vidual concentrations up to 68 mM have been determinedin blood from the hepatic vein, meaning that duringnormal ethanol oxidation substantial acetaldehyde gradi-ents exist in the circulation [99]. Eriksson & Fukunaga[99] estimated the hepatic efficacy of acetaldehyde oxida-tion under normal conditions at 99%. However, most ofthe information available is on salivary acetaldehyde (seeabove). If we assume in a worst-case scenario a salivaryacetaldehyde concentration of 100 mM for 12 hours andan average salivary flow rate of 0.5 ml/min [100], theexposure due to metabolically formed acetaldehyde in thesaliva would be 0.03 mg/kg body weight/day.The MOE forthis exposure would be 1866, which signifies that acetal-dehyde from metabolism is also a public health risk.Further research into the total exposure from metabolicacetaldehyde in all tissues is required.
The most problematic limitation concerns the geneticpolymorphism in acetaldehyde metabolism. In their har-monized approach for risk assessment, the EFSA warnedof the impact of metabolism polymorphisms on cancersusceptibility, which can lead to a more than 10-fold dif-ference in the internal dose of the substance. Acetalde-hyde is often provided as an exemplary substance forgenetic aspects in toxicology [101] and, as detailed above,there is an excellently characterized functional polymor-phism in the major route for the elimination of acetalde-hyde. However, no established safety factor or geneticepidemiological proof for the risk associated with acetal-dehyde outside ethanol metabolism is available in the lit-erature. We think that the default factor allowing possibleinter-species differences and human variability may notreflect the risk correctly for ALDH-deficient humans.Definitively, a value higher than 10 000 must be used asthe threshold to evaluate the MOE for ALDH deficienthumans, e.g. 100 000 using an extra safety factor of 10.However, as all calculated MOEs were even below 10 000and pose a public health relevant risk for humans withthe active enzyme, we currently do not have to delvefurther into evaluating the influence of polymorphisms.Nevertheless, we should keep in mind that the cancer riskcould be higher than our estimation for ALDH-deficient
1 2 3 4 5 6 7 8 9 1010-5
10-4
10-3
10-2
Life
time
canc
er r
isk
(for
dai
ly d
rinke
rs)
Number of daily drinks(1 drink = 50 ml at 40% vol)
Exposure scenarios in Russia Homemade Samogon Commercial Vodka
Figure 3 Life-time cancer risk calculated with T25 method forhomemade samogon and vodka consumers in Russia (mean with95th percentile as error bar are shown for vodka; mean withmaximum concentration as error bar according to the study ofNuzhnyi [24] are shown for samogon)
Risk assessment of acetaldehyde 543
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550
humans, as was hinted by the genetic–epidemiologicalstudies mentioned above, and that mitigation measuresshould be applied with priority for alcoholic beveragesintended for populations with ALDH deficiency.
Another important limitation is the fact that weassume a uniform distribution of acetaldehyde in thewhole body. However, the tissues of the oral cavity, larynxand pharynx that come into direct contact with the alco-holic beverage are exposed at considerably higher levelsthan other tissues and organs. First evidence shows thatthe salivary acetaldehyde might be increased by certainacetaldehyde-rich beverages above carcinogenic levels[2–4]. Therefore, the risk for oral cancer could be evenhigher than the assumptions in our risk assessment forlife-time cancer risk.
All things considered, the limitations of our study donot indicate that we have overestimated the risk of acetal-dehyde, but suggest that it may be even higher. Therefore,
the current scientific evidence points conclusively to thefact that acetaldehyde is a human health risk in alcoholicbeverages above and beyond that of ethanol alone.
Other sources for acetaldehyde exposure
We do not want to conclude our risk assessment ofacetaldehyde from alcoholic beverages without pointingout that humans may be exposed to considerableamounts of acetaldehyde from other sources. However,sources for current data on the occurrence of acetalde-hyde only allow for rough estimations (see Table 10).
According to Feron et al. [1], acetaldehyde was used asa flavouring additive for a wide variety of food products,such as milk products (fruit yoghurt), baked foods, fruitjuices, candies, desserts, soft drinks and margarine. TheFEMA has assumed an individual annual consumption of0.1581 mg/kg/day of acetaldehyde from flavourings
1 2 3 4 5
1E-6
1E-5
1E-4
1E-3
Exposure scenario: fruit and marc spirit consumption in Europe
Life
time
canc
er r
isk
Number of drinks per occasion(1 drink = 30 ml at 40% vol)
Drinking occasions: Every day 5 per week 3 per week 1 per week 2 per month 1 per month 1 per year
Figure 4 Life-time cancer risk calcu-lated withT25 method for fruit and marcspirit consumption in Europe (mean with95th percentile as error bar are shown)
1 2 3 4 5
100
1000
10000
100000
Mar
gin
of E
xpos
ure
Number of drinks per occasion(1 drink = 50 ml at 15% vol)
Drinking occasions: Every day 5 per week 3 per week 1 per week 2 per month 1 per month 1 per year
Drinking behaviorwith health riskdue to acetaldehyde
Exposure scenario: sherry consumption in Europe
Figure 5 Margin of exposure calcu-lated using the benchmark dose methodfor different exposure scenarios ofsherry consumption in Europe (meanwith 95th percentile as error bar areshown)
544 Dirk W. Lachenmeier et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550

[102].The JECFA estimated similar daily per capita intakesof acetaldehyde from flavourings to be 0.16 mg/kg bodyweight/day for the United States and 0.18 mg/kg bodyweight/day for Europe [36].
The exposure from cosmetics appears to be almost neg-ligible, with a maximum exposure of 0.1 mg/kg bodyweight/day according to SCCNFP [94]. Other minor expo-sures include migration from packaging materials [e.g.polyethylene terephthalate (PET)] [103,104], certainurban environments [105–107], exposure in the work-place [108] and car exhaust if bioethanol [109,110] isused as the fuel source. Besides alcoholic beverages,tobacco smoke appears to be the most significant exposure[111–114], followed by food flavourings [36,102].
The next step for a holistic risk assessment of acetal-dehyde would therefore be to include all these othersources into the exposure assessment. As current andsystematic data on acetaldehyde exposure in productsother than alcoholic beverages appear to be lacking, sys-tematic research into the occurrence and exposure ofacetaldehyde, especially as flavouring in foodstuffs, whichappear to be a significant factor, should be undertakenwith priority.
CONCLUSION
The major result from this study is the fact that acetalde-hyde outside ethanol metabolism poses a risk for drinkersof alcoholic beverages above the risk of ethanol andmetabolically formed acetaldehyde. The risk for acetalde-hyde outside ethanol metabolism largely depends uponthe type of beverage consumed as the contents vary con-siderably. To evaluate the above life-time risks, we wouldlike to give some comparisons with other life-time risks;for example, for environmental exposures over time, mostgovernments use a standard of an increased life-timecancer risk between 1 : 10 000 and 1 : 1 000 000 as notacceptable [115,116]. For acetaldehyde exposure in thecity of Toronto, the set benchmark of 1 : 1 000 000 was
exceeded by a factor of 6, leading to a mandatory moni-toring systems via a reporting bylaw [117,118].
Also, alcohol consumption is a voluntary behaviouraccepted to a degree, which creates levels of risk above1 : 1000 for chronic or episodic heavy life-time drinkers[95,119]. As the risk for acetaldehyde via beverageconsumption outside the ethanol metabolism is also atthis level, this factor should be considered as confounderin future epidemiological studies on alcohol consump-tion, particularly in regions with high unrecordedconsumption.
Our calculation shows risk in a magnitude that is nor-mally considered a high priority for regulatory measures.This is evidenced by the application of measures toreduce human exposure to substances such as acryla-mide and ethyl carbamate, whose MOEs had been foundin the same ranges as our calculations for acetaldehyde[14,120,121]. However, as the risk from ethanol is atleast one order of magnitude higher than that fromacetaldehyde in alcoholic beverages (i.e. 10-3–10-2) [95],a re-focus of measures on acetaldehyde could distractfrom the real problem of reducing alcohol consumptionitself [122,123]. Nevertheless, under certain circum-stances (e.g. high consumption of acetaldehyde-rich bev-erages, such as certain fruit or marc spirits in Europe orcuxa spirits in Guatemala) the risk of acetaldehydebecomes significant and reaches such a high proportionthat our advice to policy makers is to reduce the exposureto this substance. In these cases, the contamination ofspirits with acetaldehyde not only poses a health risk butis also a flaw in product quality, as the acetaldehyde canbe separated effectively during distillation. While acetal-dehyde in spirits can be eliminated readily, this is moredifficult in the beverage groups of wine and beer, whichare not produced using distillation, as well as fortifiedwines, in which acetaldehyde is formed purposefully forflavouring. The EFSA states clearly that substances whichare both genotoxic and carcinogenic should not be addeddeliberately to foods [15]. This demand would certainly
Table 10 Human exposure with acetaldehyde from various sources.
Source Reference Exposure (mg/kg body weight/day) MOE
Alcoholic beverages (This study) 0.1–1.6 560–35Environmental tobacco smoke [113] 0.075–0.170 (746–329)a
Tobacco smoke Own estimation, withdata from [111]
0.3 (20 cigarettes daily, 1 mg acetaldehydeper cigarette, 60 kg body weight)
(187)a
Food flavourings [36] 0.16–0.18 350–311Cosmetics [94] 0.0001 (560 000)a
Work-place (Brazil) [108] 0.00095–0.00346 (59 072–16 185)a
aNon-oral exposure. Margin of exposure (MOE) calculated with oral lower one-sided confidence limit of the benchmark dose (BMDL) for comparisonpurposes.
Risk assessment of acetaldehyde 545
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550

also apply to the deliberate formation of acetaldehyde bymicrobiological processes.
Therefore, we recommend that the ALARA principle(‘as low as reasonably achievable’), introduced into theCodex Alimentarius standards for dealing with contami-nants and toxins [124] and the corresponding EU legis-lation [125], should be applied in these cases and thatacetaldehyde levels in beverages should be reduced as lowas technologically possible and that regulators shouldconsider the implementation of maximum limits foracetaldehyde in spirits. For precautionary public healthprotection, the same ALARA demand should be posed toacetaldehyde in tobacco smoke and other food and bever-age products.
Finally, our quantitative risk assessment providesstrong evidence against the GRAS evaluation of acetal-dehyde. The genetic epidemiological evidence also sug-gests an upgrade of the carcinogen classification ofacetaldehyde. Thus, the international and nationalbodies (IARC, JECFA, FDA and EU) should re-consider thestatus of acetaldehyde as a priority.
Declarations of interest
None.
References
1. Feron V. J., Til H. P., de Vrijer F., Woutersen R. A., Cassee F.R., van Bladeren P.J. Aldehydes: occurrence, carcinogenicpotential, mechanism of action and risk assessment.Mutat Res 1991; 259: 363–85.
2. Linderborg K., Joly J. P., Visapää J. P., Salaspuro M. Poten-tial mechanism for Calvados-related oesophageal cancer.Food Chem Toxicol 2008; 46: 476–9.
3. Lachenmeier D. W., Sohnius E. M. The role of acetaldehydeoutside ethanol metabolism in the carcinogenicity of alco-holic beverages: evidence from a large chemical survey.Food Chem Toxicol 2008; 46: 2903–11.
4. Yokoyama A., Tsutsumi E., Imazeki H., Suwa Y., Naka-mura C., Mizukami T. et al. Salivary acetaldehyde concen-tration according to alcoholic beverage consumed andaldehyde dehydrogenase-2 genotype. Alcohol Clin Exp Res2008; 32: 1607–14.
5. Lachenmeier D. W., Rehm J., Gmel G. Surrogate alcohol:what do we know and where do we go? Alcohol Clin Exp Res2007; 31: 1613–24.
6. Rehm J., Lachenmeier D. W. Composition of alcohol frommarkets in different countries. Alcohol Clin Exp Res 2008;32: A293.
7. Rehm J., Patra J., Baliunas D., Popova S., Roerecke M.,Taylor B. Alcohol, The Burden of Disease of. In: Heggen-hougen K., Quah S., editors. International Encyclopedia ofPublic Health, vol. 1. San Diego, CA: Academic Press; 2008,p. 135–51.
8. Kanteres F., Lachenmeier D. W., Rehm J. Alcohol in MayanGuatemala: consumption, distribution, production andcomposition of cuxa. Addiction 2009; in press. Epub aheadof print; DOI: 10.1111/j.1360-0443.2009.02507.x.
9. Lachenmeier D. W., Sohnius E.-M., Attig R., López M. G.
Quantification of selected volatile constituents andanions in Mexican agave spirits (Tequila, Mezcal, Sotol.Bacanora). J Agric Food Chem 2006; 54: 3911–15.
10. Oliveira V. A., Vicente M. A., Fietto L. G., Castro I. M.,Coutrim M. X., Schüller D. et al. Biochemical and molecu-lar characterization of Saccharomyces cerevisiae strainsobtained from sugar-cane juice fermentations and theirimpact in cachaça production. Appl Environ Microbiol2008; 74: 693–701.
11. Miranda M. B., Martins N. G. S., Belluco A. E. S., Horii J.,Alcarde A. R. Chemical quality of Brazilian sugarcanespirits. Cienc Tecnol Aliment 2007; 27: 897–901.
12. Paine A. J., Dayan A. D. Defining a tolerable concentrationof methanol in alcoholic drinks. Hum Exp Toxicol 2001;20: 563–8.
13. Lachenmeier D. W., Haupt S., Schulz K. Definingmaximum levels of higher alcohols in alcoholic beveragesand surrogate alcohol products. Regul Toxicol Pharmacol2008; 50: 313–21.
14. European Food Safety Authority (EFSA). Ethyl carbamateand hydrocyanic acid in food and beverages. EFSA J 2007;551: 1–44.
15. European Food Safety Authority (EFSA). Opinion of theScientific Committee on a request from EFSA related to aharmonised approach for risk assessment of substanceswhich are both genotoxic and carcinogenic. EFSA J 2005;282: 1–31.
16. Dybing E., Sanner T., Roelfzema H., Kroese D., Tennant R.W. T25: a simplified carcinogenic potency index: descrip-tion of the system and study of correlations between car-cinogenic potency and species/site specificity andmutagenicity. Pharmacol Toxicol 1997; 80: 272–9.
17. Van Landingham C. B., Allen B. C., Shipp A. M., Crump K.S. Comparison of the EU T25 single point estimate methodwith benchmark dose response modeling for estimatingpotency of carcinogens. Risk Anal 2001; 21: 641–56.
18. Sanner T., Dybing E., Willems M. I., Kroese E. D. A simplemethod for quantitative risk assessment of non-thresholdcarcinogens based on the dose descriptor T25. PharmacolToxicol 2001; 88: 331–41.
19. World Health Organization (WHO). Global InformationSystem on Alcohol and Health. Available at: http://www.who.int/globalatlas/default.asp (accessed 5 September2008).
20. Rehm J., Rehn N., Room R., Monteiro M., Gmel G., JerniganD. et al. The global distribution of average volume ofalcohol consumption and patterns of drinking. Eur AddictRes 2003; 9: 147–56.
21. Rehm J., Klotsche J., Patra J. Comparative quantification ofalcohol exposure as risk factor for global burden of disease.Int J Methods Psychiatr Res 2007; 16: 66–76.
22. Rehm J., Room R., Monteiro M., Gmel G., Graham K., RehnN. et al. Alcohol use. In: Ezzati M., Lopez A. D., Rodgers A.,Murray C. J. L., editors. Comparative Quantification of HealthRisks. Global and Regional Burden of Disease Attributable toSelected Major Risk Factors, vol. 1. Geneva: World HealthOrganization; 2004, p. 959–1108.
23. The European Spirits Organization (CEPS). EU Alcohol Con-sumption per 000 9L cases. 2005. Available at: http://www.europeanspirits.org/documents/stats_consumption_per_000_9l_cases_20051.pdf (accessed 5 September 2008).
24. Nuzhnyi V. Chemical composition, toxic, and organolepticproperties of noncommercial alcohol samples. In: HaworthA., Simpson R., editors. Moonshine Markets. Issues in
546 Dirk W. Lachenmeier et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550
Unrecorded Alcohol Beverage Production and Consumption.New York: Brunner-Routledge; 2004, p. 177–99.
25. Tuyns A. Alcohol and cancer. Alcohol Health Res World1978; 2: 20–31.
26. Tuyns A. J. Oesophageal cancer in non-smoking drinkersand in non-drinking smokers. Int J Cancer 1983; 32:443–4.
27. Brugere J., Guenel P., Leclerc A., Rodriguez J. Differential-effects of tobacco and alcohol in cancer of the larynx,pharynx, and mouth. Cancer 1986; 57: 391–5.
28. Maier H., Dietz A., Zielinski D., Junemann K. H., HellerW. D. Risk-factors associated with squamous epitheliomasof the mouth, oropharynx, hypopharynx and larynx.Dtsch Med Wochenschr 1990; 115: 843–50.
29. Seitz H. K., Oneta C. M. Gastrointestinal alcohol dehydro-genase. Nutr Rev 1998; 56: 52–60.
30. Seitz H. K., Pöschl G., Stickel F. Alcohol and colorectalcancer. In: Scheppach W., Scheuerle M., editors. ExogenousFactors in Colonic Carcinogenesis. Dordrecht, Boston,London: Kluwer Academic Publishers; 2003, p. 128–41.
31. Doll R., Forman D., La Vecchia C., Woutersen R. Alcoholicbeverages and cancers of the digestive tract and larynx. In:MacDonald I., editor. Health Issues Related to Alcohol Con-sumption, 2nd edn. Oxford: Blackwell Science; 1999, p.351–93.
32. Baan R., Straif K., Grosse Y., Secretan B., El Ghissassi F.,Bouvard V. et al. Carcinogenicity of alcoholic beverages.Lancet Oncol 2007; 8: 292–3.
33. Sim V. M., Pattle R. E. Effect of possible smog irritants onhuman subjects. JAMA 1957; 165: 1908–13.
34. Bittersohl G. Epidemiological research on cancer risk byaldol and aliphatic aldehydes. Environ Qual Saf 1975; 4:235–8.
35. Hall R. L., Oser B. L. Recent progress in the consideration offlavoring ingredients under the food additives amendment.III. GRAS substances. Food Technol 1965; 19: 197.
36. Joint FAO/WHO Expert Committee on Food Additives(JECFA). Saturated aliphatic acyclic linear primary alco-hols, aldehydes, and acids. In: WHO Food Additives Series40. Safety Evaluation of Certain Food Additives and Contami-nants. Geneva, Switzerland: World Health Organization;1998, p. 148–88.
37. Yokoyama A., Muramatsu T., Ohmori T., Higuchi S.,Hayashida M., Ishii H. Esophageal cancer and aldehydedehydrogenase-2 genotypes in Japanese males. Cancer Epi-demiol Biomarkers Prev 1996; 5: 99–102.
38. Yokoyama A., Omori T., Yokoyama T., Sato Y., KawakuboH., Maruyama K. Risk of metachronous squamous cellcarcinoma in the upper aerodigestive tract of Japanesealcoholic men with esophageal squamous cell carcinoma:a long-term endoscopic follow-up study. Cancer Sci 2008;99: 1164–71.
39. Yokoyama A., Muramatsu T., Omori T., Matsushita S.,Yoshimizu H., Higuchi S. et al. Alcohol and aldehyde dehy-drogenase gene polymorphisms influence susceptibility toesophageal cancer in Japanese alcoholics. Alcohol Clin ExpRes 1999; 23: 1705–10.
40. Zhang F. F., Hou L., Terry M. B., Lissowska J., Morabia A.,Chen J. et al. Genetic polymorphisms in alcohol metabo-lism, alcohol intake and the risk of stomach cancer inWarsaw, Poland. Int J Cancer 2007; 121: 2060–4.
41. Launoy G., Milan C., Day N. E., Faivre J., Pienkowski P.,Gignoux M. Oesophageal cancer in France: potential
importance of hot alcoholic drinks. Int J Cancer 1997; 71:917–23.
42. Launoy G., Milan C., Day N. E., Pienkowski M. P., GignouxM., Faivre J. Diet and squamous-cell cancer of theoesophagus: a French multicentre case–control study. Int JCancer 1998; 76: 7–12.
43. Yokoyama A., Ohmori T., Muramatsu T., Higuchi S.,Yokoyama T., Matsushita S. et al. Cancer screening ofupper aerodigestive tract in Japanese alcoholics withreference to drinking and smoking habits and aldehydedehydrogenase-2 genotype. Int J Cancer 1996; 68: 313–16.
44. Seitz H. K., Stickel F. Molecular mechanisms of alcohol-mediated carcinogenesis. Nat Rev Cancer 2007; 7: 599–612.
45. Pöschl G., Seitz H. K. Alcohol and cancer. Alcohol Alcohol2004; 39: 155–65.
46. Woutersen R. A., Appelman L. M., Feron V. J., Van derHeijden C. A. Inhalation toxicity of acetaldehyde in rats. II.Carcinogenicity study: interim results after 15 months.Toxicology 1984; 31: 123–33.
47. Woutersen R. A., Appelman L. M., Van Garderen-HoetmerA., Feron V. J. Inhalation toxicity of acetaldehyde in rats.III. Carcinogenicity study. Toxicology 1986; 41: 213–31.
48. Soffritti M., Belpoggi F., Lambertin L., Lauriola M., Pado-vani M., Maltoni C. Results of long-term experimentalstudies on the carcinogenicity of formaldehyde and acetal-dehyde in rats. Ann NY Acad Sci 2002; 982: 87–105.
49. Matysiak-Budnik T., Jokelainen K., Kärkkäinen P.,Mäkisalo H., Ohisalo J., Salaspuro M. Hepatotoxicity andabsorption of extrahepatic acetaldehyde in rats. J Pathol1996; 178: 469–74.
50. Til H. P., Woutersen R. A., Feron V. J., Clary J. J. Evaluationof the oral toxicity of acetaldehyde and formaldehyde in a4-week drinking-water study in rats. Food Chem Toxicol1988; 26: 447–52.
51. Homann N., Kärkkäinen P., Koivisto T., Nosova T., Joke-lainen K., Salaspuro M. Effects of acetaldehyde on cellregeneration and differentiation of the upper gastrointes-tinal tract mucosa. J Natl Cancer Inst 1997; 89: 1692–7.
52. Maltoni C., Ciliberti A., Lefemine G., Soffritti M. Results ofa long-term experimental study on the carcinogenicity ofvinyl acetate monomer in mice. Ann NY Acad Sci 1997;837: 209–38.
53. Minardi F., Belpoggi F., Soffritti M., Ciliberti A., Lauriola M.,Cattin E. et al. Results of long-term carcinogenicity bioas-say on vinyl acetate monomer in Sprague–Dawley rats.Ann NY Acad Sci 2002; 982: 106–22.
54. Belpoggi F., Soffritti M., Minardi F., Ciliberti A., PadovaniM., Cattin E. et al. Results of a long-term carcinogenicitybioassay on vinyl acetate monomer in Wistar rats. Eur JOncol 2002; 7: 279–93.
55. Soffritti M., Belpoggi F., Cevolani D., Guarino M., PadovaniM., Maltoni C. Results of long-term experimental studieson the carcinogenicity of methyl alcohol and ethyl alcoholin rats. Ann NY Acad Sci 2002; 982: 46–69.
56. International Agency for Research on Cancer (IARC).Acetaldehyde. In: IARC Monographs on the Evaluation ofCarcinogenic Risks to Humans, vol. 36. Allyl Compounds,Aldehydes, Epoxides and Peroxides. Lyon, France: Interna-tional Agency for Research on Cancer; 1985, p. 101–32.
57. International Agency for Research on Cancer (IARC).Acetaldehyde. In: IARC Monographs on the Evaluation ofCarcinogenic Risks to Humans, Supplement 7. Overall Evalu-ations of Carcinogenicity: An Updating of IARC Monographs,
Risk assessment of acetaldehyde 547
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550

vols 1– 42. Lyon, France: International Agency forResearch on Cancer; 1987, p. 77–8.
58. International Agency for Research on Cancer (IARC).Acetaldehyde. In: IARC Monographs on the Evaluation ofCarcinogenic Risks to Humans, vol. 71. Re-Evaluation ofSome Organic Chemicals, Hydrazine and Hydrogen Peroxide.Lyon, France: International Agency for Research onCancer; 1999, p. 319–35.
59. International Agency for Research on Cancer (IARC).IARC Monographs on the Evaluation of Carcinogenic Risks toHumans, vol. 96. Alcoholic Beverage Consumption and EthylCarbamate (Urethane). Lyon, France: International Agencyfor Research on Cancer; in press.
60. Theruvathu J. A., Jaruga P., Nath R. G., DizdarogluM., Brooks P. J. Polyamines stimulate the formationof mutagenic 1,N2-propanodeoxyguanosine adducts fromacetaldehyde. Nucleic Acids Res 2005; 33: 3513–20.
61. Cheng G., Shi Y., Sturla S. J., Jalas J. R., McIntee E. J., Vil-lalta P. W. et al. Reactions of formaldehyde plus acetalde-hyde with deoxyguanosine and DNA: formation of cyclicdeoxyguanosine adducts and formaldehyde cross-links.Chem Res Toxicol 2003; 16: 145–52.
62. Fang J. L., Vaca C. E. Detection of DNA adducts of acetal-dehyde in peripheral white blood cells of alcohol abusers.Carcinogenesis 1997; 18: 627–32.
63. Hecht S. S., McIntee E. J., Wang M. New DNA adducts ofcrotonaldehyde and acetaldehyde. Toxicology 2001; 166:31–6.
64. Noori P., Hou S. M. Mutational spectrum induced byacetaldehyde in the HPRT gene of human T lymphocytesresembles that in the p53 gene of esophageal cancers. Car-cinogenesis 2001; 22: 1825–30.
65. Wang M., McIntee E. J., Cheng G., Shi Y., Villalta P. W.,Hecht S. S. Identification of DNA adducts of acetaldehyde.Chem Res Toxicol 2000; 13: 1149–57.
66. Obe G., Jonas R., Schmidt S. Metabolism of ethanol in vitroproduces a compound which induces sister-chromatidexchanges in human peripheral lymphocytes in vitro:acetaldehyde not ethanol is mutagenic. Mutat Res 1986;174: 47–51.
67. Dellarco V. L. A mutagenicity assessment of acetaldehyde.Mutat Res 1988; 195: 1–20.
68. Helander A., Lindahl-Kiessling K. Increased frequency ofacetaldehyde-induced sister-chromatid exchanges inhuman lymphocytes treated with an aldehyde dehydroge-nase inhibitor. Mutat Res 1991; 264: 103–7.
69. Espina N., Lima V., Lieber C. S., Garro A. J. In vitro and invivo inhibitory effect of ethanol and acetaldehyde onO6-methylguanine transferase. Carcinogenesis 1988; 9:761–6.
70. Paget V., Lechevrel M., Sichel F. Acetaldehyde-inducedmutational pattern in the tumour suppressor gene TP53analysed by use of a functional assay, the FASAY (func-tional analysis of separated alleles in yeast). Mutat Res2008; 652: 12–9.
71. Castro G. D., de Castro C. R., Maciel M. E., Fanelli S. L., deFerreyra E. C., Gómez M. I. D. et al. Ethanol-induced oxida-tive stress and acetaldehyde formation in rat mammarytissue: potential factors involved in alcohol drinking pro-motion of breast cancer. Toxicology 2006; 219: 208–19.
72. Terry M. B., Gammon M. D., Zhang F. F., Knight J. A., WangQ., Britton J. A. et al. ADH3 genotype, alcohol intake andbreast cancer risk. Carcinogenesis 2006; 27: 840–7.
73. Obe G., Ristow H. Acetaldehyde, but not ethanol, induces
sister chromatid exchanges in Chinese-hamster cells invitro. Mutat Res 1977; 56: 211–13.
74. Salaspuro M. P. Acetaldehyde, microbes, and cancer of thedigestive tract. Crit Rev Clin Lab Sci 2003; 40: 183–208.
75. Jokelainen K., Siitonen A., Jousimies-Somer H., Nosova T.,Heine R., Salaspuro M. In vitro alcohol dehydrogenase-mediated acetaldehyde production by aerobic bacteria rep-resenting the normal colonic flora in man. Alcohol Clin ExpRes 1996; 20: 967–72.
76. Kurkivuori J., Salaspuro V., Kaihovaara P., Kari K., Rau-temaa R., Grönroos L. et al. Acetaldehyde production fromethanol by oral streptococci. Oral Oncol 2007; 43: 181–6.
77. Eriksson C. J. Measurement of acetaldehyde: what levelsoccur naturally and in response to alcohol? Novartis FoundSymp 2007; 285: 247–55.
78. Salaspuro M. Interrelationship between alcohol, smoking,acetaldehyde and cancer. Novartis Found Symp 2007; 285:80–9.
79. Homann N., Jousimies-Somer H., Jokelainen K., Heine R.,Salaspuro M. High acetaldehyde levels in saliva afterethanol consumption: methodological aspects and patho-genetic implications. Carcinogenesis 1997; 18: 1739–43.
80. Salaspuro V., Salaspuro M. Synergistic effect of alcoholdrinking and smoking on in vivo acetaldehyde concentra-tion in saliva. Int J Cancer 2004; 111: 480–3.
81. Väkeväinen S., Tillonen J., Agarwal D. P., Srivastava N.,Salaspuro M. High salivary acetaldehyde after a moderatedose of alcohol in ALDH2-deficient subjects: strong evi-dence for the local carcinogenic action of acetaldehyde.Alcohol Clin Exp Res 2000; 24: 873–7.
82. Yokoyama A., Muramatsu T., Ohmori T., Yokoyama T.,Okuyama K., Takahashi H. et al. Alcohol-related cancersand aldehyde dehydrogenase-2 in Japanese alcoholics. Car-cinogenesis 1998; 19: 1383–7.
83. Mizoi Y., Ijiri I., Tatsuno Y., Kijima T., Fujiwara S., AdachiJ. et al. Relationship between facial flushing and bloodacetaldehyde levels after alcohol intake. PharmacolBiochem Behav 1979; 10: 303–11.
84. Matsuda T., Yabushita H., Kanaly R. A., Shibutani S.,Yokoyama A. Increased DNA damage in ALDH2-deficientalcoholics. Chem Res Toxicol 2006; 19: 1374–8.
85. Lewis S. J., Smith D. G. Alcohol, ALDH2, and esophagealcancer: a meta-analysis which illustrates the potentialsand limitations of a Mendelian randomization approach.Cancer Epidemiol Biomarkers Prev 2005; 14: 1967–71.
86. Salaspuro M. P. Alcohol consumption and cancer of thegastrointestinal tract. Best Pract Res Clin Gastroenterol2003; 17: 679–94.
87. Väkeväinen S., Tillonen J., Salaspuro M. 4-Methylpyrazoledecreases salivary acetaldehyde levels in ALDH2-deficientsubjects but not in subjects with normal ALDH2. AlcoholClin Exp Res 2001; 25: 829–34.
88. Brennan P., Lewis S., Hashibe M., Bell D. A., Boffetta P.,Bouchardy C. et al. Pooled analysis of alcohol dehydroge-nase genotypes and head and neck cancer: a HuGE review.Am J Epidemiol 2004; 159: 1–16.
89. Yokoyama A., Tsutsumi E., Imazeki H., Suwa Y., Naka-mura C., Yokoyama T. Contribution of the alcoholdehydrogenase-1B genotype and oral microorganisms tohigh salivary acetaldehyde concentrations in Japanesealcoholic men. Int J Cancer 2007; 121: 1047–54.
90. Homann N., Stickel F., König I. R., Jacobs A., JunghannsK., Benesova M. et al. Alcohol dehydrogenase 1C*1 allele is
548 Dirk W. Lachenmeier et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550
a genetic marker for alcohol-associated cancer in heavydrinkers. Int J Cancer 2006; 118: 1998–2002.
91. Visapää J. P., Götte K., Benesova M., Li J., Homann N.,Conradt C. et al. Increased cancer risk in heavy drinkerswith the alcohol dehydrogenase 1C*1 allele, possibly dueto salivary acetaldehyde. Gut 2004; 53: 871–6.
92. Yang S. J., Wang H. Y., Li X. Q., Du H. Z., Zheng C. J., ChenH. G. et al. Genetic polymorphisms of ADH2 and ALDH2association with esophageal cancer risk in southwestChina. World J Gastroenterol 2007; 13: 5760–4.
93. Asakage T., Yokoyama A., Haneda T., Yamazaki M., MutoM., Yokoyama T. et al. Genetic polymorphisms of alcoholand aldehyde dehydrogenases, and drinking, smoking anddiet in Japanese men with oral and pharyngeal squamouscell carcinoma. Carcinogenesis 2007; 28: 865–74.
94. Scientific Committee on Cosmetic Products and Non-FoodProducts Intended for Consumers (SCCNFP). Opinion of theScientific Committee on Cosmetic Products and Non-FoodProducts intended for Consumers concerning Acetaldehyde.2004. Available at: http://ec.europa.eu/health/ph_risk/committees/sccp/documents/out275_en.pdf (accessed 5February 2009).
95. Rehm J., Room R., Taylor B. Method for moderation: mea-suring lifetime risk of alcohol-attributable mortality as abasis for drinking guidelines. Int J Methods Psychiatr Res2008; 17: 141–51.
96. Pelucchi C., Gallus S., Garavello W., Bosetti C., La V. C.Cancer risk associated with alcohol and tobacco use: focuson upper aero-digestive tract and liver. Alcohol Res Health2006; 29: 193–8.
97. Taylor B., Rehm J. When risk factors combine: the interac-tion between alcohol and smoking for aerodigestivecancer, coronary heart disease, and traffic and fire injury.Addict Behav 2006; 31: 1522–35.
98. Paton A. Alcohol in the body. BMJ 2005; 330: 85–7.99. Eriksson C. J., Fukunaga T. Human blood acetaldehyde
(update 1992). Alcohol Alcohol 1993; 2(Suppl): 9–25.100. Lagerlöf F., Dawes C. The volume of saliva in the
mouth before and after swallowing. J Dent Res 1984; 63:618–21.
101. Demchuk E., Ruiz P., Wilson J. D., Scinicariello F., Pohl H.R., Fay M. et al. Computational toxicology methods inpublic health practice. Toxicol Mech Methods 2008; 18:119–35.
102. Burdock G. A. Fenaroli’s Handbook of Flavour Ingredients,5th edn. Boca Raton, FL: CRC Press; 2004.
103. Mutsuga M., Kawamura Y., Sugita-Konishi Y., Hara-KudoY., Takatori K., Tanamoto K. Migration of formaldehydeand acetaldehyde into mineral water in polyethyleneterephthalate (PET) bottles. Food Addit Contam 2006; 23:212–18.
104. Choodum A., Thavarungkul P., Kanatharana P. Acetalde-hyde residue in polyethylene terephthalate (PET) bottles. JEnviron Sci Health B 2007; 42: 577–83.
105. Ho K. F., Lee S. C., Tsai W. Y. Carbonyl compounds in theroadside environment of Hong Kong. J Hazard Mater2006; 133: 24–9.
106. Bakeas E. B., Argyris D. I., Siskos P. A. Carbonyl com-pounds in the urban environment of Athens, Greece.Chemosphere 2003; 52: 805–13.
107. Clarisse B., Laurent A. M., Seta N., Le M. Y., El H. A.,Momas I. Indoor aldehydes: measurement of contamina-tion levels and identification of their determinants in Parisdwellings. Environ Res 2003; 92: 245–53.
108. Cavalcante R. M., Seyffert B. H., D’Oca M. G. M., Nasci-mento R. F., Campelo C. S., Pinto I. S. et al. Exposure assess-ment for formaldehyde and acetaldehyde in the workplace.Indoor Built Environ 2005; 14: 165–72.
109. Engelhaupt E. Clearing the air on ethanol. Environ SciTechnol 2007; 41: 3788.
110. Jacobson M. Z. Effects of ethanol (E85) versus gasolinevehicles on cancer and mortality in the United States.Environ Sci Technol 2007; 41: 4150–7.
111. Seeman J. I., Laffoon S. W., Kassman A. J. Evaluation ofrelationships between mainstream smoke acetaldehydeand ‘tar’ and carbon monoxide yields in tobacco smokeand reducing sugars in tobacco blends of U.S. commercialcigarettes. Inhal Toxicol 2003; 15: 373–95.
112. Seeman J. I., Dixon M., Haussmann H. J. Acetaldehyde inmainstream tobacco smoke: formation and occurrence insmoke and bioavailability in the smoker. Chem Res Toxicol2002; 15: 1331–50.
113. Nazaroff W. W., Singer B. C. Inhalation of hazardous airpollutants from environmental tobacco smoke in USresidences. J Expo Anal Environ Epidemiol 2004; 14: S71–S77.
114. Fowles J., Dybing E. Application of toxicological risk assess-ment principles to the chemical constituents of cigarettesmoke. Tob Control 2003; 12: 424–30.
115. National Health and Medical Research Council. NationalWater Quality Management Strategy: Australian DrinkingWater Guidelines 6. Canberra, Australia: National Healthand Medical Research Council; 2004. Available at:http://www.nhmrc.gov.au/publications/synopses/_files/adwg_11_06.pdf (5 February 2009).
116. Harrison K., Hoberg G. Risk Science and Politics: RegulatingToxic Substances in Canada and the United States. Montreal,Québec, Canada: McGill-Queens University Press; 1994.
117. Welsh M. Our smog is worse than we thought. Toronto Star2008; Saturday 6 December: A8 [see also: http://www.healthzone.ca/health/article/549457 (5 February 2009)]
118. Whate R., Mee C., White O., Macfarlane R., Belmont M.,Campbell M. Environmental Reporting, Disclosure and Inno-vation. A proposed program for the city of Toronto.Toronto, ON, Canada: Toronto Public Health; 2008.Available at: http://www.toronto.ca/health/hphe/pdf/technicalreportnov2008.pdf (5 February 2009)
119. Taylor B., Rehm J., Room R., Patra J., Bondy S. Determina-tion of lifetime injury mortality risk in Canada in 2002 bydrinking amount per occasion and number of occasions.Am J Epidemiol 2008; 168: 1119–25.
120. Barlow S., Renwick A. G., Kleiner J., Bridges J. W., Busk L.,Dybing E. et al. Risk assessment of substances that areboth genotoxic and carcinogenic. Report of an Interna-tional Conference organized by EFSA and WHO withsupport of ILSI Europe. Food Chem Toxicol 2006; 44:1636–50.
121. O’Brien J., Renwick A. G., Constable A., Dybing E., MüllerD. J., Schlatter J. et al. Approaches to the risk assessment ofgenotoxic carcinogens in food: a critical appraisal. FoodChem Toxicol 2006; 44: 1613–35.
122. Babor T., Caetano R., Casswell S., Edwards G., GiesbrechtN., Graham K. et al. Alcohol: No Ordinary Commodity.Research and Public Policy. Oxford and London: Oxford Uni-versity Press; 2003.
123. Rehm J., Greenfield T. K. Public alcohol policy: currentdirections and new opportunities. Clin Pharmacol Ther2008; 83: 640–3.
Risk assessment of acetaldehyde 549
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550

124. Codex Alimentarius. Codex General Standard for Con-taminants and Toxins in Foods (CODEX STAN 193-1995, Rev.1-1997). 1997. Available at: http://www.codexalimentarius.net (accessed 5 February 2009).
125. Council of the European Communities. Council Regula-tion (EEC) No 315/93 laying down Community proce-dures for contaminants in food. Off J Eur Comm 1993; L37:1–3.
550 Dirk W. Lachenmeier et al.
© 2009 The Authors. Journal compilation © 2009 Society for the Study of Addiction Addiction, 104, 533–550





























