Embed Size (px)
Citation preview
BL 9 Business Plan 2008-2013
Evidence for antimalarial policy and access
Draft Business Plan for JCB
May, 2007

Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 1
TABLE OF CONTENTS
EXECUTIVE SUMMARY .....................................................................................................2
1. OBJECTIVE ........................................................................................................................5
1.1. OVERALL OBJECTIVE................................................................................................5
1.2. SPECIFIC OBJECTIVES ...............................................................................................5
2. NEEDS AND OPPORTUNITIES ......................................................................................6
2.1. NEEDS............................................................................................................................6
2.2 OPPORTUNITIES...........................................................................................................7
3. COMPARATIVE ADVANTAGE ......................................................................................9
3.1 TDR COMPARATIVE ADVANTAGE ..........................................................................9
3.2 SYNERGIES WITH OTHER ORGANIZATIONS.......................................................10
4. ACTIVITIES AND END PRODUCTS............................................................................11
4.1 KEY ACTIVITIES.........................................................................................................11
4.2 END PRODUCTS..........................................................................................................14
4.3 INTERIM IMPLEMENTATION MILESTONES:........................................................15
4.4 INTERFACES WITH WHO/TDR RELATED ENTITIES ...........................................19
5. FUNDING...........................................................................................................................20
5.1 RESOURCE REQUIREMENTS ...................................................................................20
5.2 RATIONALE FOR RESOURCES REQUIRED ...........................................................20
6. RISKS..................................................................................................................................22

Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 2
EXECUTIVE SUMMARY
Needs and Opportunities
WHO estimates that malaria is responsible for over one million deaths per year. These deaths are avoidable using artemisinin-based combination therapies (ACTs), but most malarial fevers are not treated appropriately. Many patients seek treatment too late or do not reach public treatment facilities and obtain health care from the private or informal sector, where they often get inappropriate and poor quality treatment. If Millennium Development Targets 5, 8 and 17 (reducing childhood mortality, halt malaria and provide access to essential drugs) are to be met, there is an urgent need for research to complement existing malaria control policies and strategies through providing evidence for malaria treatment policy and for effective management of malaria at the community level. Several new antimalarial treatments are being developed and increased funds are being made available for DECs to deploy them. Countries need to make policy choices based on objective and comparative evidence on the safety and effectiveness of these antimalarial drugs, and to provide this evidence the different drugs need to be scientifically evaluated under real-life conditions. Research is also needed to determine the usefulness of diagnostics in different epidemiological settings, to improve diagnosis and treatment of malaria to community level and to determine effectiveness of integrated interventions against malaria and other childhood infections at the community level.
Overall Objective
To improve access to effective treatment for malaria and case-management of malaria and other childhood infections at all levels of the health system with the aim of reducing childhood mortality.
Specific Objectives
• To assess the safety and effectiveness of antimalarial drugs in "real-life" conditions of use, at different levels of the health care system, and in high-risk groups including pregnant women and persons infected with HIV;
• To develop a comprehensive package for the diagnosis and treatment of malaria episodes of various degrees of severity at the community level, determining its feasibility, acceptability, safety and cost-effectiveness;
• To develop an integrated diagnostic and treatment package to be delivered at the community level for the management of malaria and other childhood infections, and measure its impact to reduce mortality in children
Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 3
Activities
The studies to assess the safety and effectiveness of antimalarial drugs in real-life conditions of use will be undertaken by an international consortium, built around the INDEPTH network where the field studies will be undertaken. TDR will be responsible for independent scientific oversight of the studies, and other partner institutions will provide technical support in their area of expertise. The implementation research on home management of malaria and fever will be managed by TDR, and involve multicountry studies to develop and test the effectiveness and health impact of improved home treatment methods and strategies. These studies will be undertaken in close collaboration with national malaria control programs to ensure optimal relevance of the research.
End-Products
• A research framework for the generation of information on safety and effectiveness of antimalarial drugs in "real-life" conditions of use (2008)
• Independent and objective evidence on the safety and effectiveness of new antimalarial drugs in real-life conditions of use (starting 2009)
• A field-tested, community-accepted, safe and effective treatment package for malaria episodes of various degrees of severity at the community level (2010)
• Evidence of the impact of the comprehensive diagnostic and treatment package to reduce severe malaria morbidity and mortality (2012)
• Guidance on how to scale up coverage with an effective diagnostic and treatment package for malaria made available to policy makers by 2013
• Socially acceptable and operationally feasible treatment delivery model for prompt management of children with uncomplicated malaria, pneumonia and diarrhoea by community care providers (2009)
• Evidence on the impact of an integrated management package for malaria, pneumonia and diarrhoea at the community level on under-five mortality (2013)
Comparative Advantage
Over the last decade, TDR has been instrumental in developing strategies for community-level treatment of uncomplicated malaria episodes with oral drugs - it has conducted most of the original studies which led to the Home Management of Malaria strategy. TDR also undertook most of the studies that led to revised WHO recommendations for the treatment of malaria using ACTs. TDR has been instrumental in the development of several drugs against malaria such as Lapdap plus artesunate (in collaboration with MMV and GSK), rectal artesunate and the label extension of Coartem for paediatric use. It has experience in conducting post-registration studies, including multi-centre "Phase IV" trials and pharmacovigilance studies, and it has developed and refined a multicountry study model for

Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 4
this type of research. TDR is increasingly partnering in malaria research with research institutions and malaria control programmes, UN agencies (e.g. UNICEF), regulatory authorities, drug development agencies and other entities in affected African countries. By effectively combining research and capacity building, TDR has helped build a wide network of malaria researchers in Africa who can undertake the required research. TDR will work closely with WHO's Global Malaria Programme and the Roll Back Malaria Partnership to facilitate linkages between research and control.
Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 5
1. OBJECTIVE
1.1. OVERALL OBJECTIVE
To improve access to effective treatment for malaria and case-management of malaria and other childhood infections at all levels of the health system with the aim of reducing childhood mortality.
1.2. SPECIFIC OBJECTIVES
1. To assess the safety and effectiveness of antimalarial drugs in "real-life" conditions of use, at different levels of the health care system, and in high-risk groups including pregnant women and persons infected with HIV;
2. To develop a comprehensive package for the diagnosis and treatment of malaria episodes of various degrees of severity (from uncomplicated to severe) at the community level, determining its feasibility, acceptability, safety and cost-effectiveness;
3. To develop an integrated diagnostic and treatment package to be delivered at the community level for the management of malaria and other childhood infections, and measure its impact to reduce mortality in children

Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 6
2. NEEDS AND OPPORTUNITIES
2.1. NEEDS
Stalled progress in reducing under-five mortality in sub-Saharan Africa is mainly because of the failure to increase access to available effective and affordable tools. The over 1 million deaths from malaria that occur worldwide each year are avoidable, using artemisinin-based combination therapies (ACTs) and rapid diagnostic tests, but only 10% of fevers are treated appropriately. Where patients cannot reach public treatment facilities, self-medication is usual, but most fevers are treated inappropriately and the outcome of the infection depends on the efficacy of available drugs. The majority of children die before they reach the health services. Health facilities are often by-passed by communities, who seek health care from the private or informal sector, where they often get inappropriate and poor quality treatment. If Millennium Development Goals 5, 8 and 17 (reducing childhood mortality, halt malaria and other diseases incidence and provide access to essential drugs in developing countries) are to be met, there is an need for research to provide evidence for antimalarial treatment policy and scaling up of integrated management of malaria and other childhood fevers at the community level.
The negative economic and health consequences of inappropriate treatment policy decisions are obvious. Post-registration follow-up of antimalarials is scant and insufficiently developed (e.g. pharmacovigilance, pharmacoepidemiology, treatment adaptation, label extension). Some of the methodologies to obtain such information are available, but others will have to be developed or improved. Most malaria endemic countries in Africa, South America and Asia have made policy change to ACTs as first-line treatment for uncomplicated malaria, and the majority of countries have identified the regimens they wish to use. Because the available ACTs today are so limited, cost was the key factor in determining what choice countries made. Changes in antimalarial drug policy are expensive and time consuming. They represent an important challenge to Ministries of Health and the health system in general. Targeted research producing solid scientific evidence to inform malaria treatment policy decisions is therefore key to the translation of the new opportunities offered by the development of new and more efficacious drugs into a reduced malaria burden. Antimalarial drugs need to be tested broadly in the conditions of use to inform policy decisions and improve malaria management at the different levels of the health system.
Prompt assumption of effective antimalarial medicines is crucial in malaria treatment, as most severe and eventually fatal cases develop severe disease gradually and when treated late or inadequately, while only a minority of them develop life threatening signs ab initio. In most cases there is thus a window of a few hours/days when the progression of the disease can be stopped and the life of the patient saved, if effective malaria treatment is administered promptly. Furthermore, the possibility of diagnosing malaria infection through simple
Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 7
methods (rapid diagnostic tests, RDTs) is now available. However, there is still lack of clarity about their optimal conditions of use at the community level, and their usefulness in different epidemiological settings. It is thus imperative to give the possibility to children to be treated correctly as soon as possible, either at the first signs of uncomplicated disease or immediately when the first signs of severity appear. It is reckoned that at least 80% of malaria episodes seen at the community level may fall under these two categories, and a comprehensive diagnostic and treatment package for them needs to be developed.
Children living in rural areas of diseases endemic countries are often affected by a variety of infectious diseases, including malaria, pneumonia, gastro-intestinal infections and others. Most pneumonia episodes, killing a million children each year, are of bacterial origin, which can be effectively treated using inexpensive antibiotics that can be administered close to home; oral rehydration salts (ORS) for the treatment of diarrhoea are used for approximately 12% of cases only. Furthermore, the limited services which are community- or home-based are single disease, vertical and ineffective, and do not take into account the fact that children may be afflicted by multiple concurrent infections. Studies have shown that the limited impact of effective interventions is large due to low coverage of target populations, and that the community component of IMCI is not fully implemented. There is thus a need to develop new methods of strengthening care delivery at the community level, integrating treatment with effective medicines of the most common illnesses, and engaging the private sector in its various forms to develop delivery models that work both in public and private sectors in today’s pluralistic African health systems.
2.2 OPPORTUNITIES
Malaria-endemic countries are now faced with an unprecedented opportunity and challenge. Several highly effective antimalarial treatments are being developed and registered and increased funds are being made available for endemic countries to procure and deploy such antimalarials. The main and growing concern however is the significant delays in implementation in many countries. The recent creation of an international consortium built around the INDEPTH network, bringing together partners with solid scientific and operational competence such as the Swiss Tropical Institute, the London School of Hygiene and Tropical Medicine (LSHTM), the Centres for Disease Control, the University of Cape Town, WHO/AFRO and TDR represents an unique opportunity to produce the much needed solid scientific evidence to inform malaria treatment policy. If large scale implementation using the new efficacious ACTs does not take place soon, inefficacious antimalarials will continue to be used and lives will continue to be lost. On the other hand, if costly ACTs are deployed in the same manner as chloroquine and SP were used, resources will be wasted and there will be the potential risk of development of resistance. It is thus crucial to act quickly and develop a methodological framework to assess and compare effectiveness of antimalarial

Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 8
drugs under "real-life" conditions and make this available to all partners, particularly given the variety of actors with different degrees of expertise who are now involved in this research area. This information is urgently needed as countries are faced with the problem now and it will be difficult, expensive and time consuming to reverse inadequate policy decisions.
Increased funds have become available for malaria control and research in recent years, through multilateral and bilateral institutions. A number of new partners have entered the playing field, such as the Bill & Melinda Gates Foundation, the Global Fund to Fight Aids, Tuberculosis and Malaria, various NGOs, such as MMV and DNDi, and consortia. There is also a general recognition of two fundamental issues: the need to expand research beyond the moment of the registration of an antimalarial medicine, and the need to develop new, sustainable and integrated delivery strategies for treatment of malaria and other childhood infections at the community level. This business line's aim is to draw advantage from the unprecedented opportunity that the current momentum in malaria control and research is offering to have a major impact on the burden imposed by a curable disease.

Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 9
3. COMPARATIVE ADVANTAGE
3.1 TDR COMPARATIVE ADVANTAGE
TDR is uniquely situated to coordinate this important effort. It has few but adequately qualified personnel with experience in effectiveness and implementation research, including social science, policy and health systems research. TDR avails itself of the scientific guidance of the world's leading researchers in these different fields. TDR has networks and links with scientists, including TDR trainees, developers (public, private not-for-profit, for profit), academic research groups, and control programmes. TDR is thus in a position to provide rigorous scientific stewardship in all research areas covered by the business line.
TDR has been instrumental in developing in the last decade strategies for prompt, community-level treatment of uncomplicated malaria episodes with oral drugs - it has conducted most of the original studies which led to the development of the Home Management of Malaria strategy - and more severe stages of malaria (patients unable to take oral drugs) with artesunate suppositories (RA), administered as pre-referral treatment. Both strategies have been field-tested extensively and shown to reduce mortality and progression towards more severe forms of malaria disease. Only TDR has the expertise in house to combine these two strategies and develop a comprehensive diagnostic and treatment package that will cater for the majority of malaria episodes occurring at the community level.
Furthermore, TDR has also accumulated experience in identifying critical public health issues and conducting the relevant research in close interaction with policy makers and translating research results into policy. The studies on ACTs that have lead to revised WHO recommendations for the treatment of malaria are a good example. At the same time, TDR has the ability to understand the issues of product development. Over the last five years TDR has been instrumental in the development of several drugs against malaria and other tropical diseases, such as Lapdap and CDA (in collaboration with MMV and GSK), rectal artesunate, the label extension of Coartem for paediatric use, miltefosine for leishmaniasis and praziquantel for schistosomiasis. TDR has experience in post-registration studies, including multi-centre "Phase IV" trials and pharmacovigilance studies, and has carried out many systematic reviews and meta-analysis, using the results to obtain consensus opinion on controversial issues. TDR also has experience in leading large community-based intervention studies. It has been instrumental in the development of community-based disease control strategies, which are currently fundamental elements of policy, such as malaria home management and community directed treatment for onchocerciasis.
Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 10
3.2 SYNERGIES WITH OTHER ORGANIZATIONS
TDR, as part of WHO, can work closely in a coordinated fashion with other WHO departments involved in malaria control (e.g. GMP, CAH, PSM, AFRO), UN agencies (e.g. UNICEF), research institutions and malaria control programmes in disease endemic countries, regulatory authorities, drug development agencies and various other partners. In the consortium to evaluate new antimalarials in real life conditions of use TDR will, in a synergistic action with the other consortium partners ensuring technical or operational support to the field sites, play an essential role in ensuring independent scientific coordination and stewardship. TDR is also part of a consortium (headed by the London School of Hygiene and Tropical Medicine) promoting research on the use of ACTs at the community level and itself coordinates a consortium to develop integrated, community-level management packages for childhood infections. The latter comprises research institutions located in the South and in the North (Karolinska Institute, Sweden, the WHO/Child and Adolescent Health department and Global Malaria Programme, Makerere University in Uganda, the Health Research Unit in Ghana and the CNRFP in Burkina Faso, UNICEF and USAID), all of whom are interested in child survival and have research expertise both in malaria and pneumonia, and in community-based interventions.
TDR will be able to build on already initiated activities in numerous African countries. Studies are ongoing to establish the feasibility, acceptability, and effectiveness of the use of ACTs at the community level. A study has been initiated to measure the impact of community-level deployment of ACTs on children Under 5 mortality. Exploratory studies are ongoing for testing strategies for deploying ACTs at the community level in continuously growing urban and semi-urban populations in sub-Saharan Africa. Pilot studies on the use of RDTs at the community level to optimize deployment of ACTs and guide treatment for malaria and other febrile illnesses have been initiated in four countries, and two studies are ongoing to develop the strategy for integrated management of malaria and pneumonia at the community level. Finally, a Pregnancy Register, monitoring maternal outcomes, birth outcomes, child development and perinatal mortality in women exposed to Coartem or Sulphadoxine-pyrimethamine (SP) has been initiated in Zambia.
Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 11
4. ACTIVITIES AND END PRODUCTS
4.1 KEY ACTIVITIES
Objective 1
• Ensure independent scientific oversight and monitoring of studies to assess safety and effectiveness of antimalarial drugs in real-life conditions of use. The studies will be sponsored by an international consortium, built around the INDEPTH network, where the field studies will be undertaken. TDR will also collaborate with other consortium members to develop protocols for safety and effectiveness measurement.
• 2008: The consortium will consult with key stakeholders in malaria treatment policy and implementation, including national health policy makers, regulatory bodies, drug manufacturers and WHO, to discuss the draft evaluation framework and whether this meets their needs for evidence on new antimalarials. These consultations will allow further optimization of the evaluation framework on the basis of the feedback from the stakeholders, and to reach a broad consensus on the parameters to be included and the information to be collected in the phase IV studies.
• 2008-2010: TDR will provide independent scientific oversight of studies to assess programmatic effectiveness when drugs are used in the general population at different levels of the health system, including the community level, and using different distribution channels, such as health personnel, trained community members, private sector operators. As part of the research an appropriate methodology will be developed for drug evaluation; some studies will concern specific sub-populations (e.g. safe and efficacious alternatives to SP in the intermittent preventive treatment of pregnant women, people co-infected with HIV). Field protocols and training approaches will be developed for measuring effectiveness and monitoring safety of antimalarial drugs. This will include monitoring indicators that will describe and characterize the performance and reach of the local district health system to allow meaningful comparisons across sites and countries and help explain where losses of efficacy (i.e. effectiveness) occur. The implementation research on home management of malaria and fever will be managed by TDR, and involve multicountry studies to develop and test the effectiveness and health impact of improved home treatment methods and strategies. These studies will be undertaken in close collaboration with national malaria control programs to ensure optimal relevance of the research.
• 2008-2012: Studies will develop and field-test innovative approaches to improve adherence, ensure pharmacovigilance and pharmacoepidemiology adapted to the
Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 12
conditions of use (within and outside the health sector, including communities) and suited to resource-constrained settings. Social science research will contribute to better understanding factors contributing to adherence to therapy
• 2010-2013: Studies will assess programmatic effectiveness of new antimalarial drugs that will become available in future years
• every year: provide information to policy makers on the safety and effectiveness of antimalarial drugs in "real-life" conditions of use.
Objective 2
• 2008-2009: Complete studies to produce evidence on the use of ACTs and RDTs at the community level in various epidemiological and socio-cultural and socio-economic settings, thus contributing to expanding access to effective treatment by target populations;
• 2008-2010: Funding research grants to develop a comprehensive diagnostic and treatment package for malaria episodes of various degrees of severity (from uncomplicated malaria with oral ACTs to severe malaria with rectal artesunate) at the community level. The studies will develop approaches for optimal delivery of RDTs, ACTs and RA at the community level and determine the potential contribution of various categories of actors, in particular from the informal private sector, in the implementation of the package. Studies will see that strong links between the community and the health facilities of reference are created and maintained to ensure appropriate case management of the most severe cases and overall supervision. Furthermore, they will develop community-level surveillance systems for monitoring adverse events and the possible development of drug resistance.
• 2009-2013: Funding research grants to determine the large-scale impact and thus the cost-effectiveness of the comprehensive diagnostic and treatment package to reduce severe malaria morbidity, mortality and sequelae. This will be accomplished through studies carried out in association with large scale implementation programmes;
• 2011-2013: Studies will be funded in which diagnostic and treatment packages for malaria (uncomplicated+severe) and other childhood infections (see objective 3 below) are merged, and the impact of comprehensive packages is assessed.
• 2010-2013: Funding research grants to incorporate new ACTs and RDTs in the package as they become available;
• every year: provide information to policy makers on the results of the studies and provide guidance on how to scale up coverage with an effective diagnostic and treatment package for malaria.
Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 13
Objective 3
• 2008-2010: Complete studies to develop an integrated diagnostic and treatment package for the management of malaria, pneumonia and diarrhoea in children at the community level and determine, through a community based vital statistics monitoring system, its impact and cost-effectiveness on under-five mortality
• 2008-2010: Funding research grants to develop community-level surveillance systems for monitoring adverse events and the possible development of drug resistance;
• 2011-2013: As mentioned under Objective 2.4, activities under Objective 3 will merge with Objective 2 as from 2011. Studies will be funded in which diagnostic and treatment packages for malaria (uncomplicated + severe) and other childhood infections are implemented together on a large scale, and the impact of comprehensive packages will be established.
• every year: provide information to policy makers on the results of the studies and provide guidance on how to scale up coverage with an effective diagnostic and treatment package for malaria and other childhood infections.
All studies funded will integrate a solid capacity building component to enable continuing generation of data at the national level. They will put emphasis on strengthening community participation with the aim to ensure ownership of malaria control activities by communities, link malaria control with other development activities and facilitate community based financing initiatives to ensure sustainability of activities. Studies will utilize a mix of large-scale community-based, randomized trials and before-and-after interventional studies, including demographic surveillance and cost analysis. The study sites will cover settings with different intensities of malaria transmission, healthcare infrastructure and socio-economic development. In some countries pilot activities are ongoing; they will provide crucial information for the development of the intervention strategy to be tested in large-scale studies. The ultimate goal of all research activities sponsored under the business line is to increase access by target populations (mainly children and pregnant women) leaving in remote areas of malaria-endemic countries to prompt and effective treatment.
Gender
Gender issues and differentials affect, to a large extent, access to and uptake of malaria-related interventions at the community level. Therefore, research activities of this business line will systematically address the effects of gender differentials in the planning and implementation process at the community level, and define gender-sensitive malaria interventions. The core concept of community-level treatment of malaria and other acute childhood infections, which is adopted and will be further developed in this business line, places emphasis on the mothers' responsibility as the first and principal providers of care for the children, in recognition of their role in society. Their is the decision to treat the sick child, while the member of the community who holds the drugs is instructed to deliver treatments

Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 14
upon their request, provided the child does not need referral. Training material and drug packaging will be thus designed to specifically help mothers, in particular illiterate mothers, to treat correctly their children. Furthermore, with regard to the selection of the members of the community who will hold the drugs, this research will include a detailed analysis of the role of gender in the decision process, and to what extent a reinforcement of the role of women within the context of the prevailing social cultural environment would strengthen intervention delivery and its sustainability. In order to address these gender research needs, the BL's Scientific Advisory Committee will need expertise in social science research, including gender. Particular attention will be paid to gender balance in the composition of the business line's Scientific Advisory Committee. The committee will also annually review the gender-specific research activities and findings, synthesize the main findings for sharing with other business lines and reporting to STAC, and advise on the future direction of gender related research of the business line.
4.2 END PRODUCTS
Objective 1:
• A research framework for the generation of information on safety and effectiveness of antimalarial drugs in real-life conditions of use developed by 2008;
• Methodological guidelines to assess programmatic effectiveness of antimalarials used at different levels of the health system and in specific sub-populations to inform policy makers developed by 2010;
• Independent and objective evidence on the safety and effectiveness of new antimalarial drugs in real-life conditions of use made available to policy makers within 1-2 years after drug registration;
• A document describing field-tested, innovative approaches to assess adherence to and ensure pharmacovigilance and pharmacoepidemiology of antimalarials disseminated to partners in malaria control by 2012;
Objective 2:
• A field-tested, community-accepted, safe and effective treatment package for malaria episodes of various degrees of severity to be implemented at the community level developed and disseminated to partners in malaria control by 2010;
• Evidence on the safety of the treatment package and on its effect on the development of resistance to antimalarial drugs produced and disseminated to partners in malaria control by 2010;
Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 15
• Evidence of the impact of the comprehensive diagnostic and treatment package to reduce severe malaria morbidity and mortality produced and disseminated to partners in malaria control by 2012;
• Guidance on how to scale up coverage with an effective diagnostic and treatment package for malaria made available to policy makers by 2013;
Objective 3:
• A socially acceptable and operationally feasible treatment delivery model for involving a variety of community care providers in the prompt management of children with uncomplicated malaria, pneumonia and diarrhoea produced and disseminated to partners by 2009;
• Guidance on how to establish community-level surveillance systems for monitoring adverse events and the possible development of drug resistance developed and disseminated to partners by 2010;
• Evidence on the impact of an integrated management package for malaria, pneumonia and diarrhoea in children at the community level on under-five mortality produced and disseminated to partners by 2013
4.3 INTERIM IMPLEMENTATION MILESTONES:
Objective 1:
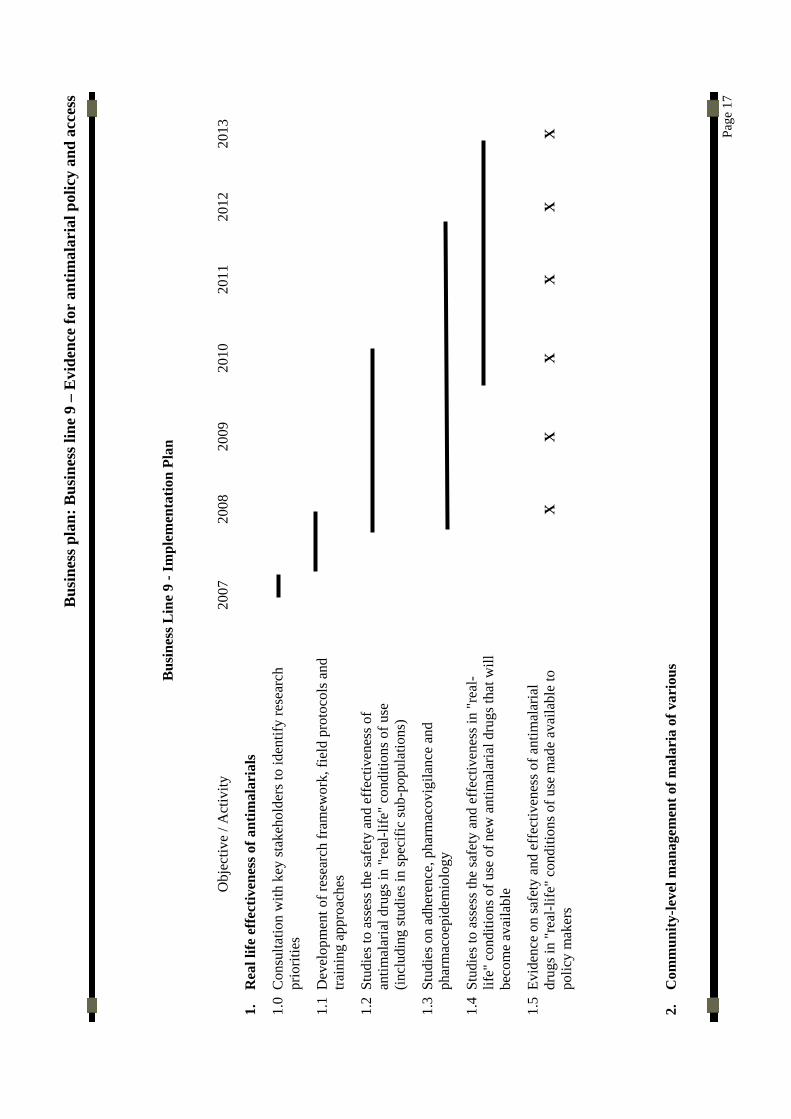
A meeting with key stakeholders and relevant departments in WHO to identify research priorities for optimizing malaria treatment at all levels of care convened by 2007; field protocols and training approaches for measuring effectiveness and safety of antimalarial drugs by developed by 2007 as part of the consortium activities; studies on programmatic effectiveness and on innovative approaches to assess adherence, ensure pharmacovigilance and pharmacoepidemiology funded and ongoing by 2008; studies to identify best treatment options in specific sub-populations (e.g. as part of IPTp or in persons co-infected with HIV will be funded and ongoing by 2008; final reports from studies on programmatic effectiveness are expected by 2010; final reports from studies on innovative approaches received by 2012; studies on programmatic effectiveness of newly developed antimalarials will be funded by 2010; final reports from studies on programmatic effectiveness of new antimalarials received by 2013.

Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 16
Objective 2:
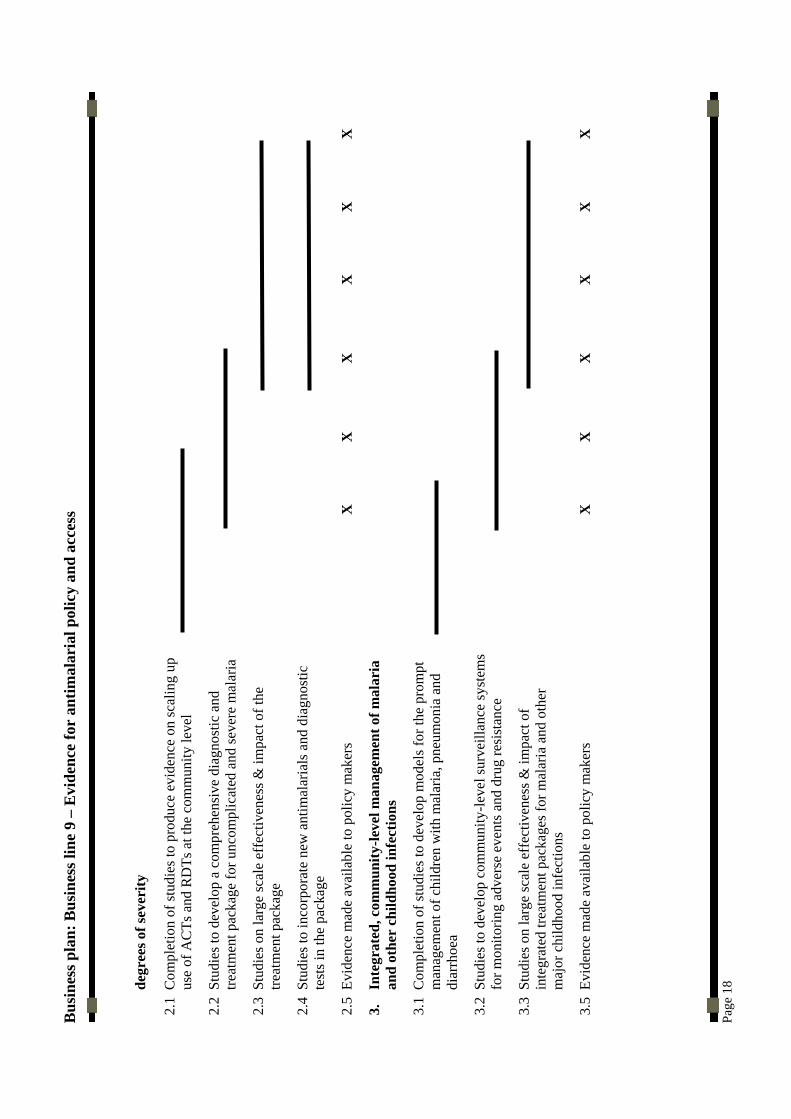
Relevant call for applications published by 2007; proposal development workshops held by June 2008; at least 3 implementation research grants to develop the treatment package for malaria of various degrees of severity, including safety and monitoring of resistance, issued by 2008; studies to produce conclusive evidence on scaling up use of ACTs at the community level completed by mid 2009; studies completed and results available by early 2010; at least 3 implementation research grants to determine the impact and cost-effectiveness of the treatment package issued by the end of 2009-2010; studies completed and results available by 2013.
Objective 3:
Studies to develop treatment delivery models for the management of children with uncomplicated malaria, pneumonia and diarrhoea completed by 2008; Relevant call for applications for large scale impact studies published by 2007; proposal development workshops as appropriate held by June 2008; at least 2 studies to develop community-level surveillance systems for monitoring adverse events and the possible development of drug resistance funded by 2008; studies completed and results available by early 2010; at least 3 studies to determine the impact and cost-effectiveness of the integrated management package for malaria, pneumonia and diarrhoea funded by 2009; studies completed and results available by 2013.
Bus
ines
s pla
n: B
usin
ess l
ine
9 –
Evi
denc
e fo
r an
timal
aria
l pol
icy
and
acce
ss
Pa
ge 1
7
B
usin
ess L
ine
9 - I
mpl
emen
tatio
n Pl
an
Obj
ectiv
e / A
ctiv
ity
2007
20
08
2009
20
10
2011
20
12
2013
1.
Rea
l life
eff
ectiv
enes
s of a
ntim
alar
ials
1.0
Con
sulta
tion
with
key
stak
ehol
ders
to id
entif
y re
sear
ch
prio
ritie
s
1.1
Dev
elop
men
t of r
esea
rch
fram
ewor
k, fi
eld
prot
ocol
s and
tra
inin
g ap
proa
ches
1.2
Stud
ies t
o as
sess
the
safe
ty a
nd e
ffec
tiven
ess o
f an
timal
aria
l dru
gs in
"re
al-li
fe"
cond
ition
s of u
se
(incl
udin
g st
udie
s in
spec
ific
sub-
popu
latio
ns)
1.3
Stud
ies o
n ad
here
nce,
pha
rmac
ovig
ilanc
e an
d ph
arm
acoe
pide
mio
logy
1.4
Stud
ies t
o as
sess
the
safe
ty a
nd e
ffec
tiven
ess i
n "r
eal-
life"
con
ditio
ns o
f use
of n
ew a
ntim
alar
ial d
rugs
that
will
be
com
e av
aila
ble
1.5
Evid
ence
on
safe
ty a
nd e
ffec
tiven
ess o
f ant
imal
aria
l dr
ugs i
n "r
eal-l
ife"
cond
ition
s of u
se m
ade
avai
labl
e to
po
licy
mak
ers
X
X
X
X
X
X
2.
Com
mun
ity-le
vel m
anag
emen
t of m
alar
ia o
f var
ious
Bus
ines
s pla
n: B
usin
ess l
ine
9 –
Evi
denc
e fo
r an
timal
aria
l pol
icy
and
acce
ss
Pa
ge 1
8 degr
ees o
f sev
erity
2.1
Com
plet
ion
of st
udie
s to
prod
uce
evid
ence
on
scal
ing
up
use
of A
CTs
and
RD
Ts a
t the
com
mun
ity le
vel
2.2
Stud
ies t
o de
velo
p a
com
preh
ensi
ve d
iagn
ostic
and
tre
atm
ent p
acka
ge fo
r unc
ompl
icat
ed a
nd se
vere
mal
aria
2.3
Stud
ies o
n la
rge
scal
e ef
fect
iven
ess &
impa
ct o
f the
tre
atm
ent p
acka
ge
2.4
Stud
ies t
o in
corp
orat
e ne
w a
ntim
alar
ials
and
dia
gnos
tic
test
s in
the
pack
age
2.5
Evid
ence
mad
e av
aila
ble
to p
olic
y m
aker
s
X
X
X
X
X
X
3.
Inte
grat
ed, c
omm
unity
-leve
l man
agem
ent o
f mal
aria
an
d ot
her
child
hood
infe
ctio
ns
3.1
Com
plet
ion
of st
udie
s to
deve
lop
mod
els f
or th
e pr
ompt
m
anag
emen
t of c
hild
ren
with
mal
aria
, pne
umon
ia a
nd
diar
rhoe
a
3.2
Stud
ies t
o de
velo
p co
mm
unity
-leve
l sur
veill
ance
syst
ems
for m
onito
ring
adve
rse
even
ts a
nd d
rug
resi
stan
ce
3.3
Stud
ies o
n la
rge
scal
e ef
fect
iven
ess &
impa
ct o
f in
tegr
ated
trea
tmen
t pac
kage
s for
mal
aria
and
oth
er
maj
or c
hild
hood
infe
ctio
ns
3.5
Evid
ence
mad
e av
aila
ble
to p
olic
y m
aker
s
X
X
X
X
X
X
Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 19
4.4 INTERFACES WITH WHO/TDR RELATED ENTITIES
Objective 1:
All activities will be planned and implemented in close collaboration with the Global Malaria Programme (GMP). Additional technical advice will be sought from the departments of Policy Access and Rational Use (PSM/PAR) and Technical Cooperation for Essential Drugs and Traditional Medicine (TCM); the Regional Office for Africa (AFRO) will be a key partner in the implementation. As described earlier, TDR will implement research activities related to objective 1 as a member of a specific consortium (see 3.2); collaborations will be also sought with MMV and DNDi.
Objective 2:
Collaboration both with GMP and AFRO will be key in all steps of the implementation plan.
Objective 3:
Activities will be planned and implemented in collaboration with GMP and the Child and Adolescent Health department (CAH). Outside WHO, UNICEF will be a key partner.
Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 20
5. FUNDING
5.1 RESOURCE REQUIREMENTS
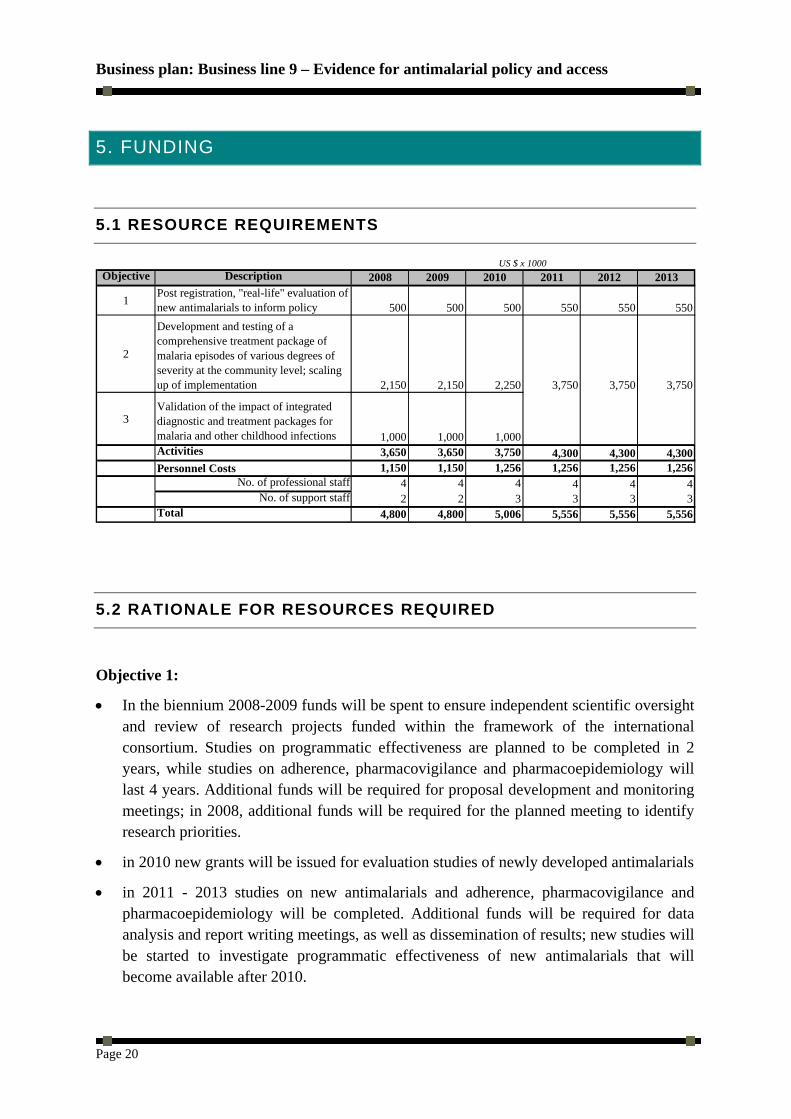
US $ x 1000Objective Description 2008 2009 2010 2011 2012 2013
1Post registration, "real-life" evaluation of new antimalarials to inform policy 500 500 500 550 550 550
2
Development and testing of a comprehensive treatment package of malaria episodes of various degrees of severity at the community level; scaling up of implementation 2,150 2,150 2,250 3,750 3,750 3,750
3Validation of the impact of integrated diagnostic and treatment packages for malaria and other childhood infections 1,000 1,000 1,000Activities 3,650 3,650 3,750 4,300 4,300 4,300Personnel Costs 1,150 1,150 1,256 1,256 1,256 1,256
No. of professional staff 4 4 4 4 4 4No. of support staff 2 2 3 3 3 3
Total 4,800 4,800 5,006 5,556 5,556 5,556
5.2 RATIONALE FOR RESOURCES REQUIRED
Objective 1:
• In the biennium 2008-2009 funds will be spent to ensure independent scientific oversight and review of research projects funded within the framework of the international consortium. Studies on programmatic effectiveness are planned to be completed in 2 years, while studies on adherence, pharmacovigilance and pharmacoepidemiology will last 4 years. Additional funds will be required for proposal development and monitoring meetings; in 2008, additional funds will be required for the planned meeting to identify research priorities.
• in 2010 new grants will be issued for evaluation studies of newly developed antimalarials
• in 2011 - 2013 studies on new antimalarials and adherence, pharmacovigilance and pharmacoepidemiology will be completed. Additional funds will be required for data analysis and report writing meetings, as well as dissemination of results; new studies will be started to investigate programmatic effectiveness of new antimalarials that will become available after 2010.
Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 21
Objective 2:
• In the biennium 2008-2009 funds will be required to a) complete and scale up ongoing studies on expanding access to ACTs at the community level; b) to initiate studies to develop the integrated treatment package for malaria of various degrees of severity, including safety and monitoring of resistance; it is foreseen that 1 study on the impact of the integrated package could start in 2009.
• in the biennium 2010-2011, funds will be required to launch at least 3 additional large scale trials to assess the impact of the integrated package for malaria treatment and to address issues related to scaling up of implementation, including incorporation of newly developed antimalarials that may become available; the budget includes salaries for full time personnel to be appointed in countries to ensure field coordination of the studies.
• in the biennium 2012-2013, large scale implementation research studies will be funded to produce conclusive evidence on the public health impact of the treatment package, and of integrated treatment packages incorporating malaria of various degrees of severity (developed under work package N.2) and other major childhood infections (developed under work package N.3).
Objective 3:
• Until 2008 funds will be required to complete ongoing studies to develop and pre-test an integrated management package for malaria and other childhood infections at the community level.
• in the biennium 2010-2011, other implementation research studies will be funded for multiple site evaluation of the intervention package and/or incorporation of new medicines or diagnostics.
• in the years 2011-2013 the treatment package will be expanded to cover additional childhood infections (e.g. intestinal parasites, other neglected diseases) and to establish the impact of integrated treatment packages incorporating malaria of various degrees of severity (developed under objective 2) and other major childhood infections (developed under objective N.3); the budget includes salaries for full time personnel to be appointed in countries to ensure field coordination of the studies.

Business plan: Business line 9 – Evidence for antimalarial policy and access
Page 22
6. RISKS
Most activities can be started now. TDR has in its current portfolio projects falling into this BL; new activities can be staggered. The implementation plan provides for engaging stakeholders early in the course of planning.
Many of the issues being addressed by research in this business line are pressing and require rapid answers; both countries and donors need quick results. However, there is a risk related to the complexity of the environment and of players involved in the research. TDR, as a research coordinating programme, is not carrying out research studies itself, and this could lead to studies not being done properly. The challenge for this business line is to foster quickly the generation of data to inform community-based malaria control policy. It will fail if speedy and high quality delivery cannot be achieved. Therefore, bureaucratic, administrative and managerial huddles that slow down TDR`s speed of implementation must be minimized or eliminated.
There is an understandable lag time between initiating research and producing research results but all technical and other support should be provided to projects to minimize this time lag. Time lines and milestones must be closely monitored and go-no-go decisions taken in time. To be relevant, these activities should start or be scale-up very soon and research should be conducted within the context of country programmes and as a concerted effort with relevant stakeholders. This business line will fail if true partnerships cannot be developed. The credibility and legitimacy of this business line will be jeopardized if TDR fails to operate as a honest broker between all sectors and organizations involved.





























