Embed Size (px)
Citation preview
Autonomic Nervous SystemTesting
A utonomic nervous system testingis used to document diabetic au-tonomic failure. Diabetic auto-
nomic failure is defined as impairedfunction of the peripheral autonomicnervous system and can be divided intotwo categories: 1) autonomic neuropa-thy, in which there is a structural lesionof the peripheral autonomic neuron and2) functional autonomic failure, in whichno known structural lesion occurs. Inaddition to the classic neurotransmitters(acetylcholine and norepinephrine),newer neurotransmitters and neuromod-ulators such as substance P, neuropep-tide K, calcitonin gene-related peptide,and nitric oxide are also involved. Also,the adrenal medullae are an integral partof the autonomic nervous system. Withthese caveats, the following definition isproposed, wherein autonomic abnormal-ities are classified as structural or func-tional with further subdivisions based onthe overt or subclinical nature of the dis-order, the specific subdivisions of theautonomic nervous system, and the spe-cific organ systems involved.
AUTONOMIC NEUROPATHY INDIABETES — In the setting of diabetesmellitus without other causes of auto-nomic neuropathy there is a structurallesion that comprises a diffuse disorderof small nerve fibers of the cholinergic,adrenergic, and peptidergic nervous sys-tems. This may be further divided into:1) subclinical—that which is diagnosedonly by tests and 2) clinical—that whichpresents with symptoms or signs.
FUNCTIONAL AUTONOMICFAILURE IN DIABETES— Reducedautonomic responses not attributable toclassic diabetic autonomic neuropathyalso occur and cause clinically importantproblems. An example is hypoglycemia-associated autonomic failure (HAAF;1,2). HAAF is a recently described func-tional disorder without a known struc-tural lesion characterized by selectivelyreduced adrenomedullary (epinephrine)and parasympathetic (pancreatic poly-peptide) responses to a given degree ofhypoglycemia. It is associated with theinterrelated clinical syndromes of defec-tive glucose counterregulation, hypogly-cemia unawareness, and elevated glyce-mic thresholds for symptoms of andautonomic responses to hypoglycemiaduring effective intensive therapy, andwith a high frequency of iatrogenic hy-poglycemia. A further example of func-tional autonomic failure is the impair-ment of gastric emptying with severehyperglycemia (3).
TESTS OF AUTONOMICFUNCTION — The autonomic nervoussystem is usually tested by evaluatingreflex arcs. A reflex arc involves a stim-ulus, a receptor, an afferent nerve, centralprocessing, an efferent nerve and an end-organ response. In addition to the reflexarc, there are several synapses involvedthroughout the pathway and differentneurotransmitters at each synaptic cleft.It is important that, where possible, theconfounding variables, standardizationof stimulus, and normal end-organ func-
ADDRESS CORRESPONDENCE AND REPRINT REQUESTS TO DR. RICHARD KAHN, AMERICAN DIABETES ASSO-
CIATION, 1660 DUKE STREET, ALEXANDRIA, VA 22314.
THIS MATERIAL IS BEING PUBLISHED SIMULTANEOUSLY IN NEUROLOGY AND MUSCLE AND NERVE.
tion be established before one elicits thereflex arc to test the autonomic nervoussystem.
Many organs are dually inner-vated. Innervation of parasympatheticand sympathetic pathways often work asa check and balance system. Therefore,where possible, the autonomic nervoussystem needs to be evaluated recognizingthat the result may reflect a decrease inone pathway or an increase in another.
An ideal test should be simple,noninvasive, easy for the operator andsubjects, reproducible, sensitive, relevantto known physiological functions, suit-able for longitudinal evaluation, and spe-cific. The confounding variables affectingthe test should be fairly well delineated.Some of the current autonomic tests ful-fill nearly all of these obligations.
Standardization of testingTo reduce great variability in assessingthe autonomic nervous system, it is im-portant to standardize the test wherepossible. It is known that eating, drink-ing coffee, smoking, volume status, up-right posture, medicines, and exercisemay affect the cardiovascular autonomicnervous system and, presumably, otherautonomic nervous organ systems.Therefore, in an ideal situation, studiesshould be performed with the patienthaving had no acute illness for the pre-ceding 48 h; unaccustomed vigorous ex-ercise for 24 h, anticholinergic drugs (in-cluding antidepressants), antihistaminesand over-the-counter cough and coldmedications, 9 -a-fluorohydrocortisone,diuretics, sympathomimetic and para-sympathomimetic medications, and aspi-rin for 18 h; alcohol or hypoglycemicepisodes for 12 h; or food, caffeine, ortobacco products for 8 h. Moreover, thestudies should be performed in themorning in a quiet relaxed atmosphere.The patient should have been taught andpracticed the procedure, and at the timeof the study should not be wearing com-pressive clothing or Jobst stockings,should have the blood glucose stabilized
DIABETES CARE, VOLUME 15, SUPPLEMENT 3, AUGUST 1992 1095
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/15/8/1095/441790/15-8-1095.pdf by guest on 07 July 2022
Autonomic nervous system testing
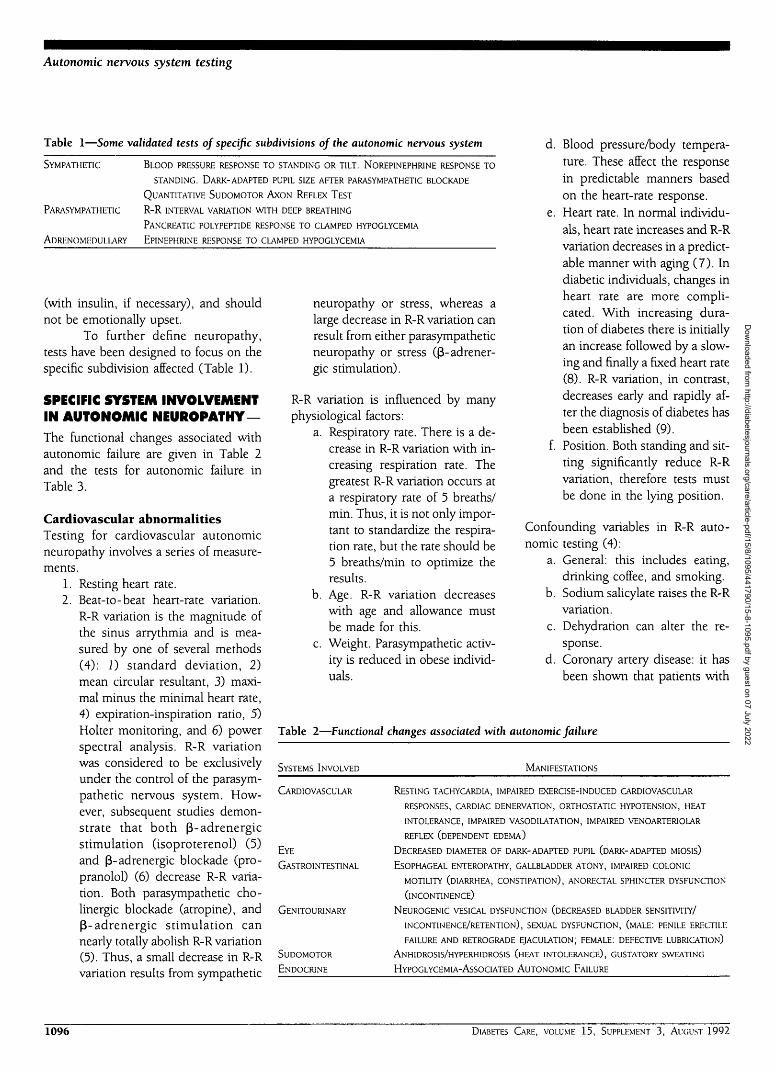
Table 1—Some validated tests of specific subdivisions of the autonomic nervous system
SYMPATHETIC BLOOD PRESSURE RESPONSE TO STANDING OR TILT. NOREPINEPHRINE RESPONSE TO
STANDING. DARK-ADAPTED PUPIL SIZE AFTER PARASYMPATHET1C BLOCKADE
QUANTITATIVE SUDOMOTOR AXON REFLEX TEST
PARASYMPATHETIC R-R INTERVAL VARIATION WITH DEEP BREATHING
PANCREATIC POLYPEPTIDE RESPONSE TO CLAMPED HYPOGLYCEMIA
A D R E N O M E D U L L A R Y EPINEPHRINE RESPONSE TO CLAMPED HYPOGLYCEMIA
(with insulin, if necessary), and shouldnot be emotionally upset.
To further define neuropathy,tests have been designed to focus on thespecific subdivision affected (Table 1).
SPECIFIC SYSTEM INVOLVEMENTIN AUTONOMIC NEUROPATHY—
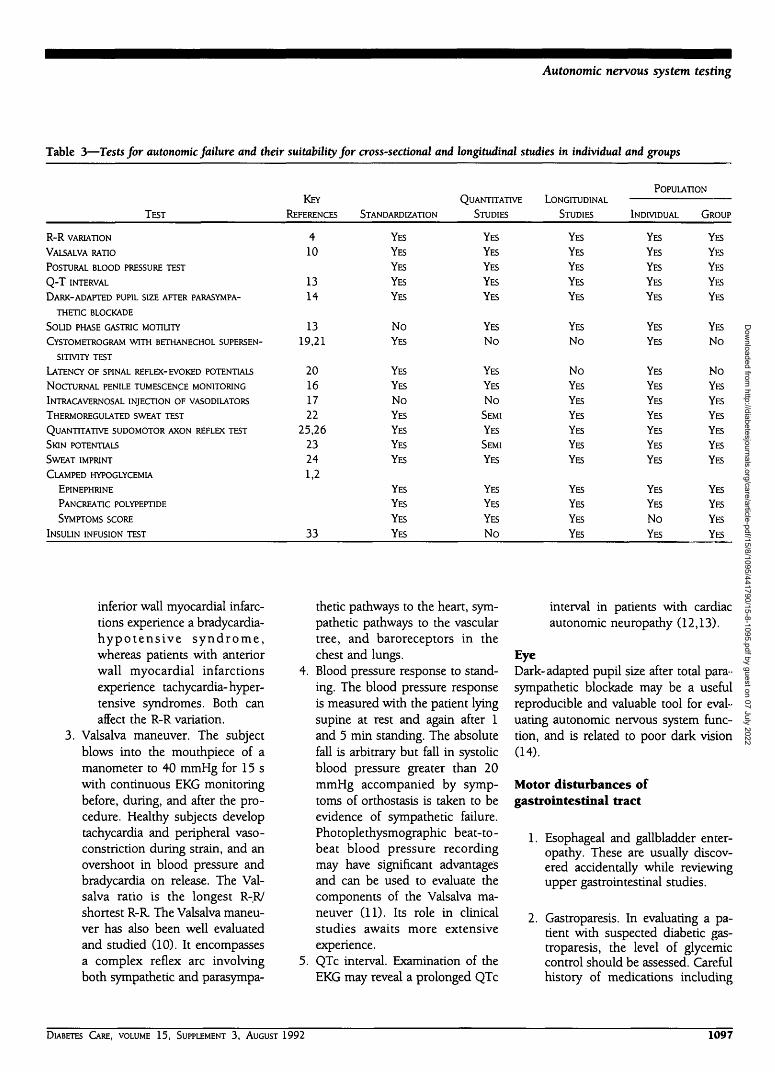
The functional changes associated withautonomic failure are given in Table 2and the tests for autonomic failure inTable 3.
Cardiovascular abnormalitiesTesting for cardiovascular autonomicneuropathy involves a series of measure-ments.
1. Resting heart rate.2. Beat-to-beat heart-rate variation.
R-R variation is the magnitude ofthe sinus arrythmia and is mea-sured by one of several methods(4): 1) standard deviation, 2)mean circular resultant, 3) maxi-mal minus the minimal heart rate,4) expiration-inspiration ratio, 5)Holter monitoring, and 6) powerspectral analysis. R-R variationwas considered to be exclusivelyunder the control of the parasym-pathetic nervous system. How-ever, subsequent studies demon-strate that both P-adrenergicstimulation (isoproterenol) (5)and 0-adrenergic blockade (pro-pranolol) (6) decrease R-R varia-tion. Both parasympathetic cho-linergic blockade (atropine), and(3-adrenergic stimulation cannearly totally abolish R-R variation(5). Thus, a small decrease in R-Rvariation results from sympathetic
neuropathy or stress, whereas alarge decrease in R-R variation canresult from either parasympatheticneuropathy or stress (f$-adrener-gic stimulation).
R-R variation is influenced by manyphysiological factors:
a. Respiratory rate. There is a de-crease in R-R variation with in-creasing respiration rate. Thegreatest R-R variation occurs ata respiratory rate of 5 breaths/min. Thus, it is not only impor-tant to standardize the respira-tion rate, but the rate should be5 breaths/min to optimize theresults.
b. Age. R-R variation decreaseswith age and allowance mustbe made for this.
c. Weight. Parasympathetic activ-ity is reduced in obese individ-uals.
d. Blood pressure/body tempera-ture. These affect the responsein predictable manners basedon the heart-rate response.
e. Heart rate. In normal individu-als, heart rate increases and R-Rvariation decreases in a predict-able manner with aging (7). Indiabetic individuals, changes inheart rate are more compli-cated. With increasing dura-tion of diabetes there is initiallyan increase followed by a slow-ing and finally a fixed heart rate(8). R-R variation, in contrast,decreases early and rapidly af-ter the diagnosis of diabetes hasbeen established (9).
f. Position. Both standing and sit-ting significantly reduce R-Rvariation, therefore tests mustbe done in the lying position.
Confounding variables in R-R auto-nomic testing (4):
a. General: this includes eating,drinking coffee, and smoking.
b. Sodium salicylate raises the R-Rvariation.
c. Dehydration can alter the re-sponse.
d. Coronary artery disease: it hasbeen shown that patients with
Table 2—Functional changes associated with autonomic failure
SYSTEMS INVOLVED MANIFESTATIONS
CARDIOVASCULAR RESTING TACHYCARDIA, IMPAIRED EXERCISE-INDUCED CARDIOVASCULAR
RESPONSES, CARDIAC DENERVATION, ORTHOSTATIC HYPOTENSION, HEAT
INTOLERANCE, IMPAIRED VASODILATAT1ON, IMPAIRED VENOARTER1OLAR
REFLEX (DEPENDENT EDEMA)
EYE DECREASED DIAMETER OF DARK-ADAPTED PUPIL (DARK-ADAPTED MIOSIS)
GASTROINTESTINAL ESOPHAGEAL ENTEROPATHY, GALLBLADDER ATONY, IMPAIRED COLONIC
MOTIL1TY (DIARRHEA, CONSTIPATION), ANORECTAL SPHINCTER DYSFUNCTION
(INCONTINENCE)
GENITOURINARY NEUROGENIC VESICAL DYSFUNCTION (DECREASED BLADDER SENSITIVITY/
INCONTINENCE/RETENTION), SEXUAL DYSFUNCTION, (MALE: PENILE ERECTILE
FAILURE AND RETROGRADE EJACULATION; FEMALE: DEFECTIVE LUBRICATION)
SUDOMOTOR ANHIDROSIS/HYPERHIDROSIS (HEAT INTOLERANCE), GUSTATORY SWEATING
ENDOCRINE HYPOGLYCEMIA-ASSOCIATED AUTONOMIC FAILURE
1096 DIABETES CARE, VOLUME 15, SUPPLEMENT 3, AUGUST 1992
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/15/8/1095/441790/15-8-1095.pdf by guest on 07 July 2022
Autonomic nervous system testing
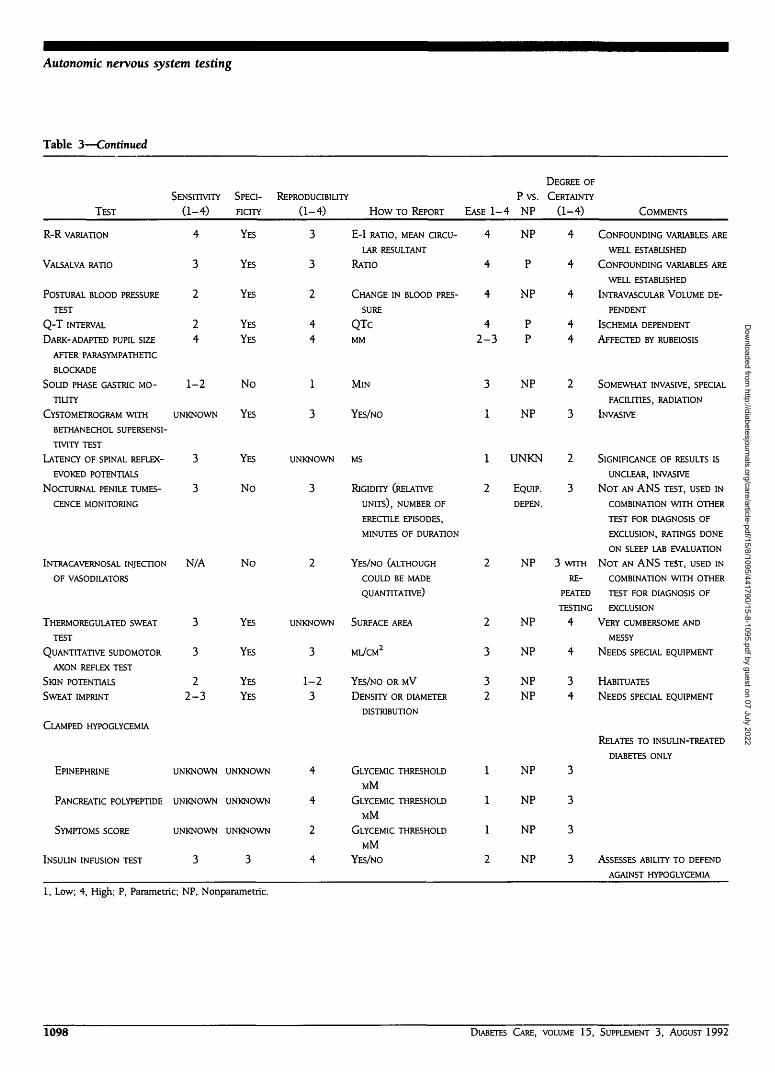
Table 3—Tests for autonomic failure and their suitability for cross-sectional and longitudinal studies in individual and groups
TEST
R - R VARIATION
VALSALVA RATIO
POSTURAL BLOOD PRESSURE TEST
Q - T INTERVAL
DARK-ADAPTED PUPIL SIZE AFTER PARASYMPA-
THETIC BLOCKADE
SOLID PHASE GASTRIC MOTILITY
CYSTOMETROGRAM WITH BETHANECHOL SUPERSEN-
SITIVITY TEST
LATENCY OF SPINAL REFLEX-EVOKED POTENTIALS
NOCTURNAL PENILE TUMESCENCE MONITORING
INTRACAVERNOSAL INJECTION OF VASODILATORS
THERMOREGULATED SWEAT TEST
QUANTITATIVE SUDOMOTOR AXON REFLEX TEST
SKIN POTENTIALS
SWEAT IMPRINT
CLAMPED HYPOGLYCEMIA
EPINEPHRINE
PANCREATIC POLYPEPTIDE
SYMPTOMS SCORE
INSULIN INFUSION TEST
KEY
REFERENCES
410
1314
1319,21
20161722
25,2623241,2
33
STANDARDIZATION
YES
YES
YES
YES
YES
NoYES
YES
YES
NoYES
YES
YES
YES
YES
YES
YES
YES
QUANTITATIVE
STUDIES
YES
YES
YES
YES
YES
YES
No
YES
YES
NoSEMI
YES
SEMI
YES
YES
YES
YES
No
LONGITUDINAL
STUDIES
YES
YES
YES
YES
YES
YES
No
NoYES
YES
YES
YES
YES
YES
YES
YES
YES
YES
POPULATION
INDIVIDUAL
YES
YES
YES
YES
YES
YES
YES
YES
YES
YES
YES
YES
YES
YES
YES
YES
NoYES
GROUP
YES
YES
YES
YES
YES
YES
No
NoYES
YES
YES
YES
YES
YES
YES
YES
YES
YES
inferior wall myocardial infarc-tions experience a bradycardia-h y p o t e n s i v e s y n d r o m e ,whereas patients with anteriorwall myocardial infarctionsexperience tachycardia-hyper-tensive syndromes. Both canaffect the R-R variation.
Valsalva maneuver. The subjectblows into the mouthpiece of amanometer to 40 mmHg for 15 swith continuous EKG monitoringbefore, during, and after the pro-cedure. Healthy subjects developtachycardia and peripheral vaso-constriction during strain, and anovershoot in blood pressure andbradycardia on release. The Val-salva ratio is the longest R-R/shortest R-R. The Valsalva maneu-ver has also been well evaluatedand studied (10). It encompassesa complex reflex arc involvingboth sympathetic and parasympa-
thetic pathways to the heart, sym-pathetic pathways to the vasculartree, and baroreceptors in thechest and lungs.
4. Blood pressure response to stand-ing. The blood pressure responseis measured with the patient lyingsupine at rest and again after 1and 5 min standing. The absolutefall is arbitrary but fall in systolicblood pressure greater than 20mmHg accompanied by symp-toms of orthostasis is taken to beevidence of sympathetic failure.Photoplethysmographic beat-to-beat blood pressure recordingmay have significant advantagesand can be used to evaluate thecomponents of the Valsalva ma-neuver (11). Its role in clinicalstudies awaits more extensiveexperience.
5. QTc interval. Examination of theEKG may reveal a prolonged QTc
interval in patients with cardiacautonomic neuropathy (12,13).
EyeDark-adapted pupil size after total para-sympathetic blockade may be a usefulreproducible and valuable tool for eval-uating autonomic nervous system func-tion, and is related to poor dark vision(14).
Motor disturbances ofgastrointestinal tract
1. Esophageal and gallbladder enter-opathy. These are usually discov-ered accidentally while reviewingupper gastrointestinal studies.
2. Gastroparesis. In evaluating a pa-tient with suspected diabetic gas-troparesis, the level of glycemiccontrol should be assessed. Carefulhistory of medications including
DIABETES CARE, VOLUME 15, SUPPLEMENT 3, AUGUST 1992 1097
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/15/8/1095/441790/15-8-1095.pdf by guest on 07 July 2022
Autonomic nervous system testing
Table 3—Continued
TEST
R - R VARIATION
VALSALVA RATIO
POSTURAL BLOOD PRESSURE
TEST
Q - T INTERVAL
DARK-ADAPTED PUPIL SIZE
AFTER PARASYMPATHET1C
BLOCKADE
SOLID PHASE GASTRIC MO-
TIUTY
CYSTOMETROGRAM WITH
BETHANECHOL SUPERSENS1-
TIVITYTEST
LATENCY OF SPINAL REFLEX-
EVOKED POTENTIALS
NOCTURNAL PENILE TUMES-
CENCE MONITORING
SENSITIVITY
(1-4)
4
3
2
24
1-2
UNKNOWN
3
3
SPECI-
FICITY
YES
YES
YES
YES
YES
No
YES
YES
No
REPRODUCIBIUTY
(1-4)
3
3
2
44
1
3
UNKNOWN
3
How TO REPORT
E-I RATIO, MEAN CIRCU-
LAR RESULTANT
RATIO
CHANGE IN BLOOD PRES-
SURE
QTcMM
MlN
YES/NO
MS
RIGIDITY (RELATIVE
UNITS), NUMBER OF
EASE 1-4
4
4
4
42-3
3
1
1
2
Pvs.NP
NP
P
NP
PP
NP
NP
UNKN
EQUIP.
DEPEN.
DEGREE OF
CERTAINTY
(1-4)
4
4
4
44
2
3
2
3
COMMENTS
CONFOUNDING VARIABLES ARE
WELL ESTABLISHED
CONFOUNDING VARIABLES ARE
WELL ESTABLISHED
INTRAVASCULAR VOLUME DE-
PENDENT
ISCHEMIA DEPENDENT
AFFECTED BY RUBEIOSIS
SOMEWHAT INVASIVE, SPECIAL
FACILITIES, RADIATION
INVASIVE
SIGNIFICANCE OF RESULTS IS
UNCLEAR, INVASIVE
N O T AN ANS TEST, USED IN
COMBINATION WITH OTHER
INTRACAVERNOSAL INJECTION N/A
OF VASODILATORS
No
THERMOREGULATED SWEAT
TEST
QUANTITATIVE SUDOMOTOR
AXON REFLEX TEST
SKIN POTENTIALS
SWEAT IMPRINT
3
3
22-3
YES
YES
YES
YES
ERECTILE EPISODES,
MINUTES OF DURATION
2 YES/NO (ALTHOUGH
COULD BE MADE
QUANTITATIVE)
UNKNOWN SURFACE AREA
3 ML/CM2
1-2 YES/NO OR MV
3 DENSITY OR DIAMETER
DISTRIBUTION
NP
2
3
32
NP
NP
NPNP
RE-PEATED
TESTING
4
4
34
CLAMPED HYPOGLYCEMIA
EPINEPHRINE UNKNOWN UNKNOWN
PANCREATIC POLYPEPTIDE UNKNOWN UNKNOWN
SYMPTOMS SCORE UNKNOWN UNKNOWN
INSULIN INFUSION TEST 3 3
TEST FOR DIAGNOSIS OF
EXCLUSION, RATINGS DONE
ON SLEEP LAB EVALUATION
3 WITH N O T AN ANS TEST, USED IN
COMBINATION WITH OTHER
TEST FOR DIAGNOSIS OF
EXCLUSION
VERY CUMBERSOME AND
MESSY
NEEDS SPECIAL EQUIPMENT
HABITUATES
NEEDS SPECIAL EQUIPMENT
RELATES TO INSULIN-TREATED
DIABETES ONLY
4
4
2
4
GLYCEMIC THRESHOLD
MM
GLYCEMIC THRESHOLD
MM
GLYCEMIC THRESHOLD
MM
YES/NO
1
1
1
2
NP
NP
NP
NP
3
3
3
3 ASSESSES ABILITY TO DEFEND
AGAINST HYPOGLYCEMIA
1, Low; 4, High; P, Parametric; NP, Nonparametric.
1098 DIABETES CARE, VOLUME 15, SUPPLEMENT 3, AUGUST 1992
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/15/8/1095/441790/15-8-1095.pdf by guest on 07 July 2022
Autonomic nervous system testing
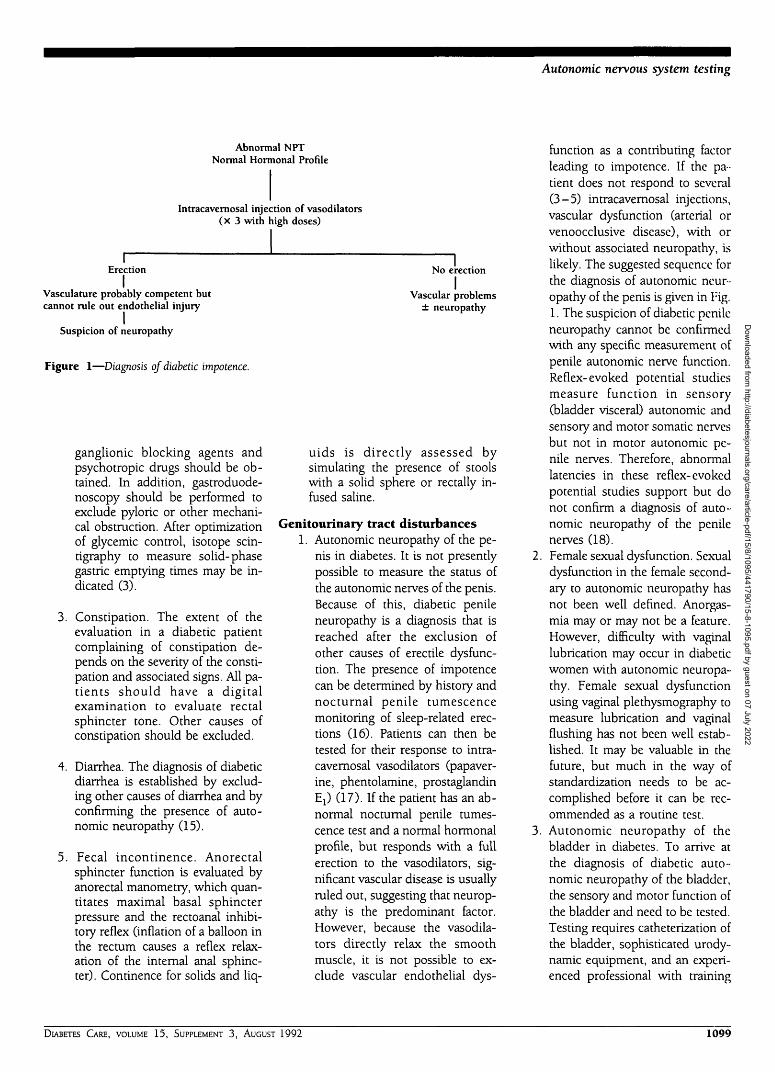
Abnormal NPTNormal Hormonal Profile
Intracavemosal injection of vasodilators(X 3 with high doses)
Erection
IVasculature probably competent butcannot rule out endothelial injury
Suspicion of neuropathy
Figure 1—Diagnosis of diabetic impotence.
ganglionic blocking agents andpsychotropic drugs should be ob-tained. In addition, gastroduode-noscopy should be performed toexclude pyloric or other mechani-cal obstruction. After optimizationof glycemic control, isotope scin-tigraphy to measure solid-phasegastric emptying times may be in-dicated (3).
3. Constipation. The extent of theevaluation in a diabetic patientcomplaining of constipation de-pends on the severity of the consti-pation and associated signs. All pa-tients should have a digitalexamination to evaluate rectalsphincter tone. Other causes ofconstipation should be excluded.
4. Diarrhea. The diagnosis of diabeticdiarrhea is established by exclud-ing other causes of diarrhea and byconfirming the presence of auto-nomic neuropathy (15).
5. Fecal incontinence. Anorectalsphincter function is evaluated byanorectal manometry, which quan-titates maximal basal sphincterpressure and the rectoanal inhibi-tory reflex (inflation of a balloon inthe rectum causes a reflex relax-ation of the internal anal sphinc-ter). Continence for solids and liq-
No erection
IVascular problems
± neuropathy
uids is directly assessed bysimulating the presence of stoolswith a solid sphere or rectally in-fused saline.
Genitourinary tract disturbances1. Autonomic neuropathy of the pe-
nis in diabetes. It is not presentlypossible to measure the status ofthe autonomic nerves of the penis.Because of this, diabetic penileneuropathy is a diagnosis that isreached after the exclusion ofother causes of erectile dysfunc-tion. The presence of impotencecan be determined by history andnocturnal penile tumescencemonitoring of sleep-related erec-tions (16). Patients can then betested for their response to intra-cavemosal vasodilators (papaver-ine, phentolamine, prostaglandinE:) (17). If the patient has an ab-normal nocturnal penile tumes-cence test and a normal hormonalprofile, but responds with a fullerection to the vasodilators, sig-nificant vascular disease is usuallyruled out, suggesting that neurop-athy is the predominant factor.However, because the vasodila-tors directly relax the smoothmuscle, it is not possible to ex-clude vascular endothelial dys-
function as a contributing factorleading to impotence. If the pa-tient does not respond to several(3-5) intracavemosal injections,vascular dysfunction (arterial orvenoocclusive disease), with orwithout associated neuropathy, islikely. The suggested sequence forthe diagnosis of autonomic neur-opathy of the penis is given in Fig.1. The suspicion of diabetic penileneuropathy cannot be confirmedwith any specific measurement ofpenile autonomic nerve function.Reflex-evoked potential studiesmeasure function in sensory(bladder visceral) autonomic andsensory and motor somatic nervesbut not in motor autonomic pe-nile nerves. Therefore, abnormallatencies in these reflex-evokedpotential studies support but donot confirm a diagnosis of auto-nomic neuropathy of the penilenerves (18).
2. Female sexual dysfunction. Sexualdysfunction in the female second-ary to autonomic neuropathy hasnot been well defined. Anorgas-mia may or may not be a feature.However, difficulty with vaginallubrication may occur in diabeticwomen with autonomic neuropa-thy. Female sexual dysfunctionusing vaginal plethysmography tomeasure lubrication and vaginalflushing has not been well estab-lished. It may be valuable in thefuture, but much in the way ofstandardization needs to be ac-complished before it can be rec-ommended as a routine test.
3. Autonomic neuropathy of thebladder in diabetes. To arrive atthe diagnosis of diabetic auto-nomic neuropathy of the bladder,the sensory and motor function ofthe bladder and need to be tested.Testing requires catheterization ofthe bladder, sophisticated urody-namic equipment, and an experi-enced professional with training
DIABETES CARE, VOLUME 15, SUPPLEMENT 3, AUGUST 1992 1099
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/15/8/1095/441790/15-8-1095.pdf by guest on 07 July 2022

Autonomic nervous system testing
in the field of neurourology. Asimple, noninvasive, and specifictest to screen for the presence ofbladder autonomic neuropathy isnot available.A. Testing of bladder sensitivity,
i. The integrity of bladderproprioception can be testedby progressive filling of thebladder with water or gas(CO2) to record when thepatient first becomes awareof a desire to void (urge)and when bladder filling be-comes painful (bladder ca-pacity) (19).
ii. Perception of visceral paincan be evaluated by deter-mining the electrical percep-tion threshold (19). A cath-eter with s t imulat ingelectrodes is placed in thevesicourethral junction; theintensity of the stimulus isprogressively increased untilthe patient first senses it. El-evated electrical perceptionthresholds are considereddiagnostic of sensory loss(19).
iii. Temperature sensation canalso be evaluated by the in-troduction of warm or coldfluid through the catheter(19).
iv. Another way of determiningthe status of bladder sensorynerves is by measuring thelatency of spinal reflex-evoked potentials (20).Electrical s t imulat ionthrough an indwelling cath-eter in the urethra or vesi-courethral junction elicits acontractile response of theanal sphincter. This re-sponse can be recorded witha bipolar needle placed inthe sphincter. The latencybetween the stimulus andthe response can be mea-sured to assess the integrity
of this reflex pathway, inwhich the afferent limbcomprises sensory auto-nomic fibers traveling in thepelvic nerves and the effer-ent limb, motor somaticnerve fibers in the pudendalnerve. It is possible that theabnormality in the reflexpathway is due to an altera-tion in the efferent ratherthan in the afferent limb. Todifferentiate an autonomicsensory from a somatic mo-tor alteration, the bulbocav-ernosus reflex can be tested.In this reflex both limbs areformed by somatic fibers. Ifthe latency of this reflex isnormal, it can be concludedthat the increase in the re-flex latency after visceralstimulation is likely due toneuropathy of the sensoryautonomic fibers. In addi-tion, electromyography ofthe anal sphincter aftervoluntary contraction willassist in determining thepresence or absence of neu-ropathy in this somatic mo-tor pathway. The advantageof this method over thosedescribed in i, ii, and iii isthat is does not rely on thepatient reporting a sensationbut rather on an electro-physiological measurement.The disadvantage of mea-suring the latency of spinalreflex-evoked potentials isthat there is limited experi-ence with this method and itrequires sophisticated elec-trophysiological equipment.Although this method isquantitative and can bestandardized, its reproduc-ibility and specificity are notknown. The invasive andcomplicated nature of thistest makes it a poor candi-
date for longitudinal stud-ies.
B. Testing of bladder motor func-tion.
The ability of the bladder toempty urine not only de-pends on the ability of thedetrusor to contract but alsoon a nonobstructed bladderoutlet. Therefore, when eval-uating the motor function ofthe bladder, it is necessary torule out bladder outlet ob-struction. This is particularlyimportant in older men inwhom bladder outlet ob-struction is prevalent,
i. Detrusor motor functioncan be studied by perform-ing a cystometrogram(19,20). This test studies thedetrusor reflex function.The normal bladder, whenfilled with fluid or gas, re-sponds with a reflex con-traction of the detrusor.This contraction can bevoluntarily suppressed. Abladder that does not con-tract with filling is consid-ered an areflexic bladder.This can be due to an in-ability to suppress the psy-chogenic central influencecontrolling this reflex, toneuropathy of sensor auto-nomic nerves, and/or toneuropathy of motor auto-nomic fibers responsiblefor contraction of the de-trusor muscle. Therefore,the finding of bladder are-flexia alone is not sufficientfor the diagnosis of auto-nomic motor neuropathy ofthe bladder. The bethane-chol supersensitivity test isused to determine the pres-ence of efferent denervationof the bladder (21). This testis based on Canon's law ofdenervation supersensitivity
1100 DIABETES CARE, VOLUME 15, SUPPLEMENT 3, AUGUST 1992
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/15/8/1095/441790/15-8-1095.pdf by guest on 07 July 2022

Autonomic nervous system testing
of an organ to its neuro-transmitter. Bethanechol (5mg), a muscarinic agonist, isgiven subcutaneously andthe cystometrogram is re-peated. After the bladderhas been filled with 100 mlof water or gas, if the intra-vesical pressure is >20 cmH2O above the intravesicalpressure before the adminis-tration of bethanechol, thetest is considered positive. Ifmotor autonomic neuropa-thy is present, the test willbe positive. Patients withpsychogenic suppression ofthe detrusor reflex or sen-sory autonomic neuropathyin the absence of motor neu-ropathy would have a nega-tive test. The sensitivity ofthe test is not known. It isconsidered to be specific forautonomic motor neuropa-thy, but due to its invasivenature, it is probably notuseful in longitudinal stud-ies.
ii. Finally, measurement ofvolume of residual urine af-ter urination may be used,in the absence of bladderoutflow obstruction, as anindicator of bladder motorfunction. After the patienthas urinated, the volume ofresidual urine can be deter-mined non-invasively withan ultrasound bladder scan-ner or, invasively, by cathe-terization.
Sudomotor sympathetic functionSudomotor function may be evaluatedwith the thermoregulatory sweat test,quantitative sudomotor axon reflex test,skin potentials, or sweat imprint quanti-tation.
The thermoregulatory sweat testis a sensitive test of sweat distribution(22). The subject is dusted with an indi-
cator powder that turns purple whenmoist. This qualitative test can be ren-dered semiquantitative by charting thepercentage of anterior body surface thatis anhidrotic.
The skin potential can be re-corded with standard EMG equipmentfrom the palm and sole (23). The stim-ulus is an electric shock, an inspiratorygasp, or other stimuli that activate type IIand III mechanoreceptor afferents. Theskin potential is readily evoked but ha-bituates.
The silastic skin imprint is ob-tained after the application of silastic ma-terial to stimulated skin (24). The sweatdroplet indents the imprint and thecount and diameter distribution can bedetermined. The usual stimulus is pilo-carpine administered by iontophoresis.In the quantitative sudomotor axon re-flex test the stimulus consists of theiontophoresis of acetylcholine via thestimulus compartment of a multicom-partmental sweat cell (25,26). Postgan-glionic sympathetic nerve terminals areactivated and the nerve impulse travelsretrogradely, reaches a branch point,then travels orthogradely to activate asecond population of sweat glands. Thesweat response from this second popula-tion of sweat glands is recorded by asudorometer. The stimulus compartmentsurrounds the central recording com-partment, separated by an air gap andtwo ridges (to block diffusion). This testevaluates the integrity of the distal post-ganglionic sympathetic sudomotor axon.Four recording sites (distal forearm and3 lower extremity sites) are used. Thetest has high sensitivity, a coefficient ofvariation of 20%, and, when used in con-junction with the thermoregulatory sweattest, defines the pre- or postganglionicsite of the lesion. The test requires spe-cialized equipment, trained technicians,and 20-30 min to complete.
Endocrine tests for functionalautonomic failure in diabetesHAAF appears to be distinct from classicdiabetic autonomic neuropathy (27).
First, the two disorders can occur inde-pendently. Second, deficient autonomicresponses are specific for the stimulus ofhypoglycemia in HAAF, whereas re-duced sympathetic and parasympatheticresponses to multiple stimuli character-ize autonomic neuropathy. Third,whereas reduced epinephrine responsesto hypoglycemia are a characteristic fea-ture of HAAF, epinephrine responsesare reduced little if at all in insulin-dependent diabetes mellitus (IDDM)with autonomic neuropathy comparedwith IDDM without autonomic neurop-athy. Fourth, diabetic autonomic neur-opathy, in sharp contrast to HAAF, isnot a risk factor for iatrogenic hypogly-cemia in IDDM (28,29). The pathogene-sis of HAAF is not known; it probably ismultifactorial and may be related to re-cent antecedent hypoglycemia (30-32).
Tests for functional autonomicfailure in IDDM are complex for the pa-tient as well as the investigator and laborintensive. Ideally, both glycemic thresh-olds for symptoms and counterregula-tory activation and glycemic defenseagainst mild to moderate hyperinsuline-mia should be determined in patientswith IDDM and appropriate control sub-jects. Defense against hyperinsulincmichypoglycemia is probably the more es-sential, at least for clinical purposes, be-cause it has been shown in prospectivestudies (33,34) to have clinical predictivepower, i.e., to identify patients at mark-edly increased risk (> 25-fold) for severeiatrogenic hypoglycemia.
Glycemic thresholds can be de-fined with the hyperinsulinemic steppedhypoglycemic clamp technique (1,2,35).The stepped hypoglycemic clamp tech-nique can be highly standardized (1,2).However, the test is complex. Precisequantitation of the glycemic thresholdsrequires both a euglycemic controlclamp and a stepped hypoglycemicclamp in each individual studied. Arteri-alized blood samples are also required.The reproducibility of the stepped hypo-glycemia clamp technique has not beenassessed systematically. However, the
DIABKTKS CARE, VOLUME 15, SUPPLEMENT 3, AUGUST 1992 1101
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/15/8/1095/441790/15-8-1095.pdf by guest on 07 July 2022

Autonomic nervous system testing
fact that identical glycemic thresholds forsymptoms and glucagon and epineph-rine release were calculated from datagenerated with the technique in two dif-ferent laboratories (1,2) indicates thatthe test is probably reproducible. Thetechnique is probably more suitable forpopulations rather than individuals, i.e.,it might not identify all patients withminimally altered glycemic thresholds.
The results of the stepped hypo-glycemia clamp test should be reportedas absolute glycemic thresholds (glucoseconcentration), with those of the insulininfusion test as negative (adequate glu-cose counterregulation) or positive (de-fective glucose counterregulation). Forthe stepped hypoglycemic clamp tech-nique, comparison of each response(symptom scores, hormone concentra-tions) of each individual patient with the95% confidence interval of the corre-sponding response for a nondiabeticcontrol group is preferable (1,2), al-though comparisons of group means canbe used. For the latter, either parametricor nonparametric tests will be appropri-ate to a given data set.
Glycemic defense against hyper-insulinemia can be defined with an insu-lin infusion test (33). The insulin infu-sion test can be standardized with arelatively low insulin infusion dose (0.67mU • kg"1 • min • - 1 ) and a specificplasma glucose end point (<2 mM =defective glucose counterregulation). Inaddition, a neuroglycopenic end pointmust be included for ethical reasons. In-clusion of neuroglycopenia (difficultythinking, blurred vision, dizziness, fatigueand faintness) as an additional end pointincreases the predictive power of the test(33). Although the test yields only a posi-tive or negative conclusion—defective oradequate glucose counterregulation—ithas >90% clinical predictive power fordevelopment of hypoglycemia with inten-sive insulin treatment.
The test is labor intensive, requir-ing a minimum of two people (typically aphysician and nurse); a third person isneeded if cognitive function is assessed. It
also requires accurate glucose measure-ments (e.g., with a Beckman or YSI ana-lyzer not with a portable glucose monitor)at the bedside and the analytical capacityto perform the hormone measurements.Cognitive assessment generally requires acollaborating psychologist (2,36).
The insulin infusion test has beenshown to be highly reproducible (33,34).With three replicate tests at 3- to 4-wkintervals, coefficients of variation for glu-cose and key counterregulatory hormone(glucagon, epinephrine) responses were<8% (34). One can estimate sensitivityand specificity to be ~90% from the dataof White et al. (33). But, these are mini-mum estimates. In the data of Bolli et al.(34), none of the patients with a negativetest (nadir >2.2 mM) subsequently suf-fered severe clinical hypoglycemia,whereas all of those with a positive test(nadir <2.2 mM) suffered severe hypogly-cemia during subsequent intensive ther-apy.
SUMMARY ANDRECOMMENDATIONS— Severalorgan systems can be monitored by reli-able longitudinal testing. These include:
1. Cardiovascular systema. R-R variationb. Valsalva maneuverc. Postural blood pressure testing
2. Sudomotora. Postganglionic function with
QSART3. Eye
a. Dark-adapted pupil size aftertotal parasympathetic blockade.
Specific research projects may in-clude other tests but these tests do notlend themselves easily for large, multi-center type of studies. The test listedabove are noninvasive, quantitative, andare sufficiently standardized to allow lon-gitudinal assessment in diabetic patients.Furthermore, these tests allow evaluationof at least three different organ systems.
HAAF, an example of functionalautonomic failure in diabetes, is best as-sessed by evaluation of the glycemic
thresholds for epinephrine and pancre-atic polypeptide secretion and hypogly-cemic symptoms using a stepped hypo-glycemic clamp protocol. The status ofphysiological defense against hyperinsu-linemic hypoglycemia can be assessedwith the insulin infusion test.
References
1. Schwartz NS, Clutter WE, Shan SD,Cryer PE: The glycemic thresholds foractivation of glucose counterregulatorysystems are higher than the threshold forsymptoms. J Clin Invest 79:777-81, 1987
2. Mitrakou A, Ryan C, Veneman T, MokanM, Jennssen T, Kiss 1, DurrantJ, Cryer P,Gerich J: Hierarchy of glycemic thresh-olds for counterregulatory hormone se-cretion, symptoms, and cerebral dys-function. Am] Physiol 260:E67-74, 1991
3. Achem-Karam SR, Funakoshi A, VinikAl: Plasma motilin and migrating motorcomplex in diabetic gastroparesis. Gas-troenterology 88:492-94, 1985
4. Genovely H, Pfeifer MA: RR-Variation:the autonomic test of choice in diabetes.Diabetes Metab Rev 4:255-71, 1988
5. Pfeifer MA, Cook D, BrodskyJ, Tice D,Reenan A, Swedine S, Halter JB, Porte JrD: Quantitative evaluation of cardiacparasympathetic activity in normal anddiabetic man. Diabetes 31:339-45, 1982
6. Weinberg CR, Pfeifer MA: Developmentof a predictive model for symptomaticneuropathy in diabetes. Diabetes 35:873-80, 1986
7. Pfeifer MA, Halter JB, Weinber CR, CookD, Best J, Reenan A, Porte D Jr: Differen-tial changes of autonomic nervous sys-tem function with age in man. Am J Med75:249, 1983
8. Ewing DJ, Campbell IW, Clarke BF:Heart rate changes in diabetes mellitus.Lancet 1:183, 1981
9. Pfeifer MA, Weinberg CR, Cook D, Re-enan A, Halter JB, EnsinckJ, Porte Jr D:Autonomic neural dysfunction in re-cently diagnosed diabetic subjects. Dia-betes Care 7:447-53, 1984
10. Rothschild AH, Weinberg C, Cook D,Halter J, Porte D, Pfeifer MA: Sensitivityof R-R variation and the Valsalva ratio inthe assessment of cardiovascular diabetic
1102 DIABETES CARE, VOLUME 15, SUPPLEMENT 3, AUGUST 1992
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/15/8/1095/441790/15-8-1095.pdf by guest on 07 July 2022
Autonomic nervous system testing
autonomic neuropathy. Diabetes Care 40:735-41, 1987
11. Sandroin P, Benarroch EE, Low PA:Pharmacologic dissection of the compo-nents of the valsalva maneuver in adren-ergic failure. J Appl Physiol 71:1563-67,1991
12. KahnJK, Sisson JC, Vinik Al: QT Intervalprolongation and sudden cardiac deathin diabetic autonomic neuropathy. J ClinEndocrinol Metab 64:751-54, 1987
13. Gonin JM, Kadrofske MM, Schmaltz S,Vinik Al: Corrected Q-T interval prolon-gation as diagnostic tool for assessmentof cardiac autonomic neuropathy in dia-betes mellitus. Diabetes Care 13:68-71,1990
14. Pfeifer MA, Code DL, BrodskyJ: Quan-titative evaluation of sympathetic andparasympathetic control of iris function.Diabetes Care 5:518-28, 1982
15. Barnett JL, Vinik Al: Gastointestinal dis-turbances in diabetes. In Therapy for Di-abetes Mellitus and Related Disorders. Leb-
ovitz AE, Ed. Alexandria, VA, Am.Diabetes Assoc, 1991, p. 279-87
16. Karacan 1, Salis PJ, Ware JC, Derveut B,Williams RL, Scott FB, Attia SL, BeutlerLE: Nocturnal penile tumescence and di-agnosis in diabetic impotence. AmJ Psy-chiatry 135:191-97, 1978
17. Krane RJ, Goldstein I, Saenz de Tejada I:Impotence. N EnglJ Ued 321:1648-59,1989
18. Sarica Y, Karacan I: Bulbocavernosus re-flex to somatic and visceral nerve stimu-lation in normal subjects and in diabeticswith erectile impotence. J Urol 138:55-58, 1987
19. Fridmodt-Moller C: Diabetic cystopathy.Danish Med Bull 25:49-59, 1978
20. Bradley WE: Diagnosis of urinary blad-der dysfunction in diabetes mellitus. AnnIntern Med 92:323-26, 1980
21. Lapides J: Denervation supersensitivityas a test for neurogenic bladder. SurgGynecol Obstet 114:241-49, 1962
22. Fealey RD, Low PA, Thomas JE: Themo-regulatory sweating abnormalities in di-abetes mellitus. Mayo Clin Proc 64:617-28, 1989
23. Shahani BT, HalperinJJ, Boulu P, CohenJ: Sympathetic skin response: a methodof assessing unmyelinated axon dysfunc-tion in peripheral neuropathies. J NeuralNeurosurg Psychiat 47:536-42, 1984
24. Kennedy WR, Sakuta M, Sutherland D,Goetz FC: Quantitation of the sweatingdeficit in diabetes mellitus. Ann Neurol15:482-88, 1984
25. Low PA, Zimmerman BR, Dyck PJ: Com-parison of distal sympathetic with vagalfunction in diabetic neuropathy. MuscleNerve 9:592-96, 1986
26. Low PA, Caskey PE, Tuc RR, Fealey RD,Dyck PJ: Quantitive sudomotor axon re-flex test in normal and neuropathic sub-jects. Ann Neurol 14:573-80, 1983
27. Cryer PE: Iatrogenic hypoglycemia as acause of hypoglycemia-associated auto-nomic failure in IDDM: a vicious cycle.Diabetes 41:255-60, 1992
28. Diabetes Control and ComplicationsTrial Research Group: Epidemiology ofsevere hypoglycemia in the diabetes con-trol and complications trial. Am J Med90:450-59, 1991
29. Bjork E, Palmer M, Schvarcz E, Berne C:
Incidence of severe hypoglycemia in anunselected population of patients with in-sulin-treated diabetes mellitus with specialreference to autonomic neuropathy. Diabe-tes Nutr Metab 4:303-309, 1990
30. Heller SR, Cryer PE: Reduced neuroen-docrine and symptomatic responses tosubsequent hypoglycemia after one epi-sode of hypoglycemia in nondiabetic hu-mans. Diabetes 40:223-26, 1991
31. Widom B, Simonson DC: Effect of inter-mittent hypoglycaemia on counterregu-latory hormone secretion (Abstract). Di-abetologia 33:A484, 1990
32. Davis M, Shamoon H: Adaptive counter-regulatory responses to hypogycemia innondiabetic humans (Abstract). Diabetes38:5A, 1989
33. White NH, Skor DA, Cryer PE, Bier DM,Levandoski L, Santiago JV: Identificationof type 1 diabetic patients at increasedrisk for hypoglycemia during intensivetherapy. N EnglJ Med 308:485-91, 1983
34. Bolli GB, Defeo P, DeCosmo S, Perriello G,Ventura MM, Massi-Benedetti M, Santeu-sanio F, Gerich JE, Brunetti P: A reliableand reproducible test for adequate glucosecounterregulation in type I diabetes melli-tus. Diabetes 33:732-37, 1984
35. Boyle PJ, Schwartz NS, Shah SD, ClutterWE, Cryer PE: Plasma glucose concen-trations at the onset of hypoglycemicsymptoms in patients with poorly con-trolled diabetes and in nondiabetics. NEnglJ Med 318:1487-92, 1988
36. Hirsch IB, Boyle PJ, Draft S, Cryer PE:Higher glycemic thresholds for symp-toms during beta-adrenergic blockade inIDDM. Diabetes 40:1177-86, 1991
DIABETES CARE, VOLUME 15, SUPPLEMENT 3 , AUGUST 1992 1103
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/15/8/1095/441790/15-8-1095.pdf by guest on 07 July 2022





























