Embed Size (px)
Citation preview
11Analgesic Analgesic
NephropathyNephropathy
Dr. Mohamed AbbassDr. Mohamed AbbassNephrologistNephrologist
PGDD,CARDIFF,UKPGDD,CARDIFF,UK
Renal disease Renal disease characterized by chronic characterized by chronic interstitial nephritis interstitial nephritis
(CIN) (CIN) and renal papillary and renal papillary necrosisnecrosis(RPN) (RPN) caused by caused by prolonged and excessive prolonged and excessive consumption of analgesic consumption of analgesic
mixturesmixtures
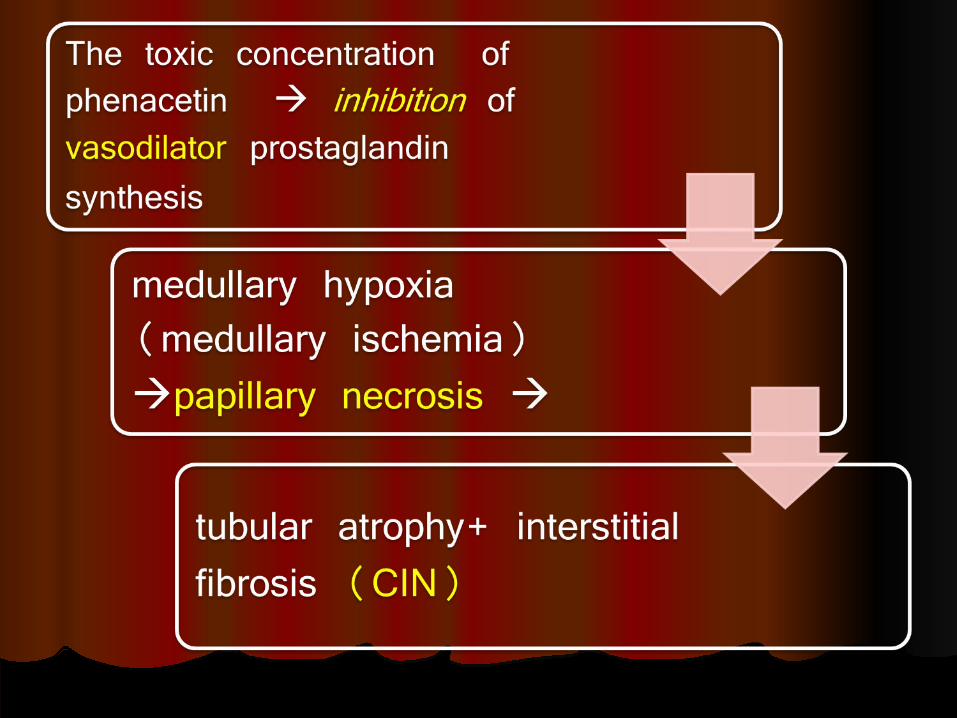
The nephrotoxic effect of The nephrotoxic effect of phenacetinphenacetin is dose is dose
dependent dependent (cumulative (cumulative effect) effect)
Some sources has reported Some sources has reported that the patient must take that the patient must take about about one gram per day one gram per day for two year for two year to have to have analgesic nephropathyanalgesic nephropathy
ANAN waswas one of the most one of the most common causes of chronic common causes of chronic
kidney disease kidney disease CKD CKD especially in Australia especially in Australia and part of Europe and part of Europe but but now marked decline now marked decline after after withdrawal of phenacetinwithdrawal of phenacetin
The most common causes The most common causes are mixtures are mixtures
containing containing phenacetin, phenacetin, aspirin and caffeine aspirin and caffeine
especially the medication especially the medication over-the-counter over-the-counter
Long-term use of Long-term use of aspirin aspirin alone is not alone is not
associated with associated with analgesic nephropathyanalgesic nephropathy
AspirinAspirin can potentiate the can potentiate the nephrotoxic effect of nephrotoxic effect of phenacetin and acetaminophenphenacetin and acetaminophen
1- Inhibit the cyclooxygenase 1- Inhibit the cyclooxygenase enzymes which lead to suppress enzymes which lead to suppress prostaglandin prostaglandin 2- Deplete glutathione which is 2- Deplete glutathione which is responsible for detoxification responsible for detoxification of the reactive intermediate of of the reactive intermediate of acetaminophen and phenacetin acetaminophen and phenacetin
Pathogenesis and Pathogenesis and PathologyPathology
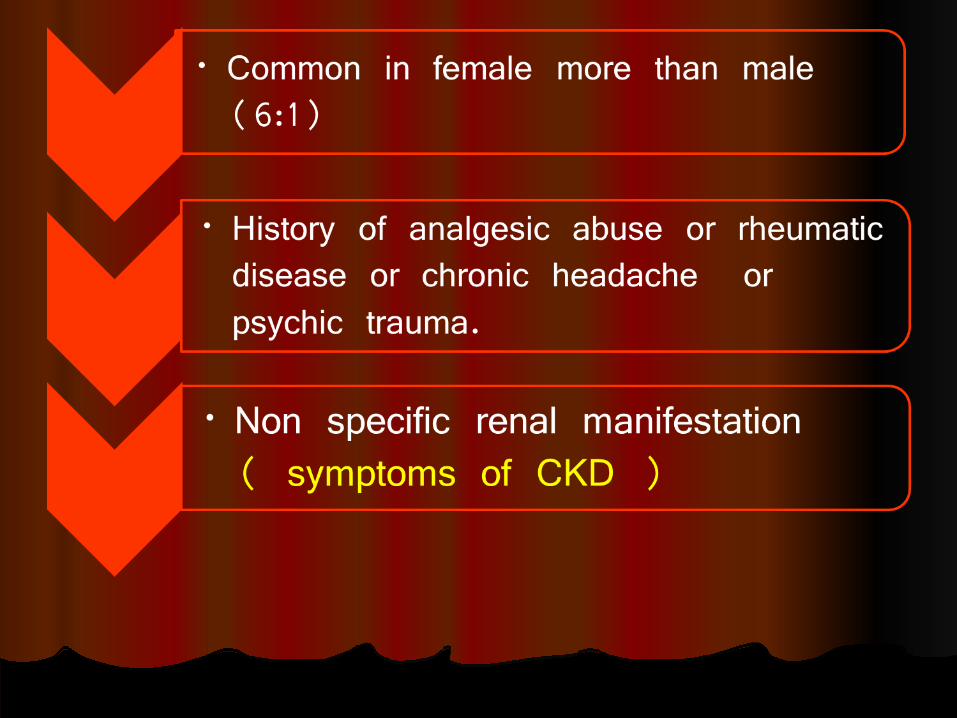
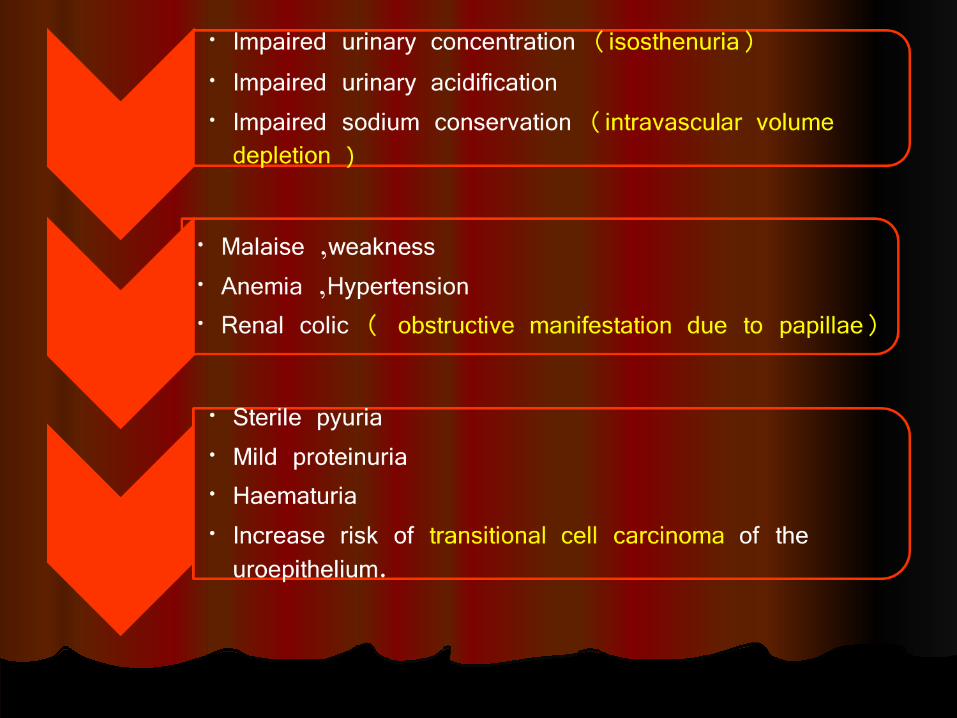
Clinical featuresClinical features

InvestigationsInvestigations
No "gold Test" to No "gold Test" to diagnose analgesic diagnose analgesic
nephropathynephropathy
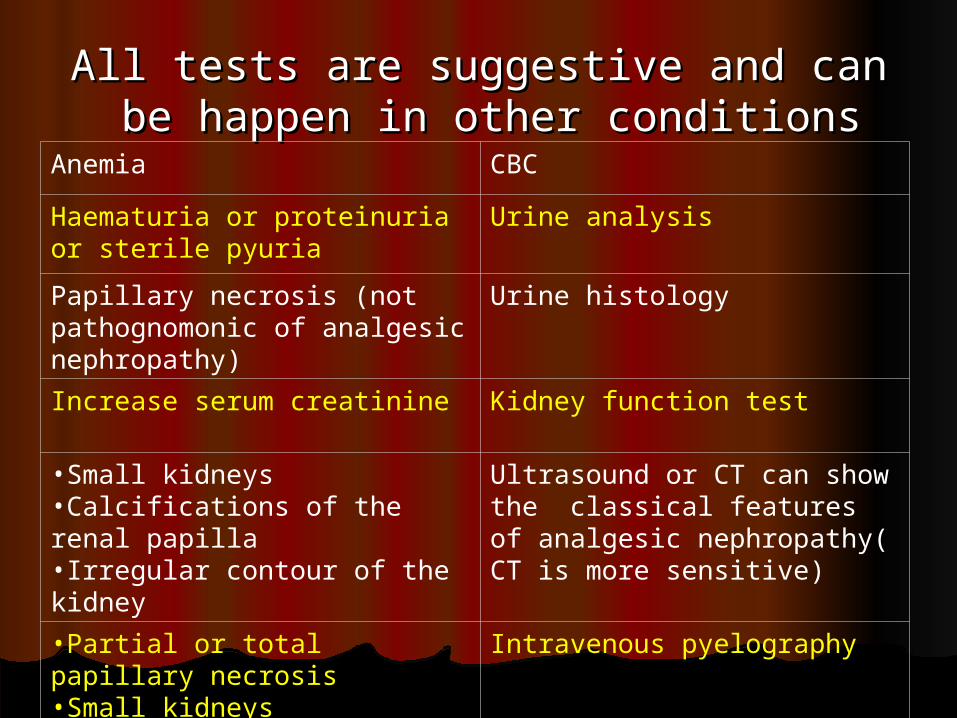
All tests are suggestive and can All tests are suggestive and can be happen in other conditionsbe happen in other conditions
CBC Anemia Urine analysis Haematuria or proteinuria
or sterile pyuria Urine histology Papillary necrosis (not
pathognomonic of analgesic nephropathy)
Kidney function test Increase serum creatinine
Ultrasound or CT can show the classical features of analgesic nephropathy( CT is more sensitive)
•Small kidneys •Calcifications of the renal papilla•Irregular contour of the kidney
Intravenous pyelography •Partial or total papillary necrosis•Small kidneys•Blunted calyces

Differential Differential diagnosisdiagnosis
Sickle cell diseaseSickle cell diseaseChronic pyelonephritisChronic pyelonephritisDiabetesDiabetesRenal tuberculosisRenal tuberculosisUrinary tract obstructionUrinary tract obstructionPolycystic kidney diseasePolycystic kidney diseaseNephrosclerosisNephrosclerosisCauses of chronic Causes of chronic tubulointerstitial tubulointerstitial (Multiple (Multiple myeloma, Sarcoid nephropathy) myeloma, Sarcoid nephropathy)

TreatmentTreatment
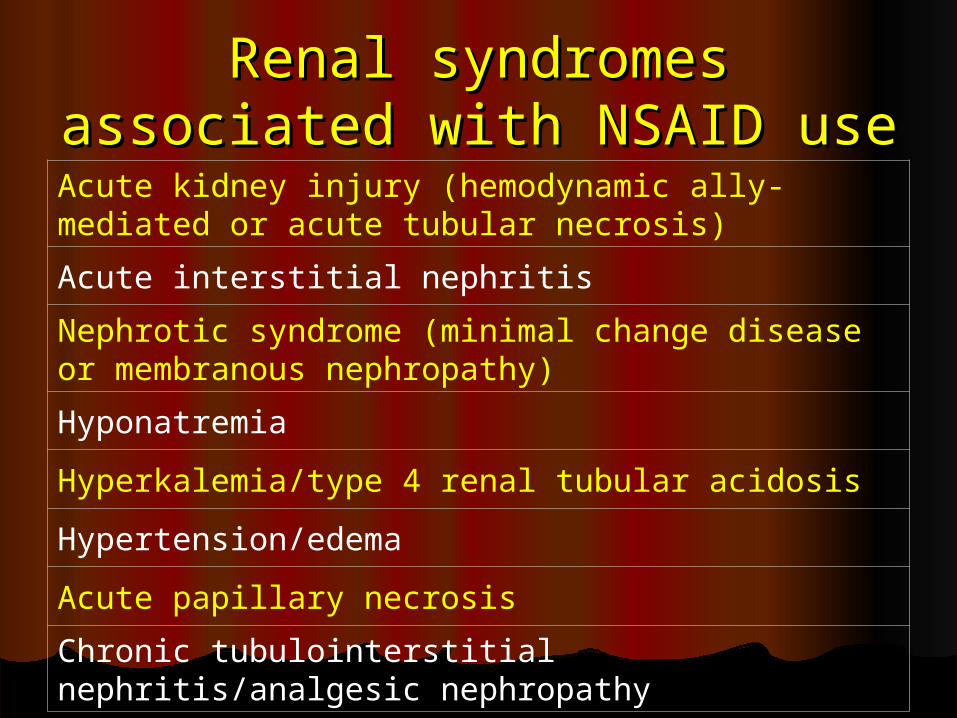
Renal syndromes Renal syndromes associated with NSAID useassociated with NSAID useAcute kidney injury (hemodynamic ally-mediated or acute tubular necrosis)Acute interstitial nephritisNephrotic syndrome (minimal change disease or membranous nephropathy)HyponatremiaHyperkalemia/type 4 renal tubular acidosisHypertension/edemaAcute papillary necrosisChronic tubulointerstitial nephritis/analgesic nephropathy
ThanksThanks
Dr. M. Dr. M. AbbassAbbass























![[Diagnostic aspects of familial juvenile hyperuriceamic nephropathy]](https://img.dokumen.tips/doc/110x75/6348ae5409e11fdd740ae4c1/diagnostic-aspects-of-familial-juvenile-hyperuriceamic-nephropathy.jpg)





