Embed Size (px)
Citation preview
CASE REPORTS
Domestic violence: the shaken adult syndrome
T D Carrigan, E Walker, S Barnes
AbstractA case of domestic violence is reported.The patient presented with the triad ofinjuries associated with the shaking ofinfants: retinal haemorrhages, subduralhaematoma, and patterned bruising; thishas been described as the shaken adultsyndrome. This case report reflects thediYculties in diagnosing domestic vio-lence in the accident and emergencysetting.(J Accid Emerg Med 2000;17:138–139)
Keywords: domestic violence; women; assault
Domestic violence is an under-reported andmajor public health problem that often firstpresents to the accident and emergency (A&E)department. It accounts for half of all violentcrimes against women, and two deaths perweek have been linked to domestic violence inBritain.1 Indeed, the Department of Health hasissued statements to ensure health profession-als are aware of domestic violence in this con-text when patients present with consistenttraumatic injuries.2
The following case report reflects thediYculties in diagnosing domestic violence inthe A&E setting, and stresses the timelyreferral of such patients to the relevantauthorities.
Case reportA 34 year old woman was brought to the A&Edepartment by ambulance at 0400 hours withhead injuries. When handed over from theambulance crew an assault was queried,although the patient later stated she had fallendown stairs after moderate alcohol ingestion.
Her initial blood pressure was 119/72 mmHg, pulse 88 beats/min, her pupils were equaland reactive directly and consensually, and herGlasgow coma score was 13/15 (she wasconfused and was opening her eyes to com-mand). Examination of the head showed bilat-eral periorbital ecchymoses, nasal bridge swell-ing and epistaxis, a right frontal abrasion, andan occipital scalp haematoma. Ecchymoseswere also noted on her back and buttocks,being linear in fashion on both upper arms,and her underpants were torn. Initial skull andfacial x ray films were normal, and she wasadmitted under the care of A&E for neurologi-cal observations.
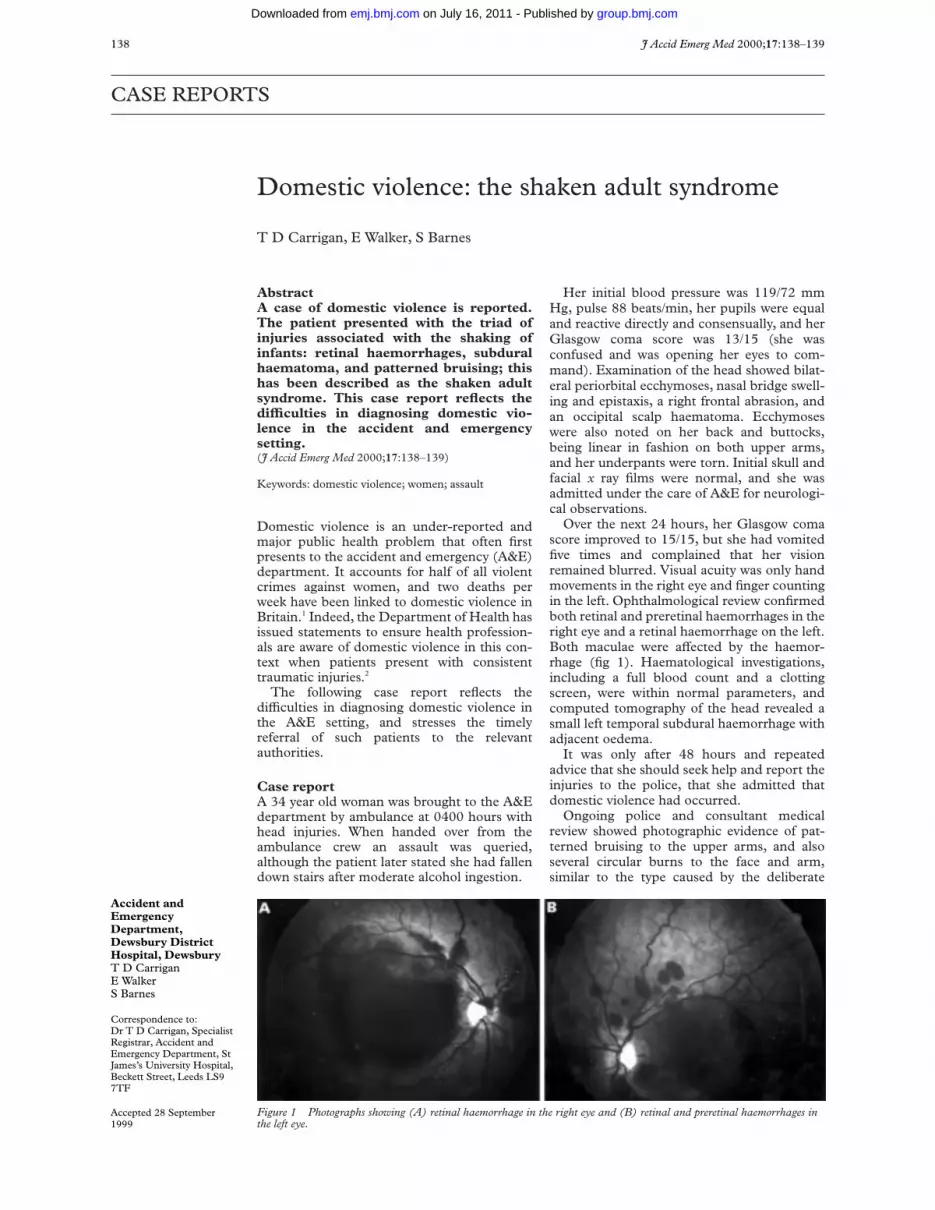
Over the next 24 hours, her Glasgow comascore improved to 15/15, but she had vomitedfive times and complained that her visionremained blurred. Visual acuity was only handmovements in the right eye and finger countingin the left. Ophthalmological review confirmedboth retinal and preretinal haemorrhages in theright eye and a retinal haemorrhage on the left.Both maculae were aVected by the haemor-rhage (fig 1). Haematological investigations,including a full blood count and a clottingscreen, were within normal parameters, andcomputed tomography of the head revealed asmall left temporal subdural haemorrhage withadjacent oedema.
It was only after 48 hours and repeatedadvice that she should seek help and report theinjuries to the police, that she admitted thatdomestic violence had occurred.
Ongoing police and consultant medicalreview showed photographic evidence of pat-terned bruising to the upper arms, and alsoseveral circular burns to the face and arm,similar to the type caused by the deliberate
Figure 1 Photographs showing (A) retinal haemorrhage in the right eye and (B) retinal and preretinal haemorrhages inthe left eye.
J Accid Emerg Med 2000;17:138–139138
Accident andEmergencyDepartment,Dewsbury DistrictHospital, DewsburyT D CarriganE WalkerS Barnes
Correspondence to:Dr T D Carrigan, SpecialistRegistrar, Accident andEmergency Department, StJames’s University Hospital,Beckett Street, Leeds LS97TF
Accepted 28 September1999
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from

application of lit cigarettes. She suVeredpostconcussional symptoms for two weeks.Five weeks after the initial injury shereattended with persistent atypical chest pain.Three months later her visual acuity hadimproved on the left to 6/24, but remainedunchanged on the right, and a vitrectomy wascontemplated for that side.
DiscussionThis patient had the diagnostic triad of retinalhaemorrhages, subdural haematoma, and pat-terned bruising that is associated with forcefuland repeated shaking of infants. Such a triadhas previously been documented postmortemin a Palestinian adult who died under interro-gation by the Israeli security forces, and hasbeen described as the shaken adult syndrome.3
Even when the presenting history is misguid-ing, all injuries must be thoroughly docu-mented, and appropriate treatment instituted.Management also involves guiding the patientto autonomously decide whether to accept helpand/or legal assistance. In most states ofAmerica, it is mandatory to report domesticviolence related injuries, though the AmericanCollege of Emergency Physicians oppose this,stating that reporting should be in accordancewith the patient’s wishes.4 Confidentiality wasconsidered in this case, and gradual discussionbroke down the barriers of denial. Eventualadmission of domestic violence took three daysthough, a luxury not often available toemergency clinicians.
Early detection and documentation of inju-ries consistent with domestic violence must beattempted, and in this case, earlier documenta-tion of visual acuity would have facilitated anearlier diagnosis of retinal haemorrhage.
The diagnosis of “shaken adult syndrome”was eventually made, supported by delayeddiagnosis of some of the classical signs consist-ent with non-accidental injury.
Domestic violence victims are often dis-charged home the same day, thus losing thatwindow of opportunity to allow for intrinsicallymotivated acceptance of help. Not all A&Edepartments have access to their own observa-tion beds, though many departments are nowmanaging head injuries, especially now thatneurosurgical care has centralised to regionalcentres of excellence.
The way forward should be a more struc-tured method of follow up of suspected victimsof domestic violence that is initiated in theA&E department. As it is in suspected paediat-ric non-accidental injury, so one can preventrepeat episodes to not only the patient, but alsoto their children and other family members.The A&E department should grasp this initia-tive.
ContributorsThomas Carrigan, guarantor of the case report, initiated andcoordinated the collection of the clinical history, investigationconfirmation, and writing of the abstract.
Ed Walker was involved with interpretation of the case, back-ground research, and writing of the report. Dr Barnes wasinvolved with the critical revision of the report, and with thecollation of photographic evidence of the patient.
Conflict of interest: none.
Funding: none.
1 Hall C. One in four women face violence in the home. DailyTelegraph, 1 July 1998.
2 Department of Health NHS Executive. Domestic violence.London. Department of Health, 1997.
3 Pounder D. Shaken adult syndrome. Am J Forensic MedPathol 1997:18:321–4.
4 American College of Emergency Physicians. Mandatoryreporting of domestic violence to law enforcement andcriminal justice agencies. Ann Emerg Med 1997;30:561.
Airbag associated fatal head injury: case reportand review of the literature on airbag injuries
K Cunningham, T D Brown, E Gradwell, P A Nee
AbstractAirbags have been shown to significantlyreduce mortality and morbidity in motorvehicle crashes. However, the airbag, likethe seat belt, produces its own range ofinjuries. With the increasing use of air-bags in the UK, airbag associated injurieswill be seen more often. These are usuallyminor, but in certain circumstances se-vere and fatal injuries result. Such inju-ries have been described before in themedical literature, but hitherto mostreports have been from North America.This is the first case report from the UK ofserious injury due to airbag deploymentand describes the case of a driver who wasfatally injured when her airbag deployed
in a moderate impact frontal collisionwhere such severe injury would not nor-mally have been anticipated. The range ofairbag associated injuries is described andpredisposing factors such as lack of seatbelt usage, short stature, and proximity toairbag housing are discussed. The par-ticular dangers airbags pose to childrenare also discussed.(J Accid Emerg Med 2000;17:139–142)
Keywords: airbags; head injury
The introduction of airbags has led to a signifi-cant reduction in morbidity and mortality fromroad traYc accidents.1 2 However, the airbaglike the seat belt produces its own range of
Airbag associated fatal head injury 139
Whiston Hospital,Prescot, MerseysideL35 5DR: Departmentof Accident andEmergency MedicineK CunninghamT D BrownP A Nee
Department ofPathologyE Gradwell
Correspondence to:Dr Cunningham (e-mail:[email protected])
Accepted 10 November 1999
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from

injuries. In the case of the airbag this rangesfrom relatively minor injuries, such as abra-sions and superficial burns to unexpectedfatalities. Case reports of such fatalities haveappeared in the North American literaturesince 1993,3 4 but hitherto none have beenreported from the UK.
Case reportA 47 year old woman driving a 1997 registeredRover 414 at an estimated 19 mph wasinvolved in a head-on collision with a 13year old Opel Ascona driven at approximately27 mph. There was structural damage to thefront end and bonnet of the Rover but nosubstantial intrusion into the passengercompartment and the windscreen remainedintact. The driver of the Rover had beenwearing her seat belt and her airbag wasdeployed. She appeared to be unconscious inthe vehicle and the emergency services wereactivated by a passer-by. The driver of theOpel was a 21 year old male. His vehicle wasnot equipped with an airbag, but he had beenwearing his seat belt. He was uninjured apartfrom a cut lip and was ambulant at scene. Aparamedic crew arrived approximately 10minutes after the crash. The patient wasunresponsive during extrication and aGlasgow coma score of 3 was recorded atscene (no eye opening, no motor response topainful stimuli, and no vocalisation). She wasnoted to have Cheyne-Stokes respirations anda palpable radial pulse. She was intubated andintravenous access was established. Duringtransport to hospital the patient becameasystolic and advanced cardiac life supportwas initiated according to standardprotocols.5
On arrival in the emergency departmentthere were no signs of life and asystole wasapparent on the monitor. Bruising to the abdo-men and sternal area, and bleeding from bothears was noted. Resuscitation was continuedaccording to protocol for a further five minuteswithout success and the patient was declareddead.
A postmortem examination was carried outthe next day. There was horizontal bruising ofthe lower abdomen, abrasions of the left ante-rior iliac region, and bruising from the centralsternum to the left iliac region, all consistentwith a seat belt mark. In addition there was an8 cm diameter bruise in the middle of the ster-nal region. There was blood in both externalear canals and bruising of the nasal bridge. Noother major facial injuries were noted. Oninternal examination there was a fracture ofthe sternum at the junction of manubrium andbody, and fractures of the fourth to seventhleft ribs laterally. In the skull there was a largering fracture beginning just behind the pitui-tary fossa and extending through the righttemporal bone posteriorly to the midline 8 cmbehind the foramen magnum and anteriorlythrough the roof of the left temporal bone tothe origin. The anterior and middle cranialfossae on both sides were freely mobile aroundthis fracture. The brain showed diVuse swell-ing with blood in the subarachnoid space and
at the base of the brain. The spinal columnand nerve cord were normal. The immediatecause of death was deemed to have been asevere head injury.
The subject of this report was a middleaged woman of stout build, height 5' 7", weight92 kg. Crash investigators have postulated thatthe unexpectedly severe injuries sustainedwere caused by her sitting too far forwardwhen the airbag was deployed. As a result, thebag expanded suddenly into her chest andup towards the face, rather than the bodyimpacting with the fully expanded bag asintended by design. This lead to suddenforced hyperextension of the head and neckresulting in the base of skull ring fracture asdescribed.
DiscussionHISTORY AND DEVELOPMENT OF AIRBAGS
An airbag is a deflated balloon contained inthe steering wheel or dashboard, whichinflates rapidly on crash impact to cushion theoccupant from injury within the car. Inflationis triggered by a deceleration sensor, whichcan be situated in various sites such as thefront bumper or engine firewall. Triggering ofthe sensor activates a pyrotechnic device con-taining sodium azide that ignites producing alarge volume of nitrogen gas, which theninflates the airbag to a volume of about 30litres (Eurobag design) or about 70 litres (USfull size) within 50 msec. The airbag thendeflates almost immediately through vents inits lining. The timing of airbag inflation iscrucial. If it fires too soon, it will already bedeflating when the driver hits it, and will fail toprovide any protection. If it fires too late,the driver’s head will have already hit thesteering wheel or will impact with the balloon-ing bag.
The first automobile airbag patent was filedin 1949 and issued in 1953. Since then airbagdesign and operation has been continuallymodified and improved. Design alterationshave focused on such aspects as constituentmaterials, optimum bag size, inflation speed,and deployment threshold. However, it is onlyin the last decade that airbags have entered theUK car fleet in any significant numbers, andthe proportion of vehicles equipped withairbags still lags well behind that in NorthAmerica. Figures from the US show that in1995 over 70% of US made new cars had air-bags installed compared with 7% in 1989.Since 1998 car manufacturers in the US havebeen obliged to fit dual airbags in all new cars.The National Highway TraYc Safety Adminis-tration (NHTSA), a division of the USDepartment of Transportation, estimates thatbetween 1986 and October 1999 airbags havesaved 4758 lives (4011 drivers and 747 frontpassengers). This eVect has occurred mainly inthe last few years.1
AIRBAG ASSOCIATED INJURY
With the increasing prevalence of airbags inNorth America, reports began to appear in themedical literature there in the early 1990s ofinjuries related to airbag deployment.6 The
140 Cunningham, Brown, Gradwell, et al
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from

diVerent constituents of the airbag, propellantcapsule7 and chemicals,8 9 airbag modulecover,10 and the actual bag itself, have all beenimplicated in diVerent injuries. However, mostof the more serious injuries are caused by theact of deployment and are secondary to theshearing forces produced by the “punch-out”of the bag.11–13
The most commonly observed injuries areminor bruises and abrasions, mainly to theface, neck, and upper limbs.14 These are oftenreferred to as “bag slap” injuries. Some of thefirst reports were of eye injuries.6 The eye maybe injured by the fully deployed airbag causingcorneal abrasions, but more serious injuriessuch as retinal detachment and orbital blowout fractures can be sustained from an activelydeploying airbag.15–17 These injuries may beworse if the patient is wearing spectacles.18
Also, an alkaline chemical keratitis has beenreported from the combustion byproducts ofthe conversion of sodium azide to nitrogen.8
Superficial burns of the upper extremities,face, and neck are well documented,19 20 andfull thickness burns can also occur.21 Tempo-rary hearing impairment and tinnitus havebeen reported on a number of occasions.22 23
Upper limb injuries occur due to the proxim-ity of the forearm to the deploying airbag andare caused either by direct contact with theactivated bag, or by flinging the limb into inte-rior car structures.24–26 Fractures of the fore-arm are rare and are usually due to directimpact with the opening of the airbag modulecover.10
Minor chest injuries and rib fractures havebeen reported, and more serious thoracic inju-ries have occurred in comparatively low veloc-ity crashes. These include rupture of the rightatrium27 and aortic dissection.28 The aerosolsgenerated by airbag deployment have alsoinduced exacerbations of asthma in susceptibleindividuals.9
UNEXPECTED DEATHS
In recent years there have been a numberof reports of serious and fatal injuriesoccurring in low velocity crashes where theforces involved would not normally beexpected to cause serious harm.4 12 13 Also, theparticular dangers passenger airbags pose tochildren placed in the front seat have been welldocumented.29 30 The NHTSA Special CrashInvestigation Program has identified 146airbag related deaths to 1 October 1999,including 84 children, 18 of whom wereinfants in rear-facing infant seats.1 Wheninfants are restrained in rear-facing childseats in the front passenger seat, the headand neck are close to the airbag housing andtraumatic brain injuries occur after adirect blow from the rapidly inflating airbag.Children who are unrestrained or poorlyrestrained will often sit or stand too close tothe airbag when it deploys. Similarly, suchchildren can be thrown forwards towardthe airbag in pre-impact braking, and willbe in front of the deploying airbag atimpact.
Serious and fatal injury attributed to airbagshas previously been reported mainly fromNorth American centres. Thus far, few airbagrelated injuries have been reported from theUK and all have been relatively minor. Apartfrom the lower prevalence of airbags (whichwill change), there are a number of otherreasons for this. Firstly, in the UK seat beltusage is mandatory and uptake is thereforemuch greater than in some US states. As aresult, fewer British vehicle occupants relysolely on the protection aVorded by the airbag.Secondly, airbags here are somewhat diVerent.European airbags are designed primarily toprotect belted drivers from making head andface contact with the steering wheel. Conse-quently, our airbags are smaller (averagevolume 30–40 litres) and deploy with muchless force than the average US airbag (about70 litres). The US airbag is designed to protectunbelted occupants, and inflation to 70 litresoccurs within the same time frame (about 50msec)—a much more violent deployment. Afinal point is that traYc laws have been inplace here for some time which prohibitchildren from travelling unrestrained in thefront seat.
When an adult driver or passenger is in anatypical position there is a change in thepattern of deployment of the airbag.31 Ratherthan preventing injury, the airbag can causeinjury. This occurs primarily when the occu-pant is in the “deployment zone” of the airbag.Specifically, if the occupant is too near thesteering wheel, the lower part of expansion ofthe airbag is restricted by the chest leading notonly to excessive forces being applied to thethorax but also to a greater upward expansionof the bag. This can cause severe head andfacial injuries with hyperextension of the neckand cervical spine injury. Reasons for beingwithin the deployment zone include not wear-ing a seat belt (the commonest cause), sittingtoo close to the airbag housing (children andadults of short stature), and where deploy-ment has occurred after pre-crash braking (theoccupant having already been thrown forwardbefore the airbag was deployed). Theoccupant could also be within the deployment
Key messagesx Airbags significantly reduce morbidity
and mortality for adult drivers and frontseat passengers in motor vehicle crashes.
x Airbags can cause serious injury or deathif the occupant is too close to the airbagwhen it deploys.
x The risk of airbag associated injury canbe minimised if all drivers wore seat beltsand sat at least 10 inches from the airbaghousing.
x Children should never travel in the frontseat of an airbag equipped vehicle.
x More airbag associated injuries will beseen in the future and greater publicawareness on airbag benefits and hazardsis required.
Airbag associated fatal head injury 141
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from

zone if for some reason the airbag shouldfire late in the crash sequence. Basilar skullfractures as seen in our patient may not beuncommon in this context as illustrated by arecent report from Denmark of two similarcases.32 However, in both of these cases thedrivers were unbelted. Our patient waswearing a seat belt, and the exact contri-bution of individual factors (such as initialseating position and pre-crash braking)that were responsible for placing her tooclose to the expanding airbag are not certain.All of these cases reinforce the need foremergency physicians to be alert to the possi-bility of significant head and cervical spineinjuries in accidents of apparently moderateimpact, particularly if the patient is uncon-scious.
RECOMMENDATIONS AND FUTURE DEVELOPMENTS
Most airbag related adult deaths are prevent-able if the occupants use seat belts, and keep atleast a 10 inch distance between the airbagcover and the front of the chest. The vastmajority of drivers (including those of shorterstature) should be able to maintain thisdistance, and the NHTSA in the US now asksdrivers to measure the distance from the ster-num to the middle of steering wheel. If thisdistance is less than 10 inches then the drivercan apply to have the bag disconnected or anon/oV switch installed. The 10 inch distance is3 inches for initial activation, 5 inches of seatbelt “give”, and an extra 2 inches.
Airbag technology continues to evolve.Future advances include the development of“smart” airbags that will adjust to seat positionand passenger weight and height. Dual stageinflation systems (that is an initial reducedcharge of propellant fires the airbag only to beaugmented milliseconds later if a more severedeceleration is detected), side airbags, anddriver feet protection airbags are all beingdeveloped.
ConclusionsThe reduction in morbidity and mortality sinceairbags became widely available in new vehiclesis well established. This report, the first fatalinjury attributed to airbags reported in the UK,highlights the need to be aware of potentialhazards associated with their use. Vehicleoccupants should always wear seat belts andplace children in approved child restraints inthe rear of the vehicle. Drivers and passengers,who are unable to maintain the recommended10 inches from the airbag cover, should consultwith vehicle manufacturers over potential solu-tions including disabling of the airbag mech-anism.
We thank Julian Hill of Birmingham Accident Research Centrefor his comments on the paper and Dave Foulkes from the Mer-seyside Police Accident Investigation Unit for crash details.
ContributorsKC is the principal author and researched and wrote the paper.PN advised on and helped write the paper. TB treated thepatient, gathered some of the initial background information,and advised on the paper. EG provided the postmortem detailsand comment.
KC is the guarantor for the paper.
Conflict of interest: none.Funding: none.
1 National Highway TraYc Safety Administration (NHTSA).Special crash investigation program summary tables (http://www.nhtsa.dot.gov/people/ncsa/pdf/Summary.pdf).
2 Lund AK, Ferguson SA. Driver fatalities in 1985–1993 carswith airbags. J Trauma 1995;38:469–75.
3 Smock WS, Nichols GRD. Airbag induced fatal injuries: acase report. Proceedings of the 45th annual meeting of theAmerican Academy of Forensic Sciences. Boston, MA, Febru-ary 1993.
4 Jumbelic MI. Fatal injuries in a minor traYc collision. JForensic Sci 1995;40:492–4.
5 Advanced Life Support Group. Advanced cardiac life support,the practical approach. 2nd Ed. London: BMJ PublishingGroup, 1998.
6 Larkin GL. Airbag-mediated corneal injury. Am J EmergMed 1991;9:444–6.
7 Daniels RJ, Fulcher RA. An unusual cause of rib fracturefollowing a road traYc accident. J Accid Emerg Med 1997;14:113–4.
8 Smally AJ, Binzer A, Dolin S, et al. Alkaline keratitis: eyeinjury from airbags. Ann Emerg Med 1992;21:1400–2.
9 Gross KB, Goets MH, D’Arcy JB, et al. Mechanism ofinduction of asthmatic attacks initiated by the inhalation ofparticles generated by the airbag system deployment. JTrauma 1995;38:521–7.
10 Smock WS, Nichols GR. Airbag module cover injuries. JTrauma 1995;38:489–93.
11 Lau IV, Horsch JD, Viano DC, et al. Mechanism of injuryfrom air bag deployment loads. Accid Anal Prev 1993;25:29–45.
12 Brown DK, Roe EJ, Henry TE. A fatality associated with thedeployment of an automobile airbag. J Trauma 1995;39:1204–6.
13 Maxeiner H , Hahn M. Airbag-induced lethal cervicaltrauma. J Trauma 1997;42:1148–51.
14 Antosia RE, Partridge RA, Virk AS. Air bag safety. AnnEmerg Med 1995;25:794–8.
15 Cacciatori M, Bell RW, Habib NE. Blow-out fracture of theorbit associated with inflation of an airbag: a case report. BrJ Oral Maxillofac Surg 1997;35:241–2.
16 Duma SM, Kress TA, Porta DJ, et al. Airbag-inducedeye injuries: a report of 25 cases. J Trauma 1996;41:114–9.
17 O’Halloran HS, Draud K, Stevens JL. Primary enucleationas a consequence of airbag injury. J Trauma 1998;44:1090.
18 Gault JA, Vichnin MC, Jaeger EA, et al. Ocular injuriesassociated with eyeglass wear and airbag inflation. J Trauma1995;38:494–7.
19 Hallock GG. Mechanisms of burn injury secondary toairbag deployment. Ann Plast Surg 1997;39:111–3.
20 Baruchin AM, Jakim I, Rosenberg L, et al. On burn injuriesrelated to airbag deployment. Burns 1999;25:49–52.
21 Vitello W, Kim M, Johnson RM, et al. Full-thickness burn tothe hand from an automobile airbag. J Burn Care Rehabil1999;20:212–5.
22 Buckley G, Setchfield N, Frampton R. Two cases of possiblenoise trauma after inflation of airbags in low speed carcrashes. BMJ 1999;318:499–500.
23 Saunders JE, Slattery WH, Luxford WM. Automobileairbag impulse noise: otologic symptoms in six patients.Otolaryngol Head Neck Surg 1998;118:228–34.
24 Huelke DF, Moore JL, Compton TW, et al. Upper extrem-ity injuries related to airbag deployments. J Trauma1995;38:482–8.
25 Freedman EL, Safran MR, Meals RA. Automotive airbag-related upper extremity injuries: a report of three cases. JTrauma 1995;38:577–81.
26 Marco F, Garcia-Lopez A, Leon C, et al. Bilateral Smithfracture of the radius caused by airbag deployment. JTrauma 1996;40:663–4.
27 Lancaster GI, DeFrance JH, Borruso JJ. Airbag associatedrupture of the right atrium [letter]. N Engl J Med1993;328:358.
28 DeGuzman BJ, Morgan AS, Pharr WF. Aortic transectionfollowing airbag deployment. [letter]. N Engl J Med1997;337:573–4.
29 Hollands CM, Winston FK, StaVord PW, et al. Lethalairbag injury in an infant. Pediatr Emerg Care 1996;12:201–2.
30 HuV GF, Bagwell SP, Bachman D. Airbag injuries in infantsand children: a case report and a review of the literature.Pediatrics 1998;102:e2 (electronic article).
31 Walter DP, James MR. An unusual mechanism of airbaginjury. Injury 1996;27:523–4.
32 Hansen TP, Nielsen AL, Thomsen TK, et al. Avulsion of theoccipital bone—an airbag-specific injury. Lancet 1999;353:1409–10.
142 Cunningham, Brown, Gradwell, et al
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from
Anaphylaxis and monoamine oxidaseinhibitors—the use of adrenaline
M J Fenwick, C L Muwanga
AbstractA 67 year old woman taking a monoamineoxidase inhibitor (MAOI) presented to theaccident and emergency department withan anaphylactic reaction to flucloxacillin.This case highlights the uncertainty re-garding the use of adrenaline (epine-phrine) in the context of concurrentMAOI use. A summary of the evidence ispresented to clarify this.(J Accid Emerg Med 2000;17:143–144)
Keywords: adrenaline; monoamine inhibitors; anaphy-laxis
Case reportA 67 year old woman presented to the accidentand emergency (A&E) department with ahistory of collapse. She had taken two doses offlucloxacillin for a wound infection prescribedby her general practitioner who was unaware ofher previous penicillin allergy. She was alsotaking phenelzine 15 mg for depression. Oninitial examination she was flushed and agi-tated. She had a tachycardia of 120 beats/min,a blood pressure of 200/120 mm Hg, a respira-tory rate of 20 breaths/min, and an oxygensaturation of 98% on air. She had a swollentongue with no stridor. An anaphylacticreaction was diagnosed. The safety and use ofadrenaline (epinephrine) was debated in viewof the potential drug interaction betweenmonoamine oxidase inhibitors (MAOIs) andsympathomimetic drugs. She was treated withoxygen and intravenous (IV) hydrocortisone200 mg, IV chlorpheniramine 10 mg, and IVranitidine 50 mg. After 30 minutes she deterio-rated, developing stridor that required intuba-
tion. During preparation for intubation andbefore any induction agents were used herblood pressure dropped to 80/20 and herstridor worsened. It was decided to give heradrenaline and after two boluses of 0.1 mg IV,she rapidly improved. Intubation was achievedeasily after gaseous induction of anaesthesiaand she was admitted to the intensive care unit.She was extubated the next day and dischargedhome four days later with no sequelae.
DiscussionAdrenaline is the treatment of choice in severeanaphylactic reactions,1 2 however there is con-troversy over the use of adrenaline in patientstaking MAOIs. Phenelzine is a non-selectiveirreversible MAOI3 4 and is known to have dan-gerous interactions with certain foodstuVs anddrugs. These include hypertensive crises withsympathomimetic drugs and central excitatorysyndromes with tyramine containing foods.5–7
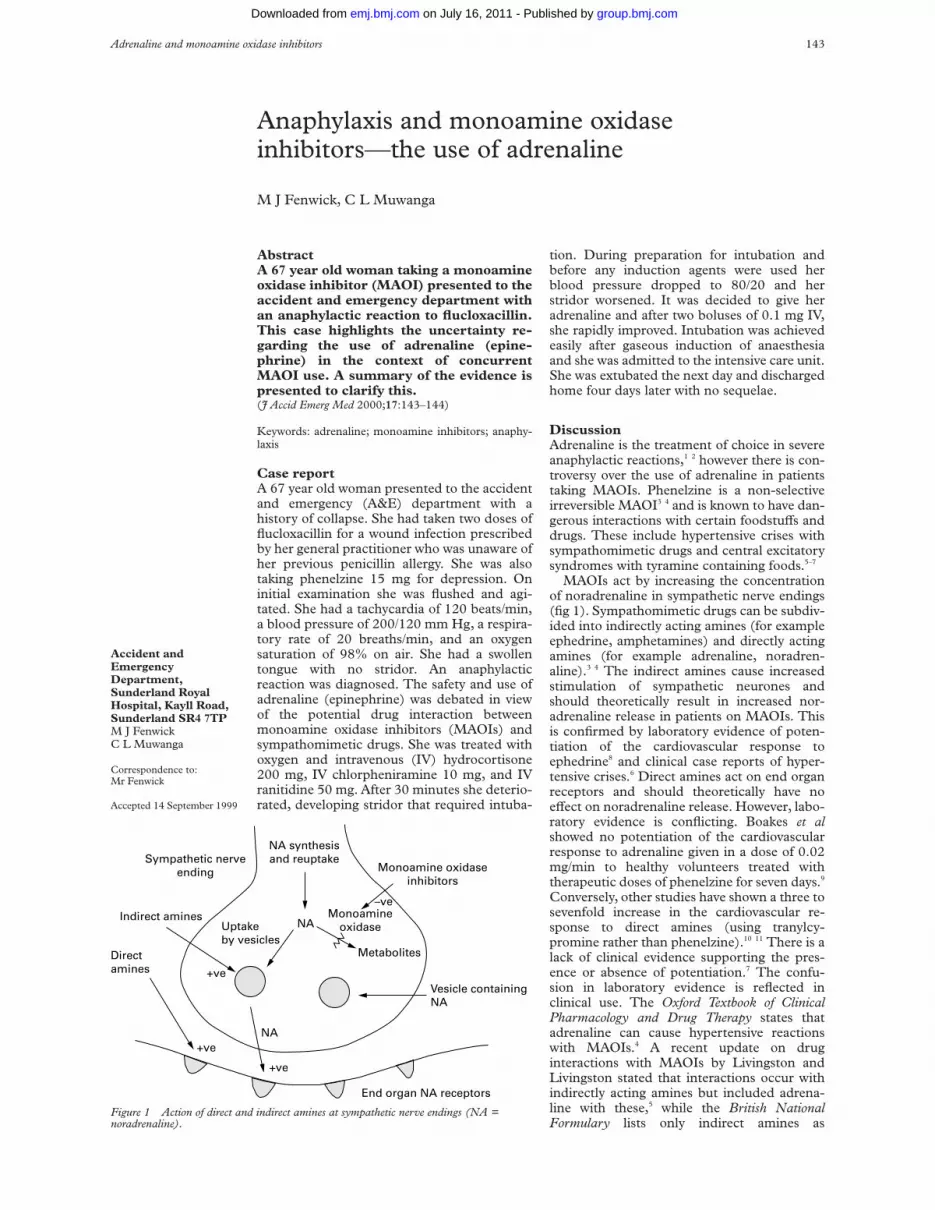
MAOIs act by increasing the concentrationof noradrenaline in sympathetic nerve endings(fig 1). Sympathomimetic drugs can be subdiv-ided into indirectly acting amines (for exampleephedrine, amphetamines) and directly actingamines (for example adrenaline, noradren-aline).3 4 The indirect amines cause increasedstimulation of sympathetic neurones andshould theoretically result in increased nor-adrenaline release in patients on MAOIs. Thisis confirmed by laboratory evidence of poten-tiation of the cardiovascular response toephedrine8 and clinical case reports of hyper-tensive crises.6 Direct amines act on end organreceptors and should theoretically have noeVect on noradrenaline release. However, labo-ratory evidence is conflicting. Boakes et alshowed no potentiation of the cardiovascularresponse to adrenaline given in a dose of 0.02mg/min to healthy volunteers treated withtherapeutic doses of phenelzine for seven days.9
Conversely, other studies have shown a three tosevenfold increase in the cardiovascular re-sponse to direct amines (using tranylcy-promine rather than phenelzine).10 11 There is alack of clinical evidence supporting the pres-ence or absence of potentiation.7 The confu-sion in laboratory evidence is reflected inclinical use. The Oxford Textbook of ClinicalPharmacology and Drug Therapy states thatadrenaline can cause hypertensive reactionswith MAOIs.4 A recent update on druginteractions with MAOIs by Livingston andLivingston stated that interactions occur withindirectly acting amines but included adrena-line with these,5 while the British NationalFormulary lists only indirect amines as
Figure 1 Action of direct and indirect amines at sympathetic nerve endings (NA =noradrenaline).
Sympathetic nerveending
Indirect amines
Direct amines
+ve
+ve
End organ NA receptors
Vesicle containing NA
NA
+ve
Uptakeby vesicles
NAMonoamine
oxidase
Metabolites
–ve
Monoamine oxidaseinhibitors
NA synthesisand reuptake
Adrenaline and monoamine oxidase inhibitors 143
Accident andEmergencyDepartment,Sunderland RoyalHospital, Kayll Road,Sunderland SR4 7TPM J FenwickC L Muwanga
Correspondence to:Mr Fenwick
Accepted 14 September 1999
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from

contraindications with MAOIs.12 Stockley re-views the evidence and concludes that adrena-line should be used with caution withMAOIs.13
ConclusionThere is confusion by clinicians as to the safetyof adrenaline with MAOIs. It is likely that likeus, clinicians are often unaware that it isindirectly acting amines that are usually impli-cated in hypertensive crises with MAOIs.However, the evidence for the safety of adrena-line in the doses used frequently in clinicalsituations is lacking. We recommend cautionwith the use of adrenaline in patients takingMAOIs, but that its use in life threatening situ-ations is not contraindicated.
ContributorsM J Fenwick initiated and wrote the paper and performed theliterature search. C L Muwanga discussed the idea and editedthe paper.
M J Fenwick is the guarantor of this paper.
Conflict of interest: none.
Funding: none.
1 Brown AFT. Therapeutic controversies in the managementof acute anaphylaxis. J Accid Emerg Med 1998;15:89–95.
2 Fisher M. Treatment of acute anaphylaxis. BMJ 1995;311:731–3.
3 Hardman JG, Limbird LE, eds. Goodman and Gillman’s thepharmacological basis of therapeutics. 9th Ed. New York:McGraw-Hill, 1996: 442–6.
4 Graham-Smith DG, Aronson JK. Oxford textbook of clinicalpharmacology and drug therapy. 2nd Ed. Oxford: OxfordUniversity Press, 1992:639.
5 Livingston MG, Livingston HM. Monoamine oxidaseinhibitors-an update on drug interactions. Drug Saf1996;14:219–27.
6 Dawson JK, Earnshaw SM, Graham CS. Dangerousmonoamine oxidase inhibitor interactions are still occur-ring in the 1990s. J Accid Emerg Med 1995;12:49–51.
7 Blackwell B. Monoamine oxidase inhibitor interactions withother drugs. J Clin Psychopharmacol 1991;11:55–9.
8 Elis J, Laurence DR, Mattie H, et al. Modification bymonoamine oxidase inhibitors of the eVect of somesympathomimetics on blood pressure. BMJ 1967;ii:75–8.
9 Boakes AJ, Laurence DR, Teoh PC, et al. Interactionsbetween sympathetic amines and antidepressant agents inman. BMJ 1973;i:311–5.
10 Cuthbert MF, Vere DW. Potentiation of the cardiovasculareVects of some catecholamines by a monoamine oxidaseinhibitor. Br J Pharmacol 1971;43:471–2.
11 Horwitz D, Goldberg LI, Sjoerdsma A. Increased bloodpressure responses to dopamine and norepinephrineproduced by a monoamine oxidase inhibitor. J Lab ClinMed 1960;56:747.
12 British Medical Association and the Royal PharmaceuticalSociety of Great Britain. British national formulary.London: British Medical Association and the RoyalPharmaceutical Society of Great Britain, 1998;34:568.
13 Stockley IH. Drug interactions. 4th Ed. London: Pharmaceu-tical Press, 1996: 668–9.
Prolonged coma due to cerebral fat embolism:report of two cases
Leonidas Gregorakos, Katerina Sakayianni, Despina Hroni, Victoria Harizopoulou,Nikos Markou, Fani Georgiadou, Maria Adamidou
AbstractFat embolism syndrome remains a rare,but potentially life threatening complica-tion of long bone fractures. The true inci-dence is diYcult to assess as many casesremain undiagnosed. Cerebral involve-ment varies from confusion to encepha-lopathy with coma and seizures. Clinicalsymptoms and computed tomography arenot always diagnostic, while magneticresonance imaging is more sensitive in thedetection of a suspected brain embolism.Two cases of post-traumatic cerebral fatembolism, manifested by prolonged comaand diVuse cerebral oedema, are pre-sented. The clinical course of the diseaseas well as the intensive care unit manage-ment are discussed.(J Accid Emerg Med 2000;17:144–146)
Keywords: cerebral fat embolism; fat embolism syn-drome; coma
Fat embolism syndrome (FES) remains a rare,but potentially life threatening complication oflong bone fractures, characterised by pulmo-nary insuYciency, neurological dysfunction,fever and petechial rash, usually occurring dur-ing the first 48 hours after injury.1 The trueincidence of this syndrome cannot be accu-
rately assessed as many subclinical formsremain unrecognised. It varies from 0.5% to30% of fractured patients2 with higher rates inmultiply injured patients and presents a meanmortality rate of 10%.3 Cerebral involvementhas been frequently reported and seems toaggravate the prognosis of FES.4 Clinicalmanifestations vary widely, from a simplealteration of vigilance (70%–85% of the cases),to seizures and coma.2 We present two cases ofpost-traumatic cerebral fat embolism, mani-fested by prolonged coma and diVuse cerebraloedema.
Case reportsCASE 1An 18 year old man who sustained an open frac-ture of the left tibia but no head injury, after amotorbike accident, was admitted to the emer-gency room of our hospital. Upon admission thepatient was alert, oriented, normotensive, andeupnoeic. Neurological examination showed noabnormalities. Two hours later, external fixationof his fracture was performed under generalanaesthesia. After complete recovery from an-aesthesia he was transferred to the orthopaedicdepartment; he was haemodynamically stableand had a normal respiratory pattern. Twelvehours postoperatively he developed signs ofFES including fever (>39°C), tachycardia,
144 Gregorakos, Sakayianni, Hroni, et al
Intensive Care Unit,Athens TraumaHospital, Athens,GreeceL GregorakosK SakayianniD HroniV HarizopoulouN MarkouF GeorgiadouM Adamidou
Correspondence to:Dr L Gregorakos, 51 AgiasSofias Str, 10444 Athens,Greece
Accepted 28 September1999
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from

petechiae over the shoulder area, hypoxaemia,oliguria, and thrombocytopenia. Six hourslater he was unconscious, responding only topainful stimuli. Neurological examinationdemonstrated a Glasgow coma score of 5 (eyeopening 1, motor response 3, verbal response1), and a normal reaction of both pupils tolight. An immediate endotracheal intubationwas performed because of unconsciousnessand respiratory insuYciency. The patient wastransferred to the intensive care unit (ICU)and mechanical ventilation initiated. Chestradiography on ICU admission demonstrateddiVuse pulmonary infiltrates. Cerebral com-puted tomography, performed shortly aftermental status deterioration, revealed diVusebrain oedema. Antioedema treatment wasinstituted, and mild hypocapnia was induced.Retinal examination performed on day 2 dem-onstrated characteristic cottonwool spotsacross the vascular beds, which are indicativeof fat embolism. Magnetic resonance imaging(MRI), performed on day 3 showed multipleareas of increased intensity in the cerebralwhite matter, which confirmed the diagnosisof cerebral fat embolism. The patient re-mained under mechanical ventilation, generalsupportive care in the ICU, and regularneurosurgical evaluation. High doses ofmethylprednisolone (30 mg/kg/8 hours intra-venously) were administered for three doses,followed by prednisolone 50 mg/day, intrave-nously, tapering oV after one week. A trache-ostomy was performed and mechanical venti-lation continued for 22 days. Thereafter, hewas breathing spontaneously through thetracheostomy. One month after initial admis-sion he started opening his eyes to intensestimuli, and computed tomography showedresolution of cerebral oedema. The tracheos-tomy tube was removed on the 35th day ofhospitalisation, by which time he had aprogressive resumption of consciousness andimproving responsiveness to external stimuli.He was in the ICU for six weeks, and his entirehospital stay after the accident was twomonths. He was discharged from the hospitalwithout any neurological sequelae. MRI per-formed before discharge detected no abnor-malities.
CASE 2A 20 year old man sustained bilateral closedtibia fractures and abdominal trauma after atraYc accident. Upon his admission to theemergency room no signs of craniocerebralinjury were present. Neurosurgical examina-tion detected no neurological abnormalities,with a Glasgow coma score of 15. Blood pres-sure was 140/90 mm Hg and heart rate 120beats/min. As indicated by intraperitoneal lav-age, an urgent laparotomy was performed,which showed rupture of the mesenterium.Limited small intestine resection and entero-entero anastomosis were performed. At thesame time the patient underwent closed reduc-tion and cast immobilisation of his fractures.After surgical intervention and complete re-covery from anaesthesia, the patient was trans-ferred extubated to the ICU. Six hours after
admission the patient had a fever (39oC),became cyanotic, comatose, and had seizures.His Glasgow coma score was 4 (eye opening 1,motor response 2, verbal response 1), whilepupils were equal in size and reactive to light.He was immediately intubated and mechani-cally ventilated. In addition, signs of systemicfat embolism, such as tachycardia, conjunctivalpetechiae, hypoxaemia, and diVuse pulmonaryinfiltrates on chest radiography, were present.Laboratory analysis revealed thrombocytope-nia and anaemia. Arterial blood gas analysisshowed a partial oxygen tension of 7.73 kPa(58 mm Hg) and partial carbon dioxidetension of 4.27 kPa (32 mm Hg).
On day 2, computed tomography of thebrain showed diVuse cerebral oedema, withoutany change in neurological status. He remainedunder mechanical ventilation for 15 days,receiving the same treatment as case 1. MRIwas performed on day 5, which showed diVusehigh intensity lesions in the subcortical andperiventricular white matter. During his stay atthe ICU he suVered two episodes of nosoco-mial pneumonia. Serial blood culture and pro-tected brush specimen cultures were obtained.Pseudomonas aeruginosa was isolated frombronchoalveolar lavage fluid and an appropri-ate antibiotic treatment was given, according tosensitivity. He was extubated on day 15 andwas transferred to the neurosurgical depart-ment five days later with moderate disorienta-tion. MRI of the brain on day 25 demonstrateda substantial resolution of the previous hyper-intense lesions. He was finally discharged fromthe hospital 35 days after the accident withoutany neurological deficit.
DiscussionFES with fat droplets larger than 8 µm indiameter occurs in more than the 90% ofpatients with long bone fractures. This syn-drome denotes clinical or subclinical respira-tory insuYciency, and usually runs a mildcourse and responds well to measures for ven-tilatory support.1 In our patients the diagnosiswas established by Gurd’s criteria,5 the charac-teristic fat globules on retinal examination, andthe findings on brain computed tomographyand MRI. There are two theories explainingthe pathogenesis of FES. According to the“mechanical” theory, free fat particles from thebone marrow enter torn vein sinusoids at thesite of the fracture and embolise the pulmonaryarterioles. The “chemical” theory suggests thatfat emboli arise from plasma fat when, throughsome type of systemic stimulus associated withtrauma and other medical conditions, chylomi-crons coalesce and fuse to form larger fatglobules.5 Victims of the fulminant form of thesyndrome on postmortem examination presentocclusion of small blood vessels by fat emboliwith areas of brain microinfarction andhaemorrhage.6 7 Due to cerebral fat emboli, thebrain often appears oedematous and shows aninflammatory reaction while the numerouspetechiae can cover the surface of the brain.8
Endothelial damage results from toxic freefat and capillary obstruction by fat globules
Cerebral fat embolism 145
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from

with associated platelet aggregation, release ofvasoactive substances, and development ofcoagulopathy.9
The presence or the reopening of a patentforamen ovale and a right to left shunt due topulmonary hypertension is associated with anincreased risk for systemic manifestations ofFES.10 However, several studies have failed todemonstrate any intracardiac shunts in pa-tients suVering from this syndrome.8 11 Pub-lished studies remain undecided whether apatent foramen ovale or other intracardiacdefects are prerequisites for the development ofcerebral symptoms.
Our patients are characteristic cases ofcerebral fat embolism, which was followed by asevere course of disease in the ICU. Theyresponded to conventional treatment andadministration of corticosteroids. Among sev-eral pharmacological treatments, only steroidshave proved to be beneficial in the prophylaxisand treatment of FES, both in high and lowdoses.12–14 The mode of action has not beenelucidated, but seems to be related to theiranti-inflammatory and antiadhesive eVects.
The long stay in the ICU was due to theincreased intracranial pressure, following cer-ebral oedema. These cases suggest that cer-ebral oedema plays a major part in theneurological deterioration in the fulminanttype of FES and that cerebral computedtomography is indicated in such patients.15
Computed tomography is also useful inexcluding traumatic cerebral involvement inmultiple trauma patients presenting with dete-rioration in their mental state, but is notspecific for the diagnosis of cerebral fatembolism.16 MRI is a better diagnostic tool forthe confirmation of brain embolism, as it ismore sensitive in the detection of degenerativeand vascular injuries and non-haemorrhagiccontusion. In addition, it seems to correlatewell with the clinical neurological course.17 18
The patients described above, despite theinitial severe neurological syndrome and pro-longed coma, had complete cerebral recovery.Several studies report that cerebral dysfunctionassociated with FES appears to be reversible inthe majority of the cases, so physicians shouldnot give up hope even in the most severe formsof the syndrome.8 10 11 19 It is likely that fatemboli of very small diameter cause reversibleischaemia and transient perivascular oedema,allowing recovery from cerebral dysfunction.17
Cerebral fat embolism should always be sus-pected when severe neurological dysfunctionappears in a patient with long bone fractures,in the absence of an initial major head injury.Although the diagnosis may be straightforwardin patients with isolated long bone fractures, itmay be diYcult in the multiple trauma patientwith head injury or under sedation. Inaddition, hypoxia may be associated withpulmonary contusion and infection and pe-techiae may occur after blood transfusion.
Many authors have suggested that early openreduction and surgical stabilisation of longbone fractures may reduce the incidence ofFES.2 10 Repeated manipulation of the frac-tured fragments may further stimulate therelease of bone marrow fat into thecirculation.10 Similarly, the type of surgicalfixation seems to influence the incidence of fatembolisation. External fixation and plate osteo-synthesis have several advantages comparedwith intramedullary nailing techniques, whichfurther increase intramedullary pressure andpromote fat emboli release.10 20 However, thesyndrome is frequently observed despiteprompt surgical intervention.
As pathophysiology of the syndrome stillremains obscure, attention should be paid toprevention and early recognition of this entity.Optimal immobilisation, adequate fluid andblood replacement, meticulous monitoring,and use of steroids are principles commonlyaccepted in current treatment.2 10
ContributorsAll of the authors listed above have contributed substantially tothe collection of data and writing of the paper.
Leonidas Gregorakos is the guarantor for the paper.
Conflict of interest: none.
Funding: none.
1 Fulde GW, Harisson P. Fat embolism: a review. Arch EmergMed 1991;8:233–9.
2 Estèbe JP. Des emboles de graisse au syndrome d’emboliegraisseuse. Ann Fr Anesth Reanim 1997;16:138–51.
3 Fabian TC, Hoots AV, Stanford DS, et al. Fat embolismsyndrome: prospective evaluation in 92 fracture patients.Crit Care Med 1990;18:42–6.
4 Jacobson TM, Terrence CF, Reinmuth OM. The neurologicmanifestation of fat embolism. Neurology 1986;36:847–51.
5 Gurd AR. Fat embolism: an aid to diagnosis. J Bone JointSurg Br 1970;52:732–7.
6 Findlay M, DeMajo W. Cerebral fat embolism. Can MedAssoc J 1984;131:755–7.
7 Meeke RI, Fitzpatrick GJ, Phelan DM. Cerebral oedemaand fat embolism syndrome. Intensive Care Med 1987;13:291–2.
8 Needham AP, McLean AS, Stewart DE. Severe cerebral fatembolism. Anaesth Intensive Care 1996;24:502–4.
9 Erdem E, Namer IJ, Saribas O, et al. Cerebral fat embolismstudied with MRI and SPECT. Neuroradiology 1993;35:199–201.
10 Ten Duis HJ. The fat embolism syndrome. Injury 1997;28:77–85.
11 Ibanez CN, Collado NR, Gavina SI, et al. Fat embolismsyndrome without respiratory failure. Clinical Intensive Care1999;10:101–3.
12 Kallenbach J, Lewis M, Zaltzman M, et al. Low-dosecorticosteroid prophylaxis against fat embolism. J Trauma1987;27:1173–6.
13 Gregorakos L, Dimopoulos G, Mavropanou D, et al. Fatembolism syndrome in traumatized patients: a five yearexperience of a single intensive care unit. AppliedCardiopulmonary Pathophysiology 1996;6:105–9.
14 Schonfeld SA, Ploysonsang Y, Dilisio R, et al. Fat embolismprophylaxis with corticosteroids: a prospective study inhigh risk patients. Ann Intern Med 1983;99:438–43.
15 Sakamoto T, Sawada Y, Yukioka T, et al. Computed tomog-raphy for diagnosis and assessment of cerebral fatembolism. Neuroradiology 1983;24:283–5.
16 Citerio G, Bianchini E, Beretta L. Magnetic resonanceimaging of cerebral fat embolism: a case report. IntensiveCare Med 1995;21:679–81.
17 Satoh H, Kurisu K, Ohtani M, et al. Cerebral fat embolismstudied by magnetic resonance imaging, transcranial Dop-pler sonography, and single photon emission computedtomography: case report. J Trauma 1997;43:345–8.
18 Vincetti-Rouquette I, David H, Borne M, et al. Intérêt del’IRM dans l’embolie graisseuse cérébrale. Ann Fr AnesthReanim 1998;17:278–80.
19 Scopa M, Magatti M, Rossitto P. Neurologic symptoms infat embolism syndrome. J Trauma 1994;36:906–8.
20 Christie J, Robinson CM, Pell AC, et al. Transcardiac echo-cardiography during invasive intramedullary procedures. JBone Joint Surg Br 1995;77:450–5.
146 Gregorakos, Sakayianni, Hroni, et al
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from

Air rifle injury to the oropharynx. The essentialrole of computed tomography in deciding onsurgical exploration
T Hung, P Huchzermeyer, A E Hinton
AbstractGunshot wounds specific to the orophar-ynx are extremely rare with no reportedcases of such injury in the world litera-ture. The importance of such cases restson the use of modern imaging techniquesincluding computed tomography, mag-netic resonance imaging, and vascularimaging in the making of managementdecisions and particularly in deciding theneed for exploration of such an injury. Inour case a conservative approach wasadopted in view of the computed tomogra-phy finding and the stable clinical condi-tion of the patient.(J Accid Emerg Med 2000;17:147–148)
Keywords: oropharynx; gunshot wound
Gunshot injuries and fatalities are common inthe United States where the firearm regula-tions are more lenient than those of the UK.However there has been a surge of gunshotincidents in the UK in recent years whenincreasing violence in the media and the dein-stitutionalisation of mental patients were con-tributory factors. Air rifles may be possessedwithout a certificate in the UK if they are not oftype declared dangerous by the Firearms Rules1969. An air rifle should discharge a pellet witha kinetic energy below 16.3 J (12 ft lb). Abovethese levels the weapon is classified as a firearmunder section 1 of the Firearm Act 1968. Airrifle injuries can range from trivial to fataldepending on the site of injury and the vascu-lar damage. The majority of entry woundsreported in the literature are external. Wereport the first case in which our patient has anintraoral entry wound. The use of emergencycomputed tomography was essential in thelocalisation of the pellet and the formulation ofa management plan.
Case reportA 22 year old man claimed to have accidentallytriggered his air rifle, which was aiming at hisopen mouth. He sustained a gunshot wound tohis oropharynx. There was a minimal amountof bleeding from his oral cavity. He did notcomplain of any breathing diYculty. Hecomplained only of discomfort of the left sideof his throat and neck.
He looked remarkably calm on arrival at theaccident and emergency department. Therewas no stertor or stridor. His cardiovascularstatus was stable. His oxygen saturation was99% on air throughout the admission. Therewas minimal swelling and tenderness of the left
upper anterior triangle of his neck. Surgicalemphysema was not elicited. A 1 cm entrywound was noted at the middle portion of theanterior faucial pillar. Flexible pharyngoscopyrevealed a bloodstained tongue base but noactive haemorrhage. The airway was com-pletely patent.
The soft tissue neck radiograph showed aradio-opaque pellet just anterior to the base ofthe odontoid peg (figs 1 and 2). The emer-gency computed tomogram of the neck showedthe metallic pellet lying in the prevertebral softtissues anterior to the transverse process of thesecond cervical vertebra (fig 3). The pellet wasfound to lie within 1 cm of and medial to theleft internal carotid artery.
The patient was treated with intravenouscefotaxime and metronidazole prophylacti-cally. Oral intake was started after 24 hours ofclose observation. He was discharged on thethird day in view of satisfactory aerodigestivefunction. The decision was made againstretrieval of the pellet by surgical exploration asthe procedure could be more hazardous thanthe risks of leaving the pellet undisturbed Thepatient was reviewed after two months without
Figure 1 Lateral soft tissue neck radiograph showing thepellet anterior to the odontoid peg.
Figure 2 Posteroanterior neck radiograph showing thepellet in the anterolateral soft tissue of the neck.
Air rifle injury to the oropharynx 147
Department ofOtolaryngology,St George’s Hospital,LondonT HungP HuchzermeyerA E Hinton
Correspondence to:Mr Terry Hung, SeniorHouse OYcer, 16 StClements Mansions, LillieRoad, Fulham, London SW67PG(e-mail: [email protected])
Accepted 14 September 1999
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from

any sequelae. As the pellet was thought to bean iron alloy, he was warned against enteringany strong electromagnetic field includingmagnetic resonance scanning. He will betreated expectantly if complications arise.
DiscussionIt is estimated that one person each year diesfrom an air powered weapon injury in the UK.1
Fatalities and injuries are most commonlyaccidents, but deliberately inflicted injuries dooccur. Airguns are dangerous weapons wheninappropriately handled and should not beconsidered as toys. Basic ballistics verifies thata projectile’s potential to disrupt tissue isdetermined by both its mass and its velocity.Modern day pneumatic rifles allow the genera-tion of muzzle velocities of up to 350 feet persecond. Speeds of 150 feet per second and 200feet per second are required for skin penetra-tion and bone penetration, respectively.2 Apressure wave follows the projectile with thecreation of a “temporary cavity” which couldhave a significant wounding mechanism. In-elastic tissues such as liver are far more suscep-tible to disruption by the temporary cavity thanare more flexible body tissue such as muscle,bowel wall, and lung.3 Nichols and Sens usedcytological technique to analyse direct ballistictrauma in several tissue type, most notably inmuscular tissue.4 Progressive damage to skel-etal and cardiac muscle was seen in multiplepreparations. This ranged from partial separa-tion of the fascicles to cytoplasmic homogeni-sation and nuclear rupture.
Most of the world literature described exter-nal gunshot wounds of the head, chest,abdomen, and the extremities. Only twobizarre and fatal cases of gunshot injuries
involving the human orifices were reported,namely intrarectal and intranasal routes.5 6
Both patients described had past psychiatrichistory. Our patient is the first case recordedwith gunshot injury via an intraoral route andhe denied such a past psychiatric history.
The first priority in the management of gun-shot injury to the head and neck region shouldalways be the securing of the airway, breathing,and circulation. There is little disagreement inthe literature about how to treat penetratingprojectile wounds of the chest and abdomen orthose that disrupt major blood vessels or bone.Ironically, most of the dispute concernstreatment of the least lethal injuries and how tomanage the soft tissue disruption.
Pathology of the oropharynx, unlike theirexternal counterpart is notoriously diYcult tovisualise in the emergency situation. Systemicsigns are only a rough guide to the progressionof complications. Acute radiological evaluationof gunshot wounds has been established inother organs.7 Imaging is most important in thedefinitive management of gunshot injuries tothe head and neck. The soft tissue neck radio-graph is only a rough guide to the anatomicalposition of the pellet. It reveals insuYcientdetails of the soft tissue anatomy. Computedtomography allows much more accurate locali-sation of the pellet in respect to the importantanatomical structures. In fact Milroy et al hadsuccessfully located both the pellet and thefragments using computed tomography.1 Con-trast enhancement allows relatively preciselocalisation of the pellet in respect of the mainblood vessels, the left internal carotid artery inour case. The use of emergency computedtomography was essential as it gave us reassur-ance of the integrity of the vasculature and itallowed us to adopt a conservative manage-ment approach in this emergency senario.
The decision of non-retrieval of the pellet ona definitive basis was an exercise of riskmanagement. Surgical access of the orophar-ynx will require the commando approach whenmandibulectomy is performed.8 This proce-dure has a very high morbidity.
Conflict of interest: none.
Funding: none.
1 Milroy CM, Clark JC, Carter N, et al. Air weapon fatalities.J Clin Pathol 1998;51:525–9.
2 Ford EG, Senac MO, McGrath N. It may be moresignificant than you think: BB air rifle injury to a child’shead. Pediatr Emerg Care 1990;6:278–9.
3 Fackler ML. Gunshot wound review. Ann Emerg Med 1996;28:194–203.
4 Nichols CA, Sens MA. Cytologic manifestations of ballisticinjury. J Clin Pathol 1991;95:660–9.
5 Prahlow JA. Suicide by intrarectal gunshot wound. Am JForensic Med Pathol 1998;19:356–61.
6 Lee KA, Opeskin K. Gunshot suicide with nasal entry.Forensic Sci Int 1995;71:25–31.
7 Phiilips CD. Emergent radiologic evaluation of the gunshotwound victim. Radiol Clin North Am 1992;30:307–24.
8 DeSanto LW, Whicker JH, Devine KD. Mandibularosteotomy and lingual flaps: use in patient with cancer ofthe tonsil area and tongue base. Archives of Otolaryngoloy1975;101:652.
Figure 3 Contrast enhanced computed tomogram showingthe metallic pellet (large arrow) lying to the left of themidline in the prevertebral soft tissue anterior to thetransverse process of the axis (small arrow shows leftinternal carotid artery).
148 Hung, Huchzermeyer, Hinton
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from

A useful form of glue ear
J R Benger, P H Davies
AbstractChildren and adults commonly present tothe emergency department with a foreignbody lodged in the ear. Over the past 15years techniques for cyanoacrylate (“su-perglue”) assisted foreign body removalhave been described, but are not widelyemployed. Two cases of successful and oneof unsuccessful removal using this tech-nique are reported, and some advice isoVered to aid others.(J Accid Emerg Med 2000;17:149–150)
Keywords: child; cyanoacrylate; ear; foreign body
Foreign body within the ear is a commonproblem presenting to emergency depart-ments. Most patients are inquisitive children inthe 2 to 8 age group,1 but adults can alsopresent in this way.2 Patients are more com-monly male and of low socioeconomic status.3
During a recent 12 month period 74 patients(representing approximately one in 500 newattendances) presented to our emergencydepartment with a foreign body lodged in theear. Of these 30 (41%) were adults and 44(59%) children. This rate is rather more thanthat of one in 1792 new patient registrationsreported from the John Hopkins emergencydepartment in 1987.3
Many diVerent techniques have been advo-cated for the removal of foreign bodies lodgedin the ear,4 though very few of these have beenformally assessed in any scientific way, relyingmore on anecdote and experience.5
We report two cases of successful and one ofunsuccessful removal of a foreign body fromthe external auditory canal using cyanoacrylate“superglue”, and make some further observa-tions based upon our experiences.
Technique for removalIn the following cases we used a blunt plasticstick, such as that contained in a “cotton bud”.The cotton wool was removed and a smallamount of cyanoacrylate glue applied. Thiswas then introduced into the ear under directvision until the foreign body was contacted. Adrying time of 30 to 60 seconds was allowed,after which the foreign body was extracted witha smooth, pulling motion.
Case reportsCASE 1A general practitioner referred a 60 year oldwoman with an asymptomatic foreign body inher ear. Removal was initially attempted withforceps, but the patient found this too painful.Instead the foreign body was removed easilyusing cyanoacrylate glue.
CASE 2A 17 year old woman placed a plastic pearl inher right ear and was unable to remove it. Inthe emergency department the pearl was easilyvisualised and removed using cyanoacrylateglue (see fig 1).
CASE 3A 4 year old girl pushed a plastic bead into herear. The bead was visualised deep within theear canal, but several attempts at removal usingcyanoacrylate glue failed due to a lack ofpatient cooperation and the plastic stickbecoming detached from the bead. The patientwas referred for removal under general anaes-thesia.
DiscussionThe first reported use of glue to remove a for-eign body from the ear was published in 1977.6
This described two successful cases in which ageneral purpose adhesive was applied to theend of a flexible plastic rod. Three subsequentreports using cyanoacrylate glue have beenpublished, the earliest in 1984.7 In 1989 Prideand Schwab claimed the first reported use ofcyanoacrylate glue for the successful removalof a foreign body from the ear, and suggestedthat a larger series would be helpful.8 Fouryears later Hanson and Stephens successfullyapplied this technique to the nose and ear of a3 year old girl and 14 year old boy respectively,9
but beyond this no further information orevaluation has been published.
Though it is clear that cyanoacrylate extrac-tion of foreign bodies can be highly successful,the eYcacy of this technique in relation to themany others available remains uncertain. It islikely to be most useful in extracting hard,spherical objects such as those describedabove. These are diYcult to remove withforceps, but may be amenable to extractionusing a Fogarty biliary catheter10 or suctiondevice,11 and as a result the role and value ofcyanoacrylate techniques remains unclear.
Above all, these cases illustrate the require-ment for a cooperative patient, good light,direct vision, and manual dexterity. AlthoughThompson7 and Hanson and Stephens9 bothreport success with children, we are doubtfulwhether many youngsters are capable ofstaying still for the time it takes the glue to dry,and would suggest that in the absence of seda-tion this technique may prove most applicableto adults.
ConclusionRemoval of foreign bodies from the ear usingcyanoacrylate glue is more useful in adults thanchildren as a high degree of cooperation isrequired. There is considerable scope forfurther research into this particular removal
Figure 1 Foreign body(plastic pearl) removed incase 2 using cyanoacrylateglue. The pearl is stilladherent to the hollowplastic tube used in theextraction.
A useful form of glue ear 149
EmergencyDepartment, FrenchayHospital, BeckspoolRoad, Frenchay,Bristol BS16 1LEJ R BengerP H Davies
Correspondence to:Dr Benger, SpecialistRegistrar In EmergencyMedicine (e-mail:[email protected])
Accepted 23 October 1999
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from

technique, and for a formal comparison of thevarious extraction methods currently in use.
ContributorsJonathan Benger and Philip Davies worked together to initiateand develop this case report. Jonathan Benger collected theclinical data and drafted the paper. Philip Davies contributed tothe literature review and edited the paper.
Both authors act as guarantors for the paper.
Conflict of interest: none.Funding: none.
1 Baker MD. Foreign bodies of the ears and nose inchildhood. Pediatr Emerg Care 1987;3:67–70.
2 Bressler K, Shelton C. Ear foreign body removal: a review of98 consecutive cases. Larygoscope 1993;103:367–70.
3 Fritz S, Kelen GD, Siverton KT. Foreign bodies of theexternal auditory canal. Emerg Med Clin North Am 1987;5:183–91.
4 Stool SE, McConnel CS. Foreign bodies in pediatricotolaryngology. Clin Pediatr (Phila) 1973;12:113–6.
5 Morris MS. New device for foreign body removal. Laryngo-scope 1984;94:980.
6 Zeinulabdeen M. New touch and pull method to removeforeign bodies from the ear. J Indian Med Assoc 1977;68:97–8.
7 Thompson MP. Removing objects from the externalauditory canal. N Engl J Med 1984;311:1635.
8 Pride H, Schwab R. A new technique for removing foreignbodies of the external auditory canal. Pediatr Emerg Care1989;5:135–6.
9 Hanson RM, Stephens M. Cyanoacrylate assisted foreignbody removal from the ear and nose in children. PediatricChild Health 1994;30:77–8.
10 Virnig RP. Nontraumatic removal of foreign bodies. MinnMed 1972;55:1123.
11 Jensen JH. Technique for removing a spherical foreign bodyfrom the nose or ear. Ear Nose Throat J 1976;55:46–7.
150 Benger, Davies
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from

doi: 10.1136/emj.17.2.149 2000 17: 149-150J Accid Emerg Med
J R Benger and P H Davies A useful form of glue ear
http://emj.bmj.com/content/17/2/149.full.htmlUpdated information and services can be found at:
These include:
References
http://emj.bmj.com/content/17/2/149.full.html#related-urlsArticle cited in:
http://emj.bmj.com/content/17/2/149.full.html#ref-list-1This article cites 9 articles
serviceEmail alerting
box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in the
CollectionsTopic
(12767 articles)Trauma � Articles on similar topics can be found in the following collections
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on July 16, 2011 - Published by emj.bmj.comDownloaded from





























