Embed Size (px)
Citation preview
PromıseVoice of St. Paul’S foundation
Fall / Winter 2016
Preventing OverdOsesSt. Paul’s study takes aim at opioid overdose crisis
transfOrming HealtH CareBuilding patient-centred care from the ground up at the new St. Paul’s
first-in-Canada diagnOstiC CtGroundbreaking technology helps cardiac patients avoid invasive procedures
a five-year $40-million initiative led by Dr. adeera levin will transform kidney care across Canada
A Revolutionin Kidney Disease Care

Brian Smith/PhC media Services
In medicine, models of care are ever evolving thanks to leading-
edge studies and advancements in research. at St. Paul’s, we’re grateful for our world-leading team of clinicians and researchers and proud of their accomplishments and goals. With the help of donors and community partners, the team at St. Paul’s is able to continue its work as a leader in medical research, innovation and teaching. as we fund studies in areas such as kidney care, hepatitis C elimination and preventing overdose deaths, St. Paul’s is poised to improve models of care not only in BC, but around the world.
Our cover story, Transforming Kidney Disease Care Across Canada (page 14), highlights Dr. adeera Levin’s Canada-wide research program – Canadians Seeking Solutions and innovations to Overcome Chronic Kidney Disease.
the project is patient focused, encompassing myriad areas of research across the country and aims to improve quality of care for Canadians living with chronic kidney disease.
in Time to MOVE on Preventing Overdose Deaths (page 18), we speak to Dr. Keith ahamad, an addiction medicine researcher with the BC Centre for Excellence (BC-CfE) in hiV/aiDS. this fall, his team at St. Paul’s launched a new study aimed at understanding overdose deaths, and, potentially, creating a model of care for their prevention.
the new focus of the BC-CfE’s gold standard targeted Disease Elimination program – hepatitis C – is discussed in Preventing the Next Lethal Health Crisis (page 22). Dr. Julio montaner is applying new provincial funding to treating those with substance use issues or mental health disorders, a critical aspect of the cascade of care to eradicate the virus.
We share some news about the new St. Paul’s (page 10), a visual and physical manifestation of improved models of care. the ambitious new health campus puts patient care and community in focus, connecting education, research, industry and
innovation to the continuum of care. as always, our community is playing
a role in supporting innovative models of care at St. Paul’s. Jens and Kerstin Locher raised $3,500 to purchase St. Paul’s first cuddle cot (Time to Grieve, page 6); and the robert L. Conconi Foundation made a donation toward the BC integrated Youth Services initiative to support mental health and substance use care for at-risk youth across the province.
heading into the holiday season, the Foundation thanks you for your continued generosity. With your support, we’re committed to delivering the highest quality health care to British Columbians across the province, through the best models of care.
Modelling Care
FROM THE TOP
Promise | Fall/WintER 20162
DOn KasIanChair, St. PauL’S FOunDatiOn; PrESiDEnt, KaSian arChitECturE intEriOr DESign anD PLanning LtD.
DIcK VOllETPrESiDEnt anD CEO, St. PauL’S FOunDatiOn
Get the latest news about St. Paul’s Hospital:
@helpstpauls
facebook.com/helpstpauls
@helpstpauls
www.helpstpauls.com

10 the new st paul’s Planning for the new St. Paul’s health campus connects
education, research, industry and innovation to the continuum of care. By allan maCdonald
14 caring for kidneys Dr. Adeera Levin’s research in kidney disease is taking a
major step forward. With over $40 million in funding, her project will look at what’s important to patients and assess new treatment models to improve the cascade of care. By laura rodgers
18 preventing overdose deaths The recently announced public health emergency has
springboarded a first-of-its-kind study at St. Paul’s aimed at understanding and preventing opioid overdose deaths. By josePh duBé
20 long-term donations Andrew Burke’s long road to recovery sparked a desire to
give back to St. Paul’s with a monthly gift, helping fund the incredible research being done at the hospital. By allan maCdonald
22 eradicating hepatitis c The BC Centre for Excellence in HIV/AIDS is targeting
the hepatitis C virus with the help of Dr. Julio Montaner’s Treatment as Prevention® model. By melissa edwards
2 FROM THE TOP Modelling Care By don Kasian and diCK Vollet
4 FRONTLINES Putting Youth at
the Centre; Three in Under 24 Hours; Time to Grieve; Beating Hearts; Innovative Ways to Give
9 BREAKTHROUGHS New 3D heart modelling
technology allows St. Paul’s doctors unprecedented accuracy in assessing heart health.
23 Q&A Meet Dr. Rita McCracken,
whose work with frail elders puts people first. By gail johnson
CoVer: dr. adeera levin, executive director of the BC renal agency and co-principal investigator at Can-solVe CKd, photographed by CLAUdETTE CARRACEdO
InsIDE
“we all think staying alive forever is a really good outcome, but lots of
people, they care a lot more about the quality of their life.” pg 14
– dr. adeera levin, principal with Can-solVe CKd
Fa L L / W i n t E r 2 0 1 6
Fall/WintER 2016 | Promise 3
We welcome your comments on Promise magazine.
Please write to us c/o st. Paul’s Foundation,
178 –1081 Burrard St, Vancouver, BC, V6Z 1Y6. Website: www.helpstpauls.com
Phone: 604-682-8206; Fax: 604-806-8326.
Promise magazine is published twice a year by Canada Wide media Limited for St. Paul’s
Foundation. no part of this magazine may be reproduced without written permission of
the publisher. Send change-of-address notices and covers of undeliverable
copies to: Promise, c/o
st. Paul’s Foundation, 178 –1081 Burrard St., Vancouver, BC, V6Z 1Y6.
For subscription enquiries, call 604-682-8206. iSSn: 1703-6151. Canadian Publications mail
Product Sales agreement no. 40065475.
230, 4321 Still Creek DriveBurnaby, British Columbia, V5C 6S7604-299-7311 Fax: 604-299-9188
Chairman, Ceo
Peter Legge, O.B.C., LL.D. (hon)
President
Samantha Legge, mBa
ChieF CreatiVe oFFiCer
Charlene rooke
senior ViCe-President oF integration
Brad Liski
ViCe-President oF Content marKeting
ryan mcKenzie
ViCe-President oF digital
Kevin hinton
editor ariane Fleischmann
ContriButing editors
Sarah Burgess, Sara turcotte
art direCtor
rick thibert
ContriButing writers
Edel Burke, Joseph Dubé, melissa Edwards,
ariane Fleischmann, gail Johnson, allan macDonald, Laura rodgers,
Sara turcotte
ContriButing PhotograPhers/illustrators
hedrich Blessing, Claudette Carracedo, anton grassl/Esto, Steve hall, Perkins+Will, Fernando Prado, greg morton and Brian Smith/
Providence health Care media Services, ron Sangha, istock
imaging teChniCian
mandy Lau, Bernhard holzmann
ProduCtion manager
Kristina Borys
V O L u m E 14 , n u m B E r 2
14
5
7 18

Following earlier reports in Promise, the BC Integrated Youth Services
Initiative (BC-IYSI) has since launched its “proof-of-concept phase” and announced that its five independent panel-recommended storefront-style centres will be located in North Vancouver, Kelowna, Campbell River, Prince George and Abbotsford.
The centres are loosely modelled after the St. Paul’s Granville Youth Health Centre (GYHC) in Vancouver. The goal of the BC-IYSI and participating local organizations, however, is to develop the centres to reflect each community.
“Every community is so unique,” says Sarah Irving (pictured), a peer support worker at the GYHC. “With the [GYHC], a lot of our clients are homeless and
street entrenched, and our community partners are agencies and resources that serve a population of homeless youth. But that isn’t necessarily a model that’s going to fit the centres in different communities across the province.”
With access to comprehensive health and social services, web-based supports and telephone help lines, the centres will bridge critical transition points, while the approachable setting and holistic treatment will help youth not only with their mental health and substance use issues, but also with improved outcomes in work, school, or finding employment.
Support from the Robert L. Conconi Foundation bolsters progress for the initiative, with Foundation president
Bob Conconi saying his intent was sparked by an appreciation for how St. Paul’s operates.
“St. Paul’s is responsive,” says Conconi. “They appreciate the changing needs of patients and they make changes, sometimes bold changes, to better serve them.”
Established in 2003, the Foundation focuses on health care, poverty and economic security, and education. It also has in its mandate to fund across the province, so it recognizes the potential for the new centres to lay groundwork for a larger, province-wide network.
In his research, Conconi spotted a pattern amongst young patients with mental health, problematic substance use, or other health or social service needs: adult clinics can be traumatizing. This prompted him to look at the BC-IYSI, whose model of care places the young people themselves at its centre, a dynamic which Conconi describes as “a transformational shift” in how we care for our young people – empowering them to thrive.
FRONTLINES >> To find out how you can support care, research and teaching at St. Paul’s, please contact St. Paul’s Foundation at 604-682-8206 or visit helpstpauls.com.
BRIAN SmITH/PHC media ServicesPromiSe | Fall/WintER 20164
PuttingYouth
at the Centre
SuPPorT this initiative in your community today!Visit bciysi.ca/donate
Spring 2016 cover story update

BRIAN SmITH/PHC media Services Fall/WintER 2016 | PromiSe 5
In the wake of performing a record-breaking three heart transplants
within 24 hours, Dr. Anson Cheung, director of Cardiac Transplant and mechanical Circulatory Assist Program of BC at St. Paul’s Hospital, is humble. He’s quick to praise his fellow surgeons and cardiologists as well as the anesthesiologists, perfusionists, nurses and other OR staff, the team in the CSICU as well as the “incredible effort” put forth by BC Transplant in helping to coordinate what was a first-in-BC medical milestone.
“This took a great deal of coordination between a lot of people,” says Dr. Cheung. “Our team here at St. Paul’s and the team at BC Transplant, the families of the organ donors, the families of the recipients. many different people helped to make this day possible.”
23 HOURS IN THE ORNot including preparation, from the beginning of the first surgery at 6:00 p.m., to the end of the third at 5:00 p.m. the following day, Dr. Cheung clocked 23 hours in the OR.
The first transplant began at 6:00 p.m. and took three hours to complete, with Dr. Cheung closing at 9:00 p.m. A mere hour later, the second, more complicated procedure took place overnight, lasting seven
hours and closing at 5:00 a.m. After a rest, the final transplant started at noon and was completed by 5:00 p.m.
The variation in procedure length relates to the unique circumstances of each patient. For example, a transplant for a patient with a condition like congenital heart disease is more complex and requires more time. Of the three procedures, the second and third were more complicated; the third had an existing ventricular assist device (VAD) implanted and the new heart necessitated its removal. To remove a VAD adds time and complexity to the procedure.
Each surgery was staffed with fresh OR personnel as per the usual hospital staff rotation, so the entire team was
at full capacity and alertness. If you’re wondering how Dr. Cheung
got through such a long day, he says he felt mentally and physically fine, which he attributes to being “in the moment” and to being “in the flow” of the busy operating room. Additionally, he was able to get some sleep during the seven-hour window between the second and third procedures.
But his work didn’t end there. Dr. Cheung had another surgery scheduled for the following day.
Dr. Cheung reports that all three procedures went smoothly and the patients are doing fine.
TRANSPLANTS ON THE RISEBetween 2010 and 2014, St. Paul’s – the only hospital in BC that performs adult heart transplants – performed an average of 19 transplants per year. In 2016, 20 transplants had already been performed by the end of August. The 2007 single-year record of 23 heart transplants could be defeated if the trajectory continues.
The number of transplants performed at St. Paul’s depends on the number of donor organs that become available.
To support the lifesaving work of the provincial Heart Centre at St. Paul’s, please contact St. Paul’s Foundation at 604-682-8206 or visit helpstpauls.com.
243in UndER
HRS
(right) Dr. Cheung checks in on a heart transplant
patient

PromiSe | Fall/WintER 20166
“Sometimes a moment is a lifetime,” reads the beautiful
inscription on St. Paul’s first cuddle cot, a gift made possible by Jens and Kerstin Locher’s fundraising efforts in memory of their infant sons marlon and Tobias. marlon passed away in 2011, two days after his birth, from complications during delivery; and in 2012 the Locher’s son Tobias was stillborn at 35 weeks gestation.
Working with St. Paul’s Foundation, Jens and Kerstin brought together a group of family and friends to raise $3,500 to purchase a cuddle cot in the fall of 2015. “It’s something that would have helped us. And because we wanted to help other parents, Kerstin and I decided that raising money to buy a cuddle cot for St. Paul’s would be fitting,” says Jens.
The Locher’s fundraiser inspired a group of respiratory therapists at St. Paul’s to do something similar in celebration of Respiratory Therapists Week in September 2015. The group gifted $3,000 to the maternity ward to fulfill a wish list that supports the cuddle cot initiative to help bereaved parents. The list includes a memory box for keepsakes like a baby blanket, scissors to collect a lock of hair, a kit to take foot- and hand-prints, a journal, books and other support resources for parents.
While these fundraising efforts were underway, Belinda-Ann Furlan, a nurse practitioner at the Atrial Fibrillation Clinic, stepped into a St. Paul’s elevator and saw a poster calling for donations for the cuddle cot campaign. It struck a deep chord, borne of personal experience – her older sister was stillborn and Belinda-Ann believed her mother still carried grief from that time. To honour her mother’s recent birthday, Belinda-Ann contacted St. Paul’s Foundation and arranged to make a donation to support the respiratory therapists’ fundraising campaign. Belinda-Ann’s mother was greatly moved by her daughter’s gesture and how many grieving parents would be impacted by it.
While the passing of a newborn is tragic, acknowledging parents’ pain and providing a means for grieving is important to St. Paul’s. The inscription on the cuddle cot resonates with both hospital staff and parents, embracing the sentiment of giving everyone the moment they need.
Time to GrieveJens and Kerstin Locher’s fundraiser for a cuddle cot
at St. Paul’s inspired others to give
What is a cuddle cot?A cuddle cot is a bassinette that keeps a stillborn infant cool, providing grieving parents time to be with their baby before they say goodbye.
The cot’s coolness slows down post-mortem physical changes, enabling the baby to stay with the parents in the hospital room longer.
many couples find that this time with their baby – especially after going through such anguish and trauma – provides great comfort and solace.
“It’s something that would have helped us... [so] raising money to buy a cuddle cot for St. Paul’s would be fitting.”

Fall/WintER 2016 | PromiSe 7
A lthough skilled at the procedure, Dr. Jamil Bashir, a cardiac surgeon
at St. Paul’s, says the best-case scenario would be eliminating laser lead extractions entirely.
Leads are wires attached to the heart that enable an implantable defibrillator to detect and correct irregular heartbeats. The leads are quickly incorporated into the heart and blood vessels with fibrous tissue and then cannot be removed without special techniques. Leads are often removed to avoid infection or when they fail.
Dr. Bashir removes the leads with an excimer laser, threading it around the lead and into the heart, and then firing when it meets the scar tissue. The objective is to destroy the scar tissue in which the lead is embedded so that it can be safely removed.
In 1994, laser lead extraction revolutionized the procedure – which typically required open-heart surgery – as a minimally invasive alternative. Dr. Bashir performed the 1,000th laser lead extraction at St. Paul’s in fall 2016.
St. Paul’s currently has the largest laser lead extraction program in Canada and is a major centre of research and innovation in the field. Thanks to donors, St. Paul’s Foundation regularly supports the program, most recently in 2014, with the purchase of a new excimer laser.
In 2014, Dr. Bashir led St. Paul’s into a new era by helming the team that implanted the hospital’s first Subcutaneous Implantable Cardioverter Defibrillator, known as the S-ICD. “It’s wonderful to work at a hospital like
St. Paul’s,” says Dr. Bashir. “Research and innovation are embraced here.”
Like the traditional implantable defibrillator, the S-ICD fires the same corrective shock that resets the arrhythmic heart. The S-ICD, however, doesn’t require wires to be attached to the heart at all – it uses electrodes placed just under the skin.
Just as laser lead extraction became the preferred alternative to open heart surgery 20 years ago, Dr. Bashir and the dedicated team of cardiac specialists at the provincial Heart Centre at St. Paul’s are now embarking on the era of the S-ICD. Thanks to its easily
accessed electrodes, the new implant and system eliminates the need for leads, and thereby their extraction from the heart.
“The S-ICD is able to sense the heart’s activity from the surface of the chest, which is the real genius of this technology,” says Dr. Bashir. “And here at St. Paul’s, we have the largest program in Canada implanting these devices.”
“It’s about continuously improving patient care. Ten years ago it was just about lead extraction, and now it’s about improving the standards for pacemakers across the province,” says Dr. Bashir.
Beating HearTS
BRIAN SmITH/PHC media Services
Dr. Jamil BaSHir performed the 1,000th lead extraction at St. Paul’s. He hopes that a new, less-invasive method using an S-iCD becomes the new norm.
PromiSe | Fall/WintER 20168
123
4
THINGS TO REMEMBER• You do not have to claim donations made this year on your
current year’s tax return;
• Any donations not claimed in the current year may be carried forward over the next five taxation years;
• The Canada Revenue Agency generally allows spouses to combine their charitable donation receipts so the highest earner may claim all the receipts and the charitable donation credit can be maximized within the family unit;
• Seek advice from a tax professional prior to implementing any strategy to ensure it’s right for you.
Does giving cost us? Absolutely – that’s why it is called giving. But
there are some innovative donation strategies that may help to reduce your tax liabilities and enhance your capacity to give.
GIFTS OF SECURITIESIf you have marketable securities with accrued gains in your portfolio, consider donating them to a charity, especially if you intend to sell them on the open market in order to fund a donation.
Ordinarily, when you sell appreciated securities you are subject to tax on half of the realized capital gain. However, if the securities are disposed of by way of transfer to a public charity, you generally will not be taxed at all on the resulting capital gain.
In addition to avoiding the capital gains tax, you’ll also receive a donation receipt for the fair market value of the marketable securities.
LEGACY GIFTSConsider leaving a lasting legacy by planning for a future gift in your Will, through your RRSP, RRIF, or through a life insurance policy. Similar to your personal investments, taking time to plan your charitable giving will go a long way – for yourself and your favourite charities.
How Annie and John Added Over $600,000 to their Legacy GiftAnnie, a 40-year-old lawyer, and John, a 42-year-old emergency room nurse, added hundreds of thousands of dollars to their legacy gifts by making some minor changes to how they give.
BeFore: Every year Annie and John donated approximately $5,000 to their favorite charity, receiving a charitable tax receipt for the full amount.
Now: The couple decided to buy a joint life insurance policy, naming the charity as both owner and beneficiary. Each year, they pay a $5,000 insurance premium.
THe reSulTS: • Annie and John still receive a
charitable receipt for $5,000 each year;• The policy now has a benefit of over
$600,000;• When the funds are paid out to
the charity, they will be tax- and probate-free.
monetary giving has its merits, but so does giving your time, food or clothing to shelters in the city. Let’s all think about new ways of giving this holiday season.
For more about gifts of securities or legacy gifts, please contact St. Paul’s Foundation at 604-806-8271 or visit helpstpauls.com/legacy-giving.
Securities and investment information provided by Ludovic Siouffi, MBC, CIM, Investment & Insurance Advisor at Canaccord Genuity Wealth Management.
Innovative Ways to
Give

Fall/WintER 2016 | PromiSe 9
S t. Paul’s Cardiac CT Laboratory is the first clinic of its kind in Canada to use non-invasive, computer generated
3D imaging to precisely measure coronary arteries and blood flow in heart disease patients.
Using a web-based technology called HeartFlow Fractional Flow Reserve-Computed Tomography (FFRct), St. Paul’s physicians are now equipped to vastly improve the way patient care is managed for many British Columbians suffering with heart problems.
“We are the first centre to have FFRct in clinical use in Canada and it’s been really disruptive to how we practice and how we’ve been able to help patients with suspected coronary artery disease,” says Dr. Jonathon Leipsic, chairman of the Department of Radiology at St. Paul’s Hospital.
“FFRct offers a real opportunity to understand the need for patients to undergo invasive angiography and potential revascularization, versus them just having medical therapy,” says Dr. Leipsic. “It’s a much more efficient utilization of resources. To date we have used the technology to help with the management of over 100 patients. For some, it enabled us to avoid an invasive procedure and for others it allowed a better understanding of their atherosclerosis, their risk, and the cause of their symptoms.”
Traditional diagnostic tests, while non-invasive, provide little information on potentially worrisome symptoms like chest pain, leading many patients to endure the stress and discomfort of unnecessary invasive testing. FFRct analysis effectively separates patients who need further in-depth testing from those who don’t, which in turn reduces health care system costs and wait times.
The state-of-the-art analysis is carried out by HeartFlow Inc., which receives data from coronary CT scans and employs highly advanced computation to assess the impact that
blockages have on blood flow. The result is a 3D model of the patient’s arteries sent back to clinicians who then use it to determine, vessel by vessel, if sufficient blood is reaching the heart.
The groundbreaking St. Paul’s Cardiac CT Laboratory is recognized as the most academically productive department of its kind in the country.
With key roles in publishing over 60 manuscripts last year and a core of dedicated specialists continuously carrying out a number of clinical trials, it’s easy to see why the department leads the way in this critical domain.
“We have exclusivity with HeartFlow Inc. based on research engagements and past relationships,” says Dr. Leipsic. “Worldwide, there are only about thirty other centres who have access so it’s a pretty unique opportunity for BC residents.”
Dr. Leipsic anticipates treating 500 patients this year with FFRct analysis. For them, the new technology will be an invaluable tool to recovering their health, and none of it would be possible without St. Paul’s Foundation and donor funding.
“We are incredibly grateful to the Foundation and our generous donors for making this unique opportunity a reality.”
Funds for the FFRct license came from a generous anonymous donor – a former patient at St. Paul’s. Additionally, John Grose, himself a recent recipient of FFRct imaging, contributed to the fund. The CT scanner at the Centre was purchased thanks to donors, with an mRI machine still to come.
To learn more about the groundbreaking work of our radiology team, visit helpstpauls.com.
Dr. Jonathon Leipsic has received an unrestricted research grant from HeartFlow Inc. and currently serves as a consultant.
Dr. JoNaTHoN leiPSiC uses 3D models of patients’ arteries to assess blood flow. The new technology is an invaluable tool in treating atherosclerosis.
BRIAN SmITH/PHC media Services
Breakthroughs
New technology allows St. Paul’s doctors unprecedented accuracy in assessing heart health
BY JOSEPH DUBé
3D MODEL HEARTS
Promise | Fall/wintER 201610
the New St. Paul’S
the BC Ministry of Health has identified the redevelopment of
St. Paul’s Hospital as a catalyst to transforming how health services are delivered in BC.
Key to this transformation is the development of a new care model that places the patient at the centre and calls for the delivery of coordinated
health care services where and when people need them most – at home, in the community, or in the hospital. This care model informs all stages of planning for the new St. Paul’s – from the relationship between research and care, to how the health campus will look and feel to patients and families.
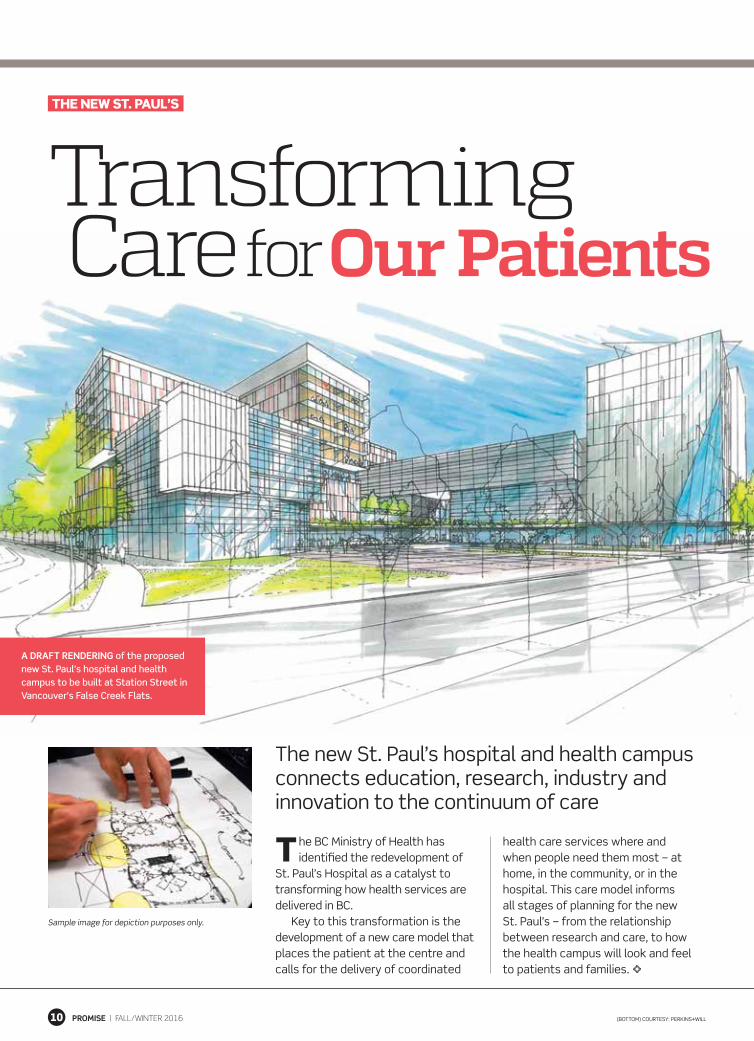
Transforming Care for Our Patients
(BoTToM) CourTeSy: PerKinS+Will
A drAft reNderiNG of the proposed new St. Paul’s hospital and health campus to be built at Station Street in Vancouver’s False Creek Flats.
The new St. Paul’s hospital and health campus connects education, research, industry and innovation to the continuum of care
Sample image for depiction purposes only.

Fall/wintER 2016 | Promise 11
the driving factors behind the design of the new St. Paul’s hospital and integrated health campus are operational
flow and patient experience. The location of each program, service, building and facility is meant to improve patient care and streamline its accessibility, as well as facilitate the research that will transform patient care in the future.
in addition to the core acute care hospital, the campus will host a range of non-acute care facilities including outpatient clinics, an urban health centre, and research and teaching spaces, all of which will be connected to optimize the continuum of care.
Patient experience and operational efficiency will be intrinsically linked in the new design. Single rooms will improve patient experiences and health outcomes by providing increased comfort, privacy and infection control. in the halls, simplified wayfinding will streamline foot traffic and reduce patient anxiety.
in addition to architecturally adaptable buildings that house state-of-the-art equipment, the new St. Paul’s will feature open spaces and natural light, cafes and shops, as well as sacred places in which patients, friends and family members can reflect and hold ceremonies.
buildiNg blockS of the New St. Paul’S
The hospital will provide essential care for patients from across BC who require active treatment due to injury and illness; this includes diagnostic evaluation, surgical procedures and overnight stays. The hospital will house key components such as an emergency department, operating rooms, a diagnostics and imaging centre, inpatient beds, labs and pharmacies.
outpatient clinics will be co-located with the main hospital to extend services beyond acute care and offer easy access for patients.
As part of the acute care hospital, an urban health centre adjacent to the emergency department will offer a range of mental health, urban health and addiction medicine programs.
overall, both indoors and out, the new St. Paul’s health campus will feature environmental design that creates a relaxing and restorative environment for patients and staff. The connected facilities on the campus will optimize the continuum of care.
CliNiCiANs ANd reseArChers will work side by side at the new st. Paul’s hospital and health campus. the environment is intended to stimulate research and community. Sample image for depiction purposes only.
CourTeSy: PerKinS+Will
deSigNiNgthe New St. Paul’sAn integrated health campus that flows with purposeful design and a layout that puts patient needs at its core

Promise | Fall/wintER 201612
AcceleratingReSeaRch aNdiNNovatioN at the New St. Paul’sInnovation will be front and centre, with clinicians and researchers working side by side
simPlified wAyfiNdiNG will improve patient experience, while the new design encourages research and innovation amongst clinicians. Sample images for depiction purposes only.
(ToP) KAiSer PerMAnenTe SMAll HoSPiTAl Big ideA CoMPeTiTion / CourTeSy: PerKinS+Will; (Middle) ©AnTon grASSl/eSTo / CourTeSy: PerKinS+Will;
Research and innovation is key to realizing the vision for the
new St. Paul’s. And the hospital has deep experience in these areas, with new programs and pioneering initiatives that have set health care standards worldwide. drawing from this knowledge and background, we’re poised to create an innovative blueprint for the new St. Paul’s that will set a benchmark for hospitals the world over.
For example, St. Paul’s Centre for Health evaluation and outcome Sciences has changed health care locally and globally with its work in health economics and clinical trials; the Centre for Heart lung innovation at St. Paul’s is the world’s top facility for cardiopulmonary research; and the BC Centre for excellence in HiV/AidS at St. Paul’s has seen its models adopted by the united nations for its initiative to end the AidS pandemic globally by 2030.
These three centres represent different areas of medicine and science, but share a common approach. in each, clinicians and researchers work side by side, not just in the same building but often in the same lab or office. The approach has resulted in two immeasurable benefits: it has stimulated research and led to more findings, and these findings are being brought to patients faster than at any other time in history.
The new St. Paul’s will apply this same approach to other areas of
research, innovation and patient care throughout its integrated campus and community networks.
To complement our commitment to research and innovation, St. Paul’s will also work more closely with industry partners to turn leading-edge ideas into better care. The planned placement of commercial buildings alongside the research towers that intersect with our acute care hospital speaks to this objective: the exchange of ideas with industry are at the very intersection of care and research.
A new office of innovation and Strategic Partnerships, funded by St. Paul’s Foundation, was recently established to support this full continuum of innovation and commercialization as envisioned.
The strong integration of research and innovation at the new St. Paul’s will create and maintain a cycle of innovation and new knowledge that will place British Columbians at the front of the line for world-class health care for generations to come.
For more information on the new St. Paul’s, please visit thenewstpauls.com.
the New St. Paul’S

Fall/wintER 2016 | Promise 13
what is transformation of care and why is it necessary?it means changing the way patients receive and access care. Currently, BC’s health care system is organized around service providers, and less so our patients. right now, patients access services for each of their health care issues from different providers in an often uncoordinated and fragmented way. For those with complex needs, it can be challenging.
how does this affect how the new st. Paul’s will be built and operated? To be successful, transformation must be system-wide, from the community to the hospital and back home. it involves breaking down the department and program structures and grouping care into service families to better support patients. This will help ensure that patients are more easily able to navigate services and access the care they need. The design will also foster a culture of innovation and scientific inquiry in research and teaching, resulting in direct benefits to patients.
what are the key benefits of transforming care?A transformed model of care means even patients with complex health care issues will receive the care they
need when and where they need it most. Providers will be able to more easily access and share critical patient information, enabling them to identify gaps and improve the delivery of care. By embracing health care as a complex and adaptive system, we will have the flexibility to meet unanticipated demands and changes in the system.
how does this change the patient experience?Here’s an example: a patient with degenerative arthritis may need to regularly undergo visits to their family doctor for checkups, to a clinic for blood work, to the hospital for x-rays and surgery, to various specialists, and arrange for in-home care and physiotherapy. Currently, these services are delivered and managed as separate streams of care, so patients may find it challenging to navigate multiple appointments, experience long wait times or discover gaps in care, repeatedly explaining their health care needs and history to different providers.
When health care becomes more integrated, streamlined, intuitive and patient-centred, patients will be able to spend more of their valuable time receiving the care they need, and less time and energy trying to navigate a complex health care system.
(Middle) STeVe HAll © HedriCH BleSSing 2012 / CourTeSy: PerKinS+Will; (BoTToM) STeVe HAll © HedriCH BleSSing 2012 /CourTeSy: PerKinS+Will; (ToP rigHT) BriAn SMiTH
Putting PatieNt exPeRieNce First
dR. Jeff Pike is the physician lead, clinical planning, for Providence health Care’s st. Paul’s redevelopment Project. he is an orthopaedic surgeon who specializes in hand and upper-extremity surgeries. dr. Pike is also a clinical assistant professor with the department of orthopaedics at UBC.
Q&a dR. Jeff Pike
Dr. ADeerA Levin (right) is setting ambitious targets for Can-SOLVE CKD. As the BC project lead, she’s working with her team to find better ways to treat kidney disease.
KidneyTransforming
Disease care across
canaDaHow do you make life better for people
with chronic diseases? You start by asking just what “better” means to them
By LAurA rODgErS
PhOtOgrAPhy By CLAuDEttE CArrACEDO
Promise | Fall/WintER 201614
Agroundbreaking Canada-wide
research program into chronic
kidney disease, with over $40
million in funding, is taking
a novel yet straightforward
approach: rather than starting
with answers, they’re starting with questions.
“A lot of research projects and networks don’t neces-
sarily start that way,” says Dr. Adeera Levin, the initia-
tive’s named principal applicant and head of the UBC
Division of Nephrology at St. Paul’s. “They start with a
couple of people with a good idea and some pet theories
they’re trying to test.”


The project is funded through the Canadian Institutes of Health Research and a variety of donations, including one for $500,000 from St. Paul’s Foundation.
Rather than starting with, say, a promising new drug molecule, the Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease (Can-SOLVE CKD) network will look at what’s important to patients, how and when they currently get treatment, then work alongside them to make those treatments better.
The five-year initiative encompasses numerous research areas: early screen-ing, patient education, novel drug treat-ments and the usefulness of stem cell therapies. A British Columbia team headed by Levin will co-lead the project, collaborating with physicians, research-ers and patients from across the country.
“In Canada and internationally, kidney disease research has been fragmented and not as integrated on patient-focused questions as some
other specialties,” Levin says. The ini-tiative aims to change that, by creating a way to gain knowledge and share best practices throughout Canada.
BreaKing new groundMore than three million Canadians incur significant damage to their kidneys, which can be caused by a number of different problems: high blood pressure, diabetes, infections, or inherited or acquired systemic diseases. Any damage to the kidneys’ ability to filter waste out of the body causes system-wide health issues or worsens other conditions, and can lead to early
death. Chronic kidney disease (CKD), the umbrella term for all conditions which cause kidney damage, costs the Canadian health care system over $50 billion each year.
According to the Kidney Foundation of Canada, more than 90 per cent of Canadians with CKD don’t know they have it. Current care models primar-ily focus on the disease’s most serious late stages: dialysis or transplants for those whose kidneys have shut down entirely. St Paul’s and the province of BC have been pioneers in treating the disease early to keep it from progressing, through the development of structured
multidisciplinary patient-focused clinics. Though kidney damage affects
more Canadians than heart disease (1.4 million) or diabetes (3.4 million), nephrology has fewer clinical trials than any other medical field. Levin aims to change that.
“If you walk into a kidney unit and try to get people to be in a study, it’s like pulling teeth,” she says. “But every-body’s in a study in the cancer or car-diology world, it’s just the way they’ve approached delivering best care and answering important questions. We’re trying to change the culture of kidney care so that everybody is part of a mean-ingful enterprise to answer questions.”
The Can-SOLVE CKD project poses a wide range of questions, relevant to all stages of the disease. They’re trying to find new methods to catch kidney problems early, even when additional, co-occuring condi-tions like diabetes make that all the more complicated; they’re trying stem-cell therapies; they’re testing established drugs that have shown promise to help kidney patients as well.
Promise | Fall/WintER 201616
“my hope is that, over the next 10 years, we will not need to build new dialysis clinics because we will have figured out a way to delay progression.” – Dr. Adeera Levin, consulting nephrologist at St. Paul’s and co-principal investigator with Can-SOLVE CKD

This fits in with the project’s overall ethos, and the philosophy that’s guided Levin’s entire career: examine every-thing that could work, then winnow it down to what works best.
TreaTing Canadians in rural areasWhile Can-SOLVE CKD aims to break new ground in the worldwide field of kidney care, Canada’s unique geogra-phy and population shape its goals. For people living hundreds of kilometres from the nearest hospital, the current care model that expects them to fre-quently visit a clinic just doesn’t make sense. The project aims to help patients in rural and remote areas by trying out new techniques like self-monitoring and telehealth videoconferencing.
CulTurally appropriaTe TreaTmenTTo better deliver treatment for Indigenous peoples, who stand at a higher statistical risk of kidney dis-ease, the research team is consulting with a team of Indigenous people to find culturally appropriate studies and therapies that address their needs.
Working with the initiative’s Indigenous Peoples’ Engagement and Research Council, Levin discovered many Indigenous people were reluctant to join in randomized controlled trials because they felt it was unfair for a con-trol group to be denied a potentially life-saving new drug or therapeutic strategy. Using this knowledge, the project team is changing study designs to respect these views, while still ensuring that there is good ‘science’ and conclusions. They’re also making sure that there is Indigenous representation in all aspects of the kidney study design and data.
“We have to design the studies dif-ferently but still robustly, so that’s been a very big eye-opener.”
amBiTious TargeTsLevin first tested the multidisciplinary, patient-first approach that informs Can-SOLVE CKD at St. Paul’s, with a 1991 study that later grew into the hos-pital’s Kidney Care Clinic (KCC). The
clinic began with the idea that a one-stop shop for kidney patients, where they could meet with doctors, dietitians, social workers and nurses all in one appointment, might improve health outcomes and quality of life. It did.
“The kidney care clinic at St. Paul’s is one of the first of its kind,” she says. “It’s grown, so now it’s a model of care.”
Established as a permanent clinic in 1999, the KCC now cares for more than 1,200 patients. By giving targeted care to people with varying stages of kidney disease, the clinic has been able to slow progression for many and reduce the need for replacement therapies like dialysis or transplants.
The goal of Can-SOLVE CKD is to take that kind of thinking and, by applying it to studies across Canada, reap the same kind of results.
The targets are ambitious. By 2020, Levin and the team hope every Canadian with, or at risk for CKD will be screened and able to access the best possible treatment. By screening and treating early, the team hopes to signifi-cantly reduce the number of patients who experience kidney failure. They also hope to double the number of peo-ple involved in clinical nephrology trials.
“My hope is that, over the next 10 years, we will not need to build new dialysis clinics because we will have figured out a way to delay progression,” Levin says. “The goals are aspirational, but they’re not unattainable.”
While the initiative will collect an unprecedented amount of data about all aspects of CKD, Levin expects some important insights to come from a place beyond hard facts and figures.
“Often, as physicians and research-ers, we ask the wrong questions,” she says. “Patients are telling us to design studies that answer the questions important to them.”
“We all think staying alive forever is a really good outcome, but people care a lot more about the quality of their life. They say, ‘If we live longer, that’s great, but living longer with the set of symptoms we have is not that much fun.’ And that’s actually a really important message.”
Fall/WintER 2016 | Promise
A PROVINCE-WIDE VISION FOR KIDNEY CAREDr. ADeerA Levin began her medical career at St. Paul’s in 1990, starting with a kidney disease project encompassing both research and clinical care. Since then, she’s become a world-renowned leader in her field. She currently serves as the president of the international Society of nephrology, and was appointed to the Order of Canada in 2015.
Aside from her work heading up Can-SOLve CKD and as a consulting nephrologist at St. Paul’s, Levin is a scientist at the Centre for Health evaluation and Outcome Sciences (CHÉOS). She has also been the driving force behind the BC renal Agency since it was formed in 1997. The agency – the only one of its kind anywhere
in Canada – allocates funding and resources for kidney care across the province for all patients.
“As a province, we don’t need to play the game of ‘whoever screams the loudest gets the dialysis units,’” says Levin. “it’s all done in a very collaborative way; we work out where the resources are and where the patients are.”
The agency also works to ensure a continuity of care if patients move within BC. “it’s very patient focused, very transparent, and we try to deliver evidence-informed care,” Levin adds.
The model of patient-first care has been proven to improve outcomes.
“it translates into more efficient use of health care resources, and cost savings,” she says. “if you can predict who’s going to get into trouble or not, then you can better streamline their therapy. That means you ultimately save patients and family time and angst, and also health care system resources. it’s really a two-for-one.”
17

Promise | Fall/wintER 201618
Imagine the equivalent of three passenger planes filled with young people crashing to the earth every year – that’s the picture
Dr. Keith Ahamad uses to describe the public health emergency announced this year in response to overdose deaths in British Columbia.
“There’s no escaping it,” he says. “Addiction hits every single patient group and every socioeconomic group. We’re seeing two to three deaths a day from this preventable disease. If you were to compare that with any other health care emergency, the public would mobilize very quickly.”
In 2015 there were more overdose deaths than in any of the previous 20 years, and in 2016 that number
has spiked even higher. More than 61 people have died from overdose every month between January and June. Fentanyl, a potent opioid, is involved in over 60 per cent of cases.
Despite the high mortality rate, little is known about what happens to the cardiopulmonary system dur-ing an overdose and who might be at increased risk. This desperate lack of knowledge is why Dr. Ahamad and his team at St. Paul’s have launched a new study, called Mobile Opioid Vital-Sign Evaluation (MOVE), that may open the door to better understanding why overdoses happen, and, potentially, how they could be prevented.
The risks of long-term opioid use are only just beginning to be revealed.
A first-of-its-kind study at st. Paul’s is laying the groundwork for a breakthrough in
understanding opioid overdoses
By Melissa edwardsPhotograPhy By Brian sMith
Time ToMove on
PrevenTing OverdOse
DeaThs

Fall/wintER 2016 | Promise 19
In a recent study in the US, patients with non-cancer chronic pain who had been prescribed opioids were shown to not just be at greater risk of unintention-al overdose, but also at greater risk of death from all causes – particularly from cardiac events. The goal of MOVE is to create and test a new way of using vital-sign monitoring equipment, setting the groundwork to gather first-of-its-kind data on the cardiopulmonary effects of opioids, both in hospital settings and among those who use injection drugs.
“St. Paul’s has a long history of engaging with populations that other groups haven’t been interested in engaging with,” says Dr. Ahamad proudly. “We look at the data and the science and say: ‘This is what we need to do to improve outcomes.’ And this study is another example of that.”
Because there’s no previous research of its kind, the first phase of MOVE is a feasibility study. To start, Dr. Ahamad has partnered with researchers in the United States, using a mobile vital signs monitoring proto-type, called the “Canary I.”
In September, Dr. Ahamad and his team began the study with five
participants receiving in-hospital care at St. Paul’s, and 20 on injectable treat-ment at the Providence Crosstown Clinic in the Downtown Eastside. Patients wear the device, supervised, for two-hour periods after taking opioids during regular visits. Sensors measure heart rate, respiration and participant movements, and transmit the data securely via mobile phone to a server, where it is being held for future analysis to see how opioid use affects these vital signs.
While this initial research is only a first step in determining if patients could tolerate wearing the device, as well as collecting initial data, “the long-term application is really unlimited,” says Dr. Ahamad. Once the device can be adapted for more consistent use and to track further vital signs, such as oxygen saturation and blood pressure, work can begin on recognizing the real physiological effects of long-term opioid use, and how overdose warning signs might manifest in different people.
“This may revolutionize the prescrip-tion and safety of these medications, or it may inform us about who we need to be careful with when prescribing them,” says Dr. Ahamad. “And, for patients who use opioids recreationally, it could change the face of harm reduction.”
As the science improves and such a monitor becomes smaller and more responsive, it could be programmed to send out warning messages when the wearer is close to an overdose event. A future device could even be fitted with a naloxone pump that would auto-matically administer the anti-overdose drug when crisis is imminent.
Dr. Ahamad calls the research “new and leading-edge,” so every step must be invented. “It’s very exciting,” he says. “There is a lot to learn from the data, and we’re laying the framework for some amazing interventions. The potential for saving lives in an innovative, non-stigmatizing way is pretty great.”
To learn more about how you can help St. Paul’s reduce overdose deaths in British Columbia, visit helpstpauls.com.
Dr. Keith AhAmAD pictured with moVe team members, Jill Fikowski (left), clinical trials research coordinator, and Cheyenne Johnson (middle), clinical and research leader, BC Centre for excellence in hiV/AiDs. the team partnered with researchers in the United states to reconfigure existing equipment to create a prototype called the “Canary i.” it will be used to collect and send data for further analysis about the cardiopulmonary effects of opioid use on patients.
Fernando Prado

Promise | Fall/wintER 201620
In 2015, local business owner Andrew Burke made a $10,000 gift to support Dr. David Landsberg’s research in renal medicine at St. Paul’s. He also became a monthly donor in 2016, giving back to the hospital that helped
him through a physically painful three years of treatment. “I wanted to give monthly because it represents the long
process Dr. Landsberg and I went through together during my treatment. It wasn’t a one-off thing, so I like the idea that every month I’m helping fund the incredible work being done at St. Paul’s.”
Andrew Burke first came to Canada from the UK in 2001 at the age of 21, on a one-year work visa. In that short time he says he fell in love with Canada, and decided to make a more permanent move.
But during a 2004 trip to England to visit family, Andrew
felt sluggish and short of breath. Concerned, he saw a doctor, but was told it was likely just a minor infection.
Feeling bloated at the end of his trip, Andrew stepped on a scale to find he had gained 18 pounds in just two weeks. While he could feel the weight and the bloating, he didn’t know that his body was retaining fluids due a serious problem with his kidney. During his flight back to Canada, the excess fluid went into Andrew’s legs, causing them to balloon to twice their reg-ular size and bringing immense pain. At 30,000 feet above the Atlantic, all he could do was suffer.
Back in Vancouver, Andrew went immediately to a walk-in clinic, where within minutes he was redirected to St. Paul’s in an ambulance.
At the hospital, Dr. Landsberg, division head for the St. Paul’s Renal Program, performed a number of tests,
Andrew Burke (left) with dr. david Landsberg (right), division head for the st. Paul’s renal Program.
Fall/wintER 2016 | Promise 21
including a kidney biopsy. The results showed a specific type of nephrotic syndrome that is more common in children and considered rare in adults.
It turns out Dr. Landsberg himself had suffered from a simi-lar condition in childhood. “I can’t say it was the same for sure,” recalls Dr. Landsberg. “It was the early 1960s, I was seven years old. This was a time before kidney biopsies, which is the key diagnostic we use for such a condition today. So with no biopsy, I will never be 100 per cent sure of the condition I had.”
“I felt a connection with Andrew because of our shared experience,” says Landsberg. “I felt the distress of the swell-ing that this condition can cause and I had experienced the side effects of the treatment – heavy doses of steroids.”
Thanks to medical advancement, Andrew was provided medicine with lower steroids, translating to fewer side
effects and a more permanent response to treatment.Over the course of three and a half years Andrew received
treatment, though at times perceived successes were followed by relapses. During those times, Andrew says his weight would balloon from 200 to 260 pounds.
“I wasn’t doing very well,” says Andrew. “I was young, I didn’t have much money, I wasn’t able to work, and I didn’t have any family here.” Although Andrew was alone in that respect, he always felt that Dr. Landsberg went above and beyond for him. “He was more than just a doctor. He became a very special and significant presence in my life. At the end of the day, I feel that I am here because of him.”
To donate to St. Paul’s in support of live-saving kidney research and care, visit helpstpauls.com.
A Symbolic monthly
Donation St. Paul’s Foundation donor Andrew Burke
feels privileged to support Dr. David Landsberg’s research in renal medicine
By AllAn MAcDonAlD
PhotogrAPhy By BriAn sMith
Promise | Fall/WintER 201622
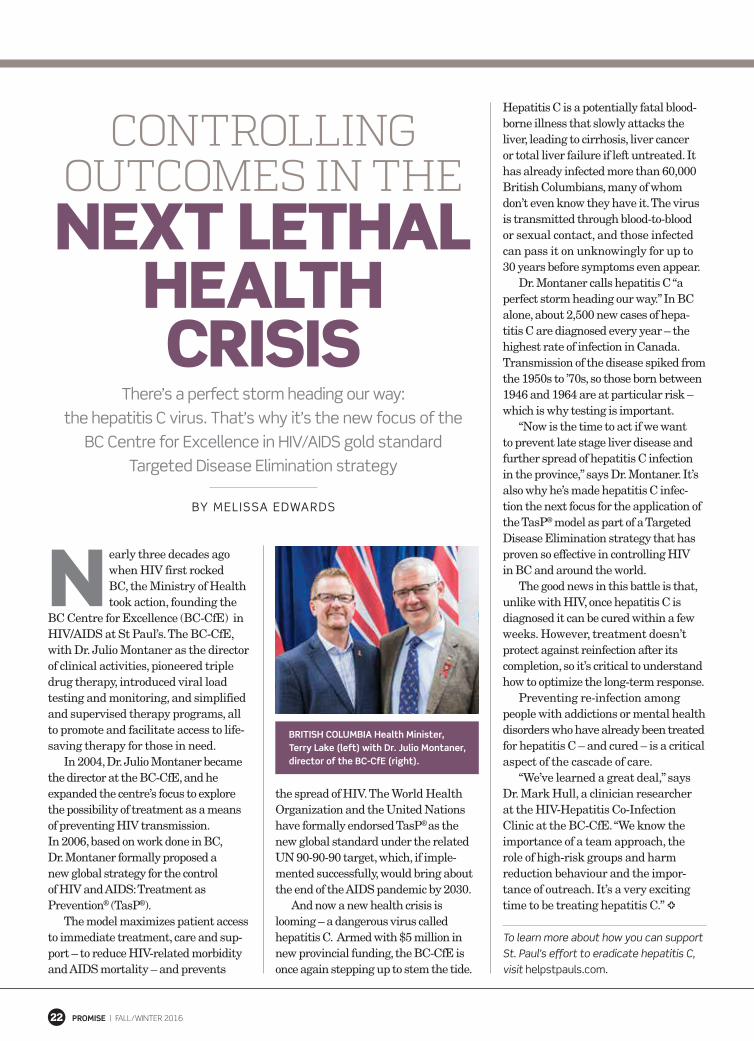
ControllingoutComes in theNext LethaL
heaLthCrisis
There’s a perfect storm heading our way: the hepatitis C virus. That’s why it’s the new focus of the
BC Centre for Excellence in HIV/AIDS gold standard Targeted Disease Elimination strategy
By MElISSA EDwArDS
N early three decades ago when HIV first rocked BC, the Ministry of Health took action, founding the
BC Centre for Excellence (BC-CfE) in HIV/AIDS at St Paul’s. The BC-CfE, with Dr. Julio Montaner as the director of clinical activities, pioneered triple drug therapy, introduced viral load testing and monitoring, and simplified and supervised therapy programs, all to promote and facilitate access to life-saving therapy for those in need.
In 2004, Dr. Julio Montaner became the director at the BC-CfE, and he expanded the centre’s focus to explore the possibility of treatment as a means of preventing HIV transmission. In 2006, based on work done in BC, Dr. Montaner formally proposed a new global strategy for the control of HIV and AIDS: Treatment as Prevention® (TasP®).
The model maximizes patient access to immediate treatment, care and sup-port – to reduce HIV-related morbidity and AIDS mortality – and prevents
the spread of HIV. The World Health Organization and the United Nations have formally endorsed TasP® as the new global standard under the related UN 90-90-90 target, which, if imple-mented successfully, would bring about the end of the AIDS pandemic by 2030.
And now a new health crisis is looming – a dangerous virus called hepatitis C. Armed with $5 million in new provincial funding, the BC-CfE is once again stepping up to stem the tide.
Hepatitis C is a potentially fatal blood-borne illness that slowly attacks the liver, leading to cirrhosis, liver cancer or total liver failure if left untreated. It has already infected more than 60,000 British Columbians, many of whom don’t even know they have it. The virus is transmitted through blood-to-blood or sexual contact, and those infected can pass it on unknowingly for up to 30 years before symptoms even appear.
Dr. Montaner calls hepatitis C “a perfect storm heading our way.” In BC alone, about 2,500 new cases of hepa-titis C are diagnosed every year – the highest rate of infection in Canada. Transmission of the disease spiked from the 1950s to ’70s, so those born between 1946 and 1964 are at particular risk – which is why testing is important.
“Now is the time to act if we want to prevent late stage liver disease and further spread of hepatitis C infection in the province,” says Dr. Montaner. It’s also why he’s made hepatitis C infec-tion the next focus for the application of the TasP® model as part of a Targeted Disease Elimination strategy that has proven so effective in controlling HIV in BC and around the world.
The good news in this battle is that, unlike with HIV, once hepatitis C is diagnosed it can be cured within a few weeks. However, treatment doesn’t protect against reinfection after its completion, so it’s critical to understand how to optimize the long-term response.
Preventing re-infection among people with addictions or mental health disorders who have already been treated for hepatitis C – and cured – is a critical aspect of the cascade of care.
“We’ve learned a great deal,” says Dr. Mark Hull, a clinician researcher at the HIV-Hepatitis Co-Infection Clinic at the BC-CfE. “We know the importance of a team approach, the role of high-risk groups and harm reduction behaviour and the impor-tance of outreach. It’s a very exciting time to be treating hepatitis C.”
To learn more about how you can support St. Paul’s effort to eradicate hepatitis C, visit helpstpauls.com.
British ColumBia health minister, terry lake (left) with Dr. Julio montaner, director of the BC-Cfe (right).

By GAIl JoHnSonQ&a
Dr. Rita McCrackenas the associate head at Providence Health Care’s
Department of Family and Community Medicine, and PhD candidate in experimental medicine at UBC, Dr. rita McCracken is known for her work with the elderly. She studies polypharmacy in frail elders, has an interest in patients with HIV and has her own family practice. Dr. McCracken is also a scientist at the Centre for Health Evaluation and outcome Sciences (CHÉoS).
What drew you to your research in polypharmacy and frail elders?There’s concern regarding the number of medications we’re exposing our frail elders to. I saw this in my own practice and went to the literature to learn about the right amount of treatment and found there was almost no research. I thought, ‘This isn’t right.’ In my PhD, I’m quantifying harms and benefits to make better decision-making tools.
how does your background play a role in your work in healthy aging?I was raised in a big Catholic family and someone was always
being born or dying. later, at medical school, I was surprised at how death and aging, part of the normal life cycle, were ignored and maybe even feared. But I feel very comfortable working with this group of patients and feel privileged to have the opportunity.
aging really is just one more stage of life, isn’t it?It is. GPs understand that part of healthy aging is the realization that growing older is normal; that dying is normal. Every family doctor knows from the start that we are needed by our patients and their families at all stages of life. End of life can be a difficult part of our job; but it is not failure when it happens.
tell us about a professional accomplishment of which you’re especially proud.Two of my patients recently died and even though they were in a nursing home, I was able to ensure that their personhood was honoured. This was important for patient and family. one of the reasons I love practising medicine with Providence is because that’s one of its stated values: “we put people first.” As a family doctor, that’s what I always strive to do.
23Fall/WintER 2016 | Promiseron SAnGHA
You hold the hopeOur patients benefit directly from your generosity.
#LightsofHope
This holiday season, please think about the patients at St. Paul’s. Through Lights of Hope, you can contribute to their greatest needs.
Donate at lightsofhope.com/promise
PM 4
00
65
47
5





























