Embed Size (px)
Citation preview
ABSTRACTS OF OPEN PAPERS
700Extracranial-to-intracranial Bypass for OcclusiveCerebrovascular Disease and IntracranialAneurysms in the United States, 1992–2001:A Population-based StudySepideh Amin-Hanjani, M.D., Bob S. Carter, M.D., Ph.D.,William E. Butler, M.D., Christopher S. Ogilvy, M.D.,Fred G. Barker II, M.D.
INTRODUCTION: We assessed the results of extracranial-to-intracranial (EC-IC) bypass surgery in the treatment of occlusivecerebrovascular disease and intracranial aneurysms in the UnitedStates between 1992 and 2001 using population-based methods.
METHODS: This was a retrospective cohort study using the Na-tionwide Inpatient Sample (Healthcare Cost and Utilization Project,Agency for Healthcare Research and Quality, Rockville, MD). Statis-tical methods included multivariate ordinary and proportional-oddsordinal logistic regression with adjustment for clustering of outcomes.
RESULTS: In all, 558 operations were performed at 158 hospitals by145 identified surgeons. For 74% of operations, the indication was cere-bral ischemia (2.4% mortality); 19% were for unruptured aneurysms(7.7% mortality) and 7% for ruptured aneurysms (21% mortality). Over-all, 4.6% died, 4.6% were discharged to long-term facilities, 16.5% toshort-term facilities, and 74% home. The annual number of admissions inthe United States increased from 190/year (1992–1996) to 360/year(1997–2001), whereas mortality rates increased from 2.5% (1992–1996) to5.9% (1997–2001). The median annual number of procedures was 3 perhospital (range, 1–27) or 2 per surgeon (range, 1–21). For 29% of patients,their bypass was the only one recorded at that hospital that year; for theseinstitutions, the average annual caseload was 0.4 admissions/year. For42% of patients, their surgeon performed no other bypass that year.Older age (P ! 0.001) and black race (P " 0.005) were risk factors foradverse outcome. In multivariate analysis adjusted for age, sex, race,diagnosis, admission type, geographic region, medical comorbidity, andyear of surgery, higher-volume hospitals had less frequent adverse dis-charge disposition (odds ratio, 0.54; P " 0.03).
CONCLUSION: Most EC-IC bypasses in the United States in thelast decade were performed for occlusive cerebrovascular disease.Actual surgical mortality rates in the United States medical commu-nity currently exceed published values for EC-IC bypass from special-ist centers in the setting of aneurysms and probably ischemic cerebro-vascular disease as well, and mortality rates are increasing over time.This technically demanding procedure has become a very low-volumeoperation at nearly all United States centers.
701Determinants of Intellectual Outcome after SurgicalRevascularization in Pediatric Moyamoya Disease:A Multivariate AnalysisKuroda Satoshi, M.D., Houkin Kiyohiro, M.D.,Ishikawa Tatsuya, M.D., Iwasaki Yoshinobu, M.D.
INTRODUCTION: Various surgical procedures have been reportedfor pediatric patients with moyamoya disease. However, their intel-lectual outcome is still unsatisfactory. The aim of this study was toclarify predictors for poor intellectual outcome in pediatric moya-moya disease.
METHODS: Fifty-two pediatric patients were included. Clinical
diagnosis was transient ischemic attack in 35 and completed stroke in17. Ten patients underwent indirect synangiosis through “small cra-niotomy” limited in the temporoparietal region. Another 42 under-went superficial temporal artery-middle cerebral artery anastomosisand indirect synangiosis through “large craniotomy” extending to thefrontal region. Full-scale IQ (FSIQ) was measured using the WechslerIntelligence Scale for Children after surgery. Multivariate logistic re-gression models were applied to test the effect of clinical factors onintellectual outcome. Patient sex, onset age, preoperative diseasedperiod, cerebral infarction, disease type, and procedure of bypasssurgery were analyzed as the possible factors.
RESULTS: Eight patients revealed mentally impaired status (FSIQ !70). Multivariate analysis revealed that completed stroke and small cra-niotomy surgery were significantly associated with poor intellectual out-come. Odds ratios of each factor were 33.4 (95% CI, 2.4–474) and 19.6(95% CI, 1.8–215), respectively. Other factors had no significant impact.Postoperative single photon emission computed tomography revealedthat the small craniotomy group had significantly lower blood flow (P !0.0001) and reactivity to acetazolamide (P ! 0.05) in the bilateral frontallobes than the large craniotomy group.
CONCLUSION: The present results suggest that early diagnosisand the revascularization procedure over as wide as area as possiblemay be essential to improve their intellectual outcome.
702Temporal Variation of Induction Neurogenesisin a Rat Model of Transient Middle CerebralArtery OcclusionJohn M. Abrahams, M.D., Dheeraj Khurana, M.D.,Christopher J. Lenart, M.D., Solen Gokhan, M.D.,Mark F. Mehler, M.D.
INTRODUCTION: Recent studies have shown that the adult brainis capable of neurogenesis in the presence of ischemia. We investi-gated the presence of new neural precursors after transient middlecerebral artery ischemia adult rats.
METHODS: Transient middle cerebral artery ischemia was induced inadult Wistar Rats (n " 13) using the monofilament method. In theexperimental group (n " 8), animals were killed at days 3, 7, 10, 17, and21 after inducing ischemia, and five animals served as controls. Sagittalsections through the ischemic cortex were double-stained for neural(nestin and !-tubulin, nestin and proliferating cell nuclear antigen[PCNA]), glial (nestin and glial fibrillary acidic protein [GFAP]), andoligodendroglial (nestin and O4, CNP and PCNA) precursors. Double-stained cells were also counted under high-power view and tabulated.
RESULTS: In the subventricular zone (SVZ), there was positivedouble-staining starting at 3 days showing proliferating astrocyticprecursors (nestin # GFAP, 5–20% of cells), neuronal stem cells (nes-tin # PCNA, 95% of cells), and neuronal precursors (nestin #!-tubulin, 50% of cells). There was a more robust response within thepenumbra along the stroke border zone. There were more astrocyticprecursors (50–80% of cells), premature as well as more differentiatedoligodendrocytes, neuronal stem cells (85% of cells), and neuronalprecursors (15% of cells). There was an intermediate response withinthe stroke bed also. There were more astrocytic precursors (10–20% ofcells), premature oligodendrocytes (45–100% of cells), neuronal stemcells (95% of cells), and neuronal precursors (25% of cells). Resultswere confirmed with cell counting analysis.
452 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

CONCLUSION: Our results show that not only do neural precur-sors proliferate in the SVZ and general cortex, but there is also adefinite response in the penumbra and ischemic cortex.
703Endosaccular Treatment of Intracranial AneurysmsUsing a New Hydrogel-coated Self-expandable Coil(HydroCoil): Early Experience from a SingleLarge-volume CenterJonathan L. Brisman, M.D., Joon K. Song, M.D.,Yasunari Niimi, M.D., David Langer, M.D.,Mark J. Kupersmith, M.D., Patricia Fernandez, M.D.,Alejandro Berenstein, M.D.
INTRODUCTION: HydroCoils are a new generation of enhancedcoils developed for endovascular occlusion of intracranial aneurysms.These self-expanding coils are intended to result in increased volu-metric filling, thereby reducing coil compaction and aneurysm recan-alization. We review our initial experience with the technical aspectsof this coil, as well as early clinical and angiographic results.
METHODS: Data were prospectively collected on 51 intracranial saccularaneurysms (of a total of 126 aneurysms treated during this period) in 50patients treated between November 2002 and November 2003 in which atleast one HydroCoil was used. Information collected included patient ageand presentation, aneurysm location and size, initial occlusion status, clinicalstatus at discharge, number and percentage of HydroCoils used and initialand follow-up angiographic results, when available.
RESULTS: Thirty patients (59%) presented with subarachnoid hemor-rhage (SAH). Thirty-seven (73%) aneurysms were in the anterior circu-lation, and the average aneurysm diameter was 9.3 mm. There were notechnical difficulties with coil preparation or deployment. Forty-twoaneuryms (82%) had initial angiographic occlusion of $90%, with Hy-droCoils constituting an average of 68% of total coil volume. There wasangiographic follow-up in 23 aneurysms (45%) showing stable occlusionin 18 (78%) and coil compaction in 5 (22%) at a mean follow-up of 6.7months; 2 of these were recoiled, and 1 was referred for surgical clipping.Glasgow Outcome Scale score on discharge and percentage discharged tohome were similar to those for patients treated with other coils. Therewere four complications (8%) related to treatment, none with clinicalsequelae. There were two rehemorrhages.
CONCLUSION: This represents the largest series of intracranialaneurysms treated with HydroCoils. We found the coils easy to useand to have similar early angiographic and clinical results, includingcomplication and compaction rates, compared with GDC coils. Fur-ther long-term studies are needed to assess the ability of HydroCoilsto decrease recanalization rates.
704Prospective, Randomized, Multicenter Trial ofArtificial Disc versus Fusion for Single-level LumbarDegenerative Disc Disease: A 2-year Follow-upInvestigational Device Exemption StudyFred H. Geisler, M.D., Ph.D., Scott L. Blumenthal, M.D.,Paul C. McAfee, M.D., Richard D. Guyer, M.D.,Stephen H. Hochschuler, M.D., Rolando Garcia, Jr., M.D.,John J. Regan, M.D.
INTRODUCTION: Prior reports of artificial disc replacements inthe lumbar spine have been described retrospectively. We report the
first results from a randomized controlled trial of the Charite artificialdisc replacement versus fusion for the treatment of lumbar degener-ative disc diseaseat one level.
METHODS: The study was conducted after review and approvalby the United States Food and Drug Administration and each site’sinstitutional review board. All enrolled subjects had failed at least 6months of nonoperative management and were being treated forsingle-level symptomatic disc degeneration verified by radiographicdiagnostic studies, including discography. After informed consent,304 subjects from 15 centers were randomized using a 2:1 randomiza-tion scheme, with 205 subjects enrolled in the Charite group (C) and99 in the Fusion group (F) who had anterior lumbar interbody fusion(ALIF) with Bagby and Kuslich (BAK) cages and autograft. Demo-graphics were statistically similar (except for weight) between groups.All subjects were treated at one level, at either L4–L5 (C " 61, F " 32)or L5–S1 (C " 144, F " 67) via a mini-ALIF retroperitoneal approach.Clinical outcomes were determined by visual analog score (VAS),Oswestry (ODI), Short-Form 36 questionnaires, and subject satisfac-tion.
RESULTS: Mean operative time (C " 111 min, F " 114 min) andperioperative blood loss (C " 207 ml, F " 209 ml) were equivalent.The length of hospital stay was significantly less in the Charite group(3.7 versus 4.3 d) compared with the Fusion group. The VAS and ODIscores improved significantly in both groups, with the Charite groupexperiencing significantly greater improvement than the Fusion groupat all time points but the 24-month follow-up. Subject satisfaction wassignificantly higher in the Charite group (C " 77%, F " 59%). Asidefrom graft site pain in 17% of the fusion group, the complication rateswere similar for both groups.
CONCLUSION: The results of this prospective, randomized studysupports the proposition that Charite artificial disc replacement is asafe and effective alternative to fusion for one-level symptomaticlumbar disc disease in appropriately selected patients.
705Cervical Disc Arthroplasty: A Controlled,Randomized, Prospective Study with IntermediateFollow-up Results from One CenterRobert J. Hacker, M.D.
INTRODUCTION: Studies of anterior cervical fusion (ACF) fordisc-related pathology document satisfying clinical results and infre-quent complications. Outside the United States, cervical disc arthro-plasty (CDA) has increasingly been used as a treatment alternative toACF. Some think that CDA may provide superior results and achievebetter long-term outcomes, with anecdotal reports and prospectivestudies offering some support. However, no controlled randomizedstudies have documented equivalence or superiority of this new pro-cedure. This paper presents intermediate data from such a study.
METHODS: Failing conservative therapy, 46 patients with one-level discogenic cervical radiculopathy and/or myelopathy were ran-domized to CDA or ACF as part of a Food and Drug Administrationdevice study. Follow-up visits were scheduled for 1, 6, and 12 weeksand at 6, 12 and 24 months.
RESULTS: This study is in progress. Thus far, randomization hasresulted in 22 CDA and 24 ACF procedures. Surgical parameters weresimilar between groups other than operative time: CDA, 84 and ACF,50 minutes. At 1 year, pain scores were 23 and 55% of preoperativevalues for the CDA and ACF groups, respectively, with similar resultsfor Short-Form 36 data. CDA patients rated their outcome as excellent,
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 453

17; fair, 3; and rating pending, 2, whereas ACF patients reported 7excellent, 12 good, 1 fair, 2 poor, and 2 unrated. CDA complicationsincluded dysphonia (resolved) 2; wound hematoma evacuation, 1;and subsequent adjacent level fusion, 1. ACF complications includedfailed fusion, 1, and persistent myelopathy, 1. Radiographs showedthat motion was maintained in the CDA group.
CONCLUSION: Disc arthroplasty surgery seems to be an equiva-lent and possibly superior treatment for discogenic disorders of thecervical spine. It avoids the inherent morbidities of fusion. Althoughextended follow-up data and larger numbers of patients are needed,these results support CDA as a viable alternative to ACF.
706A Prospective, Randomized, Controlled Investigationof the Prestige Cervical Disc: Early Experience at aParticipating Investigational SiteWade M. Ceola, M.D., Charles Mace, M.D.
INTRODUCTION: Anterior cervical discectomy with fusion has along and successful history. Delayed problems with transitional syn-drome have been encountered and have led to development of artifi-cal disc technology. The following includes early follow-up results ofa single site involved in the Prestige Cervical Disc investigation deviceexemption (IDE) study.
METHODS: All patients included in this series were treated at asingle site by the author as the primary or assistant surgeon. Thepatients are included in an IDE clinical investigation of the PrestigeCervical Disc System sponsored by Medtronic Sofamor Danek, Mem-phis, Tennessee. The randomized, prospective study is designed toshow clinical equivalence of the treatments with a maintenance ofmotion in the investigational group in a total of 550 patients. Allpatients randomized into the study demonstrated clinical and radio-graphic evidence of single-level cervical disc disease causing painfulradiculopathy and/or myelopathy with no previous surgery. In theinvestigational group, patients are treated with Prestige Cervical Discimplanted via a modified anterior cervical technique. In the controlgroup, patients are treated by a standard anterior cervical discectomyand fusion using cortical allograft and anterior cervical plating. Ac-cording to the protocol, all patients are evaluated clinically and radio-graphically preoperatively, at discharge, and at 6 weeks and 3, 6, 12,and 24 months postoperatively. The outcomes measures used areneurological status, visual analog pain scales, the Neck DisabilityIndex, the Short-Form 36 General Health Survey, and radiographicexaminations. Rigid inclusion and exclusion criteria are adhered to.
RESULTS: At the time of this report, data from 47 patients havebeen reviewed, beginning in January 2003. Analysis includes preop-erative through 12-month follow-up. Demographic and surgical vari-ables are statistically comparable. Patients in both treatment groupsshowed improvement in all outcome measures and statistically simi-lar in both treatment groups in all categories. Early radiographicevidence shows maintenance of motion in the Prestige group andfusion rates for the control group approaching 100%.
CONCLUSION: In this series, patients treated with the Prestigedevice show improvement in all outcome measures similar to ananterior cervical discectomy and fusion (ACDF) while maintainingmotion at the treated level. The Prestige device has a simple, soliddesign with a long clinical history in Europe. The technique forimplantation of the Prestige device is straightforward and very similarto a standard ACDF, with similar risks and discomforts. Early results
are encouraging, and motion in the treated area is maintained, butlonger follow-up with more patient data is needed to see whetherdelayed ACDF complications (transitional syndrome) is avoidableand whether this treatment is to become a standard in spine care.
707Phase 1 Veterinary Trial of Intravenous/topicalPolyethylene Glycol in Naturally Occurring DogComplete Spinal Cord InjuryScott A. Shapiro, M.D., Richard Borgens, Ph.D.,Peter Laverty, D.V.M., Alena Leskovar, Ph.D.,Joan Coates, D.V.M., William Widmer, D.V.M.,James Toombs, D.V.M., Scott Purvines, M.D.
INTRODUCTION: Topical and subcutaneous polyethylene glycol(a membrane surfactant) can fuse in vitro severed axons back together,restoring electrical conduction, seal membrane defects, and improvethe functional outcome of spinal cord injury in guinea pigs. A phase1 safety trial was performed in natural occurring dog complete spinalcord injury caused by disc herniation.
METHODS: Dogs with complete spinal cord injury caused byruptured discs diagnosed within 72 hours with myelography wereeligible. A quantified total neurological examination (deep/superficialpain, proprioception, weight bearing, ambulation, and bladder con-trol) was videotaped and scored. Dogs were given intravenous poly-ethylene glycol (PEG) (3500 daltons, 2 ml/kg over 15 minutes) andintravenous methylprednisolone 30 mg/kg and then taken to surgeryfor a discectomy and durotomy with topical PEG treatment for 2minutes. Six hours after surgery, a second dose of intravenousPEG was given. The animals were studied at 3 days, 1 week, and 6weeks.
RESULTS: Nineteen dogs were treated, with no complications andno mortality. For deep and superficial pain, 4 of 19 (21%) recovered at3 days, 9 of 19 (47%) recovered at 1 week, and 10 of 19 (53%) recoveredat 6 weeks. For ambulation, 4 of 19 (21%) recovered ambulation at 1week and 13 of 19 (68%) recovered at 6 weeks. For bladder control, 13of 19 (68%) regained continence at 6 weeks. For somatosensory evokedpotentials, 64% of the dogs recovered their tibial somatosensoryevoked potential that were absent before surgery.
CONCLUSION: Intravenous and topical PEG in dog spinal cordinjury is safe and probably very effective. In previously publishedreports from our veterinary hospital documented for dogs with com-plete spinal cord injury caused by disc herniation treated with steroidsand surgery alone, only 25% recovered ambulation at 6 months. Wehave never seen such rapid and dramatic recovery. A randomizedcontrolled trial is under way in dogs, and a human phase I trial isbeing planned.
708Effect of Artificial Disc Placement on Facet Loading:Unconstrained versus SemiconstrainedMissoum Moumene, Ph.D., Fred H. Geisler, M.D., Ph.D.
INTRODUCTION: The design of an artificial disc and its surgicalplacement in the disc space dictates the path of the instantaneous axisof rotation (centrode). Changing the location of the centrode from anormal spine unit as a result of disc replacement will change thestresses and stiffness of the structural elements that govern the specific
ABSTRACTS OF OPEN PAPERS
454 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com
motion. The purpose of this study was to evaluate the effect ofartificial disc placement on facet loading using finite element analysiswith two artificial disc designs, Charite (unconstrained) and ProDisc(semiconstrained).
METHODS: A three-dimensional nonlinear finite element model ofthe intact ligamentous L4–L5 motion segment was generated andvalidated in all 6 degrees of freedom on the basis of experimentsconducted on human cadavers. Facet loading was estimated for eachrange of motion with four different prosthesis placements. The im-plants were placed in the nucleus center and offset anteriorly 6 mm,posteriorly 4 mm, and laterally 5 mm, representing the worst cases ofplacement. Imposed displacements in flexion (9 degrees), extension (3degrees), torsion (%2 degrees), and lateral bending (%5 degrees) wereapplied to the intact and implanted spinal segment while under acompressive preload of 400 N.
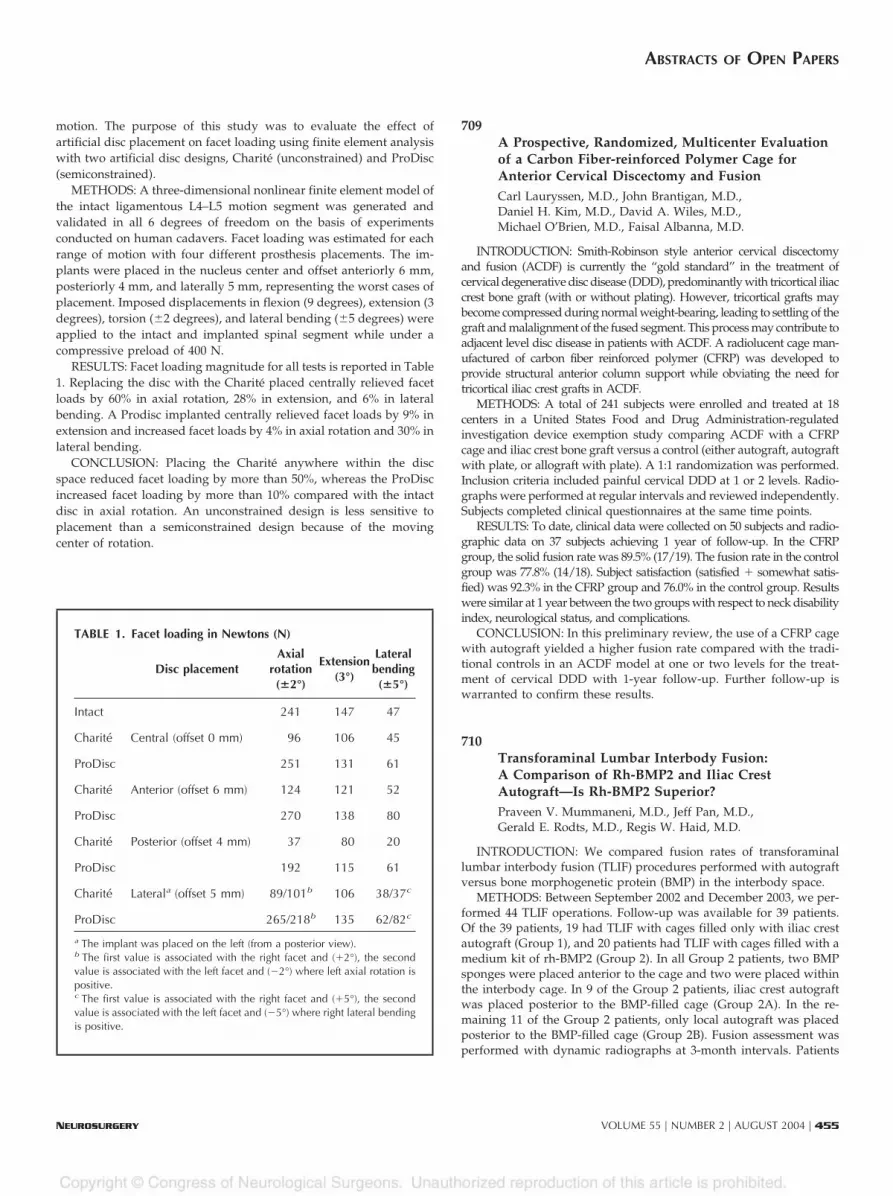
RESULTS: Facet loading magnitude for all tests is reported in Table1. Replacing the disc with the Charite placed centrally relieved facetloads by 60% in axial rotation, 28% in extension, and 6% in lateralbending. A Prodisc implanted centrally relieved facet loads by 9% inextension and increased facet loads by 4% in axial rotation and 30% inlateral bending.
CONCLUSION: Placing the Charite anywhere within the discspace reduced facet loading by more than 50%, whereas the ProDiscincreased facet loading by more than 10% compared with the intactdisc in axial rotation. An unconstrained design is less sensitive toplacement than a semiconstrained design because of the movingcenter of rotation.
709A Prospective, Randomized, Multicenter Evaluationof a Carbon Fiber-reinforced Polymer Cage forAnterior Cervical Discectomy and FusionCarl Lauryssen, M.D., John Brantigan, M.D.,Daniel H. Kim, M.D., David A. Wiles, M.D.,Michael O’Brien, M.D., Faisal Albanna, M.D.
INTRODUCTION: Smith-Robinson style anterior cervical discectomyand fusion (ACDF) is currently the “gold standard” in the treatment ofcervical degenerative disc disease (DDD), predominantly with tricortical iliaccrest bone graft (with or without plating). However, tricortical grafts maybecome compressed during normal weight-bearing, leading to settling of thegraft and malalignment of the fused segment. This process may contribute toadjacent level disc disease in patients with ACDF. A radiolucent cage man-ufactured of carbon fiber reinforced polymer (CFRP) was developed toprovide structural anterior column support while obviating the need fortricortical iliac crest grafts in ACDF.
METHODS: A total of 241 subjects were enrolled and treated at 18centers in a United States Food and Drug Administration-regulatedinvestigation device exemption study comparing ACDF with a CFRPcage and iliac crest bone graft versus a control (either autograft, autograftwith plate, or allograft with plate). A 1:1 randomization was performed.Inclusion criteria included painful cervical DDD at 1 or 2 levels. Radio-graphs were performed at regular intervals and reviewed independently.Subjects completed clinical questionnaires at the same time points.
RESULTS: To date, clinical data were collected on 50 subjects and radio-graphic data on 37 subjects achieving 1 year of follow-up. In the CFRPgroup, the solid fusion rate was 89.5% (17/19). The fusion rate in the controlgroup was 77.8% (14/18). Subject satisfaction (satisfied # somewhat satis-fied) was 92.3% in the CFRP group and 76.0% in the control group. Resultswere similar at 1 year between the two groups with respect to neck disabilityindex, neurological status, and complications.
CONCLUSION: In this preliminary review, the use of a CFRP cagewith autograft yielded a higher fusion rate compared with the tradi-tional controls in an ACDF model at one or two levels for the treat-ment of cervical DDD with 1-year follow-up. Further follow-up iswarranted to confirm these results.
710Transforaminal Lumbar Interbody Fusion:A Comparison of Rh-BMP2 and Iliac CrestAutograft—Is Rh-BMP2 Superior?Praveen V. Mummaneni, M.D., Jeff Pan, M.D.,Gerald E. Rodts, M.D., Regis W. Haid, M.D.
INTRODUCTION: We compared fusion rates of transforaminallumbar interbody fusion (TLIF) procedures performed with autograftversus bone morphogenetic protein (BMP) in the interbody space.
METHODS: Between September 2002 and December 2003, we per-formed 44 TLIF operations. Follow-up was available for 39 patients.Of the 39 patients, 19 had TLIF with cages filled only with iliac crestautograft (Group 1), and 20 patients had TLIF with cages filled with amedium kit of rh-BMP2 (Group 2). In all Group 2 patients, two BMPsponges were placed anterior to the cage and two were placed withinthe interbody cage. In 9 of the Group 2 patients, iliac crest autograftwas placed posterior to the BMP-filled cage (Group 2A). In the re-maining 11 of the Group 2 patients, only local autograft was placedposterior to the BMP-filled cage (Group 2B). Fusion assessment wasperformed with dynamic radiographs at 3-month intervals. Patients
TABLE 1. Facet loading in Newtons (N)
Disc placementAxial
rotation(!2°)
Extension(3°)
Lateralbending(!5°)
Intact 241 147 47
Charite Central (offset 0 mm) 96 106 45
ProDisc 251 131 61
Charite Anterior (offset 6 mm) 124 121 52
ProDisc 270 138 80
Charite Posterior (offset 4 mm) 37 80 20
ProDisc 192 115 61
Charite Laterala (offset 5 mm) 89/101b 106 38/37c
ProDisc 265/218b 135 62/82c
a The implant was placed on the left (from a posterior view).b The first value is associated with the right facet and (#2°), the secondvalue is associated with the left facet and (&2°) where left axial rotation ispositive.c The first value is associated with the right facet and (#5°), the secondvalue is associated with the left facet and (&5°) where right lateral bendingis positive.
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 455

were followed up to assess for any new lumbar radiculopathies and toassess iliac crest donor site pain (Visual Analog Scale).
RESULTS: Mean follow-up was 6 months (range, 3 to 18 months).Of the Group 1 patients, there was one pseudoarthrosis. Of the Group2 patients, all achieved a solid fusion on dynamic radiographs 3months after surgery (no difference between Group 2A and Group2B). No patient complained of new radiculopathy during thefollow-up period. Of the patients in whom iliac crest autograft wasused, 58% complained of donor site pain 6 months after surgery (5/10Visual Analog Scale).
CONCLUSION: Rh-BMP2 is safe for use in TLIFs when thesponges are placed away from the dura, and BMP promotes a morerapid fusion than does iliac autograft alone. The use of rh-BMP2 incombination with local autograft is an excellent option to achieve asolid fusion with the TLIF procedure and eliminates the possibility ofiliac donor site pain.
711Spine Stereotactic Radiosurgery:Evaluating Toxicity and EfficacyDeborah L. Benzil, M.D., Mehran Saboori, M.D.,Ronald Rocchio, M.S., Chitti R. Moorthy, M.D.,Alon Mogilner, M.D., Ph.D.
INTRODUCTION: Extending stereotactic radiosurgery (SRS) to thespine has the potential to benefit many patients. As in the early daysof cranial SRS, however, dose-response and toxicity are not wellunderstood. We report our initial experience with spine SRS withattention to dose, outcome, and toxicity.
METHODS: All patients treated with spine SRS with Novalis atWestchester Medical Center are included in a database with pertinentpatient, disease, dose, outcome, and complications.
RESULTS: A total of 31 patients received treatment for 35 tumors.There were 13 men and 21 women (mean age, 61 yr; median, 63 yr).Tumors included 26 metastases (lung 12, breast 9) and 8 primary (4intradural). Thoracic tumors were most common (17 metastases, 4primary), followed by lumbar (4 metastases, 4 primary). Nearly all(32/34) had rapid and significant pain relief. In patients with metas-tases, pain relief started in less than 72 hours and remained durable at3-month follow-up. Pain relief was seen at a single dose as low as 500cGy. Spinal cord isodose was less than 50% in all patients except thosewith intradural tumors (mean single dose, 268 cGy; mean total dose,689 cGy). Two patients experienced transient radiculitis (both withbiological equivalent dose [BED] $60 Gy). One patient with a multi-ply recurrent conus ependymoma had permanent neurological dete-rioration after initial improvement. Pathology revealed radiation ne-crosis with some residual/recurrent tumor. No patient experiencedother organ toxicity.
CONCLUSION: Spine SRS has significant benefit, especially forpain relief, with minimal risk of complications. BEDs $60 Gy areassociated with a higher risk of radiculitis.
712Neurogenesis in Adult Human Neocortical EpilepsyJorge A. Gonzalez-Martinez, M.D., Ph.D.,Gabriel Moddel, M.D., Imad M. Najm, M.D.,Hans O. Luders, M.D., Ph.D., William E. Bingaman, M.D.
INTRODUCTION: Neurogenesis has been described in specificareas in the normal human brain. This study was undertaken to
investigate whether neurogenesis occurs in epileptogenic areas inpatients with intractable epilepsy.
METHODS: We studied 14 patients (mean age, 19.1 yr) with med-ically intractable epilepsy who underwent epilepsy surgery. Duringsurgical resections, en bloc cortical and subcortical samples were col-lected and cultured with bromodeoxyuridine (BrdUrd) (a marker forproliferating cells) for 24, 48, and 72 hours. Cultured slices were laterfixed for immunocytochemistry (ICC) and immunofluorescence (fordouble labeling). For ICC, primary antibodies were anti-BrdUrd, anti-Tuj1, anti-GFAP, anti-nestin, and anti-CD133.
RESULTS: Histology revealed malformations of cortical develop-ment (MCD) in eight patients: two patients with hemimegalencephalyand five with focal cortical dysplasia. Perinatal infarction (PI) wasconfirmed in three patients, and two had the diagnosis of gliosissecondary to trauma. Eight patients were analyzed as controls (nor-mal temporal cortex). There was remarkable evidence of BrdUrduptake in five of eight patients with MCD and in three of threepatients with PI. Positive BrdUrd samples were located in frontal,parietal, and occipital lobes. BrdUrd immunoreactivity was observedin the entire length of the analyzed samples, from periventricular zone(PVZ) to cortical surface. In samples cultured for 24 hours, intenseexpression was observed in the PVZ, with progressive decrement inBrdUrd expressivity toward the cortical surface. In 48- and 72-hoursamples, more widely spread BrdUrd immunoreactivity was ob-served, with presence of extensive BrdUrd-stained cells in white mat-ter. Colocalized BrdUrd and nestin immunoreactivity was present inthe PVZ but not in cortical areas. BrdUrd and Tuj1 colocalization wasobserved in the entire length of the cortical mantle.
CONCLUSION: Our results demonstrate, for the first time, neuro-genesis in adult human epileptic neocortex. Our findings corroboratetheories addressing mechanisms of epileptogenicity in congenital ep-ilepsy, in which new added neurons may play a crucial role in genesisand maintenance of neocortical seizures.
713Reoperation in Failed Epilepsy SurgeryJorge A. Gonzalez-Martinez, M.D., Ph.D.,Teeradej Srikijvilaikul, M.D., William E. Bingaman, M.D.
INTRODUCTION: Treatment of patients who fail epilepsy surgeryis challenging, because there are few other treatment options availablefor this group of patients. Indeed, many of these patients may becandidates for further resective surgery. The purpose of this study isto analyze seizure outcome of reoperated patients and identify poten-tial variables that predicted satisfactory outcome after reoperation forepilepsy surgery.
METHODS: Between 1990 and 2001, 70 patients with medicallyintractable epilepsy underwent reoperation at our institution afterfailed resective surgery. The first surgery was performed between1980 and 2001. Follow-up ranged from 1 to 7 years (mean, 3.2 % 2.2 yr;median, 2.5 yr), and seizure outcomes were classified according toEngel’s classification. Fifty-seven patients with a minimum of 1-yearfollow-up were included for analysis. Factors associated with seizureoutcome were studied. "2 and Fisher’s exact tests were applied forstatistical analysis. Statistical significance was set at a value of P "0.05.
RESULTS: Histopathology of reoperated cases included tumors(31.6%), cortical dysplasia (CD) (21.1%), hippocampal sclerosis(17.5%), dual pathology (10.5%), and nonspecific pathology (19.3%).There were no significant differences in outcome in patients under-
ABSTRACTS OF OPEN PAPERS
456 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

going temporal versus extratemporal lobe reoperations. Febrile sei-zures, family history of seizures, or the seizure-free period after thefirst surgery were not predictive of persistent seizures after reopera-tion. Fifty percent of the patients had favorable outcomes (Engel I andII) after reoperation. Patients with tumors, CD as initial pathology,and reoperation at the previous resection site had better outcomes,although this did not reach statistical significance.
CONCLUSION: Our results indicated that half of the patientsfailing resective epilepsy surgery potentially benefit from reoperation.Favorable prognostic factors included neoplastic disease, presence ofcortical dysplasia, and reoperation at the previous resection site. Nomortality and acceptable morbidity occurred related to reoperation.
714Real-time, in Vivo Imaging of ConvectiveDistribution of a Low-molecular-weight TracerDavid Croteau, M.D., Stuart Walbridge, B.S.,Paul F. Morrison, Ph.D., John A. Butman, M.D., Ph.D.,Alexander O. Vortmeyer, M.D., Dennis Johnson, M.B.A.,Edward H. Oldfield, M.D., Russell R. Lonser, M.D.
INTRODUCTION: Convection-enhanced delivery (CED) is increas-ingly used to distribute therapeutic agents in the central nervoussystem. Optimal application of convective distribution of variousagents requires the development of imaging tracers to monitor CED inreal time in vivo. We examined the safety and utility of an iodine-based low-molecular-weight surrogate tracer for computed tomo-graphic (CT) imaging during CED.
METHODS: Four primates (Macaca mulatta) underwent CED ofvarious volumes (total volume, 90–150 #l) of iopamidol (777 Da) in thecerebral white matter. The distribution of this imaging tracer deliv-ered by CED was determined by serial in vivo, real-time (all animals),and postinfusion CT imaging (up to 5 days after infusion), as well asquantitative autoradiography (QAR; [14C]sucrose and [14C]dextran),and compared with a mathematical model. Clinical observation (up to5 months) and histopathological analysis were used to evaluate safetyand toxicity.
RESULTS: Real-time CT imaging of the tracer during infusionrevealed a clearly definable region of perfusion. The volume of dis-tribution (Vd) increased linearly (R2 " 0.97) with increasing volume ofinfusion (Vi). The overall Vd:Vi ratio was 4.1 % 0.7 (mean % standarddeviation). The distribution of infusate was homogeneous. QAR con-firmed the accuracy of the imaged distribution for a small (sucrose;359 Da) and a large (dextran; 70 kDa) molecule. The distribution ofinfusate was identifiable up to 72 hours after infusion. None of theanimals had clinical or histopathological evidence of toxicity.
CONCLUSION: Real-time, in vivo, CT imaging of CED using iop-amidol seems to be safe, feasible, and suitable for monitoring convec-tive delivery of drugs with certain features and low infusion volumes.
715Multipotent Astrocytes Mature into Neurons in theAdult Mammalian BrainDean D. Lin, M.D., Bjorn Scheffler, M.D., Noah Walton, B.Sc.,Katrin Goetz, M.D., Dennis Steindler, Ph.D.,Steven Roper, M.D.
INTRODUCTION: For the past decade, neural stem/precursorcells native to the adult mammalian subventricular zone (SVZ) have
been studied as an inducible source to generate newborn neurons andglia. Until now, however, there has been a surprising shortage of datacharacterizing the cellular nature of these multipotent precursors. Inthis study, we used morphological and electrophysiological methodsto characterize the transitional events of neurogenesis as an astrocyte-like SVZ cell population developed into functional neurons.
METHODS: Young postnatal and adult rats were killed, andastrocyte-like cells from the SVZ were harvested and cultured inmedia containing fibroblast-derived growth factor and epidermalgrowth factor. Under these conditions, these cells maintain their mul-tipotentiality and proliferative capacity for extended passages in cul-ture. Upon withdrawal of growth factors, however, spontaneous dif-ferentiation occurs. Immunohistochemical and whole-cell patch-clamp techniques were used to evaluate their differentiation intoneuronal phenotypes over a period of 4 weeks.
RESULTS: Withdrawal of growth factors resulted in both a dra-matic change in morphologies and characteristic membrane propertyalterations. Within 2 to 3 days after withdrawal, multiple rapid celldivisions generated a cell phenotype similar to primitive neuroblasts.
CONCLUSION: We describe here morphological and functionalcellular transitions of neurogenic multipotent astrocytes. Large num-bers of these self-renewing SVZ cells can be generated, and subse-quently, these cells may eventually serve as a potential donor sourcein the treatment of CNS disease.
716Defining the Role of Stereotactic Radiosurgery in theManagement of Newly Diagnosed, Multiple (Threeor More) Intracranial Metastases: Is Whole BrainRadiation Necessary?Mark Shaya, M.D., Ajay Jawahar, M.D., Peter Campbell,Federico Ampil, M.D., Brian Willis, M.D.,Donald Smith, M.D., Anil Nanda, M.D.
INTRODUCTION: To assess the role of stereotactic radiosurgery inthe management of newly diagnosed multiple (three or more) intra-cranial metastases from known primary cancer location by retrospec-tively analyzing the overall survival and control of brain disease inpatients from a single institution.
METHODS: One hundred thirty-nine patients received radiosur-gery with the Leksell gamma knife at our institution for metastaticbrain disease. Of these, 88 patients had newly diagnosed (1 month orless) metastatic brain disease and, of these, 50 patients (29 women and21 men) had 3 or more tumors at the first referral. Mean age was 53years (range, 35–77 yr). Lung cancer was the most common primarycancer (66%), followed by breast, melanoma, kidney, and colon can-cers. A retrospective analysis was performed for survival after diag-nosis of brain disease and brain disease-controlled period as theprimary outcomes.
RESULTS: Thirty-two patients had died at the last follow-up. Ar-rest in growth (control) of irradiated tumors was achieved in 41patients (82%). Eight patients (16%) required further intervention(stereotactic radiosurgery/external beam radiation therapy [XRT]) fornew tumors at other brain locations 2 to 24 months after the firstprocedure. Mean survival after diagnosis of brain disease was 12months (95% CI, 8–15 mo), and the brain disease-controlled periodwas 19 months (95% CI, 15–24 mo). Control of treated tumors posi-tively affected the survival after diagnosis of brain disease (P "0.0001).
CONCLUSION: Radiosurgery as adjuvant definitely improves sur-
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 457

vival in cancer patients with newly diagnosed multiple (three ormore) intracranial metastases by arresting the growth of tumors. Theoverall survival was significantly less in patients receiving XRT. Inaddition, XRT did not contribute toward control of the brain disease.
717Decreased Glutamine Synthesis in Human TemporalLobe Epilepsy: Chicken or Egg?Guy M. McKhann, M.D., Xiaoping Wu, Ph.D.,Robert R. Goodman, M.D., Ph.D.,Peter D. Crino, M.D., Ph.D., Alexander A. Sosunov, M.D.
INTRODUCTION: The mechanisms and consequences of raisedextracellular glutamate in the epileptic hippocampus are importantareas of epilepsy investigation. It was recently reported that deficiencyin the astrocytic enzyme glutamine synthetase (GS) is a possibleexplanation for elevated extracellular glutamate and seizure initiationin mesial temporal lobe epilepsy (MTLE). We studied astrocytes fromresected human temporal lobe epilepsy to determine whether alter-ations in GS are more likely a primary pathophysiological contributoror are secondary to coexisting alterations present in the epileptichippocampus.
METHODS: Resected human hippocampi from MTLE (n " 11) andnon-MTLE (n " 6) patients were studied by a combination of quan-titative immunohistochemistry and acute hippocampal slice electro-physiology. We investigated glutamate uptake and glutamine synthe-sis by epileptic astrocytes.
RESULTS: Astrocytes from non-MTLE epileptic hippocampi have ahigh level of expression of glutamate transporters and GS and corre-spondingly demonstrate inward transporter currents in response toexogenous glutamate application. In contrast, in areas with prominentneuronal loss and astrogliosis in the MTLE epileptic hippocampus,there is markedly decreased expression of both of the astrocytic glu-tamate transporters, EAAT1 (not shown) and EAAT2 (P ! 0.001versus non-MTLE, paired t test). This decrease directly parallels theobserved downregulation of GS in astrocytes in these areas. Ourimmunolabeling and quantitative immunohistochemical results aresupported by the finding of little to no inward glutamate-inducedcurrent in individual astrocytes recorded in areas of sclerosis in acutehippocampal slices from MTLE patients.
CONCLUSION: Our results demonstrate that there is decreasedglutamate transporter expression together with impaired glutamateuptake by astrocytes in areas of decreased glutamine synthetase inMTLE. These findings suggest that downregulation of GS in MTLE isa secondary phenomenon in response to glutamate not entering epi-leptic astrocytes, rather than a primary enzymatic defect. Defectiveglial glutamate uptake has also been implicated in astrocytic tumorgrowth, neurotoxicity, and seizures.
718Frameless Stereotactic Ventriculoperitoneal Shuntingfor Pseudotumor Cerebri: An Outcomes Comparisonversus Lumboperitoneal ShuntingMatthew J. McGirt, M.D., Graeme Woodworth, B.S.,George Thomas, M.D., Neil Miller, M.D.,Michael Williams, M.D., Daniele Rigamonti, M.D.
INTRODUCTION: Cerebrospinal fluid (CSF) shunting acutely re-verses symptoms of pseudotumor cerebri (PTC). Long-term outcome
remains uninvestigated. Lumboperitoneal (LP) shunts are the main-stay of CSF shunting for PTC; however, image-guided stereotaxy mayallow effective ventricular catheter placement without ventriculo-megaly in PTC. The feasibility of stereotactic ventriculoperitoneal (VP)shunting and its comparison versus LP shunting remains unstudied inPTC.
METHODS: Between 1973 and 2000, 21 consecutive patients re-ceived 79 LP shunts for pseudotumor PTC-associated intractableheadache (HA). Between 2000 and 2004, 21 consecutive patients un-derwent 36 VP shunt surgeries with frameless stereotactic imageguidance despite the absence of ventriculomegaly in all patients.Shunt revision and complication rates were compared between LPand VP shunting, and predictors of treatment failure (continued HAdespite properly functioning shunt) were assessed usingproportional-hazards regression analysis.
RESULTS: Forty patients (95%) experienced significant improve-ment of HA immediately after shunting. Severe HA recurred despiteproperly functioning shunt in 8 (20%) and 20 (48%) patients 12 and 36months after initial shunt surgery. Patients without papilledema (n "17) or with symptoms $2 years (n " 19) were 5-fold (RR, 5.2; 95% CI,1.5–17.8; P ! 0.01), and 2.5-fold (RR, 2.51; 95% CI, 1.01–9.39; P " 0.05)more likely to experience HA recurrence. LP versus stereotactic VPshunting was associated with a 2.5-fold increased risk of shunt revi-sion (RR, 2.5; 95% CI, 1.4–4.3; P ! 0.005), because of a 2.8-fold in-creased risk of shunt obstruction (RR, 2.7; 95% CI, 1.4–5.4; P ! 0.01)but similar risk of overdrainage (RR, 2.4; 95% CI, 0.7–8.5; P " 0.17),distal catheter migration (RR, 2.4; 95% CI, 0.3–21.3; P " 0.45), andshunt infection (RR, 1.5; 95% CI, 0.2–15.1; P " 0.70).
CONCLUSION: In our 30-year experience, the largest reported todate, CSF shunts were extremely effective at acutely treating PTC-associated intractable HA, providing long-term relief in the majorityof patients. Lack of papilledema and long-standing symptoms wererisk factors for treatment failure. This is the first comparison of ste-reotactic VP versus LP shunts and suggests that VP shunts placedwith image-guided stereotaxy are associated with lower risks of shuntobstruction and revision. Using stereotactic VP shunts in patients withpapilledema should be considered for patients with PTC-associatedintractable HA.
719Ventriculoperitoneal Shunting for IdiopathicNormal-pressure Hydrocephalus: Predictorsof Treatment Response and Analysisof Long-term OutcomesAlexander Coon, M.D., Matthew J. McGirt, M.D.,Graeme Woodworth, B.S., George Thomas, M.D.,Michael Williams, M.D., Daniele Rigamonti, M.D.
INTRODUCTION: Because of the difficulty in distinguishing idio-pathic normal-pressure hydrocephalus (INPH) from other neurode-generative conditions unrelated to cerebrospinal fluid (CSF) dynamicpathology, outcome after CSF shunting for presumed INPH remainshighly variable. Whereas secondary NPH often responds to shunting,INPH is still considered by most to be an untreatable disease. We setout to elucidate predictors of outcome and characterize long-termoutcome after CSF shunting for INPH.
METHODS: INPH patients with computed tomography-documented hydrocephalus, normal opening lumbar-puncture CSFpressure, two clinical features of INPH (gait, urinary, or dementia),demonstrating frequent B waves on continuous lumbar CSF pressure
ABSTRACTS OF OPEN PAPERS
458 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

monitoring, and improving with 3-day trial of lumbar CSF drainageunderwent CSF shunting. Patients were clinically followed up for 1, 3,6, and 12 months after surgery.
RESULTS: One hundred thirty-two patients underwent 179 shuntsurgeries; 44 (33%), 79 (60%), and 99 (75%) patients experiencedsymptomatic improvement 3, 6, and 24 months after shunting. Gaitimprovement was the first clinical response in 88 patients (93%)responding to CSF shunting. Dementia and urinary incontinence weretwofold less likely to improve versus gait abnormalities (RR, 0.49; 95%CI, 0.4–0.9). Radiological evidence of corpus callosum impingement(RR, 1.64; 95% CI, 1.05–2.58), gait pathology as the primary symptom(RR, 1.91; 95% CI, 1.04–3.49), and decreasing duration of INPH symp-toms in years (RR, 1.15; 95% CI, 1.04–1.27) were associated withimprovement after CSF shunting. In multivariate analysis, duration ofsymptoms (RR, 0.89; 95% CI, 0.82–0.98) and gait as the primary deficit(RR, 1.87; 95% CI, 1.02–3.43) were independent predictors of outcomeafter CSF shunting for NPH.
CONCLUSION: Shunting INPH patients with B waves on CSFpressure monitoring who improve with 3-day CSF drainage resultedin symptomatic improvement in the majority of cases (75%). Corpuscallosum impingement on magnetic resonance imaging, gait abnor-malities as the primary symptom, and shorter duration of symptomspredicted improvement with CSF shunting. This series of shuntedINPH patients is the largest to date and dispels the notion that INPHis an untreatable disease.
720Granulocyte Macrophage Colony-stimulating FactorDecreases Apoptosis and Improves NeurologicalFunctions in Spinal Cord-injured RatsYoon Ha, Yoon Seung-Hwan, Dong-Keun Hyun,Eun Young Kim, Hyung Chun Park, Chong Woon Park
INTRODUCTION: The transplantation of bone marrow cells intoan injured spinal cord improves neurological functions in experimen-tal animals. Granulocyte macrophage colony-stimulating factor (GM-CSF) is a potent cytokine that is commonly used for patients withhematological disease. Biological actions of GM-CSF are to stimulatestem cell proliferation in the bone marrow and to inhibit apoptotic celldeath in leukocytes. However, the effect of GM-CSF in the centralnervous system is not yet known. This present study is designed todetermine whether GM-CSF can rescue neuronal cells from undergo-ing apoptosis and improve neurological functions in a spinal cordinjury (SCI) model.
METHODS: To study the effect of GM-CSF treatment on apoptoticneuronal death, we conducted a test, using a staurosporin-inducedneuronal death model in an N2a cell line (in vitro) and a SCI model (invivo). To inhibit the effect of GM-CSF on N2a cells, we pretreatedneutralizing antibodies against GM-CSF receptor for 60 minutes. Ter-minal deoxynucleotidyl transferase-mediated deoxyuridine triphos-phate nick end-labeling (TUNEL) staining was performed to confirmapoptosis. SCI was made by using a model of clip compression injury.Daily GM-CSF (20 #g/d) administration was performed immediatelyafter the injury and lasted for 5 days. The number of apoptotic celldeaths in the spinal cord was counted every 5 days after the injury.Neurological improvements were checked for 4 weeks.
RESULTS: GM-CSF pretreatment significantly protected N2a cellsapoptosis. Neutralizing antibodies against GM-CSF receptors inhib-ited the rescuing effect of GM-CSF. In the case of a rat SCI model,neurological functions improved more significantly in the GM-CSF-
treated group. TUNEL staining showed that the GM-CSF administra-tion decreased the amount of apoptosis in the injured spinal cord.
CONCLUSION: The treatment of SCI with GM-CSF administrationshowed some beneficial effects. Neuronal protection against apoptosisis one of the suggested mechanisms for therapeutic advantages inGM-CSF administration for SCI patients.
721Normoxic Ventilatory Resuscitation after ControlledCortical Impact Reduces Reactive Oxygen Species-mediated Protein Nitration in the HippocampusEdward S. Ahn, M.D., Gary Fiskum, Ph.D.
INTRODUCTION: Resuscitation with 100% ventilatory O2 is rou-tinely initiated after severe traumatic brain injury (TBI). Despite theobjective to improve oxygenation of injured brain, there are concernsabout the increased production of reactive oxygen species (ROS) thatleads to further neuronal damage. 3-Nitrotyrosine (3-NT), the productof peroxynitrite-meditated tyrosine residue nitration, has been used asa marker for ROS-mediated oxidative damage to proteins. We com-pared resuscitation with normoxic ventilation (FiO2, 21%) versus re-suscitation with FiO2 100% for levels of oxidative stress after TBI byquantifying the presence of 3-NT.
METHODS: Thirteen male Sprague-Dawley rats were divided intothree groups: 1) normoxic (FiO2 21%) ventilatory resuscitation for 1hour after controlled cortical impact (CCI); 2) hyperoxic resuscitation(FiO2 100%) for 1 hour after impact; and 3) a sham-operated groupthat received hyperoxic resuscitation without CCI. At 24 hours afterinjury, animals were perfused with paraformaldehyde, and hip-pocampi were evaluated for levels of 3-NT immunostaining.
RESULTS: Mean PaO2 measurements during resuscitation of nor-moxic, hyperoxic, and sham-operated groups were 114.5 % 8.4 (stan-dard error of the mean), 356.0 % 26.8, and 349.5 % 21.9, respectively.Immunostaining and quantification with the 3-NT antibody 24 hoursafter injury revealed a significant reduction of intensity with normoxiccompared with hyperoxic resuscitation in the CA1 hippocampal re-gion by 51.0% and in the CA3 region by 50.8% (n " 4 to 5, P ! 0.05).There was no significant difference in intensity in the dentate gyrus orin the hippocampus contralateral to the injured cortex.
CONCLUSION: In this clinically relevant model of TBI, normoxicresuscitation with FiO2 21% significantly reduced levels of oxidativedamage to proteins compared with FiO2 100%. These findings indicatethat hyperoxic ventilation in the early stages after severe TBI mayexacerbate oxidative brain injury.
722Human Recombinant Factor VII for EmergencyReversal of Coagulopathy in Neurosurgical PatientsBen Roitberg, M.D., Obinna Kennedy, B.A.,Sepideh Amin-Hanjani, M.D.
INTRODUCTION: Severe coagulopathy in neurosurgical patientsis a common and serious problem. The mainstay of emergency ther-apy is fresh-frozen plasma (FFP) and vitamin K. These are not alwaysrapid enough. Recently, human recombinant factor VII has been usedto reverse coagulopathy, but data are still limited on its safety andefficacy.
METHODS: We report the use of factor VII to reverse coagulopathyin 29 neurosurgical patients (FVII group); 24 other patients treated
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 459

before introduction of factor VII, or who received no factor VII be-cause of physician preference, served as controls. Factor VII was useda second-line therapy after initial attempts at reversal with FFP hadfailed.
RESULTS: There were no significant differences in baseline vari-ables between the groups (P $ 0.5): FVII versus controls: age 60 versus57 years, 55% versus 58% male, 14 of 29 (48%) versus 9 of 24 (38%)with warfarin-induced coagulopathy, 20 of 29 (69%) versus 17 of 24(71%) presented with intracranial hemorrhage. The mean interna-tional normalized ratio (INR) upon admission was 2.33 versus 2.15(P $ 0.5). After initial FFP, before administration of factor VII, INRdecreased to 1.67 % 0.18 (mean % standard error of the mean) in theFVII group and 1.85 % 0.22 in controls. INR tended to rise againrapidly after the initial infusion of FFP in both groups and in the FVIIgroup was back to a mean of 2.20 before factor VII administration. Inthis group, 1.2 mg of factor VII resulted in immediate normalization ofINR to a mean of 1.12 (P ! 0.05). Three of 29 (10%) in the FVII groupand 4 of 24 (17%) of the control group died. One patient in the controlgroup developed deep vein thrombosis; there were no thromboticcomplications in the FVII group.
CONCLUSION: Factor VII seems to be safe and highly effectivewhen emergency reversal of coagulopathy is desired in neurosurgicalpatients. We speculate that the use of factor VII as first-line therapymay expedite normalization of INR and result in decreased use of FFP.
723Antimicrobial-impregnated External VentricularCatheters: Does the Very Low Infection RateObserved in Clinical Trials Apply to DailyClinical Practice?Chris A. Sloffer, M.D., Lori Augspurger, B.S.N., R.N.,Anne Wagenbach, M.S.N., R.N., Giuseppe Lanzino, M.D.
INTRODUCTION: A recent multicenter, randomized, prospectivestudy using antimicrobial-impregnated ventricular catheters (AIVCs)has demonstrated a dramatic reduction in the incidence of catheter-related infections. By necessity, such trials are subject to notoriouslyclose and careful monitoring; thus, results of multicenter, randomizedclinical trials do not automatically apply to daily clinical practice. Theaim of the present study was to establish whether the very lowincidence of ventriculitis with antimicrobial-impregnated cathetersreported in these trials is also observed in routine clinical practice.
METHODS: Data on 139 consecutive patients admitted to a neuro-critical intensive care unit who underwent placement of 154 antibiotic-impregnated ventricular catheters were collected prospectively. Allpatients included in the data analysis had an AIVC for at least 48hours, and cultures as well as cell counts were obtained from thecerebrospinal fluid at various intervals after placement of the AIVC.
RESULTS: One hundred thirteen catheters in 100 patients metcriteria for inclusion in the analysis. There were four positive cultures.In three patients, the culture result was thought to be a contaminant(because it was not corroborated by clinical findings or cell count, orbecause of the characteristics of the culture). Only one gram-negativeinfection was considered to be clinically significant (0.88% of cathe-ters, 1.00% of patients) and confirmed on clinical and other laboratorygrounds.
CONCLUSION: The very low infection rate with currently avail-able AIVCs observed in rigorously controlled clinical trials translatesto routine clinical practice. AIVCs should be strongly consideredwhenever external ventricular drainage is indicated.
724Injury Patterns from Operation Iraqi Freedom Seenat Walter Reed Army Medical Center and NationalNaval Medical CenterChris Neal, M.D., Randy Bell, M.D., Mario Cardoso, M.D.,Ross Moquin, M.D., James Ecklund, M.D.
INTRODUCTION: Operation Iraqi Freedom (OIF) started on March20, 2003. Major offensive campaigns ended May 1, 2003. Since that time,troops have remained in Iraq serving in a wide variety of roles. Thepurpose of this paper is to present the experience at Walter Reed ArmyMedical Center (WRAMC) and National Naval Medical Center-Bethesda(NNMC) with patients who were medically evacuated from the theaterfor neurosurgical issues over the first year of combat.
METHODS: A retrospective chart review was performed on allmedical evacuations from OIF to WRAMC and NNMC from March20, 2003, through March 20, 2004. Patients who were medically evac-uated for neurosurgical evaluation or consultation were included.
RESULTS: There were 2594 patients evacuated to WRAMC/NNMC during this time period. Two thousand twenty-three (78%)were from OIF. Neurosurgery was either the primary or consultingservice for 281 (14%) of these patients. There were 102 cranial injuries(36%) and 150 (53%) spine or spinal cord disorders. The remainingevacuations were composed of a variety of disorders such as periph-eral nerve injuries and newly discovered tumors. One hundred four(37%) were battle injuries and 177 (63%) were nonbattle injuries ordisease. Of the cranial cases, 54 (53%) were penetrating head injuries,and 48 (47%) were closed-head injuries. Of the spine cases, 134 (89%)were low back pain, neck pain, or radiculopathies. Sixteen of thesecases (11%) were penetrating spine/spinal cord injuries or fractures.
CONCLUSION: OIF and continued operations in Iraq represent thelongest continuous large-scale active military conflict since Vietnam.By reviewing the medical evacuations from the theater, it is possible todetermine the role for a military neurosurgeon in times of war. It alsoprovides evidence for further research into body armor and helmetsthat eliminate vulnerable areas, such as the neck and face, and arepractical for use in austere environments.
725USNS Comfort: Lessons Learned from OperationIraqi FreedomMarilyn L.G. Gates, M.D., Paul Hartzfeld, M.D.
INTRODUCTION: The USNS Comfort, a 1000-bed floating hospial, wasdeployed to the Persian Gulf in support of coalition forces participating inOperation Iraqi Freedom. The ship is equipped with computed tomography,angiography, 11 operating rooms, and an 80-bed intensive care unit. Surgicalstaff included most major specialities. The ship was positioned several kilo-meters off the coasts of Iran, Iraq, and Kuwait. Patients were transported tothe ship by helicopter. Despite a well-trained staff and full tertiary capabil-ities, issues related to caring for battlefield wounded on foreign soil could notbe completely prepared for. We present our experience with the neurosur-gical population during this conflict.
METHODS: Seven hundred fifty-six operations were performed in52 days. Of these, 55% were completed on Iraqi citizens. Ten craniot-omies were performed on 7 patients. Six of these patients were Iraqicitizens. One had had two prior craniotomies at other facilities, and allwere days to weeks from injury. Multiple transports and Genevaconvention protocols meant that little or no medical information wasavailable at the time of admission.
ABSTRACTS OF OPEN PAPERS
460 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

RESULTS: All Iraqi patients with penetrating brain injury wereinfected with Acinetobacter at the time of admission to the USNSComfort. All were subsequently treated with a combination of imi-penem and rifampin. Concurrent treatment with dilantin was diffi-cult. Initially, all patients treated with dilantin required daily ortwice-daily boluses to keep levels at or above 3. Liver function testlevels increased precipitously in all treated patients who were receiv-ing antiepileptic drugs (AEDs) and antibiotics. AEDs were changed tophenobarbital without further difficulty.
CONCLUSION: The latest equipment and fully staffed hospitalcannot predict the particular issues that arise from changing condi-tions while fighting a war on foreign soil and caring for thosewounded. Our experience provides some insight into specific prepa-rations that can positively affect care in future conflicts.
726Vaccine Prevention of Post-head Injury MeningitisStanley A. Shatsky, M.D., William C. Bergman, M.D.,Joshua B. Shatsky, B.S.
INTRODUCTION: There is no definitive evidence that antibioticprophylaxis prevents meningitis after basilar cranial fracture or trau-matic cerebrospinal fluid leakage. For the past two decades, we haveused polyvalent vaccines to immunize patients against Streptococcuspneumoniae and Haemophilus influenzae type B as an alternate prophy-lactic measure. We have recorded no episodes, either early or late, ofeither meningitis in 1247 patients so treated.
METHODS: Between January 1985 and December 2003, approxi-mately 11,000 patients were seen as emergencies at the Santa ClaraValley Medical Center with the primary diagnosis of either open- orclosed-head injury. Of these, 5334 patients were seen with head injuryas their primary diagnosis; 1247 patients were diagnosed as having afracture of the cranial base with either computed tomographic evi-dence of basilar fracture, cerebrospinal fluid rhinorrhea, otorrhea,pneumocephalus, Battle’s sign, otorrhagia, or hemotympanum; 103patients had cerebrospinal fluid rhinorrhea or otorrhea that persistedfor 4 days or more. Polyvalent pneumococcal and polyvalent H.influenzae vaccines were administered either in the emergency room orrapidly after admission.
RESULTS: No patient vaccinated at SCVMC for traumatic basilarcranial fracture during the treatment period developed either pneu-mococcal or H. influenzae meningitis. Three patients developed othermeningitides: one Escherichia coli at 6 weeks, one Staphylococcus aureus,and the third, H. parainfluenzae, delayed, at 37 months. Each recoveredwith treatment. No allergic or significant reactions to the vaccinesoccurred.
CONCLUSION: Vaccination seems to be a logical and safe methodof prophylaxis against pneumococcal and H. influenzae meningitis inthe post-head injury patient. It is not costly and does not facilitate thedevelopment of resistant strains or seem to have other adverse clinicaleffects.
727Secondary Ischemia Results in Ion Dysfunctionand Elevated Intracranial Pressure after TraumaticBrain InjuryMichael F. Stiefel, M.D., Ph.D., Anthony Marmarou, Ph.D.
INTRODUCTION: It is well established that posttraumatic second-ary ischemia contributes to poor patient outcome. Ion dysfunction
leading to cytotoxic edema is a primary driving force for the formationof ischemic brain edema and is a principal component of traumaticbrain swelling. Because cell swelling is the result of net ion and watermovement, it is crucial to have a thorough understanding of thesetransients. The purpose of this study was to characterize the effects ofsecondary ischemia after traumatic brain injury (TBI) on the ability torestore ion homeostasis.
METHODS: Twenty-four Sprague-Dawley rats underwent carotidartery occlusion for 15 minutes (CAO15; n " 6), 60 minutes (CAO60;n " 6), TBI (n " 6), and TBI # CAO15 (n " 6). The impact-accelerationmodel of closed-head injury was used to induce TBI. Custom-fabricated ion-selective electrodes were used to monitor extracellularpotassium ([K#]e) and sodium ([Na#]e).
RESULTS: Ischemia resulted in a rapid accumulation of [K#]e(CAO15 " 41.94 % 13.65 mmol/L, CAO60 " 66.33 % 6.63 mmol/L)with a concomitant decrease in [Na#]e (CAO15 " 64 % 18 mmol/L,CAO60 " 72 % 11 mmol/L). TBI resulted in a less severe althoughidentical trend in ion dysfunction. Despite attenuated ion concentra-tions, clearance rates (t1⁄2) were equal to CAO60 (CAO60-t1⁄2: [K#]e "3.75 % 0.50 minutes, [Na#]e " 4.25 % 2.75 minutes; TBI-t1⁄2: [K#]e "5.00 % 2.64 minutes, [Na#]e " 4.20 % 1.64 minutes). Secondary isch-emia resulted in prolonged and sustained ion dysfunction with aconcomitant elevation in intracranial pressure.
CONCLUSION: Our results indicate that ischemia and TBI aresublethal in isolation. However, when TBI is associated with second-ary ischemia, ion dysfunction is severe and sustained with associatedelevated intracranial pressure.
728Continuous Propofol Infusion in the Treatment ofPediatric Traumatic Brain Injury: Is It Safe?William F. Young, M.D., George Martin, B.A.,Mary Aaland, M.D.
INTRODUCTION: Previous reports have suggested that propofolis a safe and effective means of sedation for the control of intracranialpressure (ICP) in adults with traumatic brain injury (TBI). Moreover,one prospective randomized trial suggested that the use of propofolmay be superior to standard sedatives (e.g., morphine) in adult headinjury. However, controversy exists regarding the use of propofol inpediatric TBI. High-dose propofol infusion in some pediatric patientshas been shown to cause rhabdomyolysis, severe metabolic acidosis,and myocardial infarction. In this report, we review our own experi-ence in using this drug for pediatric TBI.
METHODS: A retrospective chart review was performed. Institu-tional review board approval was obtained for the review. From aprospectively maintained computerized database, we identified pa-tients under the age of 18 years who sustained TBI and had anadmission Glasgow Coma Scale (GCS) score of 13 or less. The years1997 to 2003 were reviewed from a single institution.
RESULTS: One hundred twelve patients meeting the study criteriawere identified. All patients underwent placement of an ICP monitor.Propofol was used when standard measures were unsucessful incontrolling ICP and at the discretion of the treating physician. Themean GCS score in those patients not receiving propofol was 5 (n "80).The mean GCS score of those patients receiving propofol was 5.7(n " 32). The mortality rate for those patients not receiving propofolwas 22% (n " 18). The mortality rate for those patients receivingpropofol was 18% (n " 6). This difference was not statistically signif-icant. None of the deaths in the propofol group were thought to be
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 461

caused by propofol infusion syndrome. Mean duration of propofolinfusion was 6 days (range, 1–15 d).
CONCLUSION: We were not able to identify any adverse conse-quences resulting from the use of propofol in our study population.However, there are obvious limitations to our study (e.g., retrospec-tive review). Even though we were not able to identify any compli-cations associated with propofol, we will continue to monitor its use.
729Experimental Ultrasound Imaging of CerebralPerfusion at High ResolutionWilliam E. Butler, M.D.
INTRODUCTION: Traumatic brain injury accounts for one-third ofthe total annual American death toll. The task of reducing the second-ary brain injury sustained by such patients would be advanced if amethod existed to image cerebral perfusion at the bedside throughoutthe day. Epidural ultrasound is demonstrated here to be capable ofimaging the perfusion of cerebral tissue at high resolution.
METHODS: An in vitro technique was developed in a phantomwith a flowing medium to obtain a linear signal calibration of theultrasound contrast agent perflutren. A 9-MHz signal was usedthroughout. In five piglets, the dura was exposed under generalanesthesia, and an ultrasound probe was rigidly fixed in relation tothe dura. An intravenous bolus of perflutren was administered as thebrain was imaged. Tracer kinetic methods were used to calculatecerebral blood volume and flow images. In two piglets, the imageswere compared with those obtained from 3-T magnetic resonanceimaging (MRI).
RESULTS: An in vitro linear calibration of the relationship betweenperflutren concentration and ultrasound signal was demonstrated invitro. In piglets, ultrasound perfusion demonstrated a capacity forhigh-resolution imaging of cerebral blood flow and volume comparedwith 3-T MRI. It afforded fine distinction between the perfusioncharacteristics of gray and white matter.
CONCLUSION: Contrast-enhanced epidural ultrasound can imagecerebral perfusion in an experimental setting with resolution at leastcomparable to 3-T MRI. Experiments are under way to evaluate itssensitivity to perfusion changes associated with experimental modelsof acute brain injury and ischemia.
730The Use of Spine Fusion in the United StatesJohn A. Cowan, M.D., Reid Wainess, B.A.,Justin B. Dimick, M.D., Frank LaMarca, M.D.
INTRODUCTION: Surgical management of spine disease is animportant component of neurosurgical practice. The pattern of use incontemporary practice of spine fusion surgery at a national level isunknown.
METHODS: Clinical data were obtained from the Nationwide In-patient Sample (NIS, 1993–2001). All patients with procedure codesindicating cervical (CF), thoracolumbar (TLF), or lumbar (LF) fusionswere identified (n " 215,471). Overall use rates and those for eachprocedure were calculated. Patient demographics, immediate out-comes, and hospital characteristics and charges were analyzed.
RESULTS: A total of 103,337 CFs, 20,700 TLFs, and 91,434 LFs wereperformed. Overall use increased by 315% (145 to 604 cases/100,000,P ! 0.001). By patient age, use increased 12.5% for patients !20 years,
214% for 20–40 years, 505% for 41–60 years, and 360% for $60 years.Patients who underwent TLFs were younger than those with CFs orLFs (30 versus 49 and 50 yr, P ! 0.001). Overall mortality was less than1% for all procedures. Length of stay was greater for TLFs comparedwith CFs or LFs (7 days versus 2 days and 4 days, P ! 0.001) anddecreased over time. Inflation-adjusted hospital charges increased forall procedures. TLF resulted in the highest median hospital charges(2001 US dollars) compared with CF and LF ($46,500 versus $16,000and $29,300, P ! 0.001). The rate of TLFs performed at teachinghospitals increased significantly over time (53% to 79%, P ! 0.001). ForCFs and LFs, the percentage performed at teaching hospitals was 50%and 53%, respectively. Teaching hospitals had a larger spine fusioncase load than nonteaching hospitals (255 versus 157 cases annually,P ! 0.001).
CONCLUSION: Spine fusion has undergone a substantial increasein use in contemporary practice. Usage for middle-aged and olderpatient populations demonstrated the greatest increase. Analysis ofimmediate outcomes revealed low mortality rates and decreasinglength of stay. The cost of spine fusion, however, is increasing. Teach-ing hospitals continue to perform the majority of spine fusions.
731Surgeon Subspecialization and Patient Outcomein Aneurysm and Supratentorial Tumor Surgery:A Population-based StudyFred G. Barker II, M.D., William T. Curry, M.D.,Sepideh Amin-Hanjani, M.D., William E. Butler, M.D.,Christopher S. Ogilvy, M.D., Bob S. Carter, M.D., Ph.D.
INTRODUCTION: Patient outcome has been correlated with sur-geon subspecialization for pediatric neurosurgery and in general sur-gery. We correlated outcome after aneurysm or supratentorial tumorsurgery with surgeon subspecialization using population-based meth-ods.
METHODS: This was a cohort study using the Nationwide Inpa-tient Sample (Healthcare Cost and Utilization Project, Agency forHealthcare Research and Quality, Rockville, MD), 1988–2001. Special-ization was defined using the proportion of a surgeon’s admissionsthat represented either aneurysm clipping or biopsy/resection of pri-mary brain tumors, meningiomas, or metastases.
RESULTS: A total of 12,876 aneurysm admissions and 35,345 tumoradmissions were studied. For the “average” (median) United Statesaneurysm patient during this period, aneurysm clipping composed4.5% of the surgeon’s practice, and for the average tumor patient,tumor surgery composed 7.7% of the surgeon’s practice. Increasingsurgeon specialization correlated with better outcome for both condi-tions. With least-specialized-quartile aneurysm surgeons (practice!2.4% aneurysms), 10.8% of patients died and 50% were dischargedhome. With most-specialized-quartile surgeons (practice $10.5% an-eurysms), 5.9% of patients died and 66.6% were discharged home.With least-specialized-quartile tumor surgeons (practice $4.7% tu-mors), 3.3% of patients died and 67% were discharged directly home.With most-specialized-quartile surgeons (practice $12.5% tumors),1.7% of patients died and 75% were discharged directly home. Aftermultivariate adjustment for age, sex, race, admission type, primaryinsurance, diagnosis (ruptured/unruptured or tumor type), biopsy/resection (for tumors), and year of surgery, increasing specializationpredicted lower mortality and more likely discharge directly home(P ! 0.001, both end points, both diseases). Patient factors significantlypredicting a more-specialized surgeon were younger age, nonblack
ABSTRACTS OF OPEN PAPERS
462 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

race, routine admission, private insurance, diagnosis (unrupturedaneurysm or primary brain tumor), higher median income in patient’sZIP code, and later treatment year (P ! 0.005 for all except race, P !0.01).
CONCLUSION: Surgeon subspecialization in aneurysm and tumorsurgery predicted better patient outcome after the respective opera-tions in this cohort. Individual patients’ racial and socioeconomiccharacteristics were correlated with their surgeon’s degree of subspe-cialization. Both aneurysm and tumor surgery are being performed byprogressively more-specialized surgeons.
732Resident Duty-Hours Reform: The Results of aNational Survey of the Program Directors andResidents in Neurosurgery Training ProgramsAaron A. Cohen-Gadol, M.D., David G. Piepgras, M.D.,Richard D. Fessler, M.D.
INTRODUCTION: The new Accreditation Council for GraduateMedical Education (ACGME) requirements regarding resident workhours have been implemented since July 2003. Neurological surgerytraining programs have been especially affected because of the limitednumber of residency positions and the residents’ long duty hours. Theperceptions of program directors and residents may provide impor-tant insight into the evolution of new guidelines for improvement ofresident training.
METHODS: We conducted a nationwide survey of 93 programdirectors and 617 residents to characterize their perception regardingthe changes in their training programs related to compliance with theACGME requirements. The survey was conducted from July throughSeptember 2003 using electronic mail.
RESULTS: The response rates were 45% and 23% among the pro-gram directors and residents, respectively. Although 92% of programshad implemented the ACGME work-hours requirements before orsince July 2003, 8% had not yet implemented these guidelines. Sixty-eight percent of program directors indicated employment of ancillaryhealth care professionals to fulfill the ACGME duty-hours reform;84% believed this practice has not limited the residents’ clinical expe-rience. Eleven percent (18/164) of respondents who provided levelone trauma coverage were unable to maintain compliance with theACGME guidelines; 93% of all respondents believed the work-hourreform has had a negative impact on the continuity of patient care;55% of the residents and only 33% of program directors believed thatthe ACGME requirements will result in improved American Board ofNeurological Surgery written test scores. Overall, 61% of the residentsand 79% of the program directors noted that the ACGME guidelineshave had a negative effect on their training programs.
CONCLUSION: More sophisticated solutions may be needed toaddress house-staff fatigue. Strategies to enhance the educationalcontent of the residents’ work hours and preserve continuity of pa-tient care are necessary.
733Health Care Financing 101: An Internet-basedLearning Platform for Nontraditional ResidentInstruction on the Economics of HealthcareJohn Tuttle, M.D., William Hamilton, M.B.A.
INTRODUCTION: There is a void in the instruction in the socio-economic factors of medicine in traditional neurosurgery resident
training programs. The result is that neurosurgeons finish their train-ing without a knowledge base in the nonclinical aspects of medicineand do not have a core for sound business decision making.
METHODS: A curriculum was created for the Medical College ofGeorgia neurosurgery residents that provided core competencies innonclinical healthcare management and a baseline of knowledge forbusiness decision making. A traditional classroom lecture format wasnot tenable for the following reasons: 1) clinical educational respon-sibilities; 2) Accreditation Council for Graduate Medical Educationwork-hour limitations; and 3) fragmented lecture attendance. Aninternet-based platform was created using a software program thatallowed for the review of a PowerPoint presentation coupled with asimple, synchronized video/audio feed that provided the studentwith a personalized lecture over the internet. A simple pretest andposttest was created that measured the effectiveness of the course interms of objective attainment. The convenience created by the internetbasis allowed the resident to complete the curriculum according tohis/her schedule and as time permitted.
RESULTS: 1) The internet based platform resulted in 100% partic-ipation in all aspects of the curriculum. 2) The pre/posttesting meth-odology showed that this training resulted in the residents meetingthe learning objectives of the course.
CONCLUSION: 1) There is a void in newly trained neurosurgeons’knowledge base in the nonclinical aspects of healthcare. This leavesthem without business decision making skills on completion of theirtraining. 2) Traditional lecture/classroom settings are not effective forthis type of training. However, an internet-based platform providesthe flexibility that allows for complete curriculum participation. 3)Neurosurgery training programs should institute a formalized curric-ulum in the socioeconomic issues in neurosurgery and healthcare ingeneral.
734Acoustic Neuroma Surgical Cost and Outcome byHospital VolumeMarc S. Schwartz, M.D., William H. Slattery, M.D.,Mark Oppenheimer, M.S., Laurel M. Fisher, Ph.D.
INTRODUCTION: To determine the relationship between hospitalvolume and surgical outcome in the treatment of acoustic neuromas,we analyzed data from the California Hospital Discharge Database.This database tracks all patients discharged from California hospitalsand includes relevent International Classification of Diseases-9 andDiagnostic Related Group coding information.
METHODS: Information for 1213 acoustic neuroma resections performedbetween 1996 and 1998 was divided into groups according to annual hos-pital volume. The resulting four hospital volume groups were compared viathe following measures: discharge status (routine [home without services]versus not routine), postoperative procedures (signifying likely complica-tions), total cost of hospitalization, and average cost per day. Odds ratioswere used to compare hospital volume groups for routine surgical outcome,defined as discharge home without additional procedures.
RESULTS: The frequency of routine surgical outcome increased ashospital acoustic neuroma surgical volume increased, ranging from68.1% among patients in the lowest-volume group to 96.9% in the high-est. Patients in the highest-hospital-volume group ($50 operations/yr)were 14.8 times more likely to have a routine surgical outcome than thosein the lowest group (1–5 operations/yr). Patients in the second-highest-hospital-volume group (15–50 operations/yr) were 4.6 times more likelyto have a routine surgical outcome than those in the lowest group. The
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 463
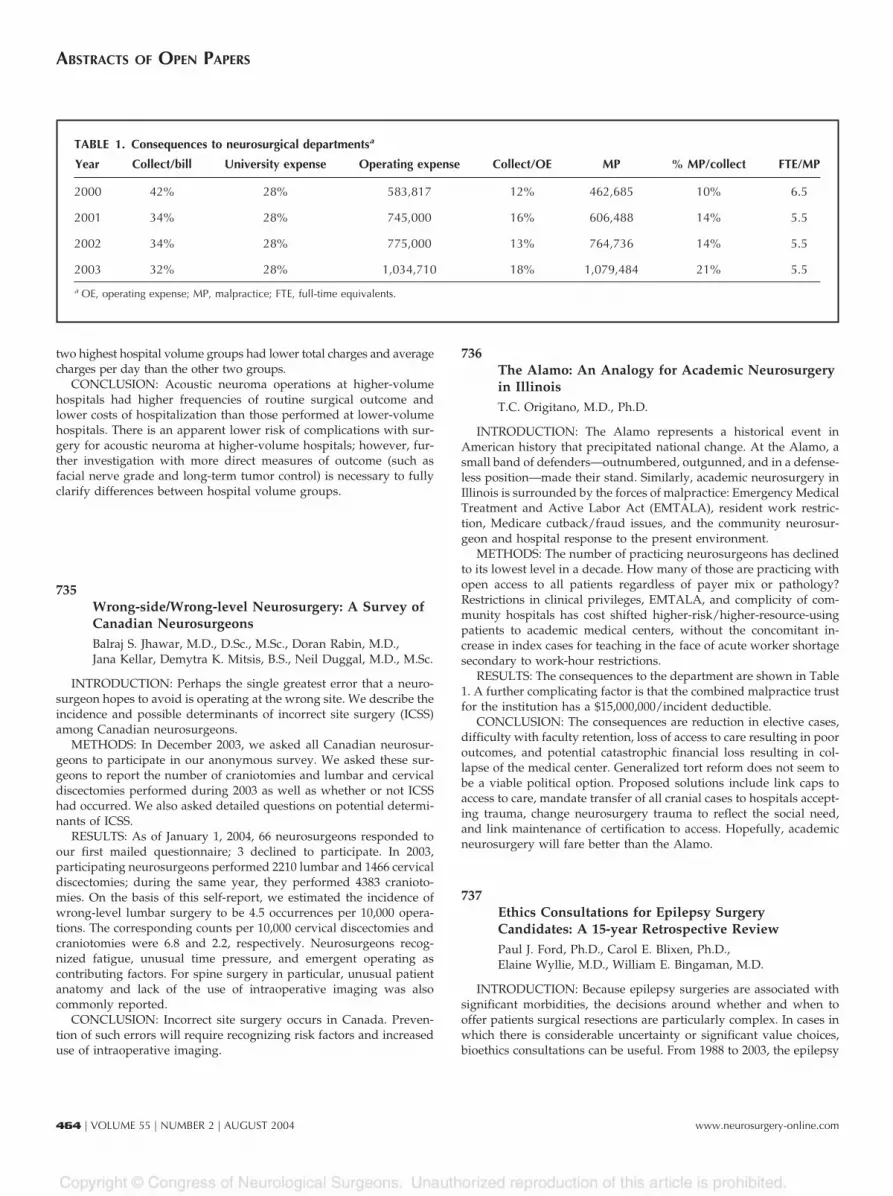
two highest hospital volume groups had lower total charges and averagecharges per day than the other two groups.
CONCLUSION: Acoustic neuroma operations at higher-volumehospitals had higher frequencies of routine surgical outcome andlower costs of hospitalization than those performed at lower-volumehospitals. There is an apparent lower risk of complications with sur-gery for acoustic neuroma at higher-volume hospitals; however, fur-ther investigation with more direct measures of outcome (such asfacial nerve grade and long-term tumor control) is necessary to fullyclarify differences between hospital volume groups.
735Wrong-side/Wrong-level Neurosurgery: A Survey ofCanadian NeurosurgeonsBalraj S. Jhawar, M.D., D.Sc., M.Sc., Doran Rabin, M.D.,Jana Kellar, Demytra K. Mitsis, B.S., Neil Duggal, M.D., M.Sc.
INTRODUCTION: Perhaps the single greatest error that a neuro-surgeon hopes to avoid is operating at the wrong site. We describe theincidence and possible determinants of incorrect site surgery (ICSS)among Canadian neurosurgeons.
METHODS: In December 2003, we asked all Canadian neurosur-geons to participate in our anonymous survey. We asked these sur-geons to report the number of craniotomies and lumbar and cervicaldiscectomies performed during 2003 as well as whether or not ICSShad occurred. We also asked detailed questions on potential determi-nants of ICSS.
RESULTS: As of January 1, 2004, 66 neurosurgeons responded toour first mailed questionnaire; 3 declined to participate. In 2003,participating neurosurgeons performed 2210 lumbar and 1466 cervicaldiscectomies; during the same year, they performed 4383 cranioto-mies. On the basis of this self-report, we estimated the incidence ofwrong-level lumbar surgery to be 4.5 occurrences per 10,000 opera-tions. The corresponding counts per 10,000 cervical discectomies andcraniotomies were 6.8 and 2.2, respectively. Neurosurgeons recog-nized fatigue, unusual time pressure, and emergent operating ascontributing factors. For spine surgery in particular, unusual patientanatomy and lack of the use of intraoperative imaging was alsocommonly reported.
CONCLUSION: Incorrect site surgery occurs in Canada. Preven-tion of such errors will require recognizing risk factors and increaseduse of intraoperative imaging.
736The Alamo: An Analogy for Academic Neurosurgeryin IllinoisT.C. Origitano, M.D., Ph.D.
INTRODUCTION: The Alamo represents a historical event inAmerican history that precipitated national change. At the Alamo, asmall band of defenders—outnumbered, outgunned, and in a defense-less position—made their stand. Similarly, academic neurosurgery inIllinois is surrounded by the forces of malpractice: Emergency MedicalTreatment and Active Labor Act (EMTALA), resident work restric-tion, Medicare cutback/fraud issues, and the community neurosur-geon and hospital response to the present environment.
METHODS: The number of practicing neurosurgeons has declinedto its lowest level in a decade. How many of those are practicing withopen access to all patients regardless of payer mix or pathology?Restrictions in clinical privileges, EMTALA, and complicity of com-munity hospitals has cost shifted higher-risk/higher-resource-usingpatients to academic medical centers, without the concomitant in-crease in index cases for teaching in the face of acute worker shortagesecondary to work-hour restrictions.
RESULTS: The consequences to the department are shown in Table1. A further complicating factor is that the combined malpractice trustfor the institution has a $15,000,000/incident deductible.
CONCLUSION: The consequences are reduction in elective cases,difficulty with faculty retention, loss of access to care resulting in pooroutcomes, and potential catastrophic financial loss resulting in col-lapse of the medical center. Generalized tort reform does not seem tobe a viable political option. Proposed solutions include link caps toaccess to care, mandate transfer of all cranial cases to hospitals accept-ing trauma, change neurosurgery trauma to reflect the social need,and link maintenance of certification to access. Hopefully, academicneurosurgery will fare better than the Alamo.
737Ethics Consultations for Epilepsy SurgeryCandidates: A 15-year Retrospective ReviewPaul J. Ford, Ph.D., Carol E. Blixen, Ph.D.,Elaine Wyllie, M.D., William E. Bingaman, M.D.
INTRODUCTION: Because epilepsy surgeries are associated withsignificant morbidities, the decisions around whether and when tooffer patients surgical resections are particularly complex. In cases inwhich there is considerable uncertainty or significant value choices,bioethics consultations can be useful. From 1988 to 2003, the epilepsy
TABLE 1. Consequences to neurosurgical departmentsa
Year Collect/bill University expense Operating expense Collect/OE MP % MP/collect FTE/MP
2000 42% 28% 583,817 12% 462,685 10% 6.5
2001 34% 28% 745,000 16% 606,488 14% 5.5
2002 34% 28% 775,000 13% 764,736 14% 5.5
2003 32% 28% 1,034,710 18% 1,079,484 21% 5.5
a OE, operating expense; MP, malpractice; FTE, full-time equivalents.
ABSTRACTS OF OPEN PAPERS
464 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

surgery program at The Cleveland Clinic Foundation referred 10 to15% of epilepsy surgery candidates to be evaluated for ethical contra-indications to surgery (e.g., lack of informed consent). The objective ofthis study was to describe the characteristics of patients being referredand the frequency of ethics recommendation types.
METHODS: A retrospective review of epilepsy surgery ethics con-sultations between January 1, 1988, and July 1, 2003, was performed(n " 174). Data were extracted and entered into an Access database.Analysis was performed with JMP statistical software.
RESULTS: The mean age of the sample was 19.5 years (standarddeviation, 13.8 yr; range, 0.1 to 61.9 yr), with 110 (63%) patients under21 years of age. Of the total sample, 92 (52%) were men. Five (3%) ofthe consultations recommended against proceeding with surgery; 16(9%) raised significant ethical issues needing resolution; 127 (73%)found either no ethical contraindications or minor education needed;and 26 (15%) did not record a recommendation. One hundred forty-five patients (83%) went forward with surgery (temporal lobe resec-tion 66 [45%], hemispherectomy 38 [26%] corpus callosotomy 18[12%], frontal lobe resection 13 [9%], and lesionectomy/other 12 [8%]).
CONCLUSION: Given the irreversible nature of these surgeriesand that parents are often central in consenting for young patients, theproportion of patients under 21 years of age in our sample is notsurprising. Although most consultations found few or no ethicalcontraindications, in some instances, the ethics consultant raised sig-nificant ethical issues regarding a patient’s candidacy for surgery. Thisstudy is significant because it is the first to analyze the use of an ethicsconsultant in epilepsy surgery evaluation.
738Socioeconomic Factors in Neurosurgical TreatmentModalities: The Difference between Older andNewer TreatmentsRavish V. Patwardhan, M.D., Anil Nanda, M.D.
INTRODUCTION: Discrepancies in allocation of advanced neuro-surgical care are not well characterized. The purpose of the presentstudy was to determine socioeconomic disparities in use betweenolder and newer neurosurgical techniques for treatment of commonlyencountered neurosurgical problems.
METHODS: The National Inpatient Sample (NIS) for the year 2000was reviewed. A total of 7.4 million inpatient entries were sorted forthe two commonly encountered diagnoses of intracerebral hemor-rhage and intracranial neoplasm and two more recently introducedprocedures of stereotactic radiosurgery and deep brain stimulation. Inconsideration of each of these factors, socioeconomic differences weredetermined.
RESULTS: In all, 29,062 inpatient admissions were analyzed usingthe criteria noted above. Significant disparity in use of newer technol-ogies (such as deep brain stimulation and stereotactic radiosurgery)was noted in lower socioeconomic classes. Lower socioeconomic classand African-American patients each had a disproportionately loweramount of each newer treatment modality with respect to databaserepresentation (one-sample test for proportion, P ! 0.0001). Disparityin socioeconomic classes was less noticeable in overall brain tumortreatment and was not present in consideration of intracerebral hem-orrhage.
CONCLUSION: Newer neurosurgical treatment modalities, de-spite having a proven benefit in the treatment of neurosurgical prob-lems, remain underused for lower socioeconomic classes; this differ-ence is no longer apparent for older, more established treatments.
739The Intractable Epilepsy Problem in DevelopingCountries: Is There a Way Out?Sujoy K. Sanyal, M.B.B.S., M.Ch.,P. Chandra, M.B.B.S., M.Ch.,Manjari Tripathi, M.B.B.S., M.Ch.
INTRODUCTION: Epidemiological studies estimate one millionpeople in India with intractable epilepsy. However, like all developingcountries, epilepsy surgery is underutilized in India, only 650 caseshaving been operated on at two major centers, including ours. Thenonavailability of intraoperative electrocorticography (ECoG) andsingle-photon emission computed tomography (SPECT)/video EEG(VEEG) has restricted this program to big centers.
METHODS: We wished to see how many of our surgical casescould have been operated on without VEEG, SPECT, and ECoG atslightly smaller centers with only EEG, magnentic resonance imaging(MRI), and facilities for a standard anteromedial temporal lobectomy(AMTL).
RESULTS: One hundred fifty-five cases of intractable epilepsy op-erated on at our center included 7 corpus callosotomies, 3 hemisphe-rotomies, and 46 lesionectomies under ECoG guidance. Ninety-ninepatients underwent standard AMTL without ECoG guidance for me-sial temporal sclerosis (MTS)/lesional temporal lobe epilepsy. Amongthese 99, MRI identified the side of MTS/temporal focus correctly in90. Three had features of bilateral MTS, 2 had bilateral gliotic foci, and4 had normal MRIs, all these 9 evidently requiring detailed evaluation.Among the remaining 90, VEEG revealed discordant foci (to theMRI-identified focus) in 13 and was noncontributory in 8. Ultimately,even the 13 patients with discordant VEEG underwent AMTL on theMRI-identified side, and all 13 had good seizure outcome. SPECT wasnoncontributory in 9 of these 90 patients and revealed discordant fociin 4. All the 4 with discordant SPECT localization ultimately under-went AMTL on the MRI-identified side with good outcome. SPECT/VEEG was therefore useful in only 9 patients with equivocal MRIfindings. All 90 patients with clear-cut MRI localization had nothingadded by VEEG/SPECT. Therefore, 90 of our 155 patients (58%) couldhave undergone surgery at a center equipped with only EEG, MRI,and AMTL facilities.
CONCLUSION: The need of the hour for developing countries is tocreate awareness regarding epilepsy surgery and creation of a two-tiered epilepsy surgery program. The first tier, equipped with EEG,MRI, and trained neurologists, neurosurgeons, and neuroradiologistscan undertake AMTL in patients with clear-cut MRI localization,which is a large proportion of the epilepsy surgery burden. Morecomplicated cases can be referred to bigger centers. This strategy islikely to popularize epilepsy surgery but would definitely requirestrict surveillance.
740Selective Ablation of Nociceptive Neurons forElimination of Neuropathic PainGabriel C. Tender, M.D., Stuart Walbridge, B.S.,Zoltan Olah, Ph.D., Laszlo Karai, M.D.,Michael Iadarola, Ph.D., Edward H. Oldfield, M.D.,Russell R. Lonser, M.D.
INTRODUCTION: Neuropathic pain is mediated by nociceptiveneurons that selectively express the vanilloid receptor 1 (VR1). Res-iniferatoxin, an excitotoxic VR1 agonist, destroys VR1-positive neu-
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 465

rons. To determine whether resiniferatoxin can selectively ablate VR1-positive neurons and eliminate neuropathic pain without affectingtactile sensation and motor function, we infused it unilaterally intoprimate trigeminal ganglia.
METHODS: We perfused resiniferatoxin (experimental " 3) orvehicle (control " 1) into the R trigeminal ganglia of Rhesus primatesand tested tactile and hyperalgesic sensation in trigeminal-innervatedterritories (corneal application of saline and capsaicin, respectively) at1, 4, and 7 weeks postoperatively. Number of blinks, eye wipes, andduration of squinting were recorded after application. Neurogenicinflammation, mediated by VR1-positive neurons, was tested by facialapplication of capsaicin cream. Immunohistochemical analyses wereperformed after euthanization.
RESULTS: Consistent with elimination of hyperalgesia on the sideof resiniferatoxin-treated ganglia, there was a dramatic reduction inthe number of blinks (mean % standard deviation; 25.7 % 4.4 versus106 % 20.8 and 112.8 % 19.7), eye wipes (1.4 % 0.8 versus 19.3 % 10.0and 16.7 % 9.0), and duration of squinting (1.4 % 1.1 seconds versus14.0 % 3.1 and 14.8 % 3.4) in response to corneal application ofcapsaicin compared with the vehicle and untreated sides, respectively(P ! 0.001). Tactile sensation (mean blinks after saline application,18.8 % 2.3 versus 18.0 % 2.6 and 18.4 % 3.3, respectively; P $ 0.05) andmotor function (mastication) remained intact. Neurogenic inflamma-tion was blocked on the resiniferatoxin-treated side. Animals showedno adverse clinical effects. Immunohistochemical analysis revealedselective ablation (mean decrease, 79.3 % 2.8%; P ! 0.001) of VR1-positive neurons in the resiniferatoxin-treated ganglia.
CONCLUSION: VR1-positive nociceptive neurons can be safelyand selectively ablated by intraganglionic resiniferatoxin infusion,eliminating hyperalgesia and neurogenic inflammation while main-taining intact tactile sensation and motor function. Intraganglionicresiniferatoxin infusion may provide a new treatment approach forneuropathic pain.
741INTERPRET Study of Proton Magnetic ResonanceSpectroscopy in Brain TumorsB. Anthony Bell, M.D., M.B.B.S.
INTRODUCTION: Proton magnetic resonance spectroscopy (MRS)allows a noninvasive study of regional brain biochemistry at the timeof a magnetic resonance imaging (MRI) scan. The INTERPRET studyrecruited patients with histologically verified intracranial tumors whohad undergone preoperative MRS from neurosurgical units in Lon-don, Barcelona, Grenoble, and Nijmegen. The results are presentedhere on behalf of all the INTERPRET study collaborators.
METHODS: This multicenter study recruited 621 patients betweenJanuary 2000 and December 2002. All clinical and radiological dataand the histological slides were reviewed by a panel of neurologists,neurosurgeons, neuroradiologists, and neuropathologists before in-clusion in the study. Pattern recognition algorithms were then devel-oped to allow automated analysis of the proton magnetic resonancespectra.
RESULTS: Using pattern recognition software, the average spectro-scopic pattern of meningiomas, grade 2 and 3 astrocytomas, glioblas-tomas, and metastases were defined, and both single-voxel and mul-tivoxel protoype analysis systems were developed. The prototypegraphical user interface systems allow spectra from new cases to beclassified with an accuracy that exceeds 90% and is similar to that
achieved by a stereotaxic biopsy and neuropathological examinationof the tissue.
CONCLUSION: Noninvasive outpatient diagnosis of intracranialtumors is now possible using proton MRS available on most clinicalMRI scanners. Automated pattern recognition software can achievesimilar diagnostic accuracy to stereotaxic biopsy.
742Reevaluation of Surgery for the Treatmentof Brain MetastasesSun Ha Paek, M.D., Paul B. Audu, M.D.,Michael R. Sperling, M.D., Joon Cho, M.D.,David W. Andrews, M.D.
INTRODUCTION: Reliable prospective randomized data from theRTOG 9508 trial are now available for radiosurgical treatment of oneto three metastases. We reviewed 208 surgical cases with comparisonto the radiosurgery arm of the RTOG 9508 trial to gain a betterunderstanding of which treatment might be more beneficial.
METHODS: We reviewed 208 surgical cases for brain metastases andincluded a comparison of RTOG 9508-eligible patients with the SRS boostarm in this multicenter trial. We assessed overall neurological and survivaloutcomes as well as recursive partioning prognostic (RPA) groups andfunctional grades of tumor location (eloquent versus noneloquent).
RESULTS: The median survival time (MST) of all patients fromsurgery was 8 months, and for RTOG 9508-eligible patients, 15months. There was no difference in the survival between single andmetastases (MST: 8 versus 9 months, respectively, P " 0.9364). Bymultivariate analysis, RPA criteria were significant. For all RTOG9508-eligible patients, the MST was 14 months, with no significantdifference between patients with single or multiple metastases (16versus 11 months, respectively, P " 0.1869). The MST of RPA Class Iand Class II patients was 21 months and 11 months, respectively,approaching significance at P " 0.0627, log rank. These survival datacompared favorably to the SRS boost arm of the RTOG 9508 trial.
CONCLUSION: For patients with single or multiple brain metas-tases, comparison to the RTOG 9508 radiosurgery trial suggestedgreater survival benefit for surgery compared with radiosurgery, par-ticularly for RPA Class I patients. For Class III single metastasispatients or for RPA Class II multiple metastasis patients, SRS boosttreatment may be preferable. An algorithm for treatment of brainmetastases is proposed.
743GliaSite Radiotherapy System for Treatmentof Recurrent Malignant Glioma:A Multi-Institutional AnalysisAbhay Sanan, M.D., Arash Gabayan, M.D.,Baldassarre Stea, M.D., Sylvan Green, M.D.,Kenneth Bastin, M.D., Stuart Burri, M.D.,Joseph Jenrette, M.D., Michael Papagikos, M.D.,Ashish Patel, M.D., Christopher Schultz, M.D.,Gordon Watson, M.D.
INTRODUCTION: The GliaSite Radiotherapy System (RTS) is anovel device consisting of an implantable balloon designed to deliverradiation to a brain tumor resection cavity. This study evaluates thecumulative experience of nine institutions in treating recurrent ma-lignant glioma with the RTS.
ABSTRACTS OF OPEN PAPERS
466 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

METHODS: Nine institutions provided data on 81 eligible patientswith recurrent high-grade glioma. All had previously received 50 to 78Gy of external beam radiation with or without chemotherapy as partof the initial management of their malignant glioma. On tumor recur-rence, the patients underwent maximal surgical debulking of themalignant lesion, during which time an inflatable balloon catheter(GliaSite RTS) was placed in the tumor bed and was later used todeliver low-dose-rate brachytherapy.
RESULTS: The median follow-up for all patients was 37 weeks(2–100 wk) from date of catheter placement. The 12 patients still alivehad a median follow-up of 62 weeks (32–96 wk). The median survivalmeasured from the date of GliaSite implantation was 38.1 weeks (95%CI, 32.7–42.7 wk). The median time to disease progression after cath-eter placement was 19.3 weeks (95% CI, 16.0–23.7 wk), and the esti-mated 1-year survival was 32.7%. Analysis of the influence of variousindividual prognostic factors on patient survival demonstrated thatonly Karnofsky Performance Scale (KPS) score predicted improvedsurvival (P " 0.01). On the basis of multivariate analysis (Coxproportional-hazards model), KPS $ 90 (RR, 0.65; P " 0.003), previousexposure to Gliadel wafers (RR, 0.71; P " 0.03), and age !50 years(RR, 0.78; P " 0.05) were shown to be favorable prognostic factors. TheGliasite RTS was well tolerated, and no adverse effects were seenwhen used concurrently with Gliadel wafers.
CONCLUSION: The use of GliaSite seems to indicate a modestsurvival advantage (median survival of 38.1 weeks) than either sur-gery alone, which has a median survival of 23 weeks after resection, orsurgery with the placement of Gliadel wafers, which has a mediansurvival of 31 weeks.
744Matrix-assisted Ionization Desorption MassSpectrometry Proteomic-based Diagnosis andPrognosis of GliomasRobert J. Weil, M.D., Sarah A. Schwartz, B.S.,Steven A. Toms, M.D., Mahlon D. Johnson, M.D.,Ph.D., Ken Niermann, Yu Shyr, Ph.D.,Bashour Shaktour, Ph.D., Reid Thompson, M.D.,Jeremy Roberts, Richard M. Caprioli, Ph.D.
INTRODUCTION: Research has focused on approaches to identifygenomic and proteomic analyses to improve the diagnosis and mon-itoring of disease. We used matrix-assisted ionization desorption massspectrometry (MALDI-MS) to characterize glioma subtypes and tostratify patient outcomes based on MS protein patterning.
METHODS: Snap-frozen tissue samples were sectioned andmounted onto gold-coated MALDI-MS plates. Consecutive sectionswere stained with hematoxylin and eosin and analyzed by a neuro-pathologist blinded to the original diagnosis, which served as the goldstandard. Spectra were obtained on a MALDI-TOF MS and analyzed.Patient information was collected, including age, sex, tumor type andWorld Health Organization (WHO) grade, treatment received, extentof tumor resection, time to recurrence, and survival.
RESULTS: One hundred forty-six tissue samples were analyzedfrom 134 patients (26 with normal temporal lobe [N], 37 with WHOgrade II tumors [T2], 27 grade III [T3], and 56 grade IV [T4] tumors)using MALDI-MS. Approximately 300 to 500 individual proteins sig-nals were identified in the m/z range of 2 to 50 kD. Bioinformaticcomparisons permitted reliable identification of tumor from normal(N/T2–4) and grades of tumor from normal (N/T2 and N/T4) with 99to 100% accuracy; similar classification (N/T3, T2/T3, T3/T4) com-
parisons were 92.5 to 98.5% accurate. Comparing all tumors withMALDI-MS identified a biomarker pattern (25 proteins) that identi-fied, from the universe of glioma patients, those who do well (meansurvival, 120 mo) from those who do not (mean, 18 mo); it alsoidentifies the few patients with T2 and T4 who do worse or better thanexpected, respectively. Finally, analysis of 56 similarly treated glio-blastoma multiforme patients demonstrated that nine differentiallyexpressed proteins identify long-term survivors (mean, 18 mo) fromshort-term survivors (mean, 9 mo), with a value of P ! 0.001. Tumor-and prognosis-specific proteins have been identified and confirmedusing MS/MS techniques.
CONCLUSION: MALDI-MS proteomic profiling reproduciblyidentifies glioma subtypes, correlates with pathological grading andoutcome, and predicts survival of subgroups of glioma patients.
745Contribution of Intraoperative CorticosubcorticalStimulations in Surgery of Low-grade Gliomas:A Comparative Study between Two Series withoutand with Functional MappingHugues Duffau, M.D., Ph.D., Manuel Lopes, Peggy Gatignol,Emmanuel Mandonnet, Ph.D., Luc Taillandier, M.D., Ph.D.,Marianne Leroy, Dominique Denvil, M.D.,Ahmad Bitar, M.D., Jean-Pierre Sichez, M.D.,Remy Van Effenterre, M.D., Laurent Capelle, M.D.
INTRODUCTION: Despite a growing use of intraoperative func-tional mapping in surgery of supratentorial hemispheric low-gradegliomas (LGGs), very few comparative studies of patients operated onwithout and with direct cortical and subcortical electrical stimulations(DES) in the same institution were reported in the literature. Here, wecompare the rate of LGG surgeries performed in eloquent areas, therate of postoperative sequelae, and the quality of resection during twoconsecutive periods in the same department: the first one without theuse of intraoperative electrophysiology, the second one with DES.
METHODS: From 1985 to 1996, 100 patients harboring a supraten-torial LGG underwent surgery with no functional mapping (S1). From1996 to 2003, 122 patients were operated on in the same departmentfor a supratentorial hemispheric LGG using intraoperative cortico-subcortical DES (S2).
RESULTS: Comparison between the two series showed that 35% ofLGG were operated on in eloquent areas (S1) versus 62% (S2) (P !0.0001), with 17% of severe permanent deficits (S1) versus 6.5% (S2) (P! 0.019). On control magnetic resonance imaging, 37% of resectionswere subtotal and 6% total (S1), versus respectively 50.8% and 25.4%(S2) (P ! 0.001).
CONCLUSION: Our results allow for the first time a quantification ofthe contribution of intraoperative cortico-subcortical DES during LGGresection. Indeed, the use of this method leads to 1) the extension ofindications of LGG surgeries within eloquent areas, 2) a decrease of therisk of sequelae, and 3) an increase of the quality of tumor resection.
746Surgical Management of Giant Glomus JugulareTumors without Rerouting of the Facial NerveLuis Borba, M.D., Samir Bark
INTRODUCTION: The surgical approach to glomus jugulare tu-mors is crucial to get a radical removal. The standard surgical tech-
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 467

nique is based in the neck exposure, temporal bone drilling, andanterior rerouting of the facial nerve. In this paper, the authors presenta surgical series of giant glomus jugulare tumors, which were re-moved with a new technique based on the removal of tumor from thejugular foramen without rerouting of the facial nerve.
METHODS: From March 1998 to February 2004, 24 patients with giantglomus tumors were operated on. The surgical techniques proposed werebased on the neck exposure with proximal control of the internal carotidartery (ICA), the external carotid artery and branches, the lower cranialnerves, and the internal jugular vein. An anterior mastoidecmy was per-formed exposing the jugular bulb, the sigmoid, which was ligated proxi-mally, the labyrinth, and keeping the posterior wall of the auditory canal, theexternal auditory canal was preferentially not opened, except in case ofanterior exposure of the tumors, which could be seen during the surgicalprocedure. The facial nerve was kept in its canal. Neither exposure of thefacial nerve in the canal or in the exit at the stylomastoid foramen wasattempted. The tumor was removed in piecemeal fashion with the help ofsuction and coagulation. The anterior border of the tumor was removedusing a dissection under the facial nerve. The dura of the posterior fossa wasopened and an intradural tumor removed. After removal, the dura wasclosed and the cavity occluded with fat.
RESULTS: Sixteen patients were female and 8 male, and totalremoval was obtained in 23. In one anterior exposure of the tumor, theencasing of the ICA was not removed. Six patients had a preoperativefacial nerve palsy and were exposed during the procedure. No newfacial nerve deficit was found. In 4, a graft was inserted, and in 2,decompression of the nerve was performed. The lower cranial nervefunctions were worse in 8 patients and unchanged in 16 patients.Cerebrospinal fluid leak was found in 2 patients. One patient died 45days after the procedure secondary to aspirative pnemonia.
CONCLUSION: The surgical removal of giant glomus jugulare tu-mors without rerouting of the facial nerve is possible independent of thesize, avoiding a severe morbidity related to the surgical approach.
747Transduced Bone Marrow-derived Cells Target BrainTumors and Express TransgeneFaith H. Barnett, M.D., Ph.D., Elizabeth L. Scheppke, B.A.,Stacey K. Moreno, M.S.,Hannele Uusitalo-Jarvinen, M.D., Ph.D.,Jun Yamanouchi, Ph.D., Sanford Shattil, M.D.,Martin Friedlander, M.D., Ph.D.
INTRODUCTION: Previously, we showed that naked plasmid de-oxyribonucleic acid encoding therapeutic genes selectively targetsbrain tumors via intra-arterial injection and improves survival (Bar-nett et al., Gene Therapy, in press). This approach is limited by thelength of time of transgene expression. To improve the efficacy anddurability of gene delivery, we have developed a highly selective,cell-based approach to therapeutic gene delivery.
METHODS: 9L gliosarcoma cells were stereotactically implanted intoSCID mouse brains. Six days later, we stereotactically implanted distinctpopulations of bone marrow-derived cells from mice or humans. Amononuclear fraction from bone marrow was further divided into Lin&and Lin# populations (Otani et al., 2002). The Lin& population is en-riched for endothelial progenitor cells, whereas the Lin# populationcontains hematopoietic precursors. These cells were transduced with alentivirus vector encoding the GFP gene. Mouse brains were removed atdifferent time points and examined by immunohistochemistry.
RESULTS: Both Lin# and Lin& cells derived from mouse proliferate and
target brain tumors, but they exhibit different behavior within the tumors.Initially, the majority of Lin# cells migrate out of the tumor, whereas theLin& cells tend to remain within the tumor. By 20 to 30 days postimplanta-tion, a subpopulation of Lin# cells is observed to proliferate within thetumor parenchyma. In contrast, a subpopulation of Lin& cells proliferate,localize along blood vessels, and migrate to satellite tumor foci. Human bonemarrow cells exhibit similar behavior in this experimental model. Mousebone marrow cells can be genetically modified ex vivo by transduction witha lentivirus vector encoding GFP. The transduction efficiencies vary from 68to 80% for the Lin& population and from 48 to 68% for the Lin# population.We demonstrate selective transgene expression within tumors.
CONCLUSION: A cell-based approach may allow for targeteddelivery of therapeutic genes to brain tumors and may be adapted foruse in humans.
748Functional Recovery after Surgical Resection ofEloquent Brain Areas Invaded by Low-gradeGliomas: The Use of Cerebral PlasticityHugues Duffau, M.D., Ph.D.,Peggy Gatignol, Emmanuel Mandonnet, Ph.D.,Dominique Denvil, M.D., Nicole Sichez, Marianne Leroy,Manuel Lopes, M.D., Ph.D., Luc Taillandier, M.D., Ph.D.,Ahmad Bitar, M.D., Jean-Pierre Sichez, M.D.,Remy Van Effenterre, M.D., Laurent Capelle, M.D.
INTRODUCTION: We describe the abilities of functional recoveryafter surgical resection of eloquent brain areas invaded by glioma anddiscuss the mechanisms of cerebral plasticity.
METHODS: Among a surgical series of 122 low-grade gliomas, 77right-handed patients without deficit were operated on for a low-gradeglioma invading primary and/or secondary sensorimotor and/or lan-guage areas, as shown anatomically by preoperative magnetic resonanceimaging (MRI) and functionally by intraoperative electrical stimulationmapping. Tumors involved 31 supplementary motor areas, 28 insulas, 8primary somatosensory areas, 4 primary motor areas, 4 Broca’s areas,and 2 left temporal language areas.
RESULTS: We observed 77 immediate postoperative deficits, withsecondary recovery within 3 months in all cases except 4 (definitivemorbidity, 5%). Of the resections, 92% were total or near-total on thecontrol MRI.
CONCLUSION: These findings suggest a dynamic spatiotemporalfunctional organization, with, before surgery, the recruitment of compen-satory areas, explaining the lack of deficit despite the tumor growth ineloquent regions; immediately after surgery, the occurrence of a deficit,most likely because of the resection of invaded areas participating in (butnot essential to) the function; and 3 months after surgery, a recovery mostlikely explained by a long-term functional reshaping. The canalization ofthis brain dynamic potential is considered to extend the limits of surgeryin eloquent areas while minimizing the risk of sequelae.
749The Mesopontine Tegmentum: A NewPain-modulatory RegionJonathan D. Carlson, M.D., Ph.D., Kim J. Burchiel, M.D.,Nathan Selden, M.D., Ph.D., Mary M. Heinricher, Ph.D.
INTRODUCTION: This study has identified another brainstem sitethat likely modulates pain. Over the last decade, a large body of
ABSTRACTS OF OPEN PAPERS
468 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

research has elucidated brainstem circuitry that modulates pain. Ingeneral, the periaqueductal gray transmits opioid-induced analgesiato the rostral ventromedial medulla (RVM); the RVM then modulatesthe spinal cord. Within the RVM, two classes of pain-modulatoryneurons are present. “On-cells” demonstrate a burst of activity relatedto nociceptive behavior and have been shown to facilitate pain. “Off-cells” demonstrate a pause in activity and are known to inhibit pain.
METHODS: Microelectrode recording was conducted in 26 rats underlight pentobarbital anesthesia in the mesopontine tegmentum, includingthe cuneiform nucleus, pedunculopontine tegmental nucleus, and lateraldorsal tegmental nucleus. Multiple trials of mechanical (paw pinch) andthermal (controlled heat lamp to tail) noxious stimulation were admin-istered for each neuron. The temporal relationships between stimuli,reflex responses, and neuronal activity were measured. Neuronal loca-tion was reconstructed from reduced nicotinamide adenine dinucleotidephosphate-diaphorase-stained sections.
RESULTS: Cells were classified by their responses to mechanical andheat stimuli and displayed behavior similar to RVM neurons. On-cells(n " 83, 40%), off-cells (n " 15, 7%), and neutral cells (n " 107, 52%) weredistributed throughout the mesopontine tegmentum. The spontaneousactivity of these mesopontine on- and off-cells cycled between active andquiet periods that were out of phase with each other. Each neuronresponded to mechanical and thermal noxious stimulation in the samemanner. These neurons had bilateral whole-body receptive fields.
CONCLUSION: These mesopontine on- and off-cells share manyfeatures of medullary on- and off-cells that are known to modulatepain. This suggests that the mesopontine tegmentum has an importantrole in pain modulation. Further research to delineate how theseneurons interact with other pain modulatory circuits is needed.
750A Neural Network Program Capable ofDistinguishing and Accurately Making theDiagnosis of Different Types of FacialPain SyndromesFarhad M. Limonadi, M.D., Kim J. Burchiel, M.D.
INTRODUCTION: We have developed and evaluated a neuralnetwork program that is capable of distinguishing and accuratelydiagnosing different types of facial pain syndromes.
METHODS: Fifty patients with a complaint of facial pain were askedto fill out a questionnaire at the time of their initial visit. The seniorinvestigator then recorded the facial pain diagnosis for each patient. Thepatients’ responses to the questionnaire and their diagnosis (as the de-sired output) were entered into our neural network program. Using agenetic training algorithm, first an initial population of 50 networks wasrandomly created, each having a different set of parameters. Each ofthese networks was then trained and evaluated (to determine its fitness)on the basis of the minimum error it achieved. The characteristics of thegood networks were then combined and mutated to create a new pop-ulation of networks. This process was repeated until a network withmean square error of 0.009 was evolved. This network was then used topredict the diagnosis of 17 new patients with facial pain.
RESULTS: Our network was able to predict the correct diagnosis ofall initial 50 patients with 100% accuracy. Then, upon being chal-lenged with 17 new patients, it made the diagnosis of TN1 (typicaltrigeminal neuralgia) with 88% sensitivity and 89% specificity. Thesevalues for TN2 (atypical) were 50% and 85%, respectively; for trigem-inal neuropathic pain, 100% and 94%; for trigeminal deafferentationpain, 100% and 100%; for symptomatic trigeminal neuralgia, 50% and
100%; and the diagnosis of postherpetic neuralgia and atypical facialpain was ruled out with 100% specificity.
CONCLUSION: Artificial intelligence programs have the potentialof making the diagnosis of trigeminal neuralgia and related facial painsyndromes with high accuracy. Improved diagnosis will direct pa-tients to appropriate resources and reduce inappropriate treatmentsfor facial pain.
751The Long-term Results of Trigeminal NeuralgiaTreated with Gamma Knife SurgeryJason P. Sheehan, M.D., Ph.D., Hung-Chuan Pan, M.D.,Mateti Stroila, Ph.D., Ladislau Steiner, M.D., Ph.D.
INTRODUCTION: Microvascular decompression has historicallybeen the treatment for medical refractory trigeminal neuralgia (TGN).More recently, gamma knife surgery has been used as an alternative,minimally invasive treatment in TGN. We evaluated the long-termresults of gamma knife surgery for the treatment of TGN.
METHODS: From 1996 to 2003, we treated 146 cases of TGN withgamma knife surgery. The median patient age was 66 years, and themedian time from diagnosis to gamma knife surgery was 72 months.The median follow-up was 18 months. Clinical outcomes and postra-diosurgical magnetic resonance imaging studies were analyzed in astatistical fashion.
RESULTS: The mean time to relief of pain was 24 days. Twenty-eight percent of patients achieved excellent results, 14.4% good re-sults, 39.8% fair results, and 17.8% poor results. The percentage ofpatients who were pain-free at 1, 2, and 3 years of follow-up was 48%,46%, and 39%, respectively. The percentage of patients who experi-enced some degree of improvement in their pain was 90%, 77%, and70% at 1, 2, and 3 years of follow-up, respectively. Thirty-three of 118patients (25%) with initial improvement later experienced recurrenceat a median time of 12 months. Eleven patients (8%) developed theonset of facial numbness after radiosurgery. Postradiosurgical mag-netic resonance imaging changes were noted in 9 patients (7%). Inunivariate analysis, right-sided neuralgia (P " 0.0002) and a previousneurectomy (P " 0.04) correlated with a pain-free outcome; in multi-variate analysis, right-sided neuralgia (P " 0.032) and age (P " 0.05)were statistically significant. New onset of facial numbness aftergamma knife surgery correlated with more than one gamma knifesurgery (P " 0.028) and a previous glycerol injection (P " 0.018).
CONCLUSION: Gamma knife surgery effectuated pain relief in39% and pain improvement in 70% of patients with TGN. Althoughless effective than microvascular decompression, radiosurgery re-mains a reasonable treatment option for those unwilling or unable toundergo more invasive surgical approaches and offers a low risk ofside effects.
752Differential Pattern of Spinal Dorsal Horn GeneExpression during the Expression and Loss ofThermal Hyperalgesia after Chronic ConstrictionInjury of the Rat Sciatic NerveDaniel K. Resnick, M.D., M.S.,Gurwattan S. Miranpuri, Ph.D., Gordanna Miletic, M.D.,Raghu L. Vemuganti, Ph.D., Viejo Miletic, Ph.D.
INTRODUCTION: Plasticity in the spinal dorsal horn may underliethe development of neuropathic pain after peripheral nerve injury. In
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 469

this study, we examined whether the expression and disappearance ofthermal hyperalgesia (as one behavioral sign of neuropathic pain) wasassociated with a differential pattern of gene expression in the spinaldorsal horn.
METHODS: We performed a deoxyribonucleic acid microarrayassay of the dorsal horn of animals exhibiting thermal hyperalgesiaafter a peripheral nerve injury. We compared data from these animalswith controls and with animals whose thermal hyperalgesia hadresolved.
RESULTS: Animals exhibiting thermal hyperalgesia 7 days afterloose ligation of the sciatic nerve (chronic constriction injury) showedsignificant changes in the expression of 16 genes (9 up-regulated, 7down-regulated). In contrast, in animals exhibiting the typical loss ofthermal hyperalgesia 28 days after loose ligation surgery, only 2 geneswere up-regulated, whereas 5 genes were down-regulated. A compar-ison of the gene expression pattern between 7- and 28-day animalsshowed that in the latter animals, some of the genes whose expressionwas up-regulated play an important role in inhibitory neurotransmis-sion (e.g., $-aminobutyric acid-A receptor %2, glycine receptor %16).
CONCLUSION: These data revealed a significant but reversibleshift in the pattern of gene expression in the spinal dorsa horn afterperipheral nerve injury. The data also suggested that in injured ani-mals in which the neuropathic pain had resolved, the pattern of geneexpression was similar to that of control, uninjured animals and thatin both of these groups, the pattern was substantially different fromthat in animals still exhibiting neuropathic pain behavior. These datalent further support to the notion that genetic plasticity in the spinaldorsal horn may be an important contributor to peripheral nerveinjury-elicited neuropathic pain.
753Clinical Results of Pulsed Radiofrequency Lesioningon Dorsal Root Ganglion in Patients with ChronicLow Back and Leg PainJung Y. Park, M.D., Ph.D., Sang H. Keem, M.D.,Sang D. Kim, M.D., Se H. Kim, M.D., Ph.D.,Dong J. Lim, M.D., Ph.D., Hoon K. Lee, M.D., Ph.D.
INTRODUCTION: Pulsed radiofrequency (RF) was recently de-scribed as an alternative technique to conventional, continuous RFlesioning. It allows for application of RF current at 42°C that is notharmful to the tissue. The present study was undertaken to investigatethe effect of pulsed RF treatment on dorsal root ganglion (DRG) forchronic segmental pain radiating to the legs.
METHODS: There were total of 50 patients with persistent lowback pain and leg pain of radicular pattern, without surgery, for morethan 6 months. Six of them had pain that had neuropathic compo-nents. Average age was 49 years, and average Visual Analog Scalescore was 8.4. After diagnostic DRG block, a maximum of 2 DRGswere treated. With a single anteroposterior view under C-arm guid-ance, a transforaminal approach was used for target selection. Afterconfirmation with contrast dye, impedance and sensory and motorthreshold were checked for correct placement of electrodes. Thepulsed RF treatment consisted of a 20-ms RF pulse delivered at a rateof 2 Hz for 240 seconds to produce tissue heated to 42°C. Minimalfollow-up period was 6 months.
RESULTS: All patients tolerated the procedures well. Satisfactoryresults were defined as 50% reduction of original pain. Thirty-eightcases (76%) were successful at 1 month. However, this was decreasedto 32 (64%) at 6 months. Overall patient satisfaction was noted in 40
cases (80%). There were no complications or side effects from theprocedures except in two patients with transient soreness.
CONCLUSION: Treatment with pulsed RF provided an improve-ment of chronic low back pain with radiating leg pain of degreessimilar to those after conventional continuous RF with a heat of 60 to67°C without complications. Thus, it would be a useful treatmentmodality in these clinical settings and may open new horizons forvarious clinical settings, including neuropathic pain.
754Percutaneous Retrogasserian Glycerol Rhizotomyfor Patients with Idiopathic Trigeminal Neuralgia:A Prospective Analysis of Factors Relatedto Pain ReliefBruce E. Pollock, M.D.
INTRODUCTION: Percutaneous retrogasserian glycerol rhizotomy(PRGR) is a commonly performed operation for patients with medi-cally unresponsive trigeminal neuralgia. This study prospectively an-alyzed factors associated with facial pain outcomes after PRGR.
METHODS: From July 1999 to December 2003, 98 patients under-went PRGR as described by Hakanson. Eight patients were lost tofollow-up. In 6 patients (6%), the trigeminal cistern could not bedefined, and the procedure was aborted. The mean patient age was72.1 years. The average pain duration before PRGR was 8.6 years; 46patients had undergone prior surgery. The mean volume of glycerolinjected was 0.31 ml. An excellent facial pain outcome was defined asthe absence of facial pain without medications.
RESULTS: Thirty-one patients (34%) had either no benefit (n " 17)or recurrent pain (n " 14) and required additional surgery at a meanof 7.2 months after PRGR; the mean follow-up of the other 59 patientswas 25.7 months (range, 3–52 mo). Including the patients who did nothave glycerol injected, the 1- and 3-year chance of an excellent facialpain outcome was 61% and 49%, respectively. Multivariate analysis ofclinical and operative factors showed that facial pain on glycerolinjection correlated with excellent facial pain outcomes (RR, 0.99; 95%CI, 0.23–1.75; P " 0.01), whereas patients with constant pain lessfrequently had excellent outcomes (RR, 1.10; 95% CI, 0.03–2.17; P "0.045). Forty-one patients developed either mild numbness/parathesias (n " 37) or dysesthesias (n " 4). New trigeminal deficitsafter PRGR were associated with excellent facial pain outcomes (RR,1.20; 95% CI, 0.51–1.88; P ! 0.001).
CONCLUSION: PRGR remains a good operation for patients withmedically unresponsive trigeminal neuralgia who are considered poorcandidates for posterior fossa exploration. Predictive factors for suc-cess included patients without any constant facial pain, immediatefacial pain after glycerol injection, and patients with new trigeminaldeficits after PRGR.
755Percutaneous Electrode Migration in Spinal CordStimulation: Problem and SolutionViolette M. Renard, M.D., Richard B. North, M.D.
INTRODUCTION: The technical advantages offered by percutane-ous electrodes for spinal cord stimulation (SCS) compared with plateelectrodes include a reduction in the patient’s insertion-related dis-comfort, ease in obtaining accurate results from a screening trial, andlongitudinal access to multiple levels in the spine. These advantages,
ABSTRACTS OF OPEN PAPERS
470 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

however, and insertion through a Tuohy needle require that percuta-neous electrodes be cylindrical, which makes them prone to longitu-dinal migration, even after encapsulation by scar tissue. Modificationof the standard insertion technique, however, can eliminate longitu-dinal migration.
METHODS: When anchoring the same type of percutaneous elec-trodes in a consecutive series of 99 patients during a 3-year period atour institution, we injected a small amount (! 0.1 ml) of siliconeelastomer adhesive between the inner surface of the sleeve and theouter surface of the lead. We reviewed the records of these patients todetermine the incidence and reasons for SCS-related postimplantationsurgical interventions.
RESULTS: By mean follow-up of 20.2 months % 12.3 months(range, 1.8–39.7 months), 15 of our 99 patients had at least one SCS-related surgical procedure (3 because of infection; 4 to increase thearea of coverage; 1 to correct lateral migration caused by sutureseroding through the supraspinous ligament; 1 to deal with posturalchanges in stimulation; 2 to counter receiver-site pain; 3 to correcttechnical failures; and 1 because of inadequate pain relief). No studypatient needed revision because of longitudinal electrode migration.
CONCLUSION: Our simple modification of a standard electrodeimplantation technique eliminates longitudinal migration of the per-cutaneous electrodes used in this study.
756Cellular and Network Mechanisms of Epileptogenesisin Cortical Dysplasia: A Combined Clinical,Pathological, and Electrophysiological StudyGary W. Mathern, M.D., Carlos Cepeda, Ph.D.,Veronique Andre, Ph.D., Mike S. Levine, Ph.D.
INTRODUCTION: Epileptogenesis in cortical dysplasia (CD) isunknown but could be caused by cytomegalic neurons and ballooncells acting as “pacemakers” and/or changes in excitatory and inhib-itory synaptic transmission. This study addressed this question usinga combined clinical-pathological-electrophysiological approach in pe-diatric epilepsy surgery patients with CD.
METHODS: In vitro electrophysiology determined intrinsic mem-brane properties and spontaneous glutamatergic and GABAergic syn-aptic activity for normal-pyramidal neurons, cytomegalic neurons,and balloon cells (n " 360) from 67 neocortical sites from 43 CDpatients (age range, 0.2–14 yr). Magnetic resonance imaging (MRI),fluorodeoxyglucose-positron emission tomography (FDG-PET), andelectrocorticography (ECoG) graded sample sites from least to worstCD abnormality.
RESULTS: Cytomegalic neurons were observed in 60% and ballooncells in 53% of pathological specimens. Cytomegalic neurons and/orballoon cells were most frequent in areas of severe CD compared withmild or normal CD regions as assessed by FDG-PET/MRI, and thepresence of cytomegalic neurons (but not balloon cells) correlatedwith the worse ECoG scores. Using voltage-clamp techniques, cyto-megalic neurons, when depolarized, generated large oscillatoryvoltage-gated calcium spikes, and 25 to 30% of normal-pyramidal andall tested cytomegalic neurons showed decreased magnesium sensi-tivity and loss of NR2B subunit expression. In current clamp, how-ever, cytomegalic and normal-pyramidal neurons displayed similaractive membrane properties without intrinsic bursting. Balloon cellswere electrically silent using similar techniques. Normal-pyramidalneurons displayed decreased spontaneous glutamatergic synaptic ac-tivity in the areas of most severe hypometabolism by FDG-PET com-
pared with normal regions, and there were no changes in GABAergicsynaptic activity based on FDG-PET/MRI abnormalities.
CONCLUSION: In CD, these findings indicate that cytomegalicand normal-pyramidal neurons but not balloon cells could be candi-date epileptogenic neurons but are not likely to be “pacemaker” cells.Instead, epileptogenic neurons and abnormal synaptic circuits work-ing together probably contribute to seizure generation in CD tissue.
757Programmable versus Fixed-pressure Valves for theTreatment of Hydrocephalus in ChildrenChris Heller, M.D., Mark D. Krieger, M.D.,David I. Sandberg, M.D., Bryan C. Oh, M.D.,J. Gordon McComb, M.D.
INTRODUCTION: Programmable shunt valves have been advo-cated for the treatment of hydrocephalus with the expectation of feweroperative revisions. We studied the efficacy of these valves in chil-dren, a group that traditionally poses unique challenges in the treat-ment of hydrocephalus.
METHODS: Under an institutional review board-approved proto-col, we retrospectively reviewed 197 children undergoing either in-sertion of a ventriculoperitoneal, pleural, or atrial shunt or shuntrevision involving valve replacement over an 18-month period.Ninety-nine children in the “Delta” group received Medtronic Deltavalves with nonadjustable pressure settings. Ninety-eight children inthe “Strata” group received Medtronic Strata programmable valves.The Delta and Strata groups were matched in terms of age (mean, 7.2and 7.4 yr, respectively) and cause of hydrocephalus. Shunt survival,infections, and valve adjustments were tabulated.
RESULTS: The Delta and Strata groups had similar rates of revision(13 of 99 [13%] and 15 of 98 [15%], respectively) and infection (5 of 99[5%] and 8 of 98 [8%], respectively). Five patients in the Strata grouprequired pressure adjusments for symptoms consistent with elevatedintracranial pressure, but three of these patients subsequently re-quired surgical revision. Three patients had their valve settingschanged by magnetic resonance imaging (MRI) with severe symptomsincluding bradycardia and posturing. All of these patients recoveredfully with reprogramming of their valves. We also noted increasedmetallic artifact on MRI with the programmable valves, which im-paired imaging of the posterior fossa.
CONCLUSION: Ninety-eight programmable valve placementswere therapeutically efficacious in two patients but caused seriousproblems after MRI in three patients and impaired MRI scans inothers. We did not find a significant advantage in using programma-ble shunt valves to offset the higher cost, post-MRI reset problems,and effect on MRI scan quality.
758Convection-enhanced Delivery ofGlucocerebrosidase to the Primate Brainas a Potential Treatment for NeuronopathicGaucher’s DiseaseMichele Aizenberg, M.D., Stuart Walbridge, B.S.,Murray J. Gary, Ph.D., Alexander O. Vortmeyer, M.D.,Roscoe O. Brady, M.D., Edward H. Oldfield, M.D.,Russell R. Lonser, M.D.
INTRODUCTION: Similar to other metabolic storage diseases, sys-temic enzyme replacement therapy for Gaucher’s disease has not
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 471

prevented the premature death or severe morbidity associated withneuronopathic variants because glucocerebrosidase does not cross theblood-brain barrier. We used convection-enhanced delivery (CED) forregional distribution of glucocerebrosidase to perfuse primate brainsand determine its safety and feasibility as a treatment option forneuronopathic Gaucher’s disease
METHODS: Toxicity studies were performed by intrastriatal infu-sion of glucocerebrosidase in 12 rats. Animals were observed clinicallyand killed at 14 hours (n " 4), 4 days (n " 4), and 6 weeks (n " 4). Twoprimates underwent perfusion of the right frontal lobe with glucoce-rebrosidase using CED. Serial real-time magnetic resonance imaging(MRI) was performed during enzyme infusion. Primates were ob-served clinically and then killed (day 2 of infusion). All animalsunderwent histological and enzymatic analyses of the brain.
RESULTS: No rats had clinical or histological evidence of toxicity.In primates, MRI revealed progressive and complete perfusion of theright frontal lobe (white and gray matter) with infusate. The primateshad no clinical deficits during infusion. Histological analysis revealedno toxicity, and immunohistochemistry demonstrated intraneuronalstaining for glucocerebrosidase. Enzyme activity (nmol of substrateconverted per h) was significantly increased in white matter (mean,5450 nmol/h) and cortex (mean, 330 nmol/h) on the infused side,compared with the control (noninfused) side (mean, 50 and 66nmol/h, respectively; P ! 0.05).
CONCLUSION: These findings suggest that CED can be used tosafely perfuse large regions of the brain with therapeutic levels of glu-cocerebrosidase. Patients with neuronopathic Gaucher’s disease maybenefit from this therapeutic approach. Moreover, other similar CNSprotein deficiency disorders may be treatable by a similar technique.
759Options for the Management of Patients withHypothalamic Hamartoma and Intractable EpilepsyHarold Rekate, M.D., Iman Feiz-Erfan, M.D.,Yu Tse Ng, M.D., John Kerrigan, M.D.,Margaret Varland, R.N.
INTRODUCTION: Hypothalamic hamartomas are rare congenitalmasses in the hypothalamus that often present with intractable epi-lepsy and behavioral disturbances. Recently, several different ap-proaches to the management of these lesions have been advocated.The purpose of this study is to analyze the various methods that havebeen shown to lead to seizure control.
METHODS: The report reviews the course of 38 patients withintractable seizures and hypothalamic hamartomas treated over an18-month period. Data were collected prospectively in our databasefor the purpose of a study of outcome. Two patients underwent anextended pterional approach. Two patients underwent gamma knifetreatment; 25 underwent a transcallosal interforniceal approach; and 9underwent endoscopic removal through the foramen of Monro. Onepatient underwent two procedures.
RESULTS: Pedunculated masses that are not in the third ventricleare not candidates for transventricular approaches. Twenty-one of 25patients undergoing transcallosal interforniceal approaches and 6 of 9endoscopically resected patients are seizure free. Only one patient ineach group has not had dramatic improvement in seizure control andquality of life. The two patients treated with gamma knife are toorecent to judge effectiveness.
CONCLUSION: Both transcallosal interforniceal and endoscopic
resection of sessile hypothalamic hamartomas are feasible, withmarked improvement in outcome and low morbidity. Endoscopicremoval seems to be as effective, with lower immediate morbidity,and is now our treatment of choice in all but very large masses insmall children.
760Management of Hydrocephalus Using a NoninvasiveMagnetic Resonance Imaging Method forMeasurement of Intracranial Compliance and PressureRoberta P. Glick, M.D., Terry Lichtor, M.D.,Patricia Raksin, M.D., Aaron Lee, B.A.,Anusha Sivaramakrishnan, M.D., Susha Surapaneni,B.A., Osbert Egibor, M.D., Noam Alperin, Ph.D.
INTRODUCTION: Measurements of intracranial compliance (ICC)and intracranial pressure (ICP) are clinically important in the manage-ment of patients with hydrocephalus, especially when treating patientswith possible shunt malfunction. In this work, we present a noninvasivemagnetic resonance imaging (MRI) technique for determination of ICPand ICC. Using standardized measurements obtained from normal pa-tients and patients with severe head trauma (with ICP monitors) we nowapplied this method to patients with hydrocephalus.
METHODS: The compliance index is derived from the measuredchanges in the ICP and volume of blood and cerebrospinal fluid (CSF)in the intracranial space that occur naturally during each cardiac cycle,obtained with a motion-sensitive MRI scan. Intracranial volume andICP changes are calculated from MRI measurements of CSF flow andblood volumetric flow rates. The change in pressure is derived fromthe pressure gradient calculated from velocity. Twenty patients pre-senting with symptoms suggestive of symptomatic hydrocephaluswere studied to determine the need for surgery.
RESULTS: The clinical cases included congenital hydrocephalus(some of which had no shunt surgery for $10 yr), tumor, toxoplas-mosis, slit ventricles, aqueductal stenosis, and Chiari malformation.Patients presented with a variety of symptoms, including headaches,visual blurring, seizures, neck pain, nausea/vomiting, gait distur-bances, and lethargy. This technique correctly identified three patientsrequiring surgery, and ICP measured at surgery correlated with MRI-ICP. Two patients with third ventriculostomies and enlarged ventri-cles avoided surgery because extraventricular drain (EVD) measure-ments correlated with normal MRI-ICP. In three patients with EVDs,pressures correlated with low MRI-ICP measurements. Nonsurgicalcases were closely observed and have remained stable.
CONCLUSION: These results suggest MRI-ICP sensitivity suffi-cient to differentiate between normal and elevated ICP in patientswith a variety of subtypes of hydrocephalus. Noninvasive MRI-ICPmay be a useful tool in the determination of the need for a shunt orshunt revision and may enable patients to avoid unnecessary surgeryor invasive monitoring procedures.
761Long-term Results of Endoscopic AqueductoplastyHenry W.S. Schroeder, M.D., Joachim M.K. Oertel, M.D.,Joerg Baldauf, M.D., Michael R. Gaab, M.D., Ph.D.
INTRODUCTION: Endoscopic aqueductoplasty is an option in thetreatment of obstructive hydrocephalus caused by aqueductal steno-ses. We report on our experience with this endoscopic technique,focusing on indications, operative technique, and results.
ABSTRACTS OF OPEN PAPERS
472 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

METHODS: A series of 39 endoscopic aqueductoplasties was per-formed in 33 patients harboring a hydrocephalus caused by aqueductalstenosis. In 13 patients, a third ventriculostomy was performed simulta-neously.
RESULTS: There was no endoscopy-related mortality. One aque-ductoplasty had to be abandoned. The mean follow-up period was 40months (range, 1 to 97 mo). In seven patients, reclosure of the restoredaqueduct required an endoscopic revision. In 25 patients (76%), thehydrocephalus-related symptoms resolved or improved. The condi-tion was unchanged in eight patients. Four patients needed to beshunted. The ventricles decreased in size in 22 patients (67%), werelarger in two, and unchanged in the remaining nine patients.
CONCLUSION: Endoscopic aqueductoplasty is a treatment optionin patients with hydrocephalus caused by membranous aqueductalstenosis. Unfortunately, the reclosure rate is higher than initiallyexpected. More experience and longer follow-up is necessary to de-termine the value of endoscopic aqueductoplasty in the treatment ofhydrocephalus caused by aqueductal stenosis.
762Age, Shunted Hydrocephalus, andMyelomeningocele as Factors PredictingOutcome with Endoscopic Third VentriculostomyPaul K. Kim, M.D., Steven S. Glazier, M.D.
INTRODUCTION: Endoscopic third ventriculostomy (ETV) hasbeen accepted as an effective treatment of obstructive hydrocephalus(OH) in selected patients. Age and presence of preexisting shunt havebeen debated as factors affecting ETV. We reviewed our series todetermine factors affecting outcome, including those with myelome-ningocele, with the aim of achieving greater success with ETV.
METHODS: From 1998 to 2003, 68 patients with OH underwentETV using a rigid endoscope with working channel and NMT ballooncatheter. Retrospective review with mean follow-up of 2 years iden-tified 47 patients with isolated aqueductal stenosis (AS), 9 with my-elomeningocele, and 12 with space-occupying lesions of the third/fourth ventricle. Success was defined as resolution of hydrocephaluswithout subsequent shunting after ETV.
RESULTS: The overall success rate was 74%. In the AS group, therewas 89% success in those $2 years old, but only 52% success in those !2years old. In those with obstructive lesions of the third/fourth ventricle,there was 100% success in the nine patients $2 years old, whereas thethree patients !2 years old failed. In the myelomeningocele group, 67%success was noted; five of the six successful myelomeningocele patientswere $2 years old and had magnetic resonance imaging (MRI) cineevidence of AS and cerebrospinal fluid (CSF) outflow obstruction. Onlytwo myelomeningocele patients did not have a preexisting shunt, andnone of the failures had previous history of meningitis.
CONCLUSION: Our results demonstrate high rates of failure inpatients !2 years old with OH, which have been supported by otherstudies. No correlation between failure and the presence of a preex-isting shunt was found in any group. The emerging acceptance of ETVfor older patients with AS is validated by our results. Moreover, oursuccess with older myelomeningocele patients indicates that MRI cineshould be considered to assess for CSF outflow obstruction and po-tential benefit from ETV. Appropriate recognition of OH and success-ful ETV has significant impact in the overall treatment of myelomen-ingocele patients, many of whom have significant comorbidities.
763The Effects of Surgical Resection and AdjuvantTherapy on Pediatric Intracranial EpendymomasMark D. Krieger, M.D., Ira Bowen, B.A.,J. Gordon McComb, M.D.
INTRODUCTION: The optimal management of pediatric intracra-nial ependymomas is controversial. The benefit of surgical resection iswidely accepted; the role of adjuvant therapy is subject to debate. Tofurther understand the efficacy of surgical and adjuvant therapies onependymomas, we retrospectively reviewed the records of 28 consec-utive children with ependymomas.
METHODS: This institutional review board-approved study con-sisted of 28 children, age 5 to 51 months (mean age, 43 mo), surgicallytreated for ependymomas between 1993 and 2003. There were 8 (29%)female and 20 (71%) male patients. Eleven (39%) of these tumors wereanaplastic, and 3 (11%) were disseminated at diagnosis. Twenty-sixependymomas (93%) were located infratentorially, whereas 2 (7%)were located supratentorially. Twenty-one patients (75%) underwentgross total resection (GTR), and 7 (25%) underwent subtotal resectionor biopsy (stereotactic radiosurgery, STR). Follow-up ranged from 1 to95 months, with a median of 30 months.
RESULTS: The 3- and 5-year progression-free survival rates (PFS)of these 28 patients were 21% and 11%, respectively; 3- and 5-yearoverall survival rates (OS) were 39% and 18%. In this limited series,age, tumor location, and tumor histology did not contribute to out-come as independent variables. The extent of surgical resection hadthe greatest influence on outcome: patients with GTR had PFS of 35months (versus 7 mo for STR, P " 0.001) and OS of 44 months (versus15 mo for STR, P " 0.02). The survival advantage of adjuvant therapyafter GTR was not statistically significant with PFS of 31 months(versus 25 mo for GTR alone, P " 0.36) and OS of 40 months (versus31 mo for GTR alone, P " 0.20).
CONCLUSION: Extent of resection is the most important determi-nant of survival in patients with ependymomas. No independentbenefit could be demonstrated with adjuvant therapy.
764Simvastatin Attenuates Experimental CerebralVasospasm and Ameliorates Serum Markers ofNeuronal and Endothelial Injury in Patients afterSubarachnoid Hemorrhage: A Dose-Response EffectDependent on Endothelial Nitric Oxide SynthaseMatthew J. McGirt, M.D., Gustavo Pradilla, M.D.,John Lynch, M.D., Federico G. Legnani, M.D.,Marilyn Perez, B.S., Rafael Tamargo, M.D.,Richard E. Clatterbuck, M.D., Ph.D., Daniel Laskowitz, M.D.
INTRODUCTION: Endothelial nitric oxide synthase (eNOS) activ-ity and nitric oxide bioavailability decline after subarachnoid hemor-rhage (SAH) and may contribute to cerebral vasospasm. We examinedwhether simvastatin increases cerebrovascular eNOS after SAH, at-tenuates cerebral vasospasm at clinically approved doses by an eNOS-dependent mechanism, and is safe in patients with SAH.
METHODS: High dose: 38 mice received simvastatin 20 mg/kg orvehicle for 14 days before endovascular perforation of the anteriorcerebral artery or sham surgery. Motor function was assessed for 3days after SAH by rotorod testing. Middle cerebral artery (MCA)diameter and cerebrovascular eNOS protein were measured 72 hoursafter SAH. The study was repeated in 16 wild-type versus transgenic
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 473

eNOS-knockout mice. Low dose: 30 mice received 1 mg/kg, 0.2 mg/kg, or vehicle for 14 days before SAH, and motor function wasassessed for 3 days after SAH. Post-SAH dose: 15 New Zealand whiterabbits underwent autologous blood injection into the cisterna magnaor sham surgery. Rabbits received simvastatin 60 mg/kg or vehicle for3 days after SAH. Basilar artery lumen patency was assessed 72 hoursafter SAH. Human dose: 17 patients were randomized to simvastatin80 mg/day or placebo for 14 days after SAH. Serum aspartateaminotransferase/alanine aminotransferase, creatine phosphokinase,von Willebrand factor (vWF), S-100a, tumor necrosis factor (TNF)-%,and transcranial Doppler (TCD) velocities were recorded for 14 days.
RESULTS: Simvastatin 20 mg/kg versus vehicle attenuated MCAvasospasm (percent lumen reduction, 27 % 18% versus 51 % 17%, P "0.02), increased cerebrovascular eNOS protein threefold (P " 0.04),and reduced neurodeficits (P " 0.01) in wild-type but not in eNOS-knockout mice (percent lumen reduction, 46 % 20% versus 50 % 19%,P " 0.82). Simvastatin 1 mg/kg, not 0.2 mg/kg, reduced neurologicaldeficits after SAH. In rabbits, post-SAH simvastatin 60 mg/kg atten-uated basilar artery vasospasm (percent lumen reduction, 16 % 5%versus 35 % 10%; P " 0.01). In patients, simvastatin 80 mg/d reducedserum vWF, S-100a, TNF, and TCD vasospasm (mean, $200 cm/s; 0%versus 38%, P " 0.08). No patients developed hepatitis/myositis.
CONCLUSION: High-dose simvastatin before SAH attenuated va-sospasm and neurological deficits in mice. This effect persisted whensimvastatin was given after SAH or at lower doses approved forhuman use but was lost in eNOS-knockout mice, suggesting an eNOS-dependent mechanism of action. Simvastatin was safe in patients withSAH and may be an effective agent in the management of SAH.
765Genome-wide Linkage Analysisof Intracranial AneurysmsBrian V. Nahed, B.S., Abigail A. Hawkins, B.A.,Michael L. Diluna, M.D., Askin Seker, M.D.,Bulent Guclu, M.D.,Andrea Chamberlain, B.S.N., C.C.R.N., R.N.,Mathew W. State, M.D., Ph.D., Murat Gunel, M.D.
INTRODUCTION: Genetic risk factors, in addition to environmen-tal risk factors, contribute to the formation and/or rupture of cerebralaneurysms. Previous genome-wide linkage studies suggest linkage at5q22-q31, 7q11, 14q22, and 19q13.3 with candidate genes such aselastin, COL3A1 (ch 2q31), fibrillin (ch 15q21), and endoglin (intron 7).However, attempts to reproduce these results failed, indicating thelimitations inherent in nonparametric and candidate gene analysis. Inthis study, genome-wide linkage analysis and parametric methodswere used to identify the gene(s) leading to intracranial aneurysm(ICA).
METHODS: Since 1994, we have prospectively screened over 3000patients with ICAs and their relatives, identifying 142 multiplex fam-ilies with 345 affected patients. Twenty-one of these families havemore than four affected members, and four have more than sevenaffected members. Using Affymetrix genechips containing over 10,500single-nucleotide polymorphisms, we performed genome-wide link-age analysis on our largest kindreds to identify regions of linkage.Once regions were identified, we fine-mapped these loci by usingmicrosatellite markers to narrow these linked intervals. Subsequentcandidate gene analysis provided novel genes of interest.
RESULTS: Genome-wide linkage analysis using Genechips iden-tifed a total of eight loci linked to ICA phenotype that gave near
maximum theoretical logarithm of the odds scores. Further analysisusing microsatelite markers excluded five of these regions, leavingthree loci possibly contributing to the formation of ICA. We are nowperforming mutational analysis within these three regions.
CONCLUSION: Parametric methods successfully identified novelchromosomal regions linked to ICA. Subsequent fine-mapping ofthese regions has confirmed linkage at our novel sites and excludedother regions, particularly those previously thought to be ICA-related.This might be caused by genetic heterogeneity of ICA or because ofinherent limitations of nonparametric studies. Finally, gene screeningand candidate gene analysis within these linked intervals have re-vealed at least two novel candidate genes involved in angiogenesis,cell adhesion, and remodeling.
766Vasospasm Probability Index: A Combinationof Transcranial Doppler Velocities, CerebralBlood Flow, and Clinical Risk Factors to PredictCerebral Vasospasm after SubarachnoidAneurysm HemorrhageNestor Gonzalez, M.D., Thomas Glenn, Ph.D.,John Boscardin, Ph.D., Fernando Vinuela, M.D.,Neil Martin, M.D.
INTRODUCTION: The purpose of this study was to evaluate trans-cranial Doppler (TCD) velocities, Lindegaard ratio (LR), and spasmindex (SI) in the diagnosis of cerebral vasospasm and to create avasospasm probability index (VPI) to improve the vasospasm diag-nosis accuracy after subarachnoid hemorrhage (SAH).
METHODS: A total of 795 patients with SAH underwent TCDsbetween April 1998 and January 2000. Of these, 154 patients hadangiographies and 75 had 133Xe cerebral blood flow studies the sameday. Seven cases were excluded because of poor sonographic window.Factors analyzed included age, sex, Hunt and Hess and Fisher grades,day after SAH, treatment day, treatment type (clipping, embolization,or conservative), and tobacco and hypertension history. Contingencytables were constructed to calculate tests accuracy. Logistic regressionwas used to evaluate the predictive factors, and their coefficients wereintegrated in the VPI.
RESULTS: Forty-one women (60.3%) and 27 men, age 35 to 84 years(mean, 58 yr) were included. Eighteen (26.5%) had symptomatic va-sospasm. Mean middle cerebral artery-TCD velocities in patients withvasospasm was 147.9 cm/s (standard deviation, 57.0), versus83.1cm/s (standard deviation, 41.1) (P ! 0.0001). Average LR was 5.14(standard deviation, 2.48) for arteries with vasospasm, versus 2.42(standard deviation, 1.01) (P ! 0.0001). Mean SI for vasospasm caseswas 5.11 (standard deviation, 2.11) versus 2.32 (standard deviation,1.05) (P ! 0.0001). Thirty-three patients (48.5%) had angiographicvasospasm. Mean middle cerebral artery-TCD velocity was 142.7cm/s (standard deviation, 62.0), versus 77.5 cm/s (standard deviation,32.4) (P ! 0.0001). Mean LR in arteries with vasospasm was 4.76(standard deviation, 2.35), versus 2.29 (standard deviation, 0.79) (P !0.0001). Mean SI in angiographic vasospasm was 4.49 (standard devi-ation, 2.17) versus 2.27 (standard deviation, 1.01) (P ! 0.0001). Nosignificant differences were observed between surgical, endovascular,and conservative treatment or in patients with history of hypertensionor smokers. Sensitivity, specificity, and predictive values are shown inTable 1. After logistic regression analysis, significant predictors ofvasospasm were Fisher grade, Hunt and Hess grade, LR, and SI. A
ABSTRACTS OF OPEN PAPERS
474 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com
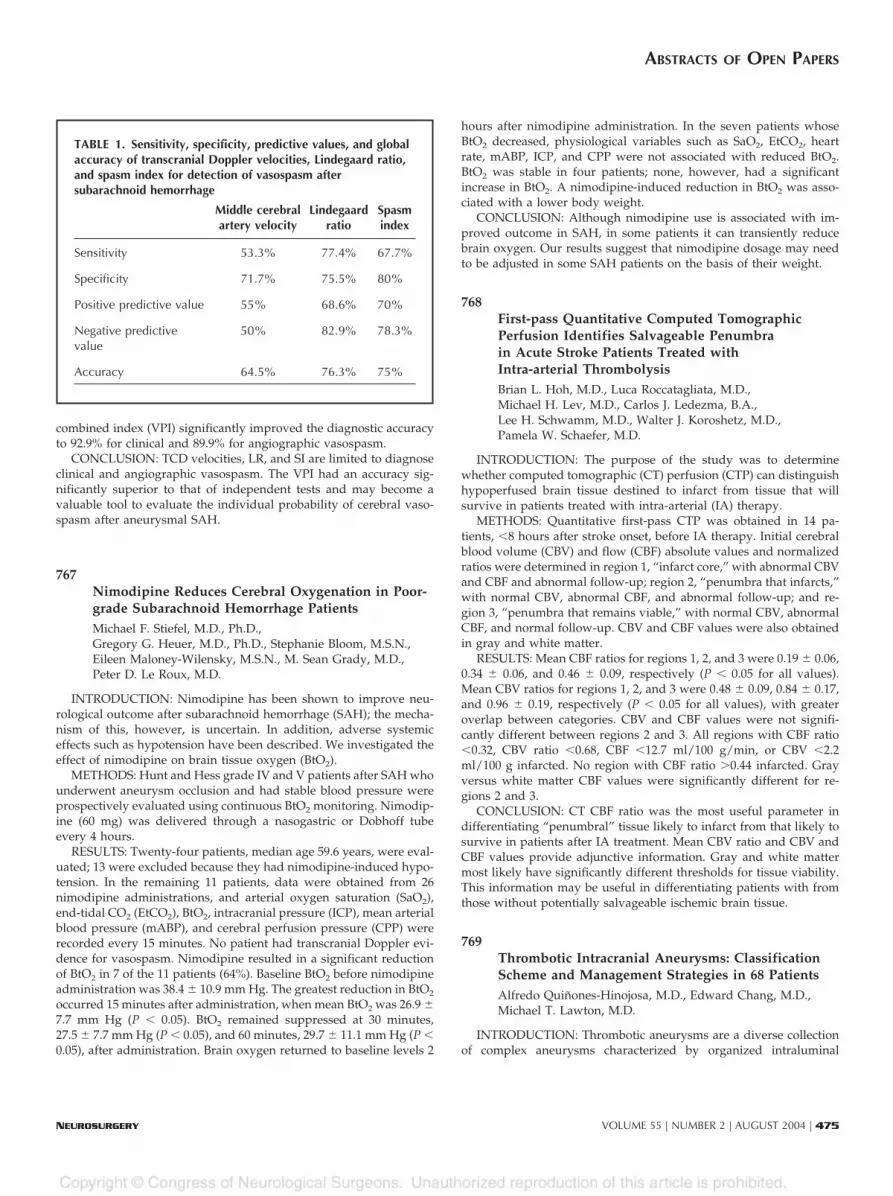
combined index (VPI) significantly improved the diagnostic accuracyto 92.9% for clinical and 89.9% for angiographic vasospasm.
CONCLUSION: TCD velocities, LR, and SI are limited to diagnoseclinical and angiographic vasospasm. The VPI had an accuracy sig-nificantly superior to that of independent tests and may become avaluable tool to evaluate the individual probability of cerebral vaso-spasm after aneurysmal SAH.
767Nimodipine Reduces Cerebral Oxygenation in Poor-grade Subarachnoid Hemorrhage PatientsMichael F. Stiefel, M.D., Ph.D.,Gregory G. Heuer, M.D., Ph.D., Stephanie Bloom, M.S.N.,Eileen Maloney-Wilensky, M.S.N., M. Sean Grady, M.D.,Peter D. Le Roux, M.D.
INTRODUCTION: Nimodipine has been shown to improve neu-rological outcome after subarachnoid hemorrhage (SAH); the mecha-nism of this, however, is uncertain. In addition, adverse systemiceffects such as hypotension have been described. We investigated theeffect of nimodipine on brain tissue oxygen (BtO2).
METHODS: Hunt and Hess grade IV and V patients after SAH whounderwent aneurysm occlusion and had stable blood pressure wereprospectively evaluated using continuous BtO2 monitoring. Nimodip-ine (60 mg) was delivered through a nasogastric or Dobhoff tubeevery 4 hours.
RESULTS: Twenty-four patients, median age 59.6 years, were eval-uated; 13 were excluded because they had nimodipine-induced hypo-tension. In the remaining 11 patients, data were obtained from 26nimodipine administrations, and arterial oxygen saturation (SaO2),end-tidal CO2 (EtCO2), BtO2, intracranial pressure (ICP), mean arterialblood pressure (mABP), and cerebral perfusion pressure (CPP) wererecorded every 15 minutes. No patient had transcranial Doppler evi-dence for vasospasm. Nimodipine resulted in a significant reductionof BtO2 in 7 of the 11 patients (64%). Baseline BtO2 before nimodipineadministration was 38.4 % 10.9 mm Hg. The greatest reduction in BtO2
occurred 15 minutes after administration, when mean BtO2 was 26.9 %7.7 mm Hg (P ! 0.05). BtO2 remained suppressed at 30 minutes,27.5 % 7.7 mm Hg (P ! 0.05), and 60 minutes, 29.7 % 11.1 mm Hg (P !0.05), after administration. Brain oxygen returned to baseline levels 2
hours after nimodipine administration. In the seven patients whoseBtO2 decreased, physiological variables such as SaO2, EtCO2, heartrate, mABP, ICP, and CPP were not associated with reduced BtO2.BtO2 was stable in four patients; none, however, had a significantincrease in BtO2. A nimodipine-induced reduction in BtO2 was asso-ciated with a lower body weight.
CONCLUSION: Although nimodipine use is associated with im-proved outcome in SAH, in some patients it can transiently reducebrain oxygen. Our results suggest that nimodipine dosage may needto be adjusted in some SAH patients on the basis of their weight.
768First-pass Quantitative Computed TomographicPerfusion Identifies Salvageable Penumbrain Acute Stroke Patients Treated withIntra-arterial ThrombolysisBrian L. Hoh, M.D., Luca Roccatagliata, M.D.,Michael H. Lev, M.D., Carlos J. Ledezma, B.A.,Lee H. Schwamm, M.D., Walter J. Koroshetz, M.D.,Pamela W. Schaefer, M.D.
INTRODUCTION: The purpose of the study was to determinewhether computed tomographic (CT) perfusion (CTP) can distinguishhypoperfused brain tissue destined to infarct from tissue that willsurvive in patients treated with intra-arterial (IA) therapy.
METHODS: Quantitative first-pass CTP was obtained in 14 pa-tients, !8 hours after stroke onset, before IA therapy. Initial cerebralblood volume (CBV) and flow (CBF) absolute values and normalizedratios were determined in region 1, “infarct core,” with abnormal CBVand CBF and abnormal follow-up; region 2, “penumbra that infarcts,”with normal CBV, abnormal CBF, and abnormal follow-up; and re-gion 3, “penumbra that remains viable,” with normal CBV, abnormalCBF, and normal follow-up. CBV and CBF values were also obtainedin gray and white matter.
RESULTS: Mean CBF ratios for regions 1, 2, and 3 were 0.19 % 0.06,0.34 % 0.06, and 0.46 % 0.09, respectively (P ! 0.05 for all values).Mean CBV ratios for regions 1, 2, and 3 were 0.48 % 0.09, 0.84 % 0.17,and 0.96 % 0.19, respectively (P ! 0.05 for all values), with greateroverlap between categories. CBV and CBF values were not signifi-cantly different between regions 2 and 3. All regions with CBF ratio!0.32, CBV ratio !0.68, CBF !12.7 ml/100 g/min, or CBV !2.2ml/100 g infarcted. No region with CBF ratio $0.44 infarcted. Grayversus white matter CBF values were significantly different for re-gions 2 and 3.
CONCLUSION: CT CBF ratio was the most useful parameter indifferentiating “penumbral” tissue likely to infarct from that likely tosurvive in patients after IA treatment. Mean CBV ratio and CBV andCBF values provide adjunctive information. Gray and white mattermost likely have significantly different thresholds for tissue viability.This information may be useful in differentiating patients with fromthose without potentially salvageable ischemic brain tissue.
769Thrombotic Intracranial Aneurysms: ClassificationScheme and Management Strategies in 68 PatientsAlfredo Quinones-Hinojosa, M.D., Edward Chang, M.D.,Michael T. Lawton, M.D.
INTRODUCTION: Thrombotic aneurysms are a diverse collectionof complex aneurysms characterized by organized intraluminal
TABLE 1. Sensitivity, specificity, predictive values, and globalaccuracy of transcranial Doppler velocities, Lindegaard ratio,and spasm index for detection of vasospasm aftersubarachnoid hemorrhage
Middle cerebralartery velocity
Lindegaardratio
Spasmindex
Sensitivity 53.3% 77.4% 67.7%
Specificity 71.7% 75.5% 80%
Positive predictive value 55% 68.6% 70%
Negative predictivevalue
50% 82.9% 78.3%
Accuracy 64.5% 76.3% 75%
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 475

thrombus and solid mass. Consequently, their treatment often re-quires techniques other than conventional clipping, such as thrombec-tomy with clip reconstruction or bypass with parent artery occlusion.A single-surgeon experience with thrombotic aneurysms was ana-lyzed to determine optimal treatment strategies. A classificationscheme was devised, based on aneurysm, thrombus, and lumen mor-phology, to relate these anatomic features to surgical therapy.
METHODS: Sixty-eight patients with thrombotic aneurysms weremanaged over a 6.25-year period. Thrombotic aneurysms were clas-sified into six types: concentric (n " 17, 25%), eccentric (n " 14, 21%),lobulated (n " 2, 3%), complete (n " 2, 3%), canalized (n " 17, 25%),and coiled (n " 16, 24%).
RESULTS: Aneurysm management consisted of direct clipping(n " 22, 32%), thrombectomy-clip reconstruction (n " 18, 26%),bypass-occlusion (n " 20, 29%), other (n " 6, 9%), or observation (n "2, 3%). Complete angiographic obliteration was achieved in 97% ofpatients, and 47% of aneurysms were thrombectomized. The surgicalmortality rate was 6%, and the permanent neurological morbidity ratewas 7%. Overall, 87% of patients were improved or unchanged atfollow-up, with 79% reaching Glasgow Outcome Scale score of 5 or 4.Management strategy was influenced by thrombotic aneurysm type,but patient outcome was not. The best results were observed inpatients treated with direct clipping and bypass-occlusion.
CONCLUSION: Despite their solid mass, one third of thromboticaneurysms can be treated surgically with conventional clipping.Direct clipping is associated with the best surgical results, and theproposed classification scheme identifies thrombotic aneurysmsthat may be clippable. Patients with unclippable thrombotic aneu-rysms had more favorable results when treated with bypass andaneurysm occlusion than with thrombectomy and clip reconstruction.The classification scheme may provide conceptual clarity and thera-peutic guidance with preoperative and intraoperative decision-making.
770Synchrotron-supported Cerebral Angiography in anAnimal ModelMichael E.B. Kelly, M.D., Elizabeth Schulke, M.D.,Stephan Fiedler, Ph.D., Michel Renier, Ph.D.,Jean-Francois Le Bas, Ph.D., Bernhard Juurlink, Ph.D.,L. Dean Chapman, Ph.D., Kotoo Meguro, M.D.
INTRODUCTION: Conventional cerebral angiography involvesintra-arterial injection of contrast material. This results in some risk topatients undergoing the procedure. A new method of intravenouscerebral angiography is possible and has been used for coronaryangiography. This technique uses monochromatic radiation from asynchrotron to perform K-edge digital subtraction angiography by anintravenous injection. We applied this technique to perform intrave-nous cerebral angiography in an animal model. To the best of ourknowledge, this represents the first attempt to perform intravenouscerebral angiography using a synchrotron radiation source.
METHODS: A total of six male 2.5-kg New Zealand rabbits weresubjected to conventional intra-arterial angiography and intravenousK-edge digital subtraction angiography. The experiments were per-formed at the European Synchrotron Radiation Source in Grenoble,France. Appropriate ethics approval was obtained. The animals wereanesthetized and tracheotomies performed. Conventional subtractionangiography was performed using direct carotid canalization in two
animals. Four animals underwent intravenous K-edge digital subtrac-tion angiography using synchrotron radiation sources. Various iodinecontrast doses were analyzed. Image analysis was then performedusing Integrated Development Environment 6.0. The animals werekilled.
RESULTS: Conventional intra-arterial angiography was able toshow the major intracranial vessels but no smaller branches. Conven-tional intravenous angiography did not show any intracranial vessels.Using intravenous K-edge digital subtraction angiography, we wereable to visualize the major intracranial vessels and smaller branches.Visualization was achieved with as little as 0.5 ml/kg of iodinatedcontrast material (Iomeprol, 714 mg/ml). Synchrotron-based comput-erized tomographic angiography was also performed.
CONCLUSION: In this study, we were able to obtain excellentcharacterization of the cerebral vasculature in an animal model usingintravenous injection of contrast material. This technique usessynchrotron-based K-edge digital subtraction angiography. Furtherstudies are needed before human studies are undertaken.
771Racial/Ethnic Differences in Demographics, AcuteComplications, and Outcome in Patients withSubarachnoid Hemorrhage: A Large Patient SeriesDavid Rosen, M.D., Roberta Novakovic, M.D.,Fernando Goldenberg, M.D., Axel Rosengart, M.D., Ph.D.,Jeffrey Frank, M.D., R. Loch Macdonald, M.D., Ph.D.
INTRODUCTION: Few studies have examined the impact of racialand ethnic differences on demographics, clinical characteristics, acutecomplications, and outcome of patients with aneurysmal subarach-noid hemorrhage (SAH). The purpose of this study was to examinethis issue.
METHODS: We evaluated prospectively collected data on 1720patients with aneurysmal SAH entered into two randomized, double-blind, placebo-controlled trials conducted in neurosurgical centers inNorth America between 1991 and 1997. Admission characteristics,treatment modalities, in-hospital complications, and 3-month out-come assessed on the Glasgow Outcome Scale were compared by useof "2 test, t test, Wilcoxon rank-sum test, and multiple logistic regres-sions with a significance level of 0.05 among black (n " 241), white(n " 1342), and other minority patients (n " 128).
RESULTS: Whites were significantly older than other races (P !0.0001). Blacks more frequently had a history of hypertension (P !0.0001) and more commonly had elevated blood pressure at the timeof admission (P ! 0.0001). Blacks and other minorities were morelikely to have internal carotid aneurysms, and whites were more likelyto have posterior circulation aneurysms (P " 0.0002). In-hospitalcomplications were not significantly different except for pulmonaryedema, which was more common in whites (P " 0.036). After adjust-ment for significant admission characteristics, 3-month outcome wasnot significantly different between the races.
CONCLUSION: Race was not found to be a prognostic factor foroutcome after aneurysmal SAH. The higher SAH mortality previouslyobserved in blacks is probably driven by a higher incidence of SAH inblacks. These findings highlight the importance of primary preventionprograms aimed at modifying risk factors for SAH.
ABSTRACTS OF OPEN PAPERS
476 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

772Two-year Follow-up on Patients in a Pilot Safetyand Efficacy Study of OP-1 (rhBMP-7) inPosterolateral Lumbar Fusion as a Replacement forIliac Crest AutograftDom Coric, M.D., Jeffrey S. Fischgrund, M.D.,Tushar Patel, M.D., Alexander R. Vaccaro, M.D.,Truumees Eeric, M.D., Harry N. Herkowitz, M.D.,Todd Albert, M.D., Alan Hilibrand, M.D.,Frank Phillips, M.D., Todd Wetzel, M.D.,John McCulloch, M.D.
INTRODUCTION: Posterolateral intertransverse lumbar fusion is acommonly performed procedure for stabilization of the degeneratedlumbar spine. A typical clinical scenario for which such fusions areused is the stabilization of a degenerative spondylolisthesis afterdecompression. In a recent large series reported in literature, this typeof fusion was noted to have a pseudarthrosis rate of up to 55%(Fischgrund, Spine 1997).
METHODS: Thirty-six patients with the diagnosis of symptomaticspinal stenosis and single-level degenerative spondylolisthesis in thelower lumbar spine (L3–S1) were enrolled. Patients were randomizedto either the OP-1 group or the control group. The OP-1 groupreceived 3.5 mg of OP-1 per side in a bone collagen putty carrier. Thecontrol group received iliac crest autograft alone. Outcomes weremeasured clinically using the Oswestry score and radiographicallyusing dynamic radiographs evaluated independently by a panel ofblinded radiologists using digital calipers. Patients were deemed aclinical success if they showed an approximately 20% improvement inOswestry score and were deemed a radiographic success if theyshowed bridging bone and spinal stability on flexion/extension films.
RESULTS: At 24 months, 16 of 17 evaluable patients (94%) in theOP-1 group and 6 of 10 evaluable patients (60%) in the autograftgroup were considered clinical successes, whereas 11 of 17 patients(65%) in the OP-1 group and 4 of 10 (40%) in the autograft group wereconsidered radiographic successes. No acute adverse events related tothe use of OP-1 were noted.
CONCLUSION: OP-1 seems to be a safe and effective replacementfor iliac crest autograft in human posterolateral lumbar fusion. Thedose, 3.5 mg per side, and the carrier, biodegradable, compression-resistant bone collagen putty, seem to provide a safe and effectivemeans of delivering the bone morphogenetic protein OP-1 to thehuman lumbar spine.
773A Prospective Randomized Study of MineralizedCollagen and Bone Marrow Aspirate versus IliacCrest Autograft for Instrumented PosterolateralLumbar FusionKitchel H. Scott, M.D.
INTRODUCTION: Harvesting iliac crest bone graft for posterolat-eral lumbar fusion is associated with high rates of postoperative graftsite pain and morbidity. Healos, an osteoconductive matrix, is abovine Type I collagen fibrous matrix, uniformly coated with hy-droxyapatite through a patented mineralization process. It has a mi-croporosity similar to that of human cancellous bone. The combina-tion of Healos and bone marrow aspirate (BMA) has yielded highrates of solid fusion in both animals and humans.
METHODS: After informed consent, 25 consecutive patients were
enrolled in the study comparing Healos/BMA to iliac crest autograftusing a same-patient control for instrumented posterolateral lumbarfusion at one level. Instrumented fusion was performed at L4–L5 in 16patients and at L5–S1 in 9 patients. Technique involved standardposterior decompression with pedicle screw instrumentation. Postero-lateral fusion was undertaken with Healos/BMA in one posterolateralgutter and iliac crest autograft on the contralateral side. Randomiza-tion was performed as right versus left for each patient. Solid fusionwas determined by two independent bone radiologists using a com-bination of lateral flexion-extension radiographs and reconstructedcomputed tomographic scans with a requirement of no motion at thetreated level and bridging bone from one transverse process to thenext. Clinical outcomes were measured with a visual analog scale forpain and the Oswestry Disability Index for function.
RESULTS: Minimum follow-up for all patients was 24 months. Inthese 25 patients, 20 (80%) of the Healos/BMA sides met the strictfusion criteria. Of the sides with autograft, 21 (84%) met this criteria.There was no statistically significant difference. Clinically, there was amean decrease in pain of 59.3% and a mean decrease in Oswestryscores of 57.1%.
CONCLUSION: Healos/BMA represents a viable alternative to theuse of autograft in a human instrumented posterolateral lumbar fu-sion model. Further trials to confirm these initial results are indicated.
774Adjacent-segment Disease after Anterior CervicalFusion: A Review of 70 Reoperated CasesHongyan Zou, M.D., Ph.D., Cecil Chang, M.D.,Hoang N. Le, M.D., Issada Thongtrangan, M.D.,John Park, M.D., Daniel H. Kim, M.D.
INTRODUCTION: Cervical spine motion segments adjacent to afused segment are prone to undergo accelerated degenerativechanges. However, published literature on additional anterior cervicalfusions for adjacent-segment disease is lacking. We reviewed ourexperiences with reoperated cases for symptomatic adjacent-segmentdegeneration after anterior cervical disectomy and fusion (ACDF).
METHODS: A retrospective study of 928 consecutive ACDF casesover the past 8 years showed that 70 were reoperations for symptom-atic adjacent-segment disease. Age ranged from 35 to 65 years. Thirty-six patients were female, and 34 were male. Segment levels, location,and time frame and symptoms were analyzed.
RESULTS: Of the index surgery, the most common level was single-level C5–C6 (29%), followed by C6–C7 (21%). Nineteen patients (27%)underwent a two-level fusion (7 had C4–C5 and C5–C6, 10 had C5–C6and C6–C7, and 2 had C6–C7 and C7–T1). Seven (10%) had a three-level fusion. Adjacent-level degeneration requiring additional fusionoccurred at C6–C7 (14 patients), C5–C6 (14 patients), C4–C5 (11 pa-tients), C3–C4 (9 patients), C7–T1 (3 patients), two-level (16 patients),and three-level (3 patients). Isolated superior segment, inferior seg-ment, superior and inferior segment, and remote degeneration oc-curred in 57%, 29%, 10%, and 4%, respectively. Nine cases showedjunctional instability evidenced by flexion/extension films. Timeframe from the index surgery to the reoperation ranged from 9months to 27 years (average, 6.75 yr) with a bimodal distribution, thefirst peak of less than 3 years (31%) and second peak of greater than10 years (19%).
CONCLUSION: Symptomatic adjacent-segment disease requiringadditional fusion involves the superior segments twice as commonlyas the inferior segments. Average time between the index ACDF and
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 477

the adjacent-segment additional fusion is 6.7 years, with a bimodaldistribution (less than 3 years and greater than 10 yr). Single-levelarthrodeses at C5–C6 and C6–C7 are the most common levels in-volved in the index surgery.
775Comparison of Self-reported Outcomes of Pediatricand Adult Patients with Phrenic Nerve StimulatorsStephen I. Ryu, M.D., Daniel H. Kim, M.D.,Ho-Yeol Zhang, M.D.
INTRODUCTION: Phrenic stimulation for quadriparesis and inother patients to alleviate chronic mechanical ventilation has beenperformed for several decades. Long-term patient-reported outcomesin the pediatric and adult populations have not been well reported.
METHODS: A total of 412 surveys, requesting data on demo-graphic factors, diagnoses, pacing statistics, functional status, qualityof life, and satisfaction, were mailed to all patients implanted with thelatest-generation commercially available pacing system from onemanufacturer.
RESULTS: Of these, 132 forms were received (32.2% response rate).Sixty-four pediatric (&18 yr) and 49 adult ($18 yr) patients wereidentified. Mean age at time of implantation was 7.8 % 5.7 years forthe pediatric group and 37.3 % 18.1 for the adult group. Duration ofimplantation was 10.4 % 8.5 for the pediatric group and 9.7 % 7.1 forthe adult group (P " 0.63). Main pediatric diagnoses were centralhypoventilation (58%) and quadriparesis (38%), unlike the adultgroup, whose main diagnoses were quadriparesis (57%) and dia-phragm paralysis (16%). Of all these patients, $80% are still pacing.Mean pacing time was significantly less for the pediatric group (12.6h/d) versus the adult group (17.0 h/d) (P ! 0.01). Of pediatricpatients, 11% paced continuously, as opposed to 45% of adults. Ofboth groups, 79% reported decreased ventilator dependence. Thirty-one percent of children were ventilator independent versus 42% ofadults. Before surgery, 28% of pediatric and 26% of adult patientswere institutionalized. This decreased to 5% and 9%, respectively.Speech, mobility, and quality of life (QOL) were significantly im-proved in both groups. QOL was statistically greater in the pediatricpopulation. Pediatric patients with congenital central hypoventilationsyndrome were most likely to report improvement. Nonquadripareticadults were least likely. Overall positive satisfaction was 98% forchildren versus 85% for adults (P ! 0.01).
CONCLUSION: Speech, mobility, and QOL are improved in themajority of patients with phrenic stimulators. Central hypoventilationpediatric patients report the most significant improvements. Quadri-paretic patients report significant improved ventilator independence.Overall satisfaction is very high in all groups.
776Marrow Stromal Cells Delivered via LumbarPuncture Home toward Spinal Cord Contusionand Cause RepairAjay Bakshi, M.D., Takahiko Mitsui, M.D., Ph.D.,Sharon Swanger, B.S., Michael Sabol, Jed Shumsky, Ph.D.,Itzhak Fischer, Ph.D.
INTRODUCTION: Cell transplantation techniques have shownpromise for improving outcomes after experimental spinal cord in-
jury, but most investigators have used direct parenchymal injection, amethod likely to be too invasive for human application. Here, wedescribe a novel technique for transplanting marrow stromal cells(MSCs) via a lumbar puncture (LP).
METHODS: MSCs were obtained from Fisher rats that have beentransgenically modified to express human placental alkaline phospha-tase (PLAP), making the cells easier to track after transplantation.Eighteen adult Sprague-Dawley rats received a moderate contusioninjury at the T9–T10 level, followed 1 week later by cell transplanta-tion via LP (2 million MSCs; n " 12) or no intervention (n " 6). Twogroups of transplanted animals (n " 3 each) were killed 1 or 2 weeksafter transplantation. All other animals received periodical behavioralanalysis (Basso, Beattie, and Bresnahan [BBB] score) for 6 weeks, andterminal cystometry was performed determine bladder function. His-tological analysis was performed using PLAP histochemistry andimmunofluorescence techniques. The extent of cell grafting into in-jury and size of the injury were determined using stereological tech-niques.
RESULTS: Transplanted MSCs were identified within the injuredspinal cords, and some cells persisted up to 6 weeks. Transplantedanimals had much smaller cysts (9% of the cord volume versus 22.7%in control groups; P ! 0.005) and significantly smaller contusions:22.2% in the transplanted group versus 34.2% in the control group; P! 0.01). BBB scores in both groups were similar, but cystometricanalysis revealed that the transplanted group has significantly lessdetrusor hypereflexia (DHR) (Control DHR " 4.2 and transplantedgroup DHR " 2.6; P ! 0.05) and a trend toward lower residual urinevolume.
CONCLUSION: We have demonstrated that MSCs transplantedvia LP migrate toward the contused spinal cord. Cells persist for aconsiderable period of time, interact with host tissues, and lead tosignificant histological and some behavioral recovery. This model oftransplantation is easily translatable to patients, making clinical trialssafer, easier, and more promising.
777Recurrent Laryngeal Nerve Injury with AnteriorCervical Spine Surgery: A Prospective, RandomizedStudy of Risk of Injury with Laterality of Side ofSurgical ApproachWilliam J. Beutler, M.D., Perri Brian, D.O.
INTRODUCTION: The anterior approach to the cervical spine isassociated with a risk of injury to the recurrent laryngeal nerve (RLN).Anatomic considerations have been used as justification for approachlaterality decisions. The purpose of the ongoing study is to determinewhether there is a greater risk of injury to the RLN on the basis of theside of surgical approach. There has never been a prospective study ofthe risk of RLN injury randomized to the side of surgical approach.
METHODS: All anterior cervical discectomy procedures completedby a single surgeon over a 3-year study period were included. Theside of surgical approach was determined soley by an approachcontralateral to the patient’s symptoms. A resident trained by otolar-yngology to evaluate RLN injury evaluated patients on the first post-operative day. Any hoarseness persisting at 2 weeks was evaluatedwith direct laryngoscopy by otorhinolaryngology.
RESULTS: There were 202 patients studied prospectively. Therewere 128 single-level, 67 two-level, and 7 three-level procedures.There were 94 procedures completed from the right and 108 proce-
ABSTRACTS OF OPEN PAPERS
478 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

dures completed from the left. There were 2 patients with RLNinjuries detected, representing a 1% incidence of RLN injury. Onepatient had an approach from the left at C6–C7. The other patient hadan approach from the right at C5–C6. This patient had resolution ofher symptoms at the 2-month follow-up. There was a 0.5% incidenceof permanent RLN injury.
CONCLUSION: In a prospective, randomized clinical study, therewas no relationship between the side of approach to the anteriorcervical spine and the incidence of RLN palsy. There was also nosignificant difference in the procedure level or number of levels andthe incidence of RLN injury. These findings suggest that anatomicdifferences between the right and left RLN do not justify a specificside for surgical approach to the anterior cervical spine.
778Phase 1 Trial of Oscillating Electrical FieldStimulation in Human Complete Spinal Cord InjuryScott A. Shapiro, M.D., Richard Borgens, Ph.D.,Robert Pascuzzi, M.D., Michael Groff, M.D.,Thomas Altstadt, M.D., Paul Nelson, M.D.,Ben Rodgers, M.D.
INTRODUCTION: An electrical field cathode has trophic/tropiceffects on injured spinal cord axons in vitro and in vivo in lamprey,rodent, and canine spinal cord injury and improves functional out-come. A human oscillating field stimulator (OFS) was built, and Foodand Drug Administration permission was given to study 10 humanswith complete spinal cord injury.
METHODS: Entry criteria were complete spinal cord injury be-tween C5 and T10 with no transection on magnetic resonance imag-ing. All must receive National Acute Spinal Cord Injury Study (NAS-CIS) therapy, 3-methylprednisolone. Cord compression and spinalinstability must be treated before entry. All must remain complete(American Spinal Injury Association [ASIA] scoring) with no somato-sensory evoked potentials (SSEPs) below the injury after surgery or 48hours. Age was between 18 and 65 years. All must be implantedwithin 18 days of injury. The OFS is explanted at 15 weeks. Patientswere checked every 2 weeks until explant. Independent neurologicalexamination (ASIA scoring and SSEP) was conducted at 6 weeks, 6months, and 1 year.
RESULTS: There were no complications on insertion and 1 woundinfection at explant. One patient was lost to follow-up after 6 months.All 10 had a mean visual analogue pain score of 8 at implantation and2 at 6 months and 1 year. Mean improvement in light touch at 1 yearwas 25.5 points (4–92; P ! 0.001, analysis of variance [ANOVA]).Mean improvement in pinprick at 1 year was 20.4 points (2–93; P !0.001, ANOVA). Mean improvement in motor recovery at 1 year was6.3 points (0–12; P ! 0.01, ANOVA). Two thoracic cord injuriesrecovered 2/5 iliopsoas and toe extension/flexion of 1/5. Of fivecervical cord injuries, four recovered upper-extremity SSEPs and onerecovered abnormal lower-extremity SSEPs. Of five thoracic injuries,one recovered incomplete leg SSEPs at 1 year.
CONCLUSION: OFS treatment for human complete spinal cordinjury is safe, reliable, and easy. NASCIS III-compliant plegic patientsrecovered a mean of 0.6 pinprick, 0.5 light touch, and 3 to 6 motor. Ourresults suggest efficacy, and the Food and Drug Administration hasgiven permission for 10 more patients.
779One-stage Surgery (Anterior and Posterior) forCraniovertebral Junction Anomalies: LessonsLearned from 632 CasesShashank S. Kale, M.Ch., Sarat P. Chandra, M.Ch.,Ashish K. Suri, M.Ch., Veer S. Mehta, M.Ch.
INTRODUCTION: Craniovertebral junction anomalies are a majorpart of the referred complex spine cases at AIIMS, a leading tertiaryreferral center in South Asia. Their management in a developingcountry is discussed with special reference to single-sitting surgery.
METHODS: The charts of 632 patients of craniovertebral (CV)junction anomalies managed between 1992 and 2003 were reviewedand the data analyzed statistically. Men composed 504 of 632 patients.Developmental anomalies were most common in 472 of 632, followedby traumatic, inflammatory, and neoplastic. Patients with only syrin-gomyelia and/or Chiari malformation, without bony anomaly, wereexcluded from this study. Pyramidal tract signs and symptoms werethe most common. Irreducible atlantoaxial dislocation with or withoutbasilar invagination was the most frequently occurring bony anomaly:540 of 632. Four hundred ninety-nine patients underwent transoralodontoid excision, and 489 underwent posterior fixations: O-C2C3contoured loop fixation (contoured loop made from Steinmann pin atsurgery), titanium plate and screw, or cable fixation. Other operationsincluded Magerl’s, Brooks’, Gallie’s, and anterior plating of C2–C3.Two hundred twenty patients underwent both procedures in a singlesitting.
RESULTS: Postoperatively, 416 patients improved, 136 were un-changed, and 51 worsened. Thirty-five patients had wound infectionand 15 cerebrospinal fluid leak. Three patients had failure of construct(2 Gallie’s wire breakage and 1 loop). Twenty-nine patients died, 8 ofcardiac causes, 8 chest infection, 2 meningitis, 6 septicemia, 1 second-ary hemmorhage from the oral wound, and 2 posterior circulationinfarctions after fixation. Two-year follow-up data are available for252 patients, with improvement in 76%. Patients operated on in asingle stage (versus 2 stages) had a shorter hospital stay (7.1 versus 13days), low infection rate (9% versus 26%), and lower mortality (3%versus 11%).
CONCLUSION: Developmental CV junction anomalies are themost common. Single-stage surgery means a shorter stay, lower in-fection, and lower mortality. Contoured loop fixation using a Stein-mann pin and stainless steel wire gives a stable and economicalposterior fixation.
780Deep Brain Stimulation for Generalized Dystoniaand Spasmodic TorticollisRichard G. Bittar, Ph.D., F.R.A.C.S., John Yianni, M.D.,ShouYang Wang, Ph.D., Xuguang Liu, M.D., Ph.D.,Dipankar Nandi, Ph.D., M.B.B.S., Carole Joint, R.N.,Richard Scott, Ph.D., Peter Bain, M.D., Ralph Gregory, M.D.,John Stein, Ph.D., Tipu Z. Aziz, M.D., D.M.Sc.
INTRODUCTION: Dystonia seems to be distinct from the othertremulous disorders in that improvement after deep brain stimulation(DBS) frequently appears in a delayed and progressive manner. Therate of this improvement and the point at which no further progresscan be expected are currently unknown.
METHODS: We studied 12 consecutive patients with generalizeddystonia (n " 6) and spasmodic torticollis (n " 6) who underwent
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 479

bilateral globus pallidus internus (GPi) DBS. Standard rating scales wereused to quantify their neurological improvement. The results were ana-lyzed by applying the Wilcoxon signed-rank test to compare rating scaleswithin each group (preoperatively and at the most recent follow-up visit).In addition, a univariate analysis was performed for each subgroup toevaluate the rate of change in patient rating scales over time.
RESULTS: Both groups experienced a statistically significant improve-ment in their rating scores at both 1 and 2 years after surgery. Meanfollow-up was 29.9 months (range, 24–48 months). At 2-year follow-up,the spasmodic torticollis group exhibited a 59% improvement in theirtotal Toronto Western Spasmodic Torticollis Rating Scale rating score,and the generalized dystonia group attained a 46% improvement in theiroverall Burke-Fahn-Marsden Dystonia Rating Scale evaluation. The totalneurological rating scores for each group of patients improved graduallybefore reaching a plateau. Ninety-five percent of the final improvementwas attained by 6.4 months in the generalized dystonia group and by 6.6months in those with spasmodic torticollis. There was no significantimprovement at 1 year after surgery. Postoperative complications oc-curred in three patients and comprised electrode displacement, leadfracture, and status dystonicus.
CONCLUSION: These findings add further support to GPi DBS asan effective treatment for generalized dystonia and spasmodic torti-collis and furnish important information as to the expected rate andmagnitude of improvement and the point at which no further gainscan be reasonably anticipated.
781Bilateral Intraputaminal Infusion of Liatermin(Glial Cell Line-derived NeurotrophicFactor r-metHuGDNF) in Subjects withAdvanced Parkinson’s DiseaseSteven Gill, F.R.C.S., Peter Heywood, F.R.C.P.,Andres M. Lozano, M.D., Ph.D.,Anthony Lang, Elena Moro, M.D., Richard Penn,Arif Dalvi, M.D., Kim J. Burchiel, M.D., John Nutt, M.D.,Patrick Kelly, M.D., Michael Hutchinson, M.D.,W.J. Elias, M.D., Frederic Wooten, M.D.,Dennis Turner, M.D., Burton Scott, M.D.,Nikunj Patel, F.R.C.S., Edward R. Laws, Jr., M.D.,James Matcham, Ph.D., Robert Coffey, M.D.,Michael Traub, M.D.
INTRODUCTION: Liatermin consistently has demonstrated neuro-protective and neuroregenerative properties in rodent and nonhumanprimate models of Parkinson’s disease (PD). A previous trial of intrace-rebroventricular infusions of glial cell line-derived neurotrophic factor(GDNF) did not yield the expected improvements noted in the animalmodels. However, direct targeted delivery of GDNF has resulted inmarked clinical improvement in open-label pilot trials of continuousintraputaminal (IPu) infusion of liatermin in patients with advanced PD.
METHODS: This was a multicenter, randomized, double-blind,placebo-controlled, parallel-group study that evaluated safety andefficacy in 34 subjects with advanced idiopathic PD. The SynchroMedInfusion System (Medtronic, Inc., Minneapolis, MN) was used toadminister liatermin (15 mg/putamen/d) or placebo bilaterally intothe dorsal posterior putamen via stereotactically implanted bilateralIPu catheters. A blinded neuroradiologist independently evaluatedcatheter tip placement and the delivery of study material on magneticresonance images. Other blinded individuals evaluated before- andafter-treatment 18F-dopa positron emission tomographic (PET) scans.
Subjects continued to receive oral anti-parkinsonian medications. Theprimary outcome was the percent change from baseline to 6 months inthe Unified Parkinson’s Disease Rating Scale (UPDRS) motor score inthe practically defined off condition.
RESULTS: Thirty-four subjects received implants and were ran-domized into the trial. The most serious implant-related adverseevents included one symptomatic intraparenchymal hemorrhage, onesubdural hygroma, and one recurrent infection that required deviceremoval and reimplantation. No deaths or permanent neurologicalworsening occurred. Because the blinded phase continues throughMay 2004, complete unblinded safety and efficacy results will berevealed during the presentation of the data at the meeting. Efficacyresults include the percent change in the UPDRS motor score in thepractically defined off period and the findings of the pretreatment andposttreatment 18F-dopa PET studies.
CONCLUSION: Continuous infusion of liatermin into the dorsalposterior putamen is well tolerated and may result in improvement(to be clarified once results are available) of parkinsonian motorsymptoms in patients with advanced PD.
782Targeted Subthreshold Cortical Stimulationfor Recovery of Motor Hand Function afterHemiparetic StrokeRobert M. Levy, M.D., Ph.D., Martin Weinand, M.D.,Sean Ruland, M.D., David Lowry, M.D., Rima Dafer, M.D.
INTRODUCTION: A prospective, randomized, multicenter feasi-bility study tested the hypotheses that targeted subthreshold corticalstimulation is safe and effective for motor hand function recoveryafter hemiparetic stroke.
METHODS: Twenty-four patients with cortical and/or subcorticalstroke with hemiparesis are undergoing functional magnetic resonanceimaging and either 6 weeks of 1) rehabilitation plus epidural motor handarea cortical stimulation (pulse frequency " 100 Hz, pulse duration " 250microsec, treatment current " 5.0 % 1.2 mA) during rehabilitation (n "12) or 2) the same rehabilitation protocol alone (n " 12) with a 12-weekfollow-up period. The following outcome measures are obtained duringbaseline, treatment, and follow-up: Arm Motor Fugl-Meyer (AMFM),Strength subscore of the Stroke Impact Scale (SIS), Emotion subscore ofthe SIS, SIS Physical Domain, Hand Grip Strength, and NIH Stroke Scale.Statistical analysis is performed on all data with analysis of variance, withsignificance defined by P ! 0.05.
RESULTS: A total of 16 men and 8 women, ages 26 to 80 years(mean % standard deviation, 56 % 12 yr) enrolled in and completed thestudy. There was no mortality or neurological deterioration; one patienthad an acute postoperative seizure unrelated to the device or treatment.At the time of abstract submission, 17 patients (7 in the investigationaltreatment group, 10 in the control group) had completed the treatmentprotocol. Patients receiving cortical stimulation plus rehabilitation im-prove in hand/arm function to a greater degree than patients receivingrehabilitation alone. The AMFM scores, by intention-to-treat analysis,demonstrated a 7.8-point improvement for treatment patients versus3.7-point improvement for control patients (maximum of 66 points). A3-point improvement is considered clinically meaningful. Statistical anal-ysis will be performed upon study conclusion.
CONCLUSION: These preliminary results suggest safety and effi-cacy of subthreshold epidural cortical stimulation for recovery ofmotor arm/hand function during rehabilitation after hemipareticstroke. Further research is needed to validate the therapeutic effect.
ABSTRACTS OF OPEN PAPERS
480 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

783Safety of Cortical Stimulation in Patients withHemiparetic StrokeJeffrey A. Brown, M.D., Helmi Letsup, M.D.,Martin Weinand, M.D., Steve Cramer, M.D.
INTRODUCTION: This is a prospective, multicenter safety andeffectiveness study of the treatment of patients with hand/arm motordeficit resulting from a stroke at least 4 months before enrollment withtargeted subthreshold cortical stimulation delivered concurrentlywith rehabilitation.
METHODS: Fourteen patients were enrolled. Ten patients wererandomized to either an investigational group who underwent crani-otomy for implantation of an epidural electrode array designed todeliver cortical stimulation concurrent with each rehabilitation sessionor to a control group who received similar rehabilitation activitiesonly. The electrode array was positioned in the hand/wrist motorcortical region as determined by functional magnetic resonance im-aging (fMRI images), then projected to a neuronavigational systemused to design the craniotomy. All subjects underwent a 16-weekprotocol that included baseline and weekly evaluations, fMRI, crani-otomy for electrode placement (if randomized), and therapy. Safetywas evaluated using predetermined criteria of function, seizure oc-currence, and other medical complications. Efficacy was evaluatedweekly for 16 weeks by 10 scales focusing on hand strength andfunction.
RESULTS: Safety criteria were met at 1- and 12-week follow-up. Nopatients treated according to the investigational plan experiencedmedical complications. Two infections occurred, one from a surgicalprotocol violation. In the investigational group, statistically significantimprovements in hand/arm function were identified in the ArmMotor Fugl-Meyer score (P ! 0.0001), Strength subscore of the StrokeImpact Scale (SIS), Emotion subscore of the SIS (P " 0.0002), the SISPhysical Domain (P " 0.0007), the NIH Stroke Scale (P " 0.0003), andHand Grip Strength (P " 0.0005). Repeated-measurement analysisusing piecewise linear fits of the two groups showed that the activetreatment group improved at a significantly higher rate and to agreater degree on the Arm Motor Fugl-Meyer score than controls (P "0.008).
CONCLUSION: Cortical stimulation during 3 weeks of rehabilita-tion in stroke patients is safe at 12-week follow-up. Preliminary effi-cacy evaluation indicates that stimulation improves hand/arm func-tion.
784The Long-term Response of Primary GeneralizedTorsion Dystonia to Bilateral Pallidal DeepBrain StimulationRon L. Alterman, M.D., Jay Shils, Ph.D.,Michele Tagliati, M.D., Joan Miravite, A.R.N.P.,Susan Bressman, M.D.
INTRODUCTION: Preliminary studies of bilateral deep brain stim-ulation (DBS) at the globus pallidus pars internus (GPi) for primarygeneralized torsion dystonia have yielded promising results; how-ever, few data exist about the long-term efficacy of this therapy.
METHODS: This was a retrospective analysis of 10 consecutivepatients (5 women, 5 men; age range, 13–63 yr) with medically intrac-table primary dystonia who underwent microelectrode-guided bilat-eral GPi DBS surgery at our center. Six patients tested positive for the
DYT1 gene defect. All patients were videotaped and evaluated withthe Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS) before andat regular intervals after surgery. DBS settings were slowly and sys-tematically increased to achieve the best clinical effect. All patientswere followed up for at least 6 months.
RESULTS: Each of the patients’ BFMDRS scores were improvedpostoperatively. The mean improvement was 47% at 3 months (n "10), 60% at 6 months (n " 10), 67.5% at 12 months (n " 8), 72.5% at 2years (n " 6), and 67.5% at 3 years (n " 4). The differences between thebaseline and follow-up scores were statistically significant at all timepoints except the 3-year follow-up (P ! 0.05, paired Student’s t test).There was no difference in the percent improvement 6 months post-operatively in the DYT1# versus DYT1& groups (63.2% versus 68.5%,respectively). Complications were limited to two extension wire frac-tures and one superficial infection, which necessitated device explan-tation.
CONCLUSION: We confirm that pallidal DBS is a safe and effectivetherapy in select patients with medically intractable primary torsiondystonia. Clinical improvement is progressive over 1 year. Positiveresponses are maintained for at least 2 to 3 years. The presence of theDYT1 gene defect does not affect clinical response in patients withidiopathic primary dystonia.
785The Speed at Which Reach Movement Plans Can BeDecoded from the Cortex and Its Implications forHigh-performance Neural Prosthetic Arm SystemsStephen I. Ryu, M.D., Gopal Santhanam, M.S.,Byron Yu, M.S., Krishna V. Shenoy, Ph.D.
INTRODUCTION: It will be possible to decode cortical motorsignals to enable a robotic arm to accurately and quickly assist spinalcord-injured patients. Understanding how quickly the brain plansreaches is important to understand the performance limit of such asystem.
METHODS: We trained a rhesus monkey to touch a center point ona video screen and to hold for 200 to 1000 ms while one of eight targetsarranged around a circle on a touch screen was shown. After a cue, hethen performed reaches out to the target. We microsurgically im-planted a 96-channel electrode array into the premotor and motorcortex of the monkey. Directional tuning curves were learned from 20to 30 repeated reaches to each target using simultaneously recordedsingle (40) and multiple (100) neuron spike rates. We then computa-tionally predicted the upcoming reach from 200 ms of neural activitystarting 150 ms after the target was shown. An icon was then renderedat the location of the predicted target before the monkey actuallyexecuted a real reach. Real and icon trials were interleaved so that themonkey would occasionally have to make real reaches.
RESULTS: Using just 200 ms of neural activity, the correct targetlocation (one of eight) could be predicted using a maximum-likelihood estimator on greater than 90% of trials. When wrong, thepredicted target was typically just next to the actual target. Predictioncomputation required less than 20 ms. Up to 10 targets in a row werepredicted from neural planning activity alone with no real reachesperformed. Up to three reach plans could be decoded in under 1second.
CONCLUSION: The cortex is able to generate discriminable plansto one of eight discrete targets in only 200 ms. Our prosthetic decoderis capable of decoding and generating a prosthetic reach faster thanreal reach capabilities.
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 481

786Targeting of the Subthalamic Area Is Superiorto the Ventrolateral Thalamus for Severe IntentionTremor, and Asymmetric Stimulation Can PreventSide EffectsWolfgang Hamel, M.D., Jan Herzog, M.D.,Roland Wenzelburger, M.D., Monika Poetter, M.D.,Frank Steigerwald, M.D., Florian Kopper, M.D.,Ulrich Stiller, M.D., Markus Pinsker, M.D.,Andre Morsnowski, Ph.D., Jens Volkmann, M.D.,Gunther Deuschl, M.D., Dieter Muller, M.D.,H. Maximilian Mehdorn, M.D.
INTRODUCTION: Although deep brain stimulation (DBS) in theventrolateral thalamus is an effective treatment for severe intentiontremor, the optimal site for stimulation is the subject of ongoingdebate.
METHODS: DBS electrodes were implanted into one of five tracksexplored by microrecording and microstimulation in seven patientswith essential tremor and six patients with multiple sclerosis. Stereo-tactic coordinates of each electrode contact were determined fromstereotactic x-rays, and the efficacy of each contact was assessed.
RESULTS: Contacts located ventral to the intercommissural planereduced lateralized Fahn scores by 63.6 % 21.1% (right) and 67.9 %18.3% (left), whereas dorsal contacts were less effective (20.5 % 16.4%and 17.6 % 16.2%, respectively). Similarly, only stimulation below theintercommissural plane resulted in pronounced reduction of intentiontremor assessed by magnetic tracking of grasping movements as wellas accelerometer total power measuring high-amplitude batwingtremor. The mean coordinates of the most effective contacts (right:12.9 % 1.6, &7.4 % 1.0, &1.6 % 1.3; left: &12.3 % 1.2, &7.3 % 1.7, &2.6 %1.1; x, y, z in mm relative to the midcommissural point) suggestedstimulation within the subthalamic area, which is corroborated bypost hoc correlation with intraoperative microrecordings. Chronaxievalues for suppression of tremor (27 % 14 #s) and induction of ataxia(52 % 15 #s; P ! 0.05) suggested that tremor suppression is caused bymodulation of large myelinated fibers. Notably, optimal contactscould not be used for permanent, bilateral stimulation in severalinstances, because this was associated with side effects, e.g., paresthe-sias or dysarthria. Whereas the optimal contact was generally chosenfor the dominant side (left electrode), contralateral stimulation wasperformed with less effective contacts located more dorsally.
CONCLUSION: For intention tremor, fiber tracks in the subtha-lamic area (zona incerta, prelemniscal radiation/cerebellothalamicprojections, Forel H2) rather than neuronal cell bodies within theventrolateral thalamus represent an effective target for DBS. Perma-nent, bilateral stimulation is frequently performed asymmetrically toprevent side effects.
787Electrode Location Does Not Predict ContralateralLimb Motor Function Improvement in SubthalamicStimulation for Parkinson’s DiseaseShearwood McClelland III, B.A., Blair Ford, M.D.,Patrick B. Senatus, M.D., Ph.D., Steven J. Frucht, M.D.,Linda M. Winfield, R.N., Yunling E. Du, Ph.D.,Seth L. Pullman, M.D., Qiping Yu, Ph.D.,Guy M. McKhann, M.D., Robert R. Goodman, M.D., Ph.D.
INTRODUCTION: Deep brain stimulation (DBS) of the subtha-lamic nucleus (STN) is an effective treatment for patients with medi-
cally refractory Parkinson’s disease (PD). The degree to which DBSelectrode tip anatomic location determines the improvement of con-tralateral limb movement function has not been defined. This retro-spective study was performed to address this issue.
METHODS: Forty-two DBS electrode tips in 21 bilaterally im-planted patients were localized on postoperative magnetic resonanceimaging (MRI). The postoperative and preoperative planning MRIscans were merged with the Stealth stereotactic planning workstationto determine the DBS tip coordinates. Stimulation settings were opti-mized postoperatively for maximal clinical effect. Patients were vid-eotaped 1 year after surgery and assessed by a movement disorderneurologist blinded to electrode tip locations. The nine limb-relatedcomponents of the Unified PD Rating Scale (UPDRS) Part III (resttremor [hand, foot], action tremor, rigidity [upper, lower extremity],finger tapping, hand gripping, hand pronation/supination, leg agil-ity) were tabulated to obtain a limb score ([off-stimulation, off-medications] minus [on-stimulation, off-medications]). The electrodetip locations associated with the 15 least and 15 greatest limb responsescores were compared with postoperative limb function.
RESULTS: Statistical analysis (two-tailed t test) revealed no signif-icant difference in electrode tip location between the two groups withregard to three-dimensional distance (P " 0.759), lateral-medial (X)axis distance (P " 0.983), anteroposterior (Y) axis distance (P " 0.949),or superoinferior (Z) axis distance (P " 0.894) from the intendedanatomic target. The range of difference in tip location (X axis, 2.5 mmlateral to 5.1 mm medial; Y axis, 4.1 mm posterior to 2 mm anterior)and limb scores (&2.5 to #22.5) was extensive.
CONCLUSION: Within the range of electrode tip locations (relativeto the intended target) in this study, the postoperative MRI-determined electrode position does not predict the improvement ofcontralateral limb motor parkinsonism. Other factors may have agreater bearing on the limb responsiveness of these patients.
788Investigation of Gravity-induced Brain Shift Basedon a Three-dimensional Finite-element Model of theHuman BrainJong Beom Lee, Ph.D., Jingwen Hu, M.S.,Liying Zhang, Ph.D., King H. Yang, Ph.D.,Albert I. King, Ph.D., Lucia Zamorano, M.D.
INTRODUCTION: Brain shift, defined as the deformation of thebrain during surgery, can invalidate preoperative image data. Al-though an intraoperative magnetic resonance imaging system can beused to ascertain the amount of brain shift, such a system is veryexpensive and not useful when conducting presurgical planning. As aresult, numerical models capable of predicting brain shift is a goodsupplemental tool for computer-assisted surgery systems. The aim ofthis study was to predict gravity-induced brain shift using a three-dimensional (3-D) finite-element (FE) model of the human brain.
METHODS: A 3-D FE model of the human brain developed atWayne State University was used. The model includes a detaileddescription of the dura, pia, falx, tentorium, ventricles, cerebrum (grayand white matter), cerebellum, and brainstem. A commercially avail-able implicit FE code LS-NIKE3D and a postprocessing programLS-POST (version 970, LSTC, Livermore, CA) were used for analysis.
RESULTS: Two head positions, a supine and 60 axial rotationpositions were simulated, and a completely void cerebral spinal fluidspace between the dura and pia mater were assumed before theapplication of gravitational force. The maximum brain shift predicted
ABSTRACTS OF OPEN PAPERS
482 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

by the model for a supine and 60 axial rotation positions was 8.64 and6.95 mm located at the anterior and right anterior region of the frontallobe. The model predicted the largest brain shift at the highest point inthe direction of gravity. Maximum model-predicted brain shifts werein the same range as experimental results reported in the literature.
CONCLUSION: A 3-D FE model of the human brain has beendeveloped to predict the brain deformation caused by gravity afterdura opening. We believe that this study represents the first attemptto simulate complex features of the human brain without the need forsurface deformation data to calculate the extent of brain shift.
789Incorporation of Bone Marrow-derived Flk-1-expressing CD34" Cells in the Endothelium ofTumor Vessels in Mouse BrainJustin G. Santarelli, B.A., Vikram M. Udani, B.A.,Samuel Cheshier, M.D., Ph.D., Stephen Huhn, M.D.,Victor Tse, M.D., Ph.D.
INTRODUCTION: Mounting evidence suggests that hemangio-blasts are recruited from reservoirs within the bone marrow and mayplay a significant part in brain tumor angiogenesis. Once havingentered the peripheral blood, bone marrow-derived (BM) cells mayhome to the tumor vasculature to support remodeling. We haveidentified a subpopulation of BM cells thought to be in part respon-sible for vessel restructuring in the presence of brain tumor.
METHODS: Cells of a cultured glioma line were implanted into thestriatum of GFP(&) mice that had been lethally irradiated and rescuedwith GFP(#) BM cells. The animals were killed at specified timepoints after tumor implantation (3, 6, 9, and 12 days), and their brainswere sectioned and stained for CD34 (an early vascular marker), Flk-1(a receptor for vascular endothelial growth factor), and CD45 (a he-matopoietic marker). Analysis was performed using a Leica confocalmicroscope and Adobe Photoshop and Improvision Volocity soft-ware.
RESULTS: We have identified a population of bone marrow-derived cells that express both CD34 and Flk-1. The proportion ofendothelial cells positive for GFP, CD34, and Flk-1 out of total endo-thelial cells increased over the time course, from 0.8 % 0.3% at day 3after tumor implantation to 4.2 % 1.2% at day 12. Most GFP# endo-thelial cells were found to coexpress CD45.
CONCLUSION: Growing brain tumor incorporates BM cells intoits neovasculature. A small but important percentage of GFP# cells inthe tumor region assumed endothelial morphology and expressedboth CD34 and Flk-1, suggesting that they had incorporated into thevascular wall, where they may facilitate growth and expansion.
790Identification of HypermethylatedTumor-specific Deoxyribonucleic Acid in Plasmaof Patients with GliomaKyle D. Weaver, M.D., Stuart A. Grossman, M.D.,James G. Herman, M.D.
INTRODUCTION: Although patients without malignancy have!100 ng/ml free deoxyribonucleic acid (DNA) in plasma, patientswith malignancy demonstrate substantial quantities of tumor-specificDNA in their plasma. Measurements of this DNA are being studied to
develop plasma markers to correlate with tumor burden. This ap-proach has not been explored in gliomas.
METHODS: Venous blood (30 ml) was collected before craniotomyfrom 10 patients with presumed glioma. After surgery, DNA wasextracted and quantified from intracranial tumor and plasma samples.The methylation status of p16, p73, RAR, and MGMT genepromoters was assayed with methylation-specific polymerase chainreaction (MSP). The presence of tumor-specific DNA in the plasmawas defined as identification of the same methylated promoter (MP)in both plasma and tumor.
RESULTS: Pathological diagnoses were glioblastoma (n " 6), ana-plastic astrocytoma (n " 2), anaplastic oligoastrocytoma (n " 1), andoligodendroglioma (n " 1). Total DNA concentration in plasma wasgrossly elevated (mean, 6503 ng/ml; standard error of the mean, 1400ng/ml). Tumor specimens revealed methylation of at least one pro-moter in 9 of 10 patients (90%). Of the 9 patients with MP, 6 (67%) hadmethylation of at least one of the same promoters in the plasma DNA.Five of these had one MP identified in the plasma, and 1 had two MPs.Overall, glioma-specific methylated DNA was present in plasma of 6of 10 patients (60%). Tumors with no plasma MP were two glioblas-toma, one anaplastic astrocytoma, and one oligodendroglioma. Nopositive markers were found in the plasma that were not also foundin the intracranial tumor.
CONCLUSION: Gliomas shed large amounts of DNA into theblood. Using MSP, we found that tumor-specific DNA is present inplasma of glioma patients. This specific as promoter methylation isnot found in normal tissue. Isolation of tumor-specific plasma DNA inthese patients represents the first step to developing a quantitativeglioma plasma biomarker that could be used to monitor tumor status.
791Extent of Brain Tumor Resection Using High-field(1.5-T) versus Low-field (0.2-T) IntraoperativeMagnetic Resonance ImagingMarvin Bergsneider, M.D., Nouzhan Sehati, M.D.,Pablo Villablanca, M.D., David McArthur, Ph.D.,Linda M. Liau, M.D., Ph.D.
INTRODUCTION: Intraoperative magnetic resonance imaging(iMRI) has been advocated as a useful tool for maximizing the extentand safety of brain tumor resections. In this study, we performed aprospective trial with retrospective case-control to compare the extentof glioma resection using high-field-strength iMRI, low-field iMRI,and conventional neurosurgery without iMRI.
METHODS: Forty-five patients with supratentorial gliomas wereentered into this study and divided into four groups: conventionalopen resection (OR) with standard frameless neuronavigation (n "12), 0.2-T low-field-strength iMRI without neuronavigation (n " 13),1.5-T high-field iMRI without neuronavigational reregistration (n "12), and 1.5-T high-field iMRI plus updated intraoperative reregistra-tion of neuronavigation (n " 8). Extent of surgical resection wasevaluated using three-dimensional volumetric analyses of MRI scans.The duration of surgical intervention and morbidity were also evalu-ated.
RESULTS: The mean percentage of tumor resection using the con-ventional OR was 78.6% % 13.8%, which was significantly worse (P "0.05) than that using the 1.5-T iMRI (88.2% % 14.3) or 0.2-T iMRI(91.4 % 6.7%). There was no statistical difference in the extent of tumorresection using the low-field 0.2-T versus high-field 1.5-T iMRI (91.4versus 88.2%, P " 0.32). However, when neuronavigation with up-
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 483

dated intraoperative reregistration was added in conjunction withiMRI, the percentage of tumor resected was significantly increased to98.5% % 1.9 (P " 0.03). Residual postoperative tumor volumes weresignificantly lower in the iMRI groups (12.5 % 14 cm3 for gliomasresected in the conventional OR, compared with 4.2 % 3.8 cm3 using0.2 iMRI (P " 0.05), 7.0 % 9.2 cm3 using 1.5-T iMRI (P " 0.07), and1.0 % 1.3 cm3 using 1.5-T iMRI with updated intraoperative neu-ronavigation (P " 0.03).
CONCLUSION: The results indicate that iMRI can enhance theextent of tumor resection for gliomas, although there was no differ-ence between the use of low-field versus high-field iMRI. However,the combination of high-field iMRI with intraoperative updated neu-ronavigation significantly improved the extent of tumor resectionbeyond that attainable by iMRI alone.
792Unique Periventricular Niche in Adult Human BrainContains Astrocytic Stem Cells but No Evidence ofChain MigrationNader Sanai, M.D., Anthony D. Tramontin, Ph.D.,Alfredo Quinones-Hinojosa, M.D.,Nicholas M. Barbaro, M.D., Nalin Gupta, M.D., Ph.D.,Sandeep Kunwar, M.D., Michael T. Lawton, M.D.,Michael W. McDermott, M.D., Andrew T. Parsa, M.D., Ph.D.,Jose Manuel-Garcia Verdugo, Ph.D., Mitchel S. Berger, M.D.,Arturo Alvarez-Buylla, Ph.D.
INTRODUCTION: The subventricular zone (SVZ) is a principalsource of adult neural stem cells in the rodent brain, generatingthousands of olfactory bulb (OB) neurons every day. If the adulthuman brain contains a comparable germinal region, this could havesignificant implications for future neuroregenerative therapy.
METHODS: Stem cells have been isolated from the human brain,but the identity, organization, and function of adult neural stem cellsin the human SVZ are unknown. Using gene reporting and cell culturetechniques, immunohistochemistry, and electron microscopy, wecharacterized this stem cell niche in adult human SVZ specimens from65 neurosurgical resections and 45 autopsied brains.
RESULTS: Here, we describe a ribbon of SVZ astrocytes lining thelateral ventricles of the adult human brain that proliferate in vivo andbehave as multipotent progenitor cells in vitro. This astrocytic ribbonhas not been observed in other studied vertebrates. Surprisingly, wefound no evidence of chains of migrating neuroblasts in the SVZ or inthe pathway to the OB.
CONCLUSION: This work identifies SVZ astrocytes as neural stemcells in a niche of unique organization in the adult human brain. Theidentification of a large, anatomically discrete population of prolifer-ating, multipotent human astrocytes may also lead to a better under-standing of the role human neural stem cells play in tumorigenesis,demyelination, and neurodegeneration.
793Cranial Base Chordomas and Chondrosarcomas:A 12-year Review of 158 Patients Treated withFractionated Proton Beam TherapyWalter D. Johnson, M.D., Lilia Loredo, M.D.,Roger I. Grove, M.S., Jerry D. Slater, M.D.
INTRODUCTION: A total of 158 patients treated over a 12-yearperiod with cranial base chordomas or chondrosarcomas were re-
viewed to assess treatment efficacy after fractionated proton beamradiation therapy (PRT).
METHODS: A total of 158 patients with cranial base tumors,treated from March 1992 until November 2003, were reviewed retro-spectively using a combination of chart review and interviews, includ-ing details of survival, current clinical condition, and recent imagingstudies.
RESULTS: Of these tumors, 110 were chordomas (65 men and 45women) and 48 were chondrosarcomas (24 men and 24 women).Average age for chordoma was 39.1 years in women, 43.6 years inmen; for chondrosarcoma, 41.8 years in women, 46.3 years in men.Gross tumor volume target dosages ranged from 36 to 79.2 (mean,71.2) cobalt gray equivalents. The range of follow-up was 2 to 139months (mean, 39.1 mo). Local control rates were 74% for chordomasand 85% for chondrosarcomas. Five-year overall survival rates were78.2 and 85.4% for chordomas and chondrosarcomas, respectively.Additional analyses were performed regarding treatment failures, sexdifferences, patient age at diagnosis, tumor size at PRT, the extent ofbrainstem involvement, and presence or absence of distant metasta-ses. Those with residual tumor volumes of 25 ml or less seemed tomaintain better local control; those involving brainstem had pooroverall survivals. Female patients under the age of 16 with diagnosisof chordoma had the worst overall survival.
CONCLUSION: Chordomas and chondrosarcomas of the cranialbase remain a significant clinical challenge, although local tumorcontrol and extended patient survival can be achieved in the majorityof patients after aggressive surgical and PRT management.
794The Surgical Management of Cushing’s Disease:Results in a Contemporary Series of 328 PatientsEdward R. Laws, Jr., M.D., John B. Hanks, M.D.,Mary L. Vance, M.D.
INTRODUCTION: Cushing’s disease, the result of hypercorti-solism secondary to an adrenocorticotropic hormone (ACTH)-secreting pituitary adenoma, produces serious morbidity and mortal-ity and is difficult to diagnose and treat effectively. This contemporaryseries of surgically treated patients delineates strategies for successfulmanagement, including the use of radiosurgery and adrenalectomy.
METHODS: A retrospective review of 328 patients initially treatedwith transsphenoidal surgery for presumed Cushing’s disease be-tween 1992 and 2003 was performed. Mean follow-up was 28 months(1–132 mo). Adjunctive therapy for failures and recurrences was alsoevaluated. Subsequent bilateral adrenalectomy was performed in 25patients.
RESULTS: Primary pituitary surgery performed in 215 patientswith microadenomas resulted in 75% remission. Secondary pituitarysurgery for 56 patients with prior surgery elsewhere resulted in 50%remission. Surgery for 58 patients with ACTH macroadenomas re-sulted in 57% initial remission. Recurrent disease developed in 11% ofpatients overall. Failures and recurrences were treated with radiosur-gery (n " 56) and/or adrenalectomy (n " 25). Radiosurgery led toremission in 73%; adrenalectomy with subsequent steroid replace-ment reliably normalized cortisol levels but led to Nelson’s syndromein 32%. Complications included one death from syndrome of inap-propriate secretion of antidiuretic hormone (SIADH)/hyponatremia,cerebrospinal fluid rhinorrhea (n " 3), DI/SIADH (n " 8), pseudotu-mor syndrome (n " 2), nasal septal perforation (n " 6), and bleeding,optic neuropathy, and deep vein thrombosis (n " one each).
ABSTRACTS OF OPEN PAPERS
484 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

CONCLUSION: Early diagnosis and effective pituitary surgery canproduce remission of Cushing’s disease in 75% of patients. Failuresand recurrences are managed with multimodality therapy includingradiosurgery and adrenalectomy in selected cases.
795Stereotactic Radiosurgery: An Alternative to SurgicalResection for Patients with Glomus Jugulare TumorsBruce E. Pollock, M.D., Michael J. Link, M.D.,Robert L. Foote, M.D.
INTRODUCTION: Microsurgical removal of glomus jugulare tu-mors is frequently associated with injury of the lower cranial nerves.To decrease the morbidity associated with management of these pa-tients, stereotactic radiosurgery was performed as an alternative tosurgical resection.
METHODS: From 1990 to 2002, 35 patients (mean age, 59 yr)underwent radiosurgery as primary management (n " 16) or forrecurrent glomus jugulare tumors (n " 19). The mean tumor volumewas 13.0 cm3; the mean tumor margin dose was 14.7 Gy. No patientwas lost; the mean follow-up was 48 months.
RESULTS: Normal facial movement was more common for patientshaving primary radiosurgery compared with patients with recurrenttumors (88 versus 53%, P " 0.03). After radiosurgery, 12 tumorsdecreased in size and 22 remained stable (tumor growth control rate,97%). One patient had tumor progression noted at 99 months andunderwent repeat radiosurgery. Five patients (14%) improved afterradiosurgery, and 25 remained neurologically unchanged. Five pa-tients (14%) developed new deficits (hearing loss, n " 4; facial numb-ness and hearing loss, n " 1) after a single procedure. For 24 patientswith testable hearing before radiosurgery, hearing preservation wasachieved in 86 and 81% at 1 and 3 years, respectively. No patientdeveloped a new lower cranial nerve deficit after single radiosurgery;the patient having repeat radiosurgery had a new vocal cord paralysisone year after his second procedure.
CONCLUSION: Radiosurgery provided tumor control with a lowrisk of new cranial nerve injury in early follow-up (mean, 4 yr).Radiosurgery can be safely used to primarily manage patients withglomus jugulare tumors that do not have significant cervical extensionor for patients with recurrent tumors in this location. Longerfollow-up is required to completely understand the role that radio-surgery should play for this patient group.
796Proteins and Protein Pattern Differences betweenGlioma Cell Lines and Glioblastoma MultiformeTimothy W. Vogel, B.A., Robert J. Weil, M.D.,Alexander O. Vortmeyer, M.D., Weifen Zeng, M.D.,Youn-soo Lee, M.D., Makoto Furata, M.D.,Edward H. Oldfield, M.D., Zhengping Zhuang, M.D., Ph.D.
INTRODUCTION: Research into the pathogenesis, molecular sig-naling, and treatment of glioblastoma multiforme (GBM) has tradi-tionally been conducted using cell lines derived from malignant gli-omas. To identify proteins whose expression may be altered in cellculture, we compared protein expression patterns between solid pri-mary GBMs and GBM cell lines.
METHODS: Cultured human glioma cell lines U87, U118, U251,and A172 and tissue from selective microdissection of eight primary
GBMs to obtain pure populations of tumor cells were studied usingtwo-dimensional gel electrophoresis (2DGE) and differential expres-sion software. Select protein targets expressed differentially betweenGBM tumors and GBM cell lines were sequenced using tandem massspectrometry (MS/MS).
RESULTS: Analysis of primary GBM (n " 8) and GBM cell linesrevealed reproducibly similar and distinct proteomic patterns for eachgroup, which distinguished tumors from the cell lines. Gels containedup to 500 proteins that were consistently identified in the pH 4 to 7range. Comparison of proteins identified in the tumors and cell linesdemonstrated approximately 160 proteins that were gained and 60proteins that were lost on culture. Using normalized intensity patternsfrom the 2DGE images, analysis of variance tests were performed andstatistically significant spots were identified. Seven proteins from thecell lines were increased compared with the tumors (P ! 0.05),whereas 10 proteins were significantly decreased from cell lines com-pared with the tumors. Proteins identified included transcription fac-tors, tumor suppressor genes, cytoskeletal proteins, and cellular met-abolic proteins.
CONCLUSION: Global protein and proteomic differences wereidentified between primary GBM tumor samples and human GBMcell lines. The proteins identified elucidate some of the selectionpressures of in vitro culture, expose certain advantages and limita-tions of cell culture, and may enhance our understanding of glio-magenesis and spur development of new therapeutics.
797Survival after Biopsy or Resection of SupratentorialLobar Glioblastoma Multiforme:A Population-based StudyFred G. Barker II, M.D., Manish K. Aghi, M.D., Ph.D.,William T. Curry, M.D., Bob S. Carter, M.D., Ph.D.
INTRODUCTION: The importance of resection rather than biopsyas a predictor of survival in glioblastoma multiforme (GBM) has beencontroversial. We studied this question using population-based meth-ods.
METHODS: The data source was the SEER Public-Use database(National Cancer Institute, Bethesda, MD), 1988–2000. Survival anal-ysis used multivariate Cox proportional-hazards regression. Resultswere validated against the Nationwide Inpatient Sample (HealthcareCost and Utilization Project, Agency for Healthcare Research andQuality, Rockville, MD) and by using a propensity score model tocompensate for selection bias.
RESULTS: There were 11,219 GBM patients in the database. Onlypatients with supratentorial, lobar tumors (frontal/temporal/parietal/occipital), not in overlapping or deep regions, and not cross-ing the midline or tentorial notch were included. Patients withouthistological confirmation or without active follow-up were excluded,as were those in whom surgery was contraindicated because of otherconditions. Biopsied patients more commonly failed to undergo radi-ation after diagnosis, so only patients who had postoperative radia-tion were included in the survival analysis. The final analysis included2496 patients (2143 deaths) and accounted for patient age, sex, andrace, tumor location, size, histology (giant cell or gliosarcoma vari-ants), and marital status. Statistically significant prognostic factorsincluded age, tumor size, and marital status. In a full multivariatemodel, the risk of death for biopsied patients was 1.6 times that ofresected patients (95% CI, 1.4–1.8; P ! 0.001). Subgroup analysesshowed similar values for the hazard ratio in patient groups defined
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 485

by age, tumor site, and size, although the actual difference in mediansurvival between biopsied and resected patients varied with somefactors (especially age).
CONCLUSION: This large, multivariate, population-based studyconfirmed the value of resection rather than biopsy as a prognosticfactor for survival in glioblastoma. Patient- and tumor-related factorssuch as age and tumor size had little interaction with the difference insurvival after resection in this cohort.
798Accuracy of Image-guided Stereotactic Brain Biopsyin the Diagnosis of Glioma: Comparison of Biopsyand Open Resection SpecimenMatthew J. McGirt, M.D., Graeme Woodworth, B.S.,Amer Samdani, M.D., Ira Garonzik, M.D.,Alessandro Olivi, M.D., Jon Weingart, M.D.
INTRODUCTION: Tissue heterogeneity and rapid tumor progres-sion may decrease the accuracy and prognostic value of stereotacticbrain biopsy in the diagnosis of gliomas. Correct tumor grading istherefore dependent on accuracy of biopsy needle placement. Theaccuracy of frameless and frame-based techniques in the diagnosisand grading of glioma remains unstudied.
METHODS: The diagnoses of 21 astrocytic brain tumors werederived using image-guided stereotactic biopsy (12 frame-based, 9frameless) and followed by open resection of the lesion 1.5 months(0.5–4 mo) later. The histological diagnoses yielded by biopsy werecompared with subsequent histological diagnosis from open tumorresection.
RESULTS: Stereotactic biopsy histology accurately represented thegreater lesion at open resection a median of 45 days later in 16 patients(76%) and correctly guided therapy in 19 (91%). Biopsy accuracy offrameless versus frame-based stereotaxy was similar (89 versus 66%, P" 0.21). In 3 patients (14%), biopsy specimens were adequate todiagnose glioma; however, histology was insufficient for definitivetumor grading (grade III versus IV). Anaplastic oligodendroglioma(ODG) was undergraded as low-grade ODG in 1 patients (5%). Biopsyof new-onset GBM yielded necrosis/gliosis and was called nondiag-nostic in one patient. Tumors $50 cm3 were eightfold less likely toaccurately represent the grade of the entire lesion at resection com-pared with lesions !50 cm3 (OR, 8.8; 95% CI, 0.9–100; P " 0.05).
CONCLUSION: Both frameless and frame-based magnetic reso-nance imaging-guided stereotactic brain biopsy are safe and accu-rately represent the larger glioma mass sufficiently to guide subse-quent therapy. The diagnostic accuracy of frameless stereotactic brainbiopsy is equivalent to the frame-based technique in the diagnosis andgrading of glioma. Glioma volume $50 cm3 may be a negative prog-nostic indicator of biopsy accuracy.
799Independent Predictors of Morbidity afterImage-guided Stereotactic Brain Biopsy: A RiskAssessment of 270 Consecutive CasesMatthew J. McGirt, M.D., Graeme Woodworth, B.S.,James Frazier, M.D., Alex Coon, M.D., Ira Garonzik, M.D.,Alessandro Olivi, M.D., Jon Weingart, M.D.
INTRODUCTION: Image-guided stereotactic brain biopsy is asso-ciated with transient morbidity in 7 to 10%, permanent morbidity in 4
to 6%, and mortality in 0.5 to 1% of patients. To date, a critical analysisof risk factors predictive of enhanced operative risk in frame-basedand frameless stereotactic brain biopsy has not been performed.
METHODS: We reviewed the clinical and radiological records of270 consecutive frame-based and frameless image-guided stereotacticbrain biopsies. The associations between biopsy-related morbidityand clinical, operative, and radiological variables were assessed viamultivariate logistic regression analysis.
RESULTS: Thirty-six patients (13%) experienced streotactic biopsy-related morbidity; 23 (8%) transient, 13 (5%) permanent, 3 (1%) mor-tality. Biopsy site hematoma occurred in 25 patients (9%), and 10 (4%)were symptomatic. Diabetes mellitus (OR, 3.73; 95% CI, 1.37–10.17;P " 0.01), thalamic lesions (OR, 4.06; 95% CI, 1.63–10.11; P " 0.002),and basal ganglia lesions (OR, 3.29; 95% CI, 1.05–10.25; P " 0.040)were independent risk factors for morbidity. In diabetic patients,operative-day glucose $200 mg/dl had 100% PPV; glucose !200mg/dl 95% NPV for biopsy-related morbidity. Pontine biopsy was nota risk factor for morbidity. Only 2 of 45 patients (1%) with prebiopsyepilepsy experience seizures postoperatively. More than one needletrajectory increased the incidence of deficits from 17% to 44% in deeplesions (basal ganglia, thalamus), P " 0.05, but was not associatedwith morbidity in cortex lesions. Number of biopsy specimens takenper trajectory was not associated with morbidity in all lesions.
CONCLUSION: Basal ganglia lesions, thalamic lesions, and dia-betic patients were independent risk factors for biopsy-associatedmorbidity. Operative day hyperglycemia strongly predicted morbid-ity in the diabetic population. Epilepsy did not predispose to biopsy-associated seizure. For deep-seated lesions, increasing the number ofbiopsy samples along an established tract versus performing a secondtrajectory may minimize morbidity. Stereotactic biopsy is a safe pro-cedure with low permanent morbidity (5%) and should be performedcautiously for lesions of the thalamus and basal ganglia. Close peri-operative glucose control is mandatory.
800Experience with Transient Spinal Cord Injuryin AthletesJulian E. Bailes, M.D.
INTRODUCTION: The phenomenon of transient spinal cord injury(TSCI) during athletic competition is one of the most difficult situa-tions that the neurosurgeon may encounter.
METHODS: Thirty-five athletes with symptoms of TSCI were evalu-ated by athletic trainers, emergency medical service personnel, and teamphysicians. Diagnosis included physical and neurological examinations,radiographs with flexion extension studies, computed tomography, andmagnetic resonance imaging (MRI). The majority of injuries occurredduring football, but also during wrestling, baseball, gymnastics, andskiing. Mechanisms in football involved tackling, driving the helmet intoan opponent, and being tackled. Symptoms included paralysis, weak-ness, or numbness of all extremities and hemiparesis and ranged from 15minutes to 48 hours. No evidence of fracture/dislocation or ligamentousinstability was seen, whereas 20 had spinal stenosis. Fourteen wereallowed to return to contact sports without recurrent TSCI, with a meanfollow-up of 40 months; others retired.
RESULTS: Several mechanisms have been proposed to attempt toexplain why this intriguing phenomenon with loss of function, with-out identifiable spinal structural deficit, may occur, often called con-cussion. Spinal stenosis was our most common finding. Recent expe-rience has led to the current emphasis on MRI assessment of
ABSTRACTS OF OPEN PAPERS
486 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

cerebrospinal fluid signal called the “functional reserve.” Indeed, thecatastrophic spinal injury that occurs in contact athletes seems not tobe caused by an athlete’s spinal anatomy but rather on use of impacttechniques of making initial contact with the top or crown of thehelmet.
CONCLUSION: There seem to be two groups of athletes whosustain TSCI: those who experience TSCI yet have normal radio-graphic studies, and those with cervical stenosis, the more difficultmanagement group. In this large series of TSCI in contact athletes, itdoes not seem that a single episode of TSCI in the presence of spinalstenosis will substantially increase the risk of subsequent catastrophicspinal cord injury and that many may safely return to play.
801Do the GM-1 Multicenter Data Confirm the NationalAcute Spinal Cord Injury Study-3?Fred H. Geisler, M.D., Ph.D., William P. Coleman, Ph.D.
INTRODUCTION: The National Acute Spinal Cord Injury Study(NASCIS) needs independent confirmation, including the comparisonbetween starting methylprednisolone sodium succinate (MPSS) at !3hours versus later. The GM-1 Multicenter Trial had more patients(760) than the primary subset (127 of 487) in NASCIS-2 or the set (499)recruited for NASCIS-3.
METHODS: This was a retrospective analysis of data from a pro-spective trial. “Marked recovery” was improvement '2 grades fromASIA Impairment Scale at baseline to Modified Benzel at Week 26. Allreceived the NASCIS-2 dose of MPSS, starting at !8 hours.
RESULTS: MPSS !3 (n " 469) and MPSS $3 (n " 289) differed inways perhaps inhering in very fact that MPSS was started early. Ofthese patients, 40.9% of MPSS !3 were admitted directly to tertiarycare, but only 34.3% of MPSS $3, P " 0.077. Furthermore, MPSS !3had earlier EMT cont.
CONCLUSION: Neither NASCIS-3 nor the GM-1 Study was pro-spectively randomized to compare MPSS ! 3 with MPSS $ 3, yet thiscomparison was implied by NASCIS-3’s conclusions and therapeuticadvice on MPSS dosage. In the GM-1 data, there is no superiority ingiving MPSS earlier rather than later.
802Brain Tissue Oxygen-guided Management ReducesMortality in Traumatic Brain InjuryMichael F. Stiefel, M.D., Ph.D., Oscar Guillamondegui, M.D.,Alicia Garuffe, Stephanie Bloom, M.S.N.,Eileen Maloney-Wilensky, M.S.N., Vincente H. Gracias, M.D.,M. Sean Grady, M.D., Peter D. Le Roux, M.D.
INTRODUCTION: Intracranial pressure (ICP) monitoring and ce-rebral perfusion pressure (CPP) management continue to be the goldstandard for managing traumatic brain injury (TBI). However, studiessuggest that optimal ICP and CPP management may not preventcerebral ischemia and infarction, which are major factors in determin-ing patient outcome. The prevention of cerebral hypoxia should resultin an improved outcome in patients with TBI. We posit that braintissue oxygen (BtO2)-guided therapy, by reducing the frequency andduration of cerebral hypoxia, will lead to improved outcome.
METHODS: As part of a prospective clinical trial, patients whosustained TBI within an 18-month period were included in this anal-ysis. Patients with penetrating cranial wounds as well as those with
fatal injuries were excluded. Two groups of patients were identified,those with (Group 1) and without (Group 2) BtO2 monitoring. Ther-apy for Group 1 was aimed at maintaining ICP ! 25 mm Hg andCPP $ 60 mm Hg. Patients with BtO2 monitors in addition hadtherapy directed at maintaining BtO2 $ 25 mm Hg.
RESULTS: Twenty-three patients, 18 men and 5 women (mean age,37 % 18 yr) were identified in Group 1. Twenty-four patients, 21 menand 3 women (mean age, 38 % 17 yr) underwent BtO2 monitoring(Group 2). Median Injury Severity Score was 26 and 27 in Groups 1and 2, respectively. The length of stay in the intensive care unit (ICU)for Group 1 patients was 4.4 % 5.2 days. Group 2 remained in the ICUfor significantly longer periods (13.4 % 15.7 d). The mortality rate forpatients undergoing conventional ICP and CPP management was52%. Patients undergoing BtO2-directed management had a signifi-cantly reduced mortality rate of 29% (P ! 0.05).
CONCLUSION: Management and therapy aimed at preventingcerebral hypoxia and maintaining brain tissue oxygen is successful inreducing mortality in traumatic brain injury.
803Study of Coagulation Factors in Patients with MildProlongation of Prothrombin Time: Implications forNeurosurgical PatientsSamuel L. Barnett, M.D., Michael Cimo, M.D.,Kar’en Matevosyan, M.D., Kevin C. Morrill, M.D.,Christopher Madden, M.D., Ravi Sarode, M.D.
INTRODUCTION: The published data do not provide evidence-basedguidance for use of preprocedure plasma therapy in patients with mild tomoderate abnormalities of coagulation tests. The international normal-ized ratio (INR) is calculated from prothrombin time (PT) and is used tomonitor coumadin therapy. However, it is frequently used erroneouslyto assess bleeding risk in patients who are not on coumadin. The purposeof this study was to correlate the levels of relevant clotting factors inpatients with mild abnormalities of PT (INR).
METHODS: Thirty-six patients with a mild prolongation of PT at12.5 to 15 seconds (normal " 9–12.5 s; INR " 1.3–1.5) and normalpartial thromboplastin time (PTT) (normal " 23–35 s) were treated bythe Neurosurgery Service at Parkland Memorial Hospital betweenSeptember 2003 and January 2004. Plasma levels of Factors (F) II, VII,and VIII (normal hemostatic levels $50%) were measured when re-quests for fresh-frozen plasma were received. The PT (INR) and PTTwere correlated with factor levels.
RESULTS: The median PT was 13.6 seconds (mean, 13.8 s), medianINR was 1.38 (mean, 1.3), and median PTT was 30.5 seconds (mean,32.8 s; range, 19.3–37.9 s). The median FII level was 66% (mean, 68%;range, 34 to 107%) The median FVII level was 51% (mean, 53%; range,28 to 124%). There was no correlation between PT or INR with FVIIlevels (P & 0.5). All patients had FVII levels greater than the 15–25%typically recommended as safe for surgery. FII, the precursor ofthrombin, was also hemostatically normal, whereas median FVIIIlevels were elevated at 126% (mean, 156%; range, 55–547%). FVIII is anacute-phase reactant and a strong procoagulant factor, which is asso-ciated with shortened PTT in many patients.
CONCLUSION: In patients with a mild prolongation of PT (INR),plasma levels of Factor II and VII were hemostatically normal,whereas FVIII was increased. Aggressive correction of mild elevationof PT (INR up to 1.5) may be unnecessary in patients with no evidenceof continued bleeding. This may lead to fewer transfusion-relatedmorbidities and help to conserve valuable blood products.
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 487

804Conventional Neuro Critical Care Monitoring Failsto Ensure Cerebral OxygenationMichael F. Stiefel, M.D., Ph.D.,Gregory G. Heuer, M.D., Ph.D.,Eileen Maloney-Wilensky, M.S.N., Alicia Garuffe,Stephanie Bloom, M.S.N., Vincente H. Gracias, M.D.,M. Sean Grady, M.D., Peter D. LeRoux, M.D.
INTRODUCTION: Intracranial Pressure (ICP) monitoring and ce-rebral perfusion pressure (CPP) management continue to be the goldstandard for managing traumatic brain injury (TBI). However, studiessuggest that optimal ICP and CPP management may not alwaysprevent cerebral ischemia and infarction. We posit that with conven-tional neuromonitoring, inadequate cerebral oxygenation may occurin some patients.
METHODS: Patients who sustained severe multisystem traumaand TBI, documented by an Injury Severity Score (ISS) $ 16 and aGlasgow Coma Scale (GCS) score ! 8, were included in this analysis.Cerebral oxygenation was measured within 8 hours of the initialinjury using the commercially available Licox Monitor. ICP, CPP, andPaO2 were also monitored continuously.
RESULTS: Twenty patients, 17 men and 3 women, with a mean ageof 37 % 18 years presented with an ISS $ 16 and GCS ! 8 after severemultisystem trauma. ICP less than 25 mm Hg was successfully main-tained in 80% of the patients, and CPP greater than 60 mm Hg wassustained in 95% of patients. Oxygen saturation (SaO2) was greaterthan 90% in 92% of the patients. Despite adequate control of both ICPand CPP, BtO2 measured during the initial hour of resuscitation wasless than 25 mm Hg in 65% of the patients and less than 20 and 10 mmHg in 45 and 25% of the patients, respectively.
CONCLUSION: Conventional strategies consisting of ICP and CPPmanagement may result in significant reductions in cerebral oxygen-ation despite what would otherwise be considered adequate intracra-nial pressure and cerebral perfusion.
805Immune System-based Therapies for CentralNervous System TraumaJonathan B. Marder, Ph.D., Gustavo Auerbach, DM.D.,Linda Jones, P.T., Irit Shefer, David Snyder, Ph.D.
INTRODUCTION: Traumatic damage to the central nervous sys-tem (CNS) leads a wave of cell degeneration causing loss of neuro-logical function. The damage is permanent because the CNS has anextremely limited capacity for nerve regeneration. Other tissues, in-cluding peripheral nerves, have active repair mechanisms in whichthe immune system plays a central role in clearing debris and toxicelements and supporting new growth. Although the immune systemdoes respond to CNS damage, the activity is suppressed by the“immune privilege.” However, controlled boosting of the immuneresponse has therapeutic potential.
METHODS: Several methods have been developed for immune ther-apies to treat CNS trauma. These include a cell therapy using autologousskin-coincubated macrophages, vaccines that induce a neuroprotectiveeffect that attenuates posttraumatic damage, and an immunomodulator(PN277) that improves the spontaneous immune response.
RESULTS: Incubated macrophages were shown to induce nerve re-covery in several preclinical models, including rat optic nerve transec-tion, rat spinal cord transection, and rat spinal contusion. The therapy
was adapted for clinical use in a Phase I clinical trial that providedprelimary evidence of safety and efficacy. Neuroprotective vaccinationwas tested in animal models of white and gray injury, with differentantigens providing protection in different models depending on theirtissue specificities. PN277 immunomodulator was found to be effective ina wide spectrum of animal models for neurotrauma and neurodegenera-tive disease, notably stroke and optic nerve trauma.
CONCLUSION: Immune-based cell therapies, neuroprotective vac-cines, and immune modulators have significant potential in the treat-ment of many neurological disorders, including trauma to the brainand spinal cord.
806Penetrating Head Injuries from Terrorist BombBlasts: The Jerusalem ExperienceGuy Rosenthal, M.D., Lilach Roemi, B.A., R.N.,Yigal Shoshan, M.D., Ricardo Segal, M.D.,Felix Umansky, M.D.
INTRODUCTION: From December 2000 to March 2004, we treated24 patients with penetrating head injuries caused by terrorist bombblasts. A variety of objects are placed in these bombs to maximizetissue damage and penetrate the cranium, including ball bearings,metal bolts, hexagonal nuts, segments of metal rods, and nails.
METHODS: Data on consective injured patients were collectedprospectively. Three patients presented with a Glasgow Coma Scale(GCS) score of between 3 and 5, six patients with a GCS score of 6 to9, four patients with a GCS score of 10 to 12, and 11 patients with aGCS score of 13 to 15. Fifteen patients underwent craniotomy, ven-triculostomy, intracranial pressure (ICP) monitoring, or a combinationimmediately after injury.
RESULTS: Of the 13 patients who underwent ICP monitoring, themean ICP at insertion was 20.3 mm Hg, with a range of 8 to 30 mmHg. The peak ICP in these patients was 33.5 mm Hg and ranged from12 to 70 mm Hg. Of the patients who did not obey commands atpresentation, the mean time to return to consciousness was 5.4 days(range, 2–12 d). Three patients died, and 21 survived. At a meanfollow-up of 18.2 months (range, 2–28 mo), 14 surviving patientsachieved a GOS score of 5, six a GOS score of 4, and one patient hada GOS score of 3. Two patients developed a traumatic intracranialaneurysm, and two patients had documented migration of a metallicfragment within the brain. One patient developed a fatal ventriculitis.Four patients underwent delayed removal of a metallic fragment withthe aid of an image-guided surgical navigation system with goodresults.
CONCLUSION: Patients with penetrating head injuries from bombblasts can achieve good functional outcomes. Complications includinginfection, traumatic intracranial aneurysm, and migration of frag-ments must be anticipated and treated aggressively. In a subgroup ofpatients, delayed removal of metallic fragments may be warranted.
807A Protocol of Delayed Surgery in 125 Cases ofPenetrating, Craniocerebral Gunshot Wounds:The Cape Town ExperienceAdriaan W. Liebenberg, Ch.B.,Andreas K. Demetriades, F.R.C.S., Sunil Naik, Ch.B.,Carl Hardwidge, M.B.B.S., Bennie H. Hartzenberg, M.Med.(S)
INTRODUCTION: We report retrospectively on 125 cases of civil-ian low-velocity penetrating craniocerebral gunshot wounds (GSWs)
ABSTRACTS OF OPEN PAPERS
488 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

treated in our unit in Cape Town, South Africa, from January 1997 toOctober 2003. All patients were acutely resuscitated and managed ina basically equipped intensive therapy unit without intracranial pres-sure monitoring or a full-time intensivist. We practice a protocol ofdelayed definitive debridement. Early surgery is reserved for cases ofsignificant, acute hematomas. Basic wound care and skin closure areperformed in all cases in the emergency room.
METHODS: Case notes were obtained retrospectively and re-viewed, and data were entered into an electronic database created bythe author. Statistical analysis was performed by the Centre for HealthCare Research of the University of Brighton, England.
RESULTS: Mean age was 24.9 years (standard deviation, 10.9 yr),and 111 patients (88.8%) were male. There were 17 (13.6%) suicidecases and 4 tangential GSWs. Mean presenting Glasgow Coma Scale(GCS) score was 7.33. In 70.4%, the presenting GCS score was 3 to 8;in 7.2%, the GCS score was 9 to 12; and in 22.4%, it was 13 to 15.Forty-eight cranial procedures were performed on 26 patients (20.8%):delayed debridement (21/26), emergency surgery (4/26), and delayedexternal ventricular drainage (1/26). Average time to delayed defin-itive debridement was 12.2 days. Infection complicated 8 patients(15.7% of survivors), with 3 having meningitis, 4 brain abscesses, and1 meningitis and a brain abscess. Total mortality was 69.6% (87/125).The discharge GOS score was poor (1–3) in 89 (71.2%) (only 2 withGOS score 2 or 3) and good (GOS 4 or 5) in 36 (28.8%). Predictors forpoor outcome included low presenting GCS score, intubation in thefield, and transventricular tract on computed tomography.
CONCLUSION: We report on a protocol of delayed debridementsecondary to wound care and closure as primary procedure. Within thesetting of limited resources, the results suggest that this would be anacceptable management strategy for penetrating craniocerebral GSWs.
808Results of Stereotactic Radiosurgery for BrainArteriovenous Malformations in Chidren:The University of Toronto ExperienceGelareh Zadeh, M.D., Yuri Andreda-Souza, M.D.,Michael Schwartz, M.D.
INTRODUCTION: Stereotactic radiosurgery has become an ac-cepted treatment modality in the management of pediatric arterio-venous malformations (AVMs). We present long-term outcomes for aseries of pediatric AVMs treated with linear accelerator (LINAC)-based radiosurgery at the University of Toronto.
METHODS: Between 1994 and 2002, of the 250 patients with AVMtreated with radiosurgery, 37 were under 18 years of age. The decisionto treat using radiosurgical management was reached by a multidis-ciplinary group at the University of Toronto composed of vascularneurosurgeons, interventional neuroradiologists, and radiation on-cologists. In eloquent brain, a marginal dose of 15 Gy at the 67%isodose contour and in noneloquent brain a marginal dose of 29 Gy atthe 90% isodose contour was administered using a LINAC modifiedfor radiosurgery. Application of the stereotactic head frame was per-formed under general anesthesia for patients less than 14 years of age.A concurrent intra-arterial digital angiograph and dynamic computedtomographic scan with selective intra-arterial injection of contrastmaterial were performed. We had follow-up information for a 36-month period on 30 patients.
RESULTS: The mean age of the patients was 12 years, and themedian age was 13 years. The majority of patients presented withhemorrhage (23 of 37), followed by 3 patients with seizures, 6 with
headaches, and one incidental presentation. The percentage of pa-tients presenting with hemorrhage was significantly higher than ouradult population. Complete angiographic follow-up was available on30 patients, and 71% showed complete obliateration of the AVMs.Four patients had a new neurological deficit as a consequence ofradiosurgery procedure, 3 of which included cerebral edema.
CONCLUSION: Our LINAC-based treatment of pediatric AVMsprovides a safe and efficacious management option, with results com-parable to other series using either gamma knife or LINAC radiosur-gery. Our obliteration rate and low rate of complications support apivotal role for LINAC radiosurgery in treatment of pediatric AVMs.
809Radiosurgery for Pediatric ArteriovenousMalformations: An Outcome StudyVini G. Khurana, M.D., Ph.D., Bruce E. Pollock, M.D.
INTRODUCTION: Although stereotactic radiosurgery is com-monly performed for patients with arteriovenous malformations(AVMs), the efficacy and safety of this management strategy is poorlyunderstood for pediatric patients.
METHODS: Between 1990 and 2001, 34 patients &18 years under-went AVM radiosurgery. The median patient age was 15 years; 16patients (47%) had sustained a prior hemorrhage. Twenty-four AVMs(71%) were Spetzler-Martin Grade III or higher; 14 patients (41%) hadAVMs located in the basal ganglia, thalamus, or brainstem. We deter-mined the radiosurgery-based AVM score for each patient (AVMscore " [0.1][volume, cm3] # [0.02][age, yr] # [0.3][location; frontal/temporal " 0, parietal/occipital/corpus callosum/cerebellar " 1,basal ganglia/thalamus/brainstem " 2]). The median radiosurgery-based AVM score was 0.98 (range, 0.36–3.80). The median initial AVMvolume was 3.3 cm3 (range, 0.2–32.4 cm3). The median AVM margindose was 20 Gy. The median follow-up was 36 months.
RESULTS: Twenty-five patients had one radiosurgery, 8 patientsunderwent repeat radiosurgery, and 1 patient had three radiosurgicalprocedures. No patient bled or required surgical resection after radio-surgery. One patient (3%) developed hand numbness after repeatradiosurgery of a thalamic AVM. Outcomes after radiosurgical man-agement were excellent (complete obliteration, no new deficit; n " 23,68%), unchanged (incomplete obliteration, no new deficit; n " 10,29%), and poor (incomplete obliteration, new deficit; n " 1, 3%). Eightof 11 patients not achieving an excellent outcome await final angiog-raphy. Univariate analysis found that patient age, AVM volume, AVMlocation, or Spetzler-Martin grade did not correlate with excellentoutcomes. Patients with a radiosurgery-based AVM score &1.00 ex-perienced an excellent outcome more frequently than patients with anAVM score $1.00 (88 versus 47%, P " 0.01).
CONCLUSION: Radiosurgery cured the majority of pediatric AVMpatients with minimal morbidity. The radiosurgery-based AVM scoreaccurately predicted outcomes for pediatric AVM patients.
810Advanced Magnetic Resonance Spectroscopy in theDiagnosis of Pediatric Brain TumorsMark D. Krieger, M.D., J. Gordon McComb, M.D.,Marvin D. Nelson, M.D., Ashok Panigrahy, M.D.,Ignacio Gonzalez-Gomez, M.D., Floyd H. Gilles, M.D.,Stefan Bluml, M.D.
INTRODUCTION: Treatment of pediatric central nervous system(CNS) neoplasms is highly dependent on identifying tumor type and
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 489
discerning tumor from other radiographic anomalies, including non-neoplastic postoperative changes. To overcome the limitations of cur-rent noninvasive imaging techniques, the present study uses novelmagnetic resonance spectroscopy (MRS) techniques to elucidate iden-tifying biochemical features of pediatric CNS neoplasms in vivo,which may facilitate diagnosis and treatment.
METHODS: Under an institutional review board-approved proto-col, 34 children were identified with newly diagnosed, untreated braintumors. Upon retrospective review, this series included 13 primitiveneuroectodermal tumors, 7 pilocytic astrocytomas, 3 astrocytomas, 4anaplastic astrocytomas, 2 ependymomas, 2 anaplastic ependymomas,and 3 choroid plexus papillomas. Using a novel technique, single-voxel 1-H MRS spectra of the tumors were acquired on a 1.5-T GEclinical scanner. This technique allowed absolute quantification (ininstitutional units) of N-acetyl-aspartate, creatine, choline, myoinosi-tol, and taurine. Controls consisted of an additional voxel in theoccipital cortex of the same patients and 25 normal age-matchedpatients studied on the same 1.5-T GE clinical scanner.
RESULTS: Taurine was significantly higher in PNET tumor regionsthan in “Other Tumor” (6.1 % 2.2 versus 1.5 % 1.4, P ! 0.0001).Myoinositol was significantly elevated in choroid plexus papillomas,distinguishing these tumors from other tumors (20.7 % 3.8 versus11.4 % 7.4, P ! 0.0001). Creatine levels were significantly reduced inpilocytic astrocytoma regions (1.0 % 0.8 versus 4.5 % 1.4, P ! 0.0001),distinguishing them from astrocytomas and other tumors.
CONCLUSION: This study identifies biochemical constituents thatuniquely identify pediatric CNS tumors and can be used as a nonin-vasive means of diagnosis and disease follow-up. Future work exam-ines the correlation of levels of these constituents with disease activity.
811Relationship between Valve Opening Pressure, BodyPosition, and Intracranial Pressure in Normal-pressure Hydrocephalus: Paradigm for Selectionof Programmable Valve Pressure SettingMarvin Bergsneider, M.D., Isaac Yang, B.S., Shon Cook, M.D.,Donald P. Becker, M.D.
INTRODUCTION: There is little scientific basis for guidance inselecting the optimal valve for the treatment of normal-pressure hy-drocephalus (NPH). The aim of this study was to determine theprogrammable valve opening pressure (OPV) setting that would re-sult in a slight reduction in intracranial pressure (ICP) after a ven-triculoperitoneal (VP) shunt. We also assessed whether shunt-inducedICP changes could be predicted on the basis of a simple hydrody-namic equation.
METHODS: In this prospective study of 11 patients with NPH, ICPwas measured before and after implantation of a shunt incorporatinga programmable valve without an antisiphon device. Pressure mea-surements, including intraperitoneal pressure (IPP), and shunt hydro-static column lengths (HC) were recorded at body angles rangingfrom 0 to 55 degrees and at valve settings ranging from 30 to 200 mmH2O. Measured ICP values were compared with values computedusing a simple hydrodynamic equation (ICPPredicted " OPV & HC #IPP).
RESULTS: Even at the highest OPV setting of 200 mm H2O, whichexceeded the mean baseline ICP (164 % 64 mm H2O), there was asignificant reduction in the postoperative ICP in the supine position(125 % 69 mm H2O, P " 0.04). The OPV did not equal the measuredpostoperative ICP. Linear regression revealed a nonunity slope (0.39)
and a nonzero y intercept (47 mm H2O versus measured IPPSupine of69 % 23 mm H2O). A precipitous decline of ICP at upright bodypositions, predicted by so-called siphoning, was not seen. Instead,postural ICP profile nearly paralleled that of the baseline measure-ments.
CONCLUSION: This study indicates that very high OPV settingsmay be optimal for the initial treatment of NPH. The relationshipbetween ICP and OPV is linear but not predicted by simple hydro-dynamics. In NPH, VP shunts seem to lower ICP in a “physiological”manner without significant siphoning.
812Transsphenoidal Surgery in Childhood andAdolescent Cushing’s DiseaseShabin Joshi, F.R.C.S., Richard J.D. Hewitt, M.B.B.S.,Kia Rejazoi, F.R.C.S., Habib Ellamushi, M.O. Savage,Fary Afshar
INTRODUCTION: Cushing’s disease (CD) in children and adoles-cents is rare. If untreated, it carries a significant morbidity and mor-tality. The aim of this study was to review the results of surgicalmanagement of CD in a specialist center.
METHODS: A retrospective review of 25 consecutive patients, allunder the age of 18 years and managed by a single surgeon, whounderwent transsphenoidal surgery for CD at St. Bartholomew’s andthe Royal London Hospitals between January 1983 and January 2004.
RESULTS: Twenty-five patients, consisting of 10 girls and 15 boyswith a mean age of 13.4 years and average symptom duration of 2.2years, were identified. The main presenting features were weight gain(100%) and impaired growth (95%), with hypertension occurring in athird of the patients. All patients underwent detailed endocrine in-vestigations and computed tomography or magnetic resonance imag-ing. Bilateral inferior petrosal sinus sampling was performed in 19patients, with successful prediction of the side of the microadenoma in14. Since 2002, neuronavigation techniques have been used. Surgicalremoval was the only treatment required in 15 patients, and wascombined with radiotherapy in 10. Fifteen patients achieved “cure” orremission. One patient had a cerebrospinal fluid leak, 9 had an iso-lated growth hormone deficiency, 3 had permanent diabetes insipi-dus, and 1 had panhypopituitarism. There were no cases of meningi-tis, no neurological deficit, no redo surgery, and no mortalities.
CONCLUSION: This review, believed to be the largest of its kind,proposes that surgery at a specialist center is a safe and effectivemanagement modality for CD.
813Familial Incidence of Moyamoya Syndrome in thePediatric PopulationEdward R. Smith, M.D., R. Michael Scott, M.D.
INTRODUCTION: In patients who present with moyamoya syn-drome, questions regarding the need for screening of family membersoften arises. Previous reports from Japan have suggested a familialincidence of 7 to 12%. Here, we report on the familial associationsidentified in a large North American clinical series of moyamoyapatients treated by a single surgeon.
METHODS: We reviewed the clinical records of a consecutiveseries of moyamoya patients operated on at 21 years of age or younger
ABSTRACTS OF OPEN PAPERS
490 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com

over a 19-year period (January 1985 to March 2004) by a singleneurosurgeon.
RESULTS: A total of 184 patients composed the study population,with a female preponderance of patients (60%). Of these 184 patients,10 were found to have a familial or hereditary syndrome (5.4%), witheither mother–child (two families) or sibling–sibling involvement,including three pairs of identical twins. In one set of identical twins,both children were affected by moyamoya. There were two other setsof identical twins in this series, but these pairs each had only oneaffected sibling.
CONCLUSION: We report on the finding of 10 patients with fa-milial associations in a series of 184 patients with moyamoya syn-drome (5.4%). The three sets of identical twins, with one pair havingboth siblings affected and the other two pairs with only one affectedsibling, are evidence supporting a role for both genetic and environ-mental factors in the pathogenesis of moyamoya. Although furtherstudy is warranted, it seems that there is some evidence supportingthe premise of screening of first-degree relatives of patients presentingwith moyamoya.
814Measurements of Magnet-induced Changes inPressure Settings of Adjustable HydrocephalusShunt ValvesSheng Liu, B.S., Richard Greene, M.D.,Gordon A. Thomas, Ph.D., Joseph R. Madsen, M.D.
INTRODUCTION: The advent of adjustable shunt valves hasadded a new possibility for management of hydrocephalus in childrenby providing control of the pressure at which a ball-in-cone valveopens. The advantage of being able to change the valve characteristicsusing an external magnet system comes with the potential disadvan-tage of unintended resetting of the valve by ambient external mag-netic fields.
METHODS: We quantified the magnetic field strengths needed toreprogram the Codman Hakim Programmable Valve (CHPV, n " 7)and the Medtronic STRATA valve (n " 4). Using a specially con-structed instrument, we determined threshold values (in gauss) of theexternal magnetic field that would change the valve setting. Wecompared different initial valve settings, directions of valve rotation,and valve type (CHPV versus STRATA).
RESULTS: As expected, all valves are susceptible to setting changesin a rotating magnetic field. The magnetic field strength required torotate the valves was dependent on the initial valve setting, withhigher fields generally required for higher settings. Field strengthsrequired to turn the valves to a higher setting were similar for the twotypes of valves (127–215 G, CHPV versus 73–150 G, STRATA), but thefield strength required for the downward turn (other than from thelowest initial setting) for the STRATA was strikingly lower than forthe CHPV (26–38 G versus 117–177 G, P ! 0.0001, analysis of variancefactorial design).
CONCLUSION: Assuming that ambient exposures in real life aredistributed favoring low field exposures with random direction ofrotation, clinicians should expect more frequent inadvertent valvesetting changes in STRATA valves, and accidental changes to a lowerlevel would be far more likely than increases with either valve type.Safety issues would depend on the still somewhat conjectural ideathat the pressure needed for opening the valve is highly correlatedwith shunt function and control of symptoms.
815Monobloc Distraction Osteogenesis in PediatricPatients with Severe Syndromal CraniosynostosisTorstein R. Meling, M.D., Bernt J. Due-Tonnessen, M.D.,Hans-Erik Hogevold, Ph.D., Per Skjelbred, Prof,Kjartan Arctander, M.D.
INTRODUCTION: The management of the hypoplastic midface insyndromic craniosynostosis remains a great challenge. Frequently, thepatients have to be operated on numerous times to achieve a satisfac-tory end result functionally and aesthetically. This is, in part, becauseof limitations in the skeletal advancement possible when using tradi-tional surgical techniques. However, during the last decade, methodsfor gradual midfacial advancement have been presented whereby thecraniofacial surgeon can obtain greater advancements.
METHODS: We present four children with severe syndromal cranio-synostosis in need of midface advancement surgery because of severerespiratory obstruction or severe exophthalmus. The patients had severalprevious craniofacial reconstructive surgeries (mean, 2.75 times; range,2–5 times) that yielded insufficient skeletal advancements and did notaddress the midface hypoplasia. Consequently, they were operated onusing distraction osteogenesis, with gradual monobloc advancements.
RESULTS: The mean length of operation was 370 minutes (range,240–455 min), and the mean amount of peroperative blood transfusionneeded was 1300 ml (range, 280-2700 ml). Not surprisingly, the patientwith the greatest number of previous operations also had the longestoperation time as well as greatest blood loss. The average midfaceadvancement obtained was 25 mm (range, 20–30 mm), resulting in asignificant decrease or cessation of preoperative respiratory problems,reduced exophthalmus, and improved facial profile. Apart from alocal infection in one patient with a connective tissue disorder andseveral previous wound infections, no major postoperative complica-tions were recorded.
CONCLUSION: Distraction osteogenesis has become a versatileand safe technique that allows for large advancements of the midface.
816Electrophysiologically Guided Tethered Spinal Cord:University of Virginia ExperienceNader Pouratian, M.D., Ph.D., Tracy L. Owensby, B.S.,W. J. Elias, M.D., Lawrence A. Phillips, M.D.,John A. Jane, M.D., Ph.D.
INTRODUCTION: Tethered cord release is often complicated bydistorted anatomy, making it difficult to identify viable nervous tis-sue. These surgeries therefore carry a high risk for neurological injury.Various intraoperative monitoring and mapping techniques havebeen described; an effective mapping system should provide imme-diate information regarding the functionality of tissue and preventpermanent injury.
METHODS: We retrospectively reviewed 102 consecutive tetheredcord surgeries in 88 patients (ages ranging from 4 d to 73 yr) over a13-year period at the University of Virginia. In all cases, we usedelectromyography to guide tethered cord release, both monitoring forpassive muscle activity changes (caused by traction or compression ofneural elements) and mapping peripheral responses to electrical stim-ulation of suspected neural elements. Recordings sites were selectedappropriately to map the nerve roots in question. The causes of oftethering included diastematomyelia, lipomyelomeningocele, myelo-meningocele, tumor, tight filum, and/or scarring from prior surgery.
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 491

RESULTS: In the majority of cases, mapping identified neuraltissue that was not otherwise visually evident directly adjacent to thearea of tethering. In these cases, the intraoperative plan was modifiedby the results of mapping: in 18 cases (18%), untethering was limitedor incomplete because of fear of iatrogenic injury and in 5 cases (5%),the untethering was completely aborted because of such fear. Inelectrophysiologically silent areas, mapping allowed more aggressivedissection and untethering. Postoperative functional deteriorationwas limited to 5% of the population, whereas improved functionalstatus was seen in $35% of cases. Nineteen percent of patients haddocumented need for further untethering surgery.
CONCLUSION: Intraoperative electrophysiological monitoringand mapping is an efficient, effective and reliable method for intra-operative guidance and limiting iatrogenic injury. The authors discussthrough their experiences the vital role monitoring has played inpreventing inadvertent nerve damage, preserving function, and po-tentially decreasing the necessity for repeat procedures.
817Complications of EndoscopicCraniosynostosis RepairSteven R. Cohen, M.D., Henry E. Aryan, M.D.,Rahul Jandial, M.D., Hal S. Meltzer, M.D.,Ralph E. Holmes, M.D., Michael L. Levy, M.D., Ph.D.
INTRODUCTION: To potentially improve outcome in nonsyn-dromic synostosis, we devised a technique of endoscope-assisted pro-cedures with definitive osteotomies and fixation using resorbableplates. These techniques are designed to achieve an immediate recon-struction of the deformity, thereby limiting the duration of the post-operative helmet or band.
METHODS: To better understand the potential problems associ-ated with endoscopic approaches considered as an alternative to opensurgery, we performed an analysis of 27 infants undergoing endo-scopic craniosynostosis repair since June of 2000 compared with acohort of 20 open cases.
RESULTS: Patients undergoing open procedures were a mean ageof 20.7 months (median, 11 mo). Mean age for the endoscopic groupwas 5.6 months. There was a significant decrease in estimated bloodloss, transfusion, and operative duration in the endoscopic group.Two patients (one coronal and one metopic) required a conversionfrom an endoscopic to an open procedure intraoperatively. One pa-tient (coronal) required a second open procedure 12 months after thefirst. One patient had a small breakdown of the skin over a macroporescrew and was treated conservatively. No seizures were noted. Therewere no infections or mortalities in the series. The mean hospital stayswere 2.6 days in the endoscopic versus 3.4 days in the open group.
CONCLUSION: Our data verify the safety of the endoscopic tech-nique. Helmets or bands are not used routinely. This approach is aworthwhile tool to consider for patients !9 months old with sagittalsynostosis and !6 months old with mild to moderate metopic/unicoronal synostosis.
818Use of Programmable Valves to PreventOvershunting Complications in InfantsVictor L. Perry, M.D., Nalin Gupta, M.D., Ph.D.
INTRODUCTION: Hydrocephalus remains a common neurosurgi-cal problem in the pediatric population. Despite the advent of newer
interventions such as third ventriculostomy, ventriculoperitonealshunting remains a mainstay of therapy. Because of the unique anat-omy of the infant cranium (e.g., open cranial sutures), overshuntingcomplications such as overriding parietal bones and microcephalymay be encountered with the use of fixed-pressure valves. We de-scribe the use of programmable valves in infants requiring ventricularcerebrospinal fluid (CSF) drainage to prevent overshunting complica-tions.
METHODS: We retrospectively examined 22 patients who under-went placement of a programmable ventriculoperitoneal shuntingdevice during the perinatal period for treatment of hydrocephalus atthe University of California, San Francisco Medical Center. Meanfollow-up period was 1.5 years. Valves were set at low pressures (30mm Hg) at insertion. Pressure settings were increased to 150 mm Hgat the 1-month interval. Head circumference measurements weretaken at presentation, at surgery, and at 1-, 3-, 6-, and 12-monthintervals. Data were analyzed for number of subsequent valve adjust-ments, number of revisions, and incidence of all complications.
RESULTS: All patients underwent successful placement of a pro-grammable ventriculoperitoneal shunting device. Two patients un-derwent removal and replacement of the device secondary to infec-tion. Seven patients underwent revision secondary to malfunction.Mean head circumference measurements remained between the 50thand 90th percentiles for age throughout the follow-up period.
CONCLUSION: The reported incidence of CSF overdrainage sec-ondary to ventriculoperitoneal shunting varies between 5 and 55%.These potential complications include intracranial hypotension, low-pressure syndromes, slit ventricle syndrome, intracranial hemorrhage,cranial deformities, and microcephaly. No overshunting complica-tions were observed in this study population. We conclude that theadvent of programmable valves may provide neurosurgeons with anadditional tool in preventing complications of overshunting in infantswith hydrocephalus.
819Venous Air Embolism during the SurgicalTreatment of Craniosynostosis Using MinimallyInvasive TechniquesDavid F. Jimenez, M.D., Constance M. Barone, M.D.,Joseph D. Tobias, M.D., Joel O. Johnson, M.D., Ph.D.
INTRODUCTION: The surgical correction of patients with cranio-synostosis can be associated with multiple intraoperative risk factors,including venous air embolism (VAE), the incidence of which hasbeen reported as high as 82.6%. This prospective study was under-taken to analyze the incidence of VAE in patients with craniosynos-tosis undergoing treatment using minimally invasive endoscopic tech-niques.
METHODS: A total of 180 patients undergoing endoscopic assistedsuture release were monitored continuously for VAE using precordialDoppler monitoring. A recording was made of the Doppler tones andlater reviewed to verify accuracy. A total of 9513 minutes were re-corded during the study.
RESULTS: The study group included 180 consecutive patients with89 sagittal, 47 coronal, 39 metopic, and 6 lambdoid synostoses. Therewere 116 boys and 64 girls. Ages ranged between 12 weeks and 14.5months. The mean surgical time was 61 minutes (range, 22 to 106min). Four patients were detected to have experienced VAE (2.2%incidence). Two episodes were Grade I (change in Doppler tones).Two were Grade II (change in Doppler tones and decrease in end-tidal
ABSTRACTS OF OPEN PAPERS
492 | VOLUME 55 | NUMBER 2 | AUGUST 2004 www.neurosurgery-online.com
CO2), and there were no Grade III (decrease in systolic blood pressureby 20% from baseline).
CONCLUSION: Endoscope-assisted craniectomies for treatment ofcraniosynostosis is associated with a very low incidence of intraoper-ative venous air embolism. The pathophysiology of VAE will bediscussed.
820Endoscope-assisted Fronto-orbital and CranialOsteotomiesSteven R. Cohen, M.D., Ralph E. Holmes, M.D.,Henry E. Aryan, M.D., Burak M. Ozgur, M.D.,Hal S. Meltzer, M.D., Michael L. Levy, M.D., Ph.D.
INTRODUCTION: An operative approach has been developed thatincorporates fronto-orbital and cranial osteotomies to achieve imme-diate correction using specially designed bioresorbable plates andscrews. Postoperative helmet/band therapy may be eliminated or itsduration shortened using these techniques.
METHODS: Forty-two patients (age, 2 to 8 mo) with sagittal (n "25), metopic (n " 11), unicoronal (n " 5), or lambdoidal synostosis(n " 1) underwent endoscopic craniosynostosis repair with complexosteotomies performed through two or three small incisions in thescalp and/or upper eyelids. Suturectomy was performed in concertwith wedge osteotomies, outfracture of parietal plates, reduction ofcranial length, and stabilization with resorbable plates and screws forpatients with sagittal synostosis, whereas unilateral or bilateral fronto-orbital advancement was performed for children with unilateral coro-nal (UCS) and metopic synostosis, respectively. Specially designedbioresorbable plates were used for fixation when appropriate.
RESULTS: Follow-up has ranged from 1 month to 2 years. Onepatient developed bleeding in the recovery room that required trans-fusion. One patient with UCS required conversion to the open proce-dure. One patient with UCS will require reoperation. All patients weredischarged by hospital Day 3. Two patients with sagittal synostosishad a small protrusion on the vertex of the cranium despite postop-erative helmet therapy. Satisfactory to excellent aesthetic results wereobtained in the remaining cases. In five of the children, helmets werenot used. The others were placed in postoperative helmets for 6 to 12weeks.
CONCLUSION: Preliminary results are encouraging. More
follow-up is necessary to determine selection criteria and criticallyevaluate outcomes. With more experience and refinement of instru-mentation, minimally invasive repair will become an important tool insurgical management of craniosynostosis.
821Early Surgical Release of Tethered Cord May BenefitChildren with a History of Imperforate AnusDarlene A. Lobel, M.D., Mark R. Lee, M.D., Ph.D.
INTRODUCTION: Anomalies of the caudal spinal cord that causetethering often present in children with a history of imperforate anus.We examined the role of early versus delayed surgery in these chil-dren.
METHODS: A retrospective review at our institution between Jan-uary 2000 and December 2003 identified eight children with a historyof imperforate anus who were referred to neurosurgery for evaluationof tethered cord. Age at diagnosis, presenting symptoms, magneticresonance imaging (MRI) findings, timing of surgery, and postoper-ative course were analyzed.
RESULTS: Two children who underwent delayed surgery (ages, 3and 8 yr) after presenting with urinary incontinence and radiculopa-thy showed no improvement in bladder function after surgery. MRIfindings revealed a dermoid tumor in one patient and a filum lipomain the other. Six children underwent early surgery (between 5 and 18months of age) after diagnosis by screening MRI shortly after birth. Ofnote, screening ultrasound at birth was normal in all but one patient.MRI findings included fibrolipomatous infiltration of the filum (fourpatients), intradural lipoma (three patients), and low-lying conus(three patients). One of these children became symptomatic withprogressive scoliosis by the time of surgery; this did not progresspostoperatively. The other five patients remained neurologically in-tact after surgery; one of these patients presented with recurrenttethered cord 2 years later.
CONCLUSION: Children born with imperforate anus may developirreversible neurological deficits caused by a tethered spinal cord.Children who presented after developing neurological deficits did notimprove with surgery. Children who underwent early surgery re-mained neurologically intact. These results suggest that children withimperforate anus may benefit from early MRI screening and earlyrelease of tethered cord to avoid permanent neurological sequelae.
ABSTRACTS OF OPEN PAPERS
NEUROSURGERY VOLUME 55 | NUMBER 2 | AUGUST 2004 | 493





























