Embed Size (px)
Citation preview

Why do older people get stuck in hospital?
Martin Vernon
Consultant Geriatrician

Answer…
• Because older people more likely to become ill..
• …and need hospital care..
• …and less likely to recover to independence…
• …and more likely to need more care…
• …for which planning and provision takes resources…

Case Study (1)
• Mrs P: 88 lives alone, type II diabetes, hypertension, eczema
• Admitted with a fall at home, confused, unable to walk
• Similar admission 1 year ago: home with carers after rehab
• In last 3 months: 2 further admissions, last one two weeks ago
• Diagnosed with pneumonia, acute kidney injury, unstable diabetes
• Brain scan indicates worsening vascular brain disease over last year

Case Study (2)
• Recovers and expresses strongly a wish to return home
• Family at distance concerned: increased frequency of admission
• During discharge planning develops hallucinations: urinary sepsis
• Treated and recovers very slowly: fluctuating cognition and capacity
• Mobility poor and high risk of falls: ward based rehab

Case Study (3)
• During rehab eczema worsens: nursing needs escalate
• Diabetes remains unstable, intermittently refusing diet
• Further respiratory infection and antibiotic associated diarrhoea
• Repeated delirium with incomplete recovery, immobile, incontinent
• Diagnosis of vascular dementia: no capacity for discharge decision
• Best interests meeting with family: care home placement, CHC

UK Delayed Discharges
• Medical discharges particularly prone to delay
• Those aged >75 most likely to experience inappropriate stay
• 14% acute bed days inappropriate, 60% for non-medical reasons
– Prognostic uncertainty
– Awaiting community services, care home or care package
– Best interests and Continuing Health Care eligibility processes
– Disputed discharge plan (patient, professionals, family)
• Up to one third of delays are avoidable: cost £0.5M/year per 30 beds
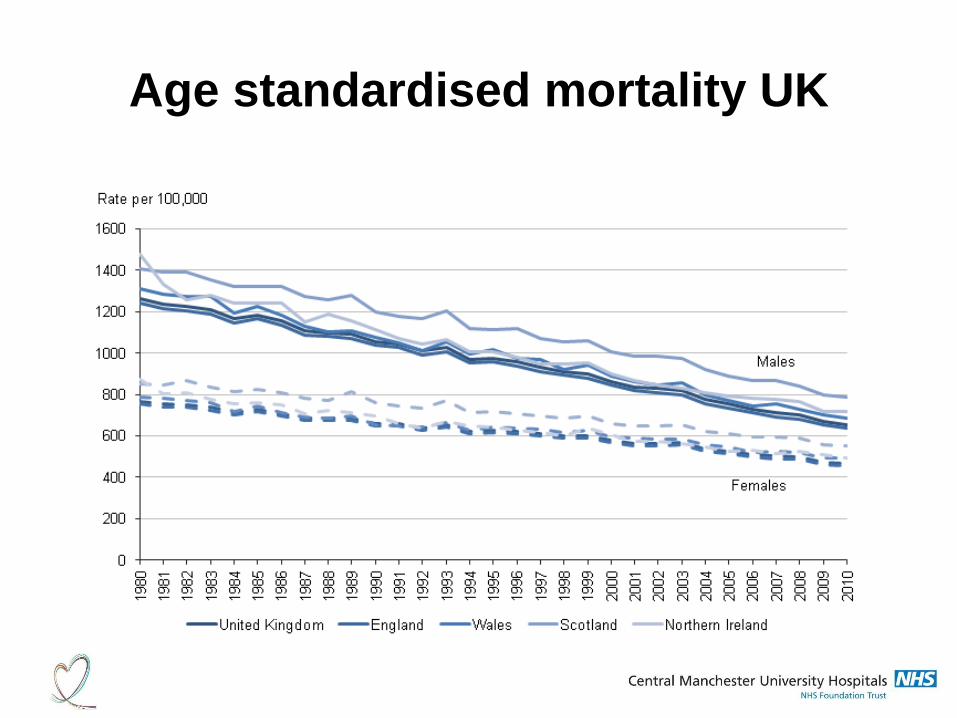
Age standardised mortality UK

Consequence of…successful ageing
Kings Fund 2013
Next 20 years number of people:
>85 in England will double >100 will quadruple
Largest single group of NHS users 2/3 acute hospital beds used by +65 +65 used 40% of all hospital bed days 43% NHS spend on those aged +65

Multi-morbidity
• 1 in 4 adults has 2 or more long term conditions
• 50% of older people have 3 or more LTC
• Comorbidity independent risk factor for adverse outcomes
– Quality of Life
– Death
– Need for healthcare
– Disability
– Treatment complication
• Multi-morbidity: co-existent, not necessarily co-dependent conditions


Multi-morbidity Endpoints
• 685K people >65 in UK with dementia
• 2025: 1M in UK will have dementia
• Dementia in UK costs £17Bn pa
• 130K people have a stroke in E&W pa
• 1/3 will be left with disability
• 250K in UK living with long term disability following stroke
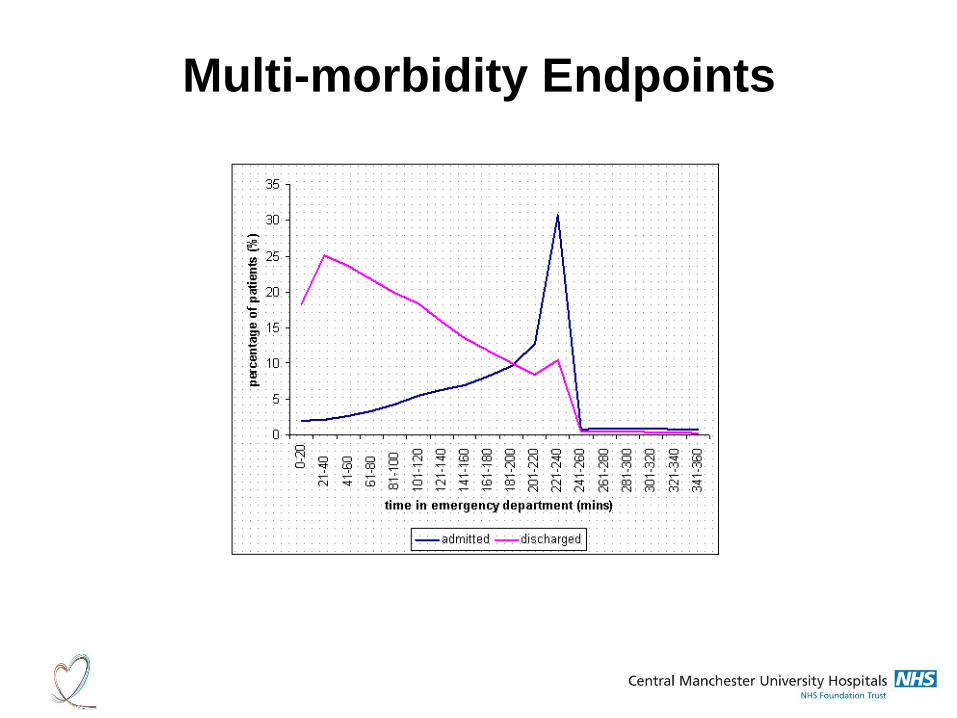
Multi-morbidity Endpoints



Wrong system configuration?
Incomplete Recovery
Dependency
Frailty
Readmission/LTC

Where does frailty fit in?
Problem…
..and opportunity?
Deficit accumulation
• As people age they are more likely to die
• Not all people at same age have same risk of death
• More things wrong, more likely to die
• Health deficits operationalise ‘things wrong’: criteria

Frailty Index
• Measures deficits, for example
• Canadian Study of Health and Aging FI (CSHA FI)
– Count of 70 deficits including
– presence and severity of current diseases
– Ability in ADLs
– Physical signs from clinical exams
• A person with 7 deficits, for example, has index score 7/10=0.1
• Relative frailty = % difference from average score at that age

Frailty Index Ceiling
• Death rate for healthiest at baseline (FI=0) 0.18 at 2 years, 0.69 at 7
years
• Baseline FI>0.45 associated with 100% 7 year mortality
• There is a limit to frailty of FI=0.7
• There is a limit to the number of health conditions people can
tolerate
Age Ageing. 2013 May;42(3):372-7

So…What’s It Telling Us?

Outcomes
• Frailty index based on Comprehensive Geriatric Assessment
• 30 day hospital mortality=12.4% (93: 95% CI=10-15%)
• Dying risk with degree of frailty
• Discharged home had lowest admitting frailty
• Admitted to Nursing Home had moderate to high frailty
• Frailty independently associated with risk of death and LOS
Age Ageing (2013) doi: 10.1093/ageing/aft156

Potential Interventions
CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 72 • NUMBER 12: 2005

What can we do now?
• Early identification of frailty pre-hospital
• Targeted advance care planning for those with high index frailty
• Integrated care using trusted assessors and senior decision makers
• Move emphasis away from hospital admission
– Temporisation in crisis: ‘assess to admit’
– Deflection towards more appropriate community responses
– Early de-escalation from hospital: ‘discharge to assess’
• Trigger and track using frailty to target those most at delay risk

A better system-wide approach
• Hospital front end services focused on frailty identification
• Trigger and track: involve social care and escalate delays early
• Encourage community services ‘pulling’
• Early identification of delirium, dementia and end of life
• Support proactive community care interventions: care homes

HOSPITAL COMMUNITY ‘PLACE’
INTERFACE
GENERAL HOSPITAL
ED
ADMISSIONS
DIAGNOSTICS
SPECIALIST HOSPITAL
OUTREACH
FIRST RESPONSE
CASE MANAGEMENT
CARE HOMES
SUPPORT
COMMUNITY BEDS
DISCHARGE PLANNING
FRAILTY
AMBULATORY CARE
LOW MEDIUM
PRIMARY CARE






























