Embed Size (px)
Citation preview

DFCM Pearls: The seven research studies that will impact clinical practice for academic family physicians
Dr. David M. Kaplan MD MSc CCFP Associate Professor, North York General, Department of Family & Community Medicine Primary Care Lead, Central Local Health Integration Network
Dr. Noah Ivers MD PhD CCFP
Assistant Professor, Women’s College Hospital, Department of Family & Community Medicine. Scientist, Women’s College Research Institute Adjunct scientist, Institute for Clinical Evaluative Studies

DISCLOSURE OF COMMERCIAL SUPPORT • This program has not received financial support

FACULTY/PRESENTER DISCLOSURE • Faculty: Dr. David M. Kaplan • Relationships with commercial interests: none
FACULTY/PRESENTER DISCLOSURE • Faculty: Dr. Noah Ivers • Relationships with commercial interests: none

The 2014 DFCM Pearls Process

DFCM 2014 – Pearl 1
Clinical characteristics associated with increased risk of adverse events in patients presenting to the emergency department with exacerbation of chronic obstructive pulmonary disease: A prospective cohort study. Stiell I, Clement C, Aaron S, Rowe B, Perry J, Brison R, Calder L, Cagaanan R, Lang E, Borgundvaag B, Forster A, Wells GA

The Bottom Line
• 5 variables were independently associated with adverse events in patients presenting to the ED with AECOPD: – prior history of intubation – initial heart rate ≥ 110/ minute – being too ill to do a walk test – hemoglobin < 100 g/L – urea ≥ 12 mmol/L
The Research Question
• Researchers sought to identify clinical characteristics associated with serious adverse events in patients with AECOPD
• Why this is important? – AECOPD is common in clinic and ED – decision to send a patient to the ED or to
admit is difficult and there is little evidence to guide management
What the Researchers Did
• N=945 patients, of whom 354 (37.5%) were admitted
• 74 (7.8%) patients with a subsequent serious adverse event, 36 (49%) had not been admitted after the initial emergency visit
• Conducted multivariable modeling to find clinical variables that were independently associated with adverse events

What the Researchers Found

What the Researchers Found
• 5 variables that were independently associated with adverse events: – prior intubation – initial heart rate ≥ 110/ minute – being too ill to do a walk test – hemoglobin < 100 g/L – urea ≥ 12 mmol/L
• Using a risk score of 2 or higher as a threshold for admission would capture all patients with a predicted risk of adverse events of 7.2% or higher, while only slightly increasing admission rates, from 37.5% to 43.2%

What This Means for Academic and Clinical Practice
• Once validated, this scale could be used to reduce mobility and mortality of patient with AECOPD by slightly increasing the admission rate for these patients
• Hospitals would need to budget for an increase of ~6% more COPD admissions (still lower than reported USA admission rate of ~80%)
• generalization to primary care is uncertain

DFCM 2014 – Pearl 2
Feasibility and Validity of the Self-administered Computerized Assessment of Mild Cognitive Impairment With Older Primary Care Patients Tierney MC, Naglie G, Upshur R, Moineddin R, Charles J, Jaakkimainen RL

The Bottom Line
• It is feasible to use self-administered computerized cognitive tests with older primary care patients and have the results uploaded to our EMRs

The Research Question
• Can the Computerized Assessment of Mild Cognitive Impairment (CAMCI) be independently completed by older primary care patients?
• Why this is important?



What the Researchers Did
• pts aged =/>65y (seen consecutively over 2 months by 1 family practice)
• Excludes: pts with dementia dx or previous work-up for dementia
• N=130 patients with cognitive concerns and a matched sample of 133 without cognitive concerns
• CAMCI was individually administered after instructions to work independently

What the Researchers Found
• 259 Pts (98.5%) completed the entire CAMCI • 241 Pts (91.6%) completed it without any questions
or after simple acknowledgment of their question. • Lack of computer experience decreased the odds
of independent CAMCI completion

What This Means for Academic and Clinical Practice
• Study supports the feasibility of using self-administered computerized cognitive tests with older primary care patients, given the increasing reliance on computers by people of all ages.
• Similar tools can be used by patients independently (regardless of age) with the results uploaded to our EMRs

DFCM 2014 – Pearl 3
Effect of payment incentives on cancer screening in Ontario primary care Kiran T, Wilton AS, Moineddin R, Paszat L, Glazier RH.

The Bottom Line
• No significant step change in the screening rate for breast, colon or cervical cancer was found the year after pay-for-performance incentives were introduced

The Research Question
• To assess whether pay-for-performance scheme for primary care physicians in Ontario was associated with increased cancer screening rates
• Why this is important? – $109M dollars were spent from 2006-2010 in
Ontario as financial incentives to FPs for cervical, breast, and colorectal cancer screening – did they public get value for its money?

What the Researchers Did
• Administrative Database • longitudinal analysis using administrative
data to determine cancer screening rates • segmented linear regression analysis to
assess whether there was a step change or change in screening rate trends after incentives were introduced in 2006/2007

What the Researchers Found
What This Means for Academic and Clinical Practice
• pay-for-performance scheme was associated with little or no improvement
• PFP costs a lot of money • Policy makers should consider other
strategies for improving rates of cancer screening

DFCM 2014 – Pearl 4
Waiting to see the specialist. Patient and provider characteristics of wait times from Primary to Specialty Care. Jaakkimainen RL, Glazier R, Barnsley J, Salkeld E, Lu H, Tu K.
The Bottom Line
• Calculated wait times for a referral from a FP to seeing a specialist physician are longer than those reported by physician surveys

The Research Question
• To calculate the wait times from when a referral is made by a family physician (FP) to when a patient sees a specialist physician and examine patient and provider factors related to these wait times.
• Why this is important? – Family physicians in TCLHIN and CLHIN have
identified access to specialist care a ‘gap’ issue for patients

What the Researchers Did
• Used an Electronic Medical Record Administrative data Linked Database
• EMR referral date was linked to the administrative physician claims date to calculate the wait times
• Patient age, sex, socioeconomic status, comorbidity and FP continuity of care were examined
• Physician age, sex, practice location, practice size and participation in a primary care delivery model were examined

What the Researchers Found

What the Researchers Found
• median waits time: – medical specialists ranged from 39-76 days – surgical specialists from 33-66 days – patient factors did not seem to be associated with wait
times from primary care to specialty care – physician factors were not consistently associated with
wait times • other than for FP practice location and size
What This Means for Academic and Clinical Practice
• Calculated wait times for a referral from a FP to seeing a specialist physician are longer than those reported by physician surveys
• Wait times from primary to specialty care need to be included in the calculation of surgical and diagnostic wait time benchmarks in Canada in order to understand true access to care

DFCM 2014 – Pearl 5
Effect of an educational toolkit on quality of care: a pragmatic cluster randomized trial. Shah BR, Bhattacharyya O, Yu CH, Mamdani MM, Parsons JA, Straus SE, Zwarenstein M.

The Bottom Line
• Despite being relatively easy and inexpensive to implement, a printed educational toolkit did not improve quality of care or cardiovascular outcomes in a population with diabetes.

The Research Question • To evaluate the effectiveness of an
educational toolkit focusing on cardiovascular disease screening and risk reduction in people with diabetes.
• Why this is important? – Printed educational materials for clinician
education are one of the most commonly used approaches for quality improvement – Do they make a difference?


What the Researchers Did

What the Researchers Found Sub Study 1 (administrative data study) • death or non-fatal myocardial infarction, occurred in
11,736 (2.5%) patients in the intervention group and 11,536 (2.5%) in the control group (p = 0.77).
Sub Study 2 (clinical data study) • use of a statin, occurred in 700 (88.1%) patients in
the intervention group and 725 (90.1%) in the control group (p = 0.26). • Pre-specified secondary outcomes, including other
clinical events, processes of care, and measures of risk factor control, were also not improved by the intervention.

What This Means for Academic and Clinical Practice
• Despite being relatively easy and inexpensive to implement, printed educational materials were not effective.
• We need to consider “rigorous and scientifically based approach to the development, dissemination, and evaluation of quality improvement interventions”

DFCM 2014 – Pearl 6
Risk of osteoporotic fractures with Angiotensin II receptor blockers versus Angiotensin Converting-Enzyme inhibitors in hypertensive community-dwelling elderly Butt D, Mamdani M, Gomes T, Lix L, Lu H, Tu K

The Bottom Line
• ARB or an ACE inhibitor have similar effects on bone health of older patients treated for hypertension
• These patients also have a decreased risk of osteoporosis-related fractures with dose escalation of either drug supporting a protective effect on bone

The Research Question
• Do ACE-I and ARBs have clinically significant effects on bone health?
• Why this is important? – ACE inhibitors and ARBs are used to treat
hypertension – No one has yet examined the risk of
osteoporosis-related fractures in hypertensive elderly treated with ARBs versus ACE inhibitors

What the Researchers Did
• population-based, retrospective cohort study • cohort of newly treated hypertensive patients
(>66y started on an ACE-I) matched to ARB users • primary outcome was hip fracture • secondary outcomes were non-hip major
osteoporotic fractures and other osteoporotic fractures.
• calculated hazard ratios (HRs) using Cox proportional hazards model

What the Researchers Found
• 87,635 newly treated Ontario hypertensive elderly
• There were 297 hip fractures, 752 non‐hip major osteoporotic fractures, and 484 other osteoporotic fractures that occurred after starting an ARB or an ACE inhibitor

What the Researchers Found
When adjusted for dosage, there was no significant difference between the effects of ARBs and ACE inhibitors on hip, other major osteoporotic and other osteoporotic fractures
What This Means for Academic and Clinical Practice
• hypertensive older patients treated with an ARB or an ACE inhibitor have similar effects on bone
• decreased risk of osteoporosis‐related fractures with dose escalation of either drug supporting a protective effect on bone

DFCM 2014 – Pearl 7
Increased collision risk among drivers who report driving after using alcohol and after using cannabis Sayer G, Ialomiteanu A, Stoduto G, Wickens CM, Mann RE, Le Foll B, Brands B

The Bottom Line • Drivers reporting neither driving under the
influence of alcohol nor driving under the influence of cannabis were significantly less likely to experience a collision than those who reported one of these behaviours
• Drivers who reported both behaviours had the highest collision risk – three times greater odds of collision than those
who reported only DUIA or DUIC

The Research Question
• To assess the self-reported collision risk among drivers who report DUIA and DUIC in the Ontario adult population.
• Why this is important? – consumption of cannabis is common in Ontario – little research exists on the prevalence of people
who report both DUIA and DUIC and the collisions experienced by this group
What the Researchers Did
• Used the CAMH Monitor (CM) • N=16,224 (2002 to 2010) • Past-year self-reported collision involvement
was examined in three groups – no DUIA or DUIC – DUIA or DUIC – DUIA and DUIC)
• Logistic regression analysis
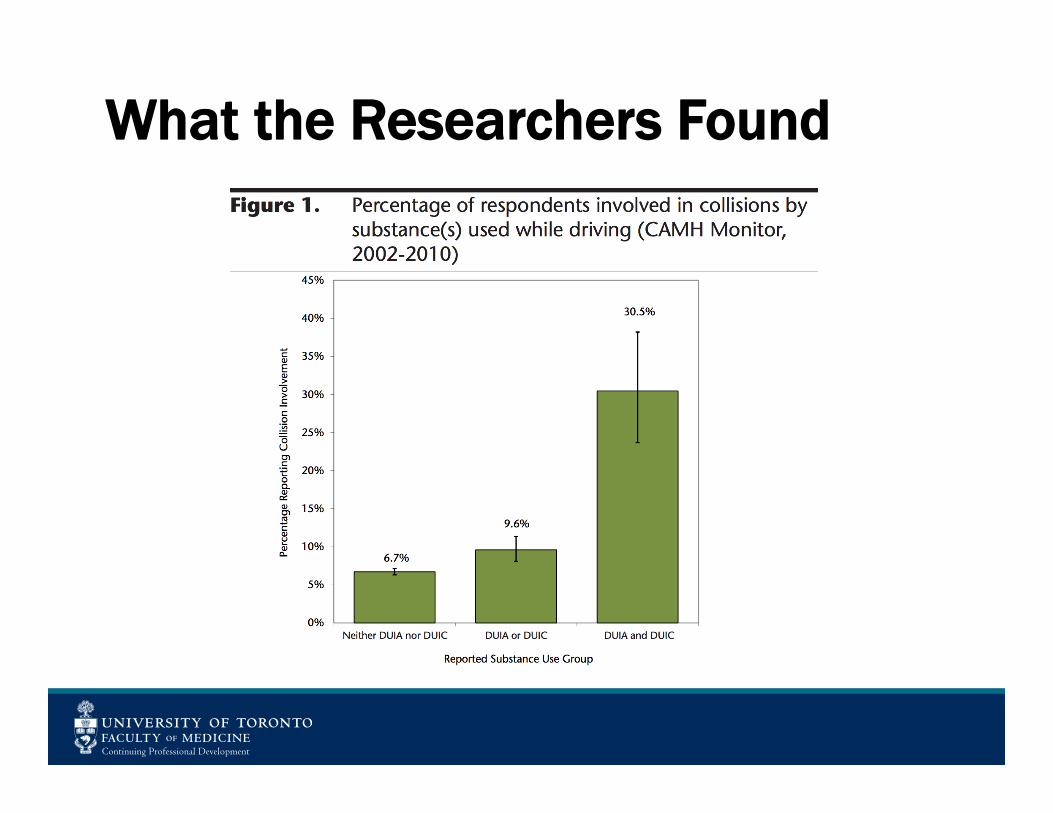
What the Researchers Found

What This Means for Academic and Clinical Practice
• Drivers who reported both behaviours had the highest collision risk - three times greater odds of collision than those who reported only DUIA or DUIC
• FPs should counsel patient who admit to cannabis use using a harm reduction approach similar to safe EtOH use






























