Embed Size (px)
Citation preview
TYPE II ENDOLEAK
FROM TREATMENT OF COMPLICATION TO PREVENTION
April 13-14, 2012
DIVISION OF VASCULAR AND ENDOVASCULAR SURGERY
Chief: Salvatore Ronsivalle, MD

TYPE II ENDOLEAK
It’s the most common form of endoleak and arises from retrograde
filling of the sac by lumbar branches or the inferior mesenteric artery
EARLY noted at the time of EVAR, 40% spontaneously
eventually thrombose
PERSISTENT an ELII that has not spontaneously resolved
within 6 months even in the absence of aneurysm
enlargement
► Selective lumbar artery embolization through hypogastric artery
► Selective AMI embolization through an AMS artery retrograde catheterism
► Laparoscopic retroperitoneal lumbar or inferior mesenteric branches ligation
► Trans distal endograft seal zone treatment
► Translumbar CT managed sac thrombization with biomaterials
► Transabdominal echo-guided sac thrombization with biomaterials
► Surgical semi convertion
► Surgical complete convertion
TYPE II ENDOLEAK WITH SAC ENLARGEMENT
TREATMENT

TYPE II ENDOLEAK
R.V., male, 72 years old
Multiple cardiovascular disease
ASA 3
2000 Aorto-Bisiliac Stent Graft ANEURX (2213135)
2001 for type II EL with sac enlargement
lumbar arteries embolization with coils
2002 for type II EL persistence with sac enlargement
surgical semi-convertion
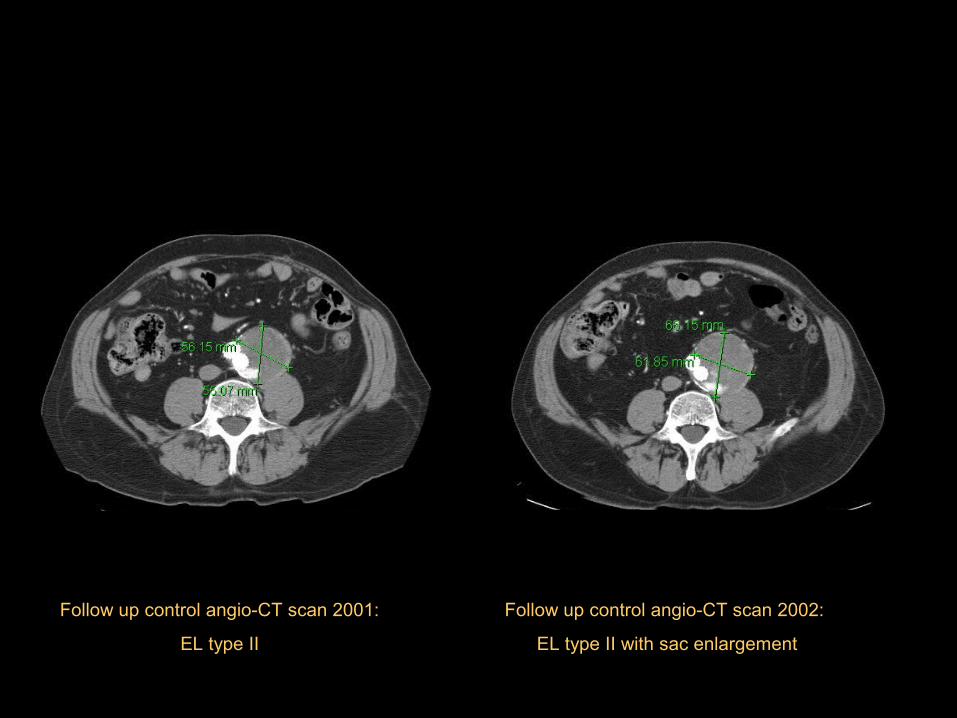
Follow up control angio-CT scan 2001:
EL type II
Follow up control angio-CT scan 2002:
EL type II with sac enlargement
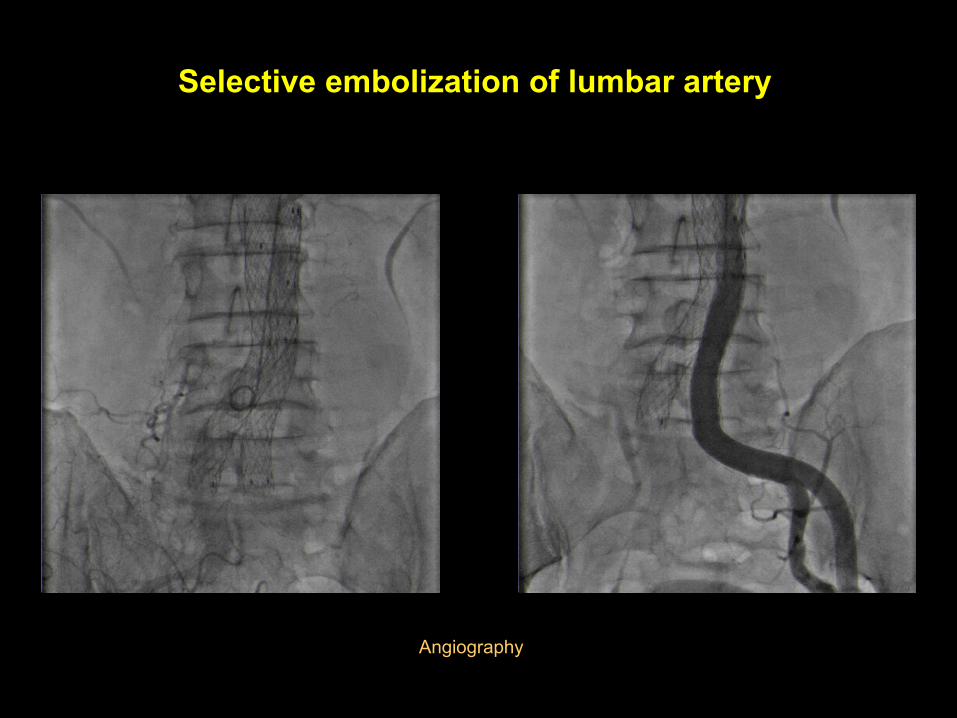
Angiography
Selective embolization of lumbar artery
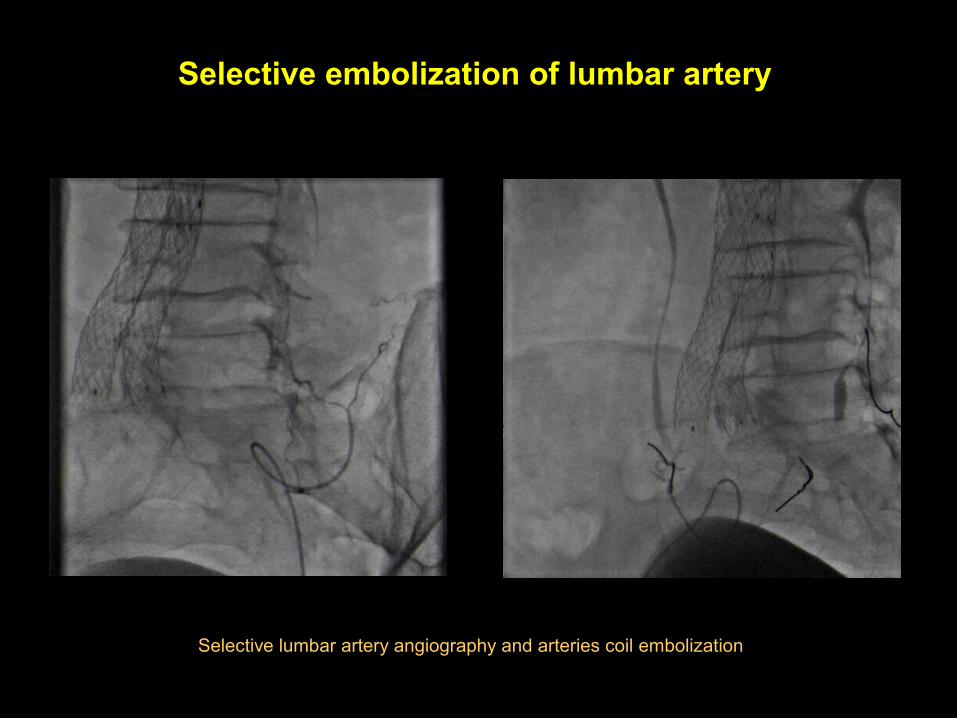
Selective lumbar artery angiography and arteries coil embolization
Selective embolization of lumbar artery

After ECD detectment of EL type II persistence with sac
enlargement, the patient underwent surgical semi-convertion
with aneurysmatic sac opening, lumbar arteries closure,
aneurysmatic sac sewing without graft removing
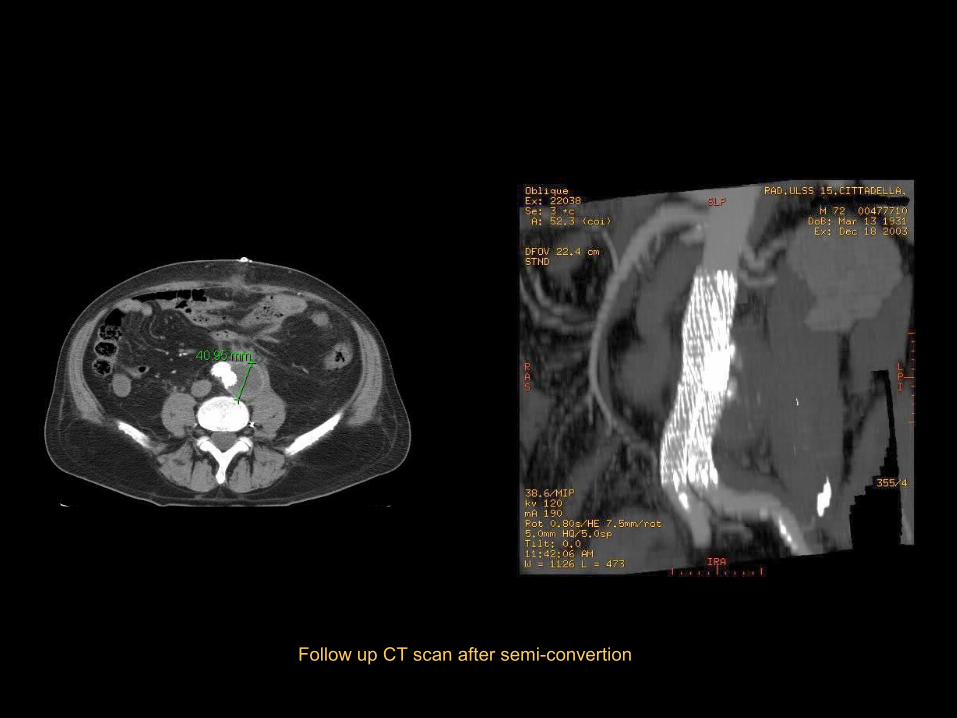
Follow up CT scan after semi-convertion

TYPE II ENDOLEAK
D.P.M. male, 67 years old
Multiple cardiovascular disease
ASA 3
2000 Aorto-Bisiliac Stent Graft ANEURX (2615165; 15115)
2001 for type II EL with sac enlargement
lumbar arteries embolization with coils
2002 for EL II persistence with sac enlargement
surgical convertion
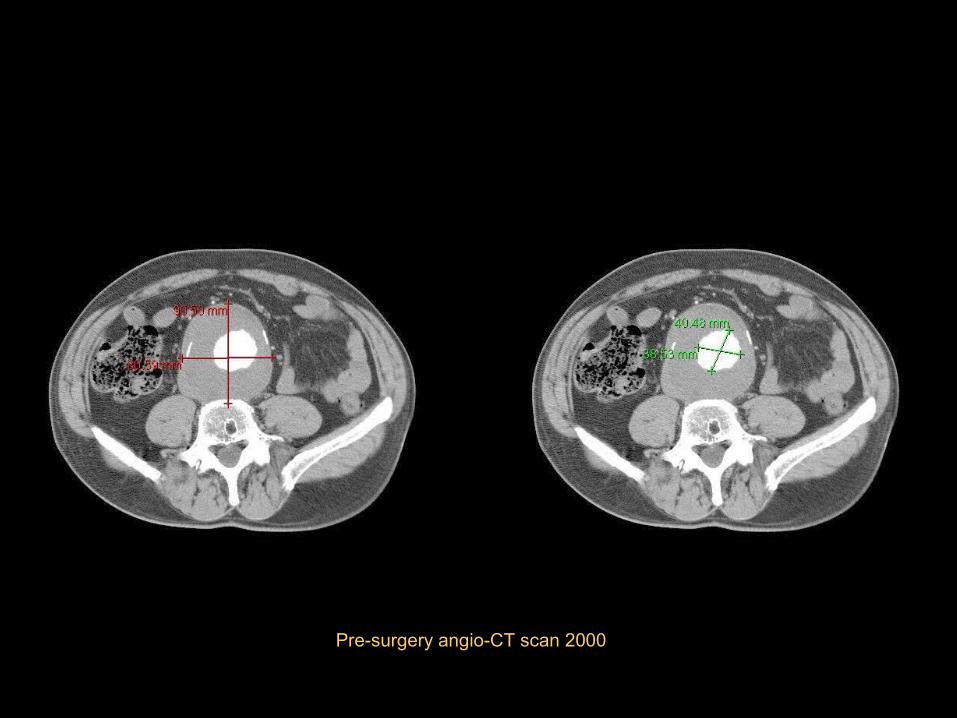
Pre-surgery angio-CT scan 2000
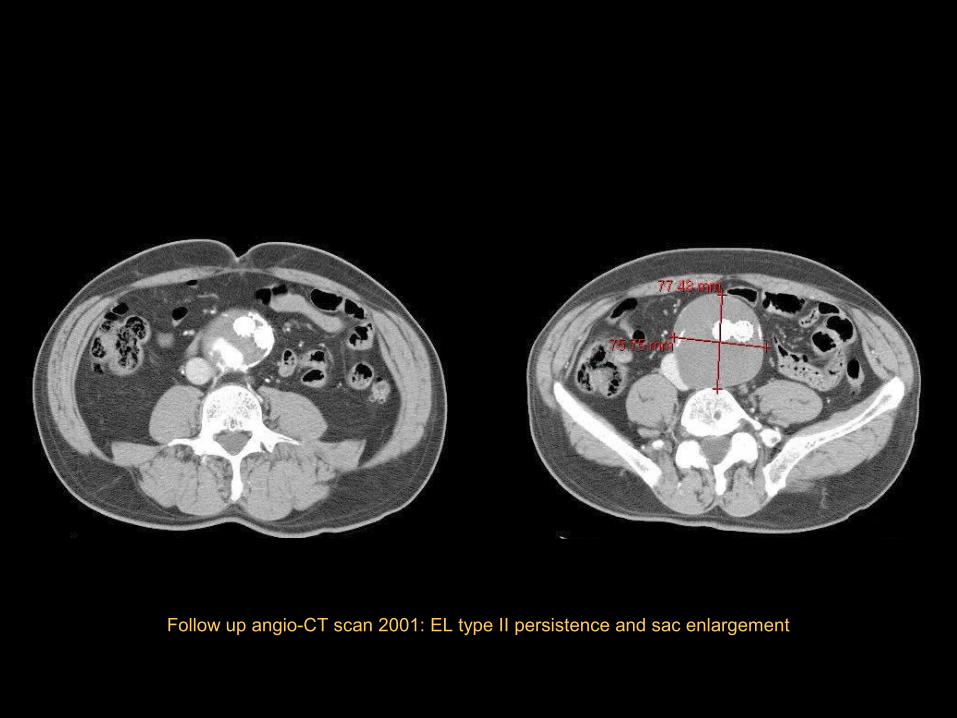
Follow up angio-CT scan 2001: EL type II persistence and sac enlargement
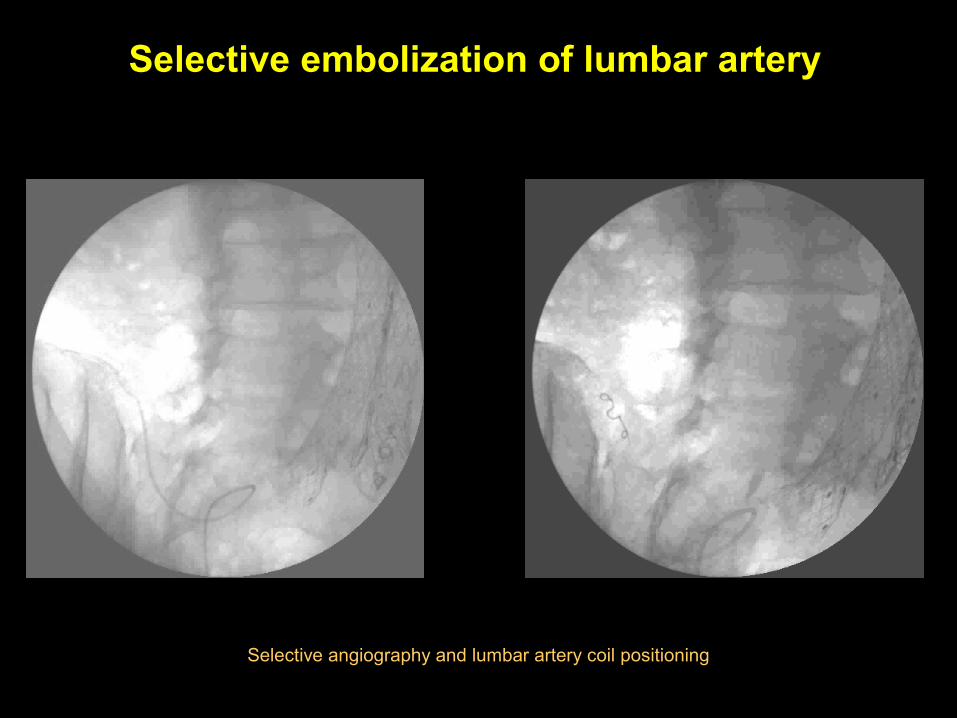
Selective angiography and lumbar artery coil positioning
Selective embolization of lumbar artery

Selective angiography and lumbar artery coil positioning
Selective embolization of lumbar artery
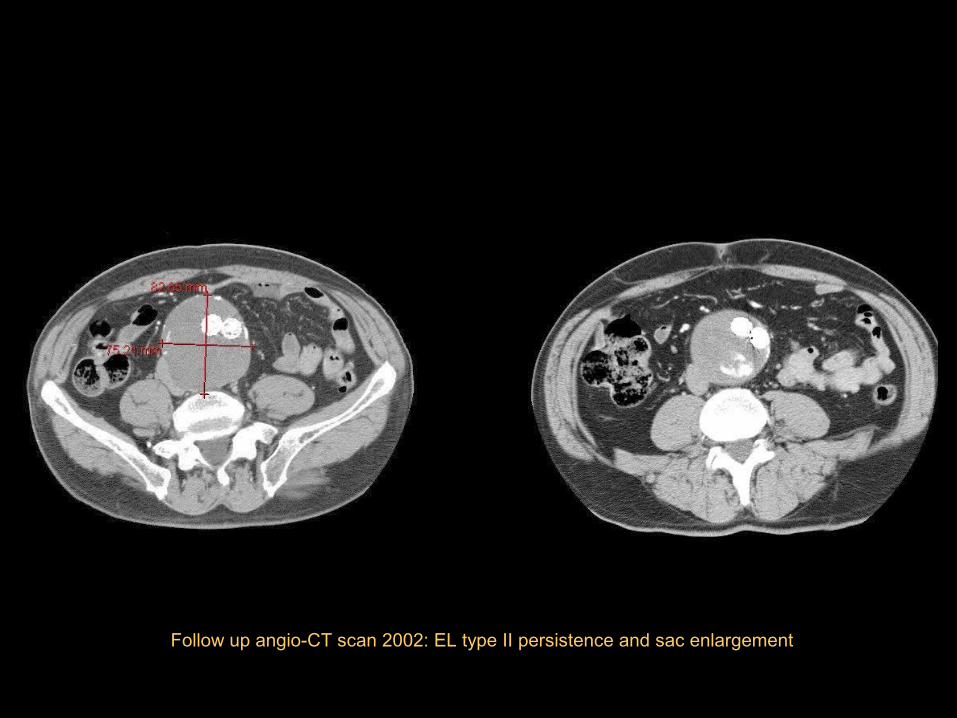
Follow up angio-CT scan 2002: EL type II persistence and sac enlargement
After ECD detectment of EL type II persistence with sac enlargement,
the patient underwent surgical convertion with
aneurysmatic sac opening, graft removing
and substitution with byfurcated graft


Type II Endoleak
Z.A. female, 83 years old
Multiple cardiovascular disease
ASA 3
2004 Aorto-Bisiliac Stent Graft TALENT (2616155-1418105)
in follow up with ECD for type II endoleak
2011 for type II EL persistence with sac enlargement
translumbar CT managed sac thrombization with fibrin glue

Follow up angio-CT scan 2011 : type II EL persistence and sac enlargement

Follow up angio-CT scan 2011: EL type II persistence and sac enlargement
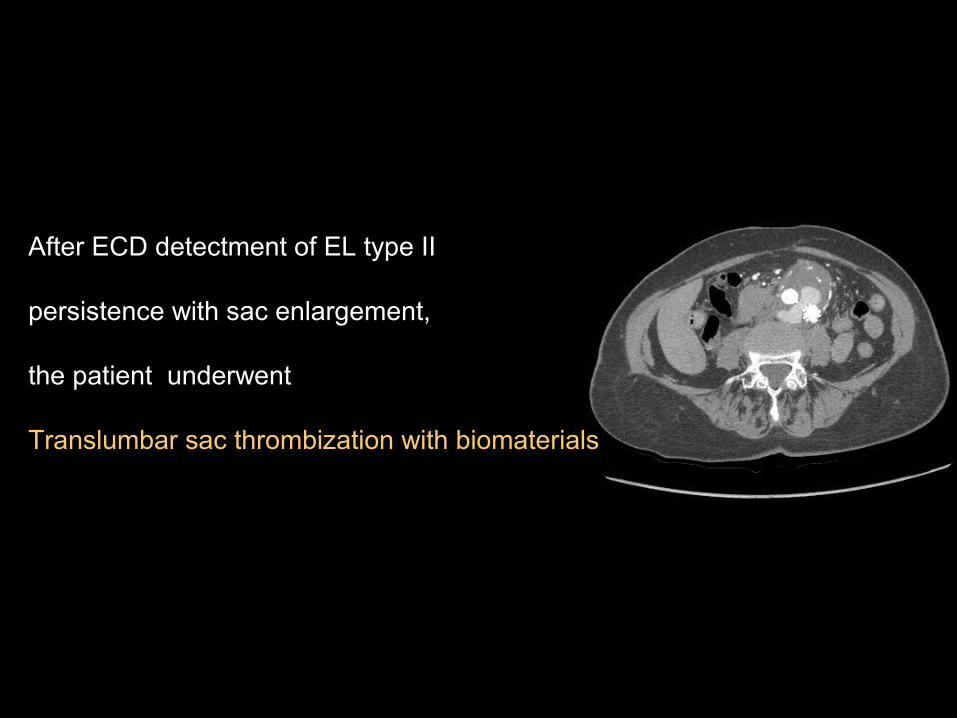
After ECD detectment of EL type II
persistence with sac enlargement,
the patient underwent
Translumbar sac thrombization with biomaterials
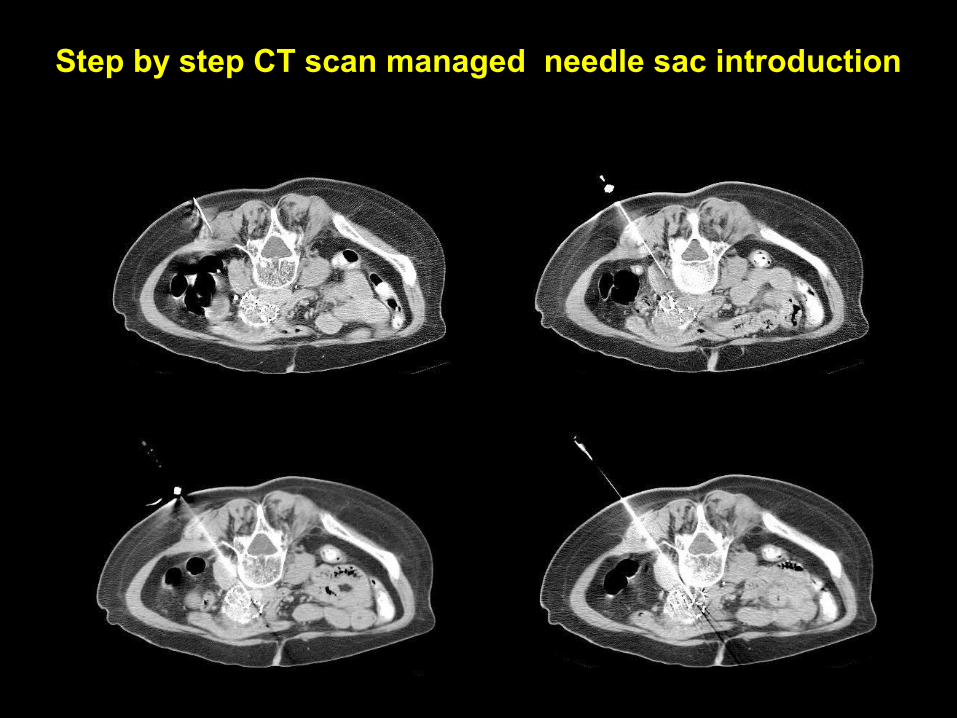
Step by step CT scan managed needle sac introduction
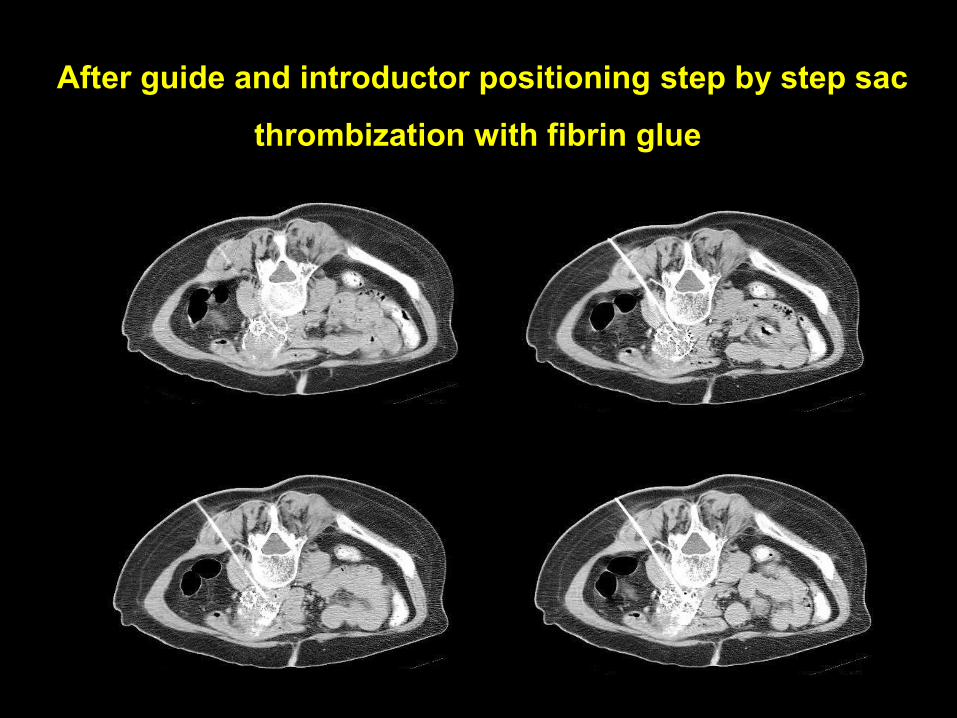
After guide and introductor positioning step by step sac
thrombization with fibrin glue
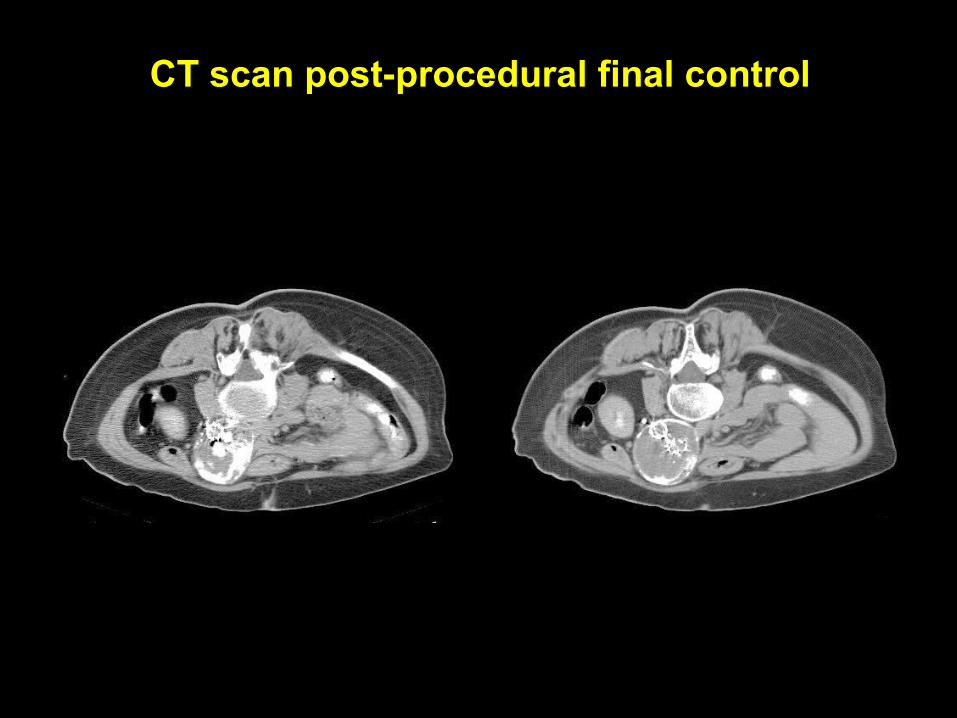
CT scan post-procedural final control

One week post procedural CT scan control

Follow up angio-CT scan 2010 : EL type II
persistence with sac refilled by a lumbar artery
One week follow up post procedural
angio-CT control scan with EL II resolution
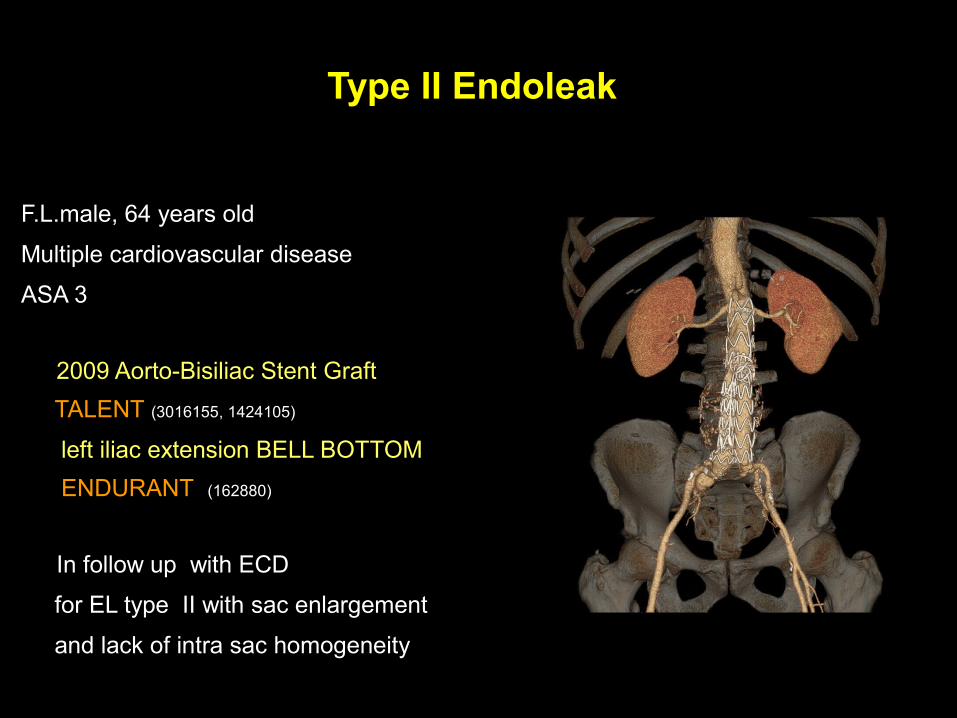
Type II Endoleak
F.L.male, 64 years old
Multiple cardiovascular disease
ASA 3
2009 Aorto-Bisiliac Stent Graft
TALENT (3016155, 1424105)
left iliac extension BELL BOTTOM
ENDURANT (162880)
In follow up with ECD
for EL type II with sac enlargement
and lack of intra sac homogeneity

Pre surgery angio-CT scan

Follow up ECD: EL type II persistence, sac enlargement and lack of intra sac homogeneity

Follow up angio CT scan which shows sac enlargement
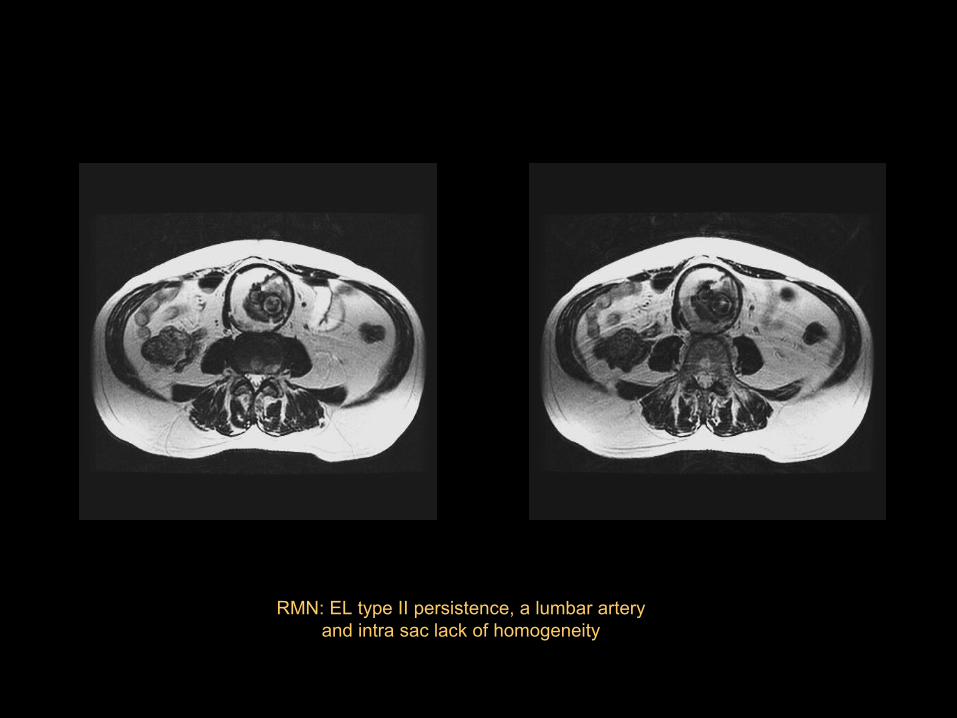
RMN: EL type II persistence, a lumbar artery and intra sac lack of homogeneity

2011 for EL type II persistence with sac enlargement the patient underwent
transabdominal echoguided sac thrombization with fibrin glue
followed by emergency surgical conversion after 24 hours due to sac rupture

Step by step echo-guided
transabdominal sac thrombization with fibrin glue
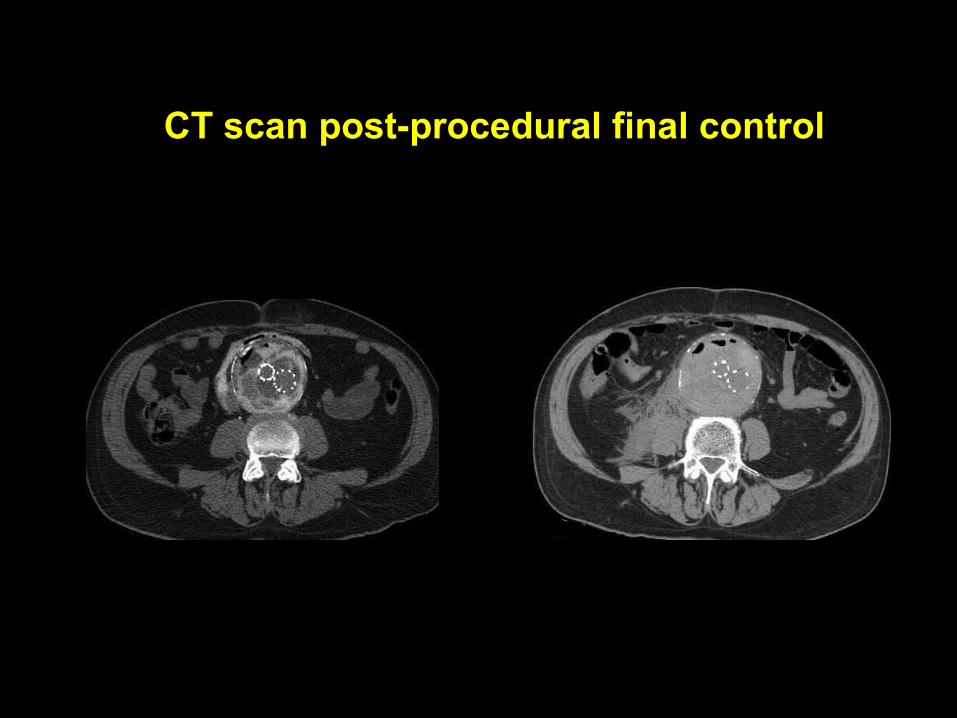
CT scan post-procedural final control
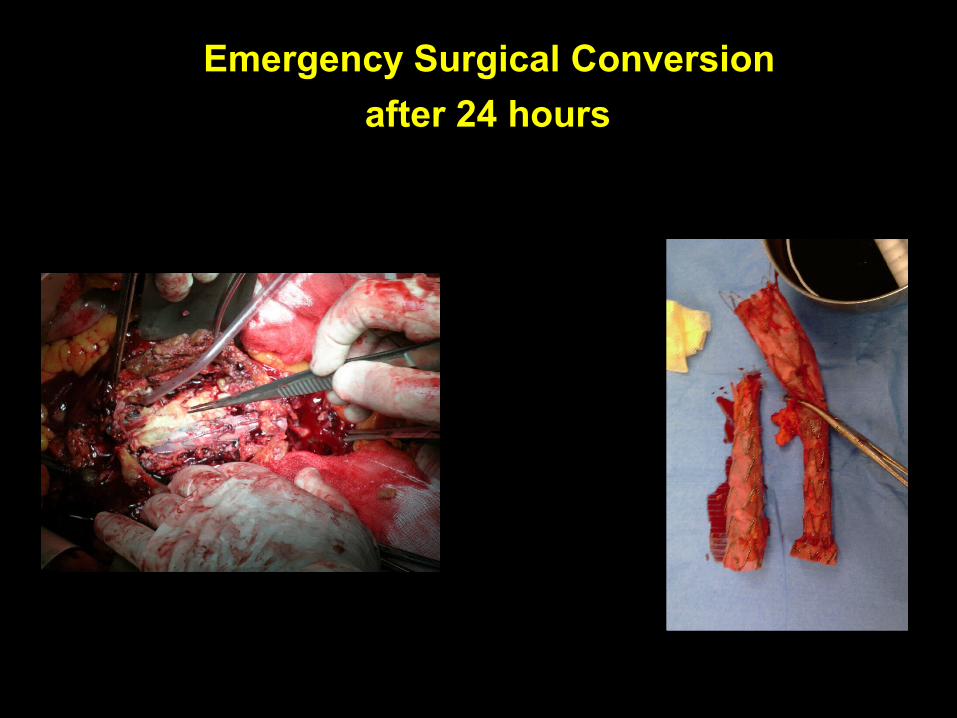
Emergency Surgical Conversion
after 24 hours

Emergency Surgical Conversion after 24 hours
10 cases treated in more than 10 years’ experience:
► 3 immediate complete convertion
► 4 convertion after unsuccessful lumbar trans-arterial embolization
► 1 patient in follow up for an EL II had a progressive aneurysmatic sac and proximal
neck enlargement with the main body partially slipping, developed an EL IA treated with intra-sac coils insertion plus a fibrin glue injection and proximal aortic cuff positioning
► 1 emergency convertion after unsuccessful echoguided transabdominal fibrin glue injection
► 1 successful CT managed translumbar thrombization with fibrin glue
Our experience in EL II with sac enlargement treatment
► After a EL II diagnosis many clinicians assume a ‘‘wait and see’’ approach with
regular follow- up when there is no expansion of the aneurysm sac
► The treatment of type II endoleak causing sac enlargement is always difficult,
dangerous, and almost always ends with a surgical conversion.
We propose
Aneurysm sac ‘‘thrombization’’ and stabilization in EVAR:
a technique to reduce the risk of type II endoleak
Ronsivalle S et al Aneurys sac “Thrombization” and Stabilization in EVAR : a technique to reduce the risk of Type II Endoleak.
J Endovasc. Ther. 2010; 17: 517-524
Ronsivalle S et al. Type II Endoleak: From Treatment of a Complication to prevention J Edovascular Ther 2012;19:128–130
Biomaterials
FIBRIN SEALANT is a fully absorbable biologic adhesive matrix made
of two main components
1) fibrinogen solution containing plasma coagulation proteins and
2) thrombin solution containing aprotinin (antifibrino-litic agent)
INCONEL (nickel and cobalt alloy) COILS are radiopaque, allow MRI scanning,
CT and CDU imaging
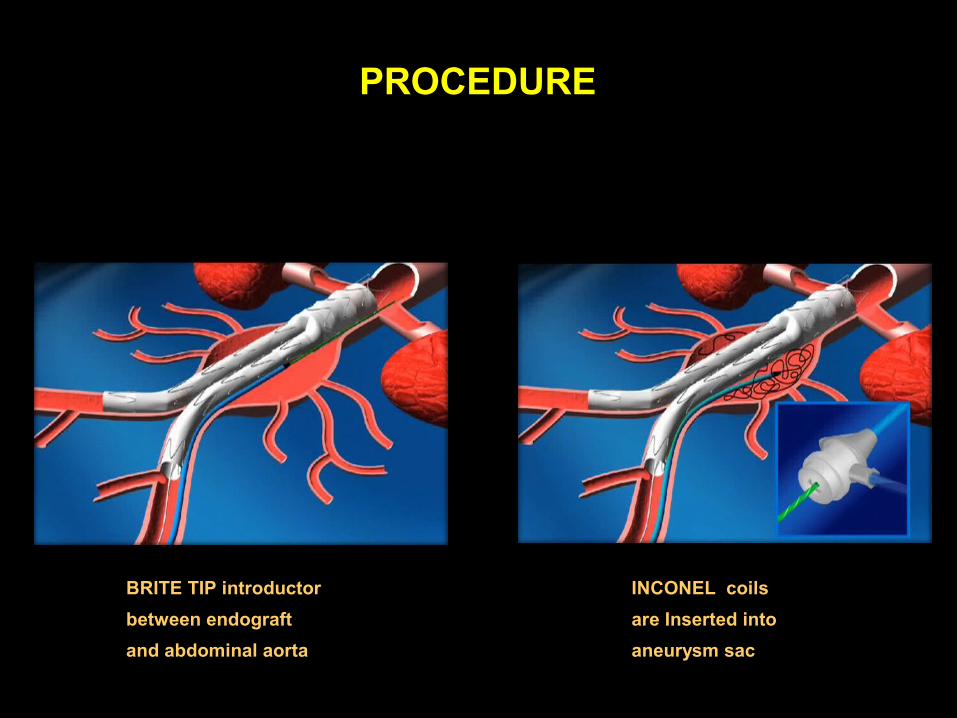
PROCEDURE
BRITE TIP introductor
between endograft
and abdominal aorta
INCONEL coils
are Inserted into
aneurysm sac

PROCEDURE
Fibrin glue injection into aneurysm sac Aneurysm sac thrombization

ANGIOGRAPHY DURING EVAR
Final angiography performed to verify sac thrombization and root occlusion of lumbar and inferior mesenteric arteries

CT SCAN
Control CT scan with evident inconel coils

September 1999 December 2010
608 patients underwent EVAR
September 1999 May 2003
228 pts: EVAR standard procedure
June 2003December 2006
131 pts: EVAR plus fibrin glue
January 2007December 2010249 pts: EVAR
plus inconel coils and fibrin glue
POPULATION

STUDY COHORT BASELINE DEMOGRAPHIC CHARATERISTICS
Armando Olivieri MD, Department of Prevention - Epidemiology Unit
(N 228) (N 317)
MALE 213 (93.4%) 285 (91.6%) §
FEMALE 15 (6.6%) 32 (8.4 %) §
AGE (YEARS) + SD 71.8 ± 8.5 72.1 ± 7.5 **
SMOKE 53 (23.2%) 53(13.9%) *
FAMILIARITY FOR AAA 2 (0.8%) 21 (5.5%) §
CHRONIC RENAL FAILURE 54 (23.7%) 100 (26.3%) §
CAROTID ARTERY DISEASE 91 (39.9%) 205 (53.9%) §
PERIFERIC ARTERY DISEASE 80 (35.1%) 64(13.8%) *
BMI > 30 47 (20.6%) 73(19.2%) §
HYPERTENSION 193 (84.6%) 356 (93.7%) *
CARDIAC DISEASE 126 (55.3%) 221 (58.2%) §
DIABETES MELLITUS 41 (18.0%) 79 (20.8%) §
HYPERLIPIDEMIA 152 (66.7%) 303 (79.7%) *§ Pearson χ2 : p>0.05
** t-test : p>0.005
GROUP II EVAR plus thrombization
GROUP I EVAR alone

INCIDENCE RATE
Armando Olivieri MD, Department of Prevention - Epidemiology Unit
cohortperson-time
(months)fai lures (num)
rates (x 1000 person-months)
EVAR alone 18845 34 1,80
EVAR plus sac thrombization 15663 12 0,77
total 34478 46 1,33
Incidence rate was 1,80 rates * 1000 person-month for EVAR alone group and 0.77 rates * 1000 person-months for EVAR plus thrombization

KAPLAN MAYER SURVIVING CURVE
Armando Olivieri MD, Department of Prevention - Epidemiology Unit
0.0
00.
25
0.5
00.
75
1.0
0
cum
ulat
ive
prob
abili
ty
379 346 272 202 132 86 67 37 10 0 0 0EVAR plus thrombization227 188 175 168 163 156 150 141 132 110 56 38EVAR alone
Number at risk
0 12 24 36 48 60 72 84 96 108 120 132 144follow up in months
EVAR alone EVAR plus sac thrombization
log-rank test p=0.0000
Kaplan–Meier Curves for the Primary End Point (endoleak type II)
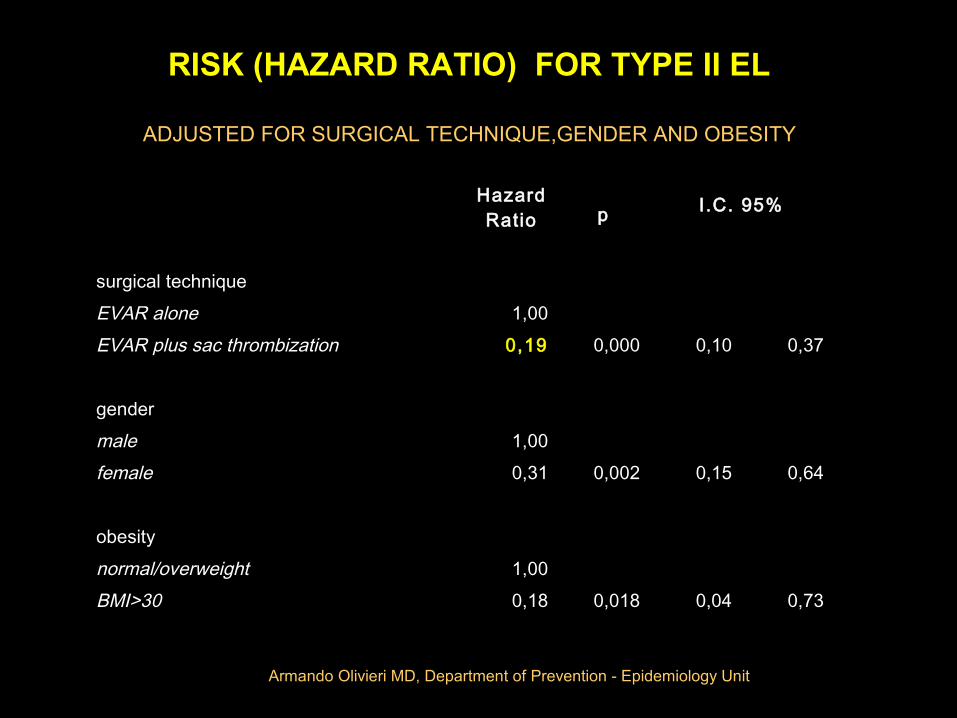
RISK (HAZARD RATIO) FOR TYPE II EL
ADJUSTED FOR SURGICAL TECHNIQUE,GENDER AND OBESITY
Armando Olivieri MD, Department of Prevention - Epidemiology Unit
Hazard Ratio p I.C. 95%
surgical technique
EVAR alone 1,00
EVAR plus sac thrombization 0,19 0,000 0,10 0,37
gender
male 1,00
female 0,31 0,002 0,15 0,64
obesity
normal/overweight 1,00
BMI>30 0,18 0,018 0,04 0,73

Prevention with biomaterials
is the best strategy to manage type II endoleak
► Reduces frequency of follow up Reduces frequency of follow up
► Increases Increases EVAR successEVAR success
► SimpleSimple
► Safe Safe
► Low costLow cost
► Independent Independent of stent graft used of stent graft used

Thank you





























