Embed Size (px)
Citation preview

0
Staying Ahead of Your Competitors in Evidence Based World – Models for Success
Seng C Tan
Regional Director, HEOR and RWE
IMS Health Asia, Singapore
5th Aug 2015

1
• What is RWE
• Why RWE
• Data Supply Issues
• Approach Overview
• Examples of Datasets in Asia
IMS Health Asia - RWE Stay Ahead
Agenda

2
What is RWE?
IMS Health Asia - RWE Stay Ahead

3
Intelligence is scattered with considerable efforts being required to optimally integrate insights across functions
IMS Health Asia - RWE Stay Ahead
Separate, disparate activities
We need a system instead
• A foundation of real-world data (RWD) from ever expanding sources
• Data that can be used for multiple purposes, consistently across the globe
• Innovative technology and analytic advances that quickly generate new insights
• Optimal organizational performance by tapping into uniquely rich insights
HEOR,
Medical
Drug
Safety Brand,
commercial
teams
OR
studies Pricing
and
market
access
DUS
study
Data-
base
subs
Data-
base
subs
Ad
boards PMR
Pricing
research
Switch
and
repeat
PV
study
Epi
studies
Patient
journey
Patient
journey
Data-
base
subs
Registry
EC
OS
YS
TE
M B
AC
KG
RO
UN
D

4
Vision for the Future: The RWE Ecosystem
IMS Health Asia - RWE Stay Ahead
An environment for building deeper insights to benefit the entire enterprise
Trial
optimization
Claims LRx
data Hospitals
Social
media
EMR
Survey Enriched
datasets
ePRO
Registries
pRCTs
EMR=
eCRF
HEOR/
Safety
R&D Commercial
EC
OS
YS
TE
M B
AC
KG
RO
UN
D

5 IMS Health Asia - RWE Stay Ahead
Broader Definition of RWE
ISPOR*
“…data used for decision-making
that are not collected in conventional
randomized
controlled trials (RCTs)”
Connected Healthcare
Many Stakeholders Asking Same
Questions Around Efficacy &
Value
Simply stated, real world
evidence is the application of real
world data to derive insights that
can be generalized to usual
settings

6 IMS Health Asia - RWE Stay Ahead
Evidence based journey of each patient could be mapped
The patient journeys in real life could be identified, linked and investigated to
answer the research questions

7 IMS Health Asia - RWE Stay Ahead
Definition of Real World Evidence (RWE)
RWE uses patient-level data to better assess the value of treatments and
services based on actual health outcomes and the total cost of care
Electronic Medical Records (EMR)
Claims Databases,
Healthcare
Registries/PROs
Fast-cycle Datasets
Identify Unmet Patient Needs
Comparative Effectiveness Studies
Deep-patient Segmentation
Better Understanding of Disease Dynamics
Meet Payer Needs for Proof of
Relative Value
Improved Drug Safety &
Monitoring
Data
Analysis
Insight
Clinical Commercial

8
Why RWE?
IMS Health Asia - RWE Stay Ahead
9 IMS Health Asia - RWE Stay Ahead
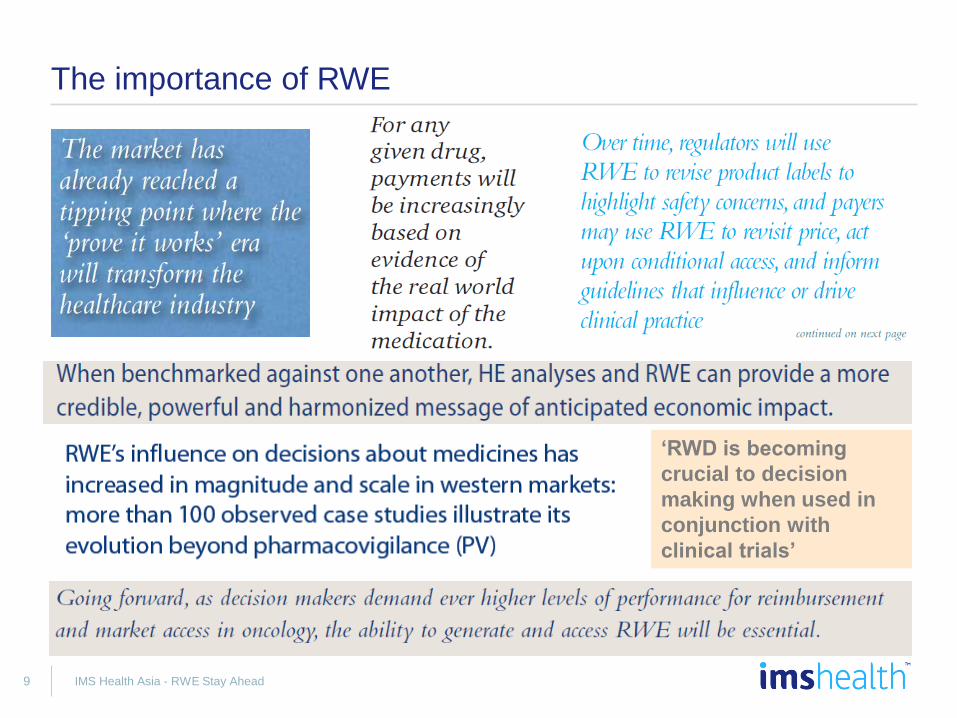
The importance of RWE
‘RWD is becoming
crucial to decision
making when used in
conjunction with
clinical trials’

10 IMS Health Asia - RWE Stay Ahead
RWE has been widely used in Western countries for different decision-making purposes
Therapy Area Brand Notes
Oncology Tysabri Tysabri was initially withdrawn from market due to serious adverse events but
was then re-introduced under CED as real world studies contributed to
demonstrating that benefits outweigh risks.
USA
CV Crestor AZ prevented the generic reference pricing of Crestor with a series of real
world studies demonstrating that Crestor was able to get more patients to
their LDL goal compared to generic simvastatin.
Italy
Parkinson Levodopa TLV reimbursed Levodopa at a premium price and granted provisional
reimbursement, conditional on the collection of RWE.
Sweden
Asthma Xolair MoH negotiated reimbursement only for patients who show improvement with
Xolair. Novartis will rebate full cost of treatment for all other patients.
Netherlands
Diabetes Byetta Payers agreed to provide provisional market access on the basis that Lilly
would monitor Byetta’s real life use, collect epidemiological and safety data
for P&R.
Italy
Oncology Avastin Full or partial reimbursement for patients in which the Avastin and Taxol
combination exceeded a specific total dosage in a study designed to test
whether the combination of both medicines could extend patient survival in
mBC and mRCC.
Germany
Schizophrenia Risperdal The full price of Risperdal funds were held in escrow until Janssen provided
proof of lower hospitalization costs from a 12-month real world study.
France
BPH Finasteride Full cost is reimbursed if patients prescribed finasteride subsequently
required surgery for benign prostatic hyperplasia after one full year of medical
therapy.
Canada
LEMS Firdapse PCTs refused access to the first licensed treatment for LEMS because of real
world use of an unlicensed therapy.
UK

11 IMS Health Asia - RWE Stay Ahead
Creating patient centered evidence based value
RWE generated from ‘Big Data’ is the healthcare’s most powerful currency via
objective understanding and robust analyses on health outcomes, costs and
quality
Payer Patient Provider
Pharma

12 IMS Health Asia - RWE Stay Ahead
RWE could answer the questions of different stakeholders
Meet commitments
Add to the safety profile
Evaluate efficacy to
improve patient outcomes
Prove value
Secure reimbursement
Enhance understanding of
unmet patient needs
Explore new indications
Generate publications
Industry Regulators Payers Providers Patients
Drug
candidates Market
Access
Detect safety signals
Ensure long-term
effectiveness
Determine value and
coverage
Monitor usage within
criteria
Cost-effectiveness
Obtain locally relevant
evidence
Advance science
Improve care
Ensure continued
reimbursement
Generate publications
My own health- what
choices do I have?
What are the
risks/benefits?
Which treatment will
improve my quality of
life?
Which treatment is
safer, more convenient
and affordable?
13
Data Supply Issues
IMS Health Asia - RWE Stay Ahead

14 IMS Health Asia - RWE Stay Ahead
Data Supply Issues: availability, completeness, quality and gaining trust of data owners are the main challenges in Asia
Data availability and completeness
• Only few providers have established RWD system
• Certain datasets lack the clinical richness required for certain evidence generation
• Variables such as costing for each resource use are not part of the database
Data confidentiality and security
• Variation in privacy laws and definition of patient identifiable information
• Lack of awareness on appropriate de-identification techniques
• Inadequate data governance standards
Trust
• Unwilling to allow or may improve access restrictions
• Data owners are not ready to build a trust with non-academic 3rd parties to enable optimal data use
Quality
• ‘Dirty Data’ – a mix of structured, semi-structure and unstructured information
• Large volume of free-text physician notes
• Data might be stored in multiple systems using different standards and formats even within the same care setting
Data Supply Issues

15
Approach Overview
IMS Health Asia - RWE Stay Ahead

16 IMS Health Asia - RWE Stay Ahead
Real World Evidence Beyond Real World Data
REAL-WORLD DATA (RWD)
Mortality,
other registries
Hospital visits,
service details Test results,
lab values,
pathology results
Pharmacy
data
Electronic medical and
health records
Claims
databases
(government and
payer)
Social
media
Consumer
information
Pharmaceuticals data
Meaningful questions
Fit-for-purpose data &
analytics
Externally validated findings
REAL-WORLD DATA
REAL-WORLD EVIDENCE (RWE)
Real-World Evidence as a capability—data,
tools, processes, organization—underpinning several
functions to drive business intelligence

17 IMS Health Asia - RWE Stay Ahead
A number of key research questions could be answered in well designed and executed RWE project
Commercial should lead the direction of the research with expertise inputs from other key
stakeholders such as medical, HEOR and MA
RWE Q1: Epidemiology and characteristics of
Disease X population
1.1 Incidence and
prevalence
1.2 Demographics
1.3 Characteristics of
patient frequently re-
admitted for
condition Y
1.4 Standard of care
in Disease X and
impact on outcomes
RWE Q2: Treatment Patterns
and Compliance
2.1 Treatment
algorithm and switch
analysis
2.2 Compliance with
treatment guidelines
2.3 Patient
adherence and
persistence with
existing treatments
2.4 Dose escalation
and de-escalation
analysis
RWE Q4: Effectiveness and
Safety
4.1 Comparative
effectiveness of
different treatments
4.2 Mortality
outcomes by
treatments
4.3 AE comparisons
across different
treatments
4.4 Resource use,
LOS and costs
associated with
different treatments
4.5 Use of rescue
therapy
RWE Q3: Predictors of
Outcomes
3.1 Prognostic
factors for in-hospital
cases
3.2 Biomarker as a
predictor of
outcomes and
resource use
3.3 Relationship
between LOS;
compliance, re-
admission and
mortality
3.4 Adverse events
and other
complications
RWE Q5: Burden of Disease X
5.1 Cost of treating
Disease X
5.2 Life years lost
5.3 Patient reported
outcomes with
Disease X
5.4 Productivity loss
5.5 Burden to
caregivers

18 IMS Health Asia - RWE Stay Ahead
Multiple data sources will be linked into a Data Platform
A cross-disciplinary matrix team is always led by CoE RWE with local and external expertise
inputs to design and plan a RWE project

19 IMS Health Asia - RWE Stay Ahead
Illustration: Unique possibilities in oncology linked data

20 IMS Health Asia - RWE Stay Ahead
IMS Health has identified the potential retrospective datasets available in the region for RWE projects
A team in IMS Health conducted a comprehensive systematic literature review to identify
and investigate datasets used published retrospective studies across Asia Pacific region
• The number of publications varies different across the countries with Australia, Korea, China and Taiwan having the largest number of publications
• For example, in the case of Taiwan, more than 550 publications using longitudinal patient data retrospectively
• A large number of publications available shows that the healthcare data of the country in the APAC region are increasingly analyzed and potentially utilized in policy making and P&R decision
• In certain countries such as South Korea and
Taiwan, claims data has been widely used and analyzed leading to high number of publications
• Nearly 50 databases have been identified for further investigation of their potential use to generate real world evidence in the region
Publications found on Pubmed. Avg: 470 publications
Publications found after deduplication Avg: 404 publications
Included papers Avg: 183 publications
No. of databases Avg: 48 databases
Duplicated publications
Excluded publications

21
Examples of Datasets in Asia (Applied in IMS Health Asia Projects)
IMS Health Asia - RWE Stay Ahead

22
Using the gov’t medical insurance database, we could obtain inpatient costs to analyze various hospitalization costs
IMS Health Asia - RWE Stay Ahead
How the data is captured
Scope of data
Hospital
Patients Medical
Insurance Account*
Provincial BoHRSS
China Health Insurance
Research Association
(CHIRA)
Employer
Contributions
Out-of-pocket
Portion under coverage cap
Sampling and data-tracking
Description:
• In-patient data that cover the costs associated with diagnostics, surgery, hospitalization fees and drugs
• It also includes patient age, sex, geography and length of hospital stay
• It does not include out-patient data
Coverage:
• 147 hospitals are sampled, which are distributed across 20 provinces and 4 autonomous regions
Data mix:
• The data specifies both reimbursed and out-of-pocket payment amount
Funding
Illustrative
Sit
e o
f C
are
Fu
nd
ing
Sou
rce
1 2

23
In CHIRA, the cost items, organized by ICD-10 diagnostic codes, for inpatient treatment in China
IMS Health Asia - RWE Stay Ahead
Key cost items for oncology…
A. Diagnosis
B. Inpatient
C. Prescription drugs
• X rays
• Clinical tests, including urine and blood tests, liver and renal function, FISH, IHC etc.
• Surgery
• Hospitalization
• Surgical materials
• Surgical drugs
• Chemo therapies
• Target therapy drugs
Cost area Cost items
…such cost items are organized by ICD-10 diagnostic codes
ICD-10 Oncology Type
Sample database

24
Overview of MDV Database in Japan
IMS Health Asia - RWE Stay Ahead
Panel
hospitals
Data
Category
1. Approx 130 DPC hospitals
2. Annual 2.5 million net patients
3. Both in-patients and outpatients
4. DPC E and F file, Form #1 (discharge summary), claim, laboratory data
5. Since April 2008, monthly update
Data Items
Details Caveats
• No University hospitals in the panel
• Typically approx half of the panels to be filtered out due to longitudinal incompleteness or lack of outpatient data
• Outpatient data not available with some panels
• Lab data available with 10% of the panel
• Lab data is only available for biochemical tests, i.e. blood and urine test (blood pressure not available)
6. Patient: Annonymized patient ID, age, gender
7. Institution: Specialty
8. Drug: Brand, form and strength based on drug code, daily dosage and duration (only for oral drugs)
9. Treatment: Treatment including test/check based on treatment code
10. Diagnosis: DPC diagnosis code (more category than ICD-10), ICD-10, first diagnosed date, treatment month
11. Hospitalization: Hospitalization date, discharge date, discharge summary
25
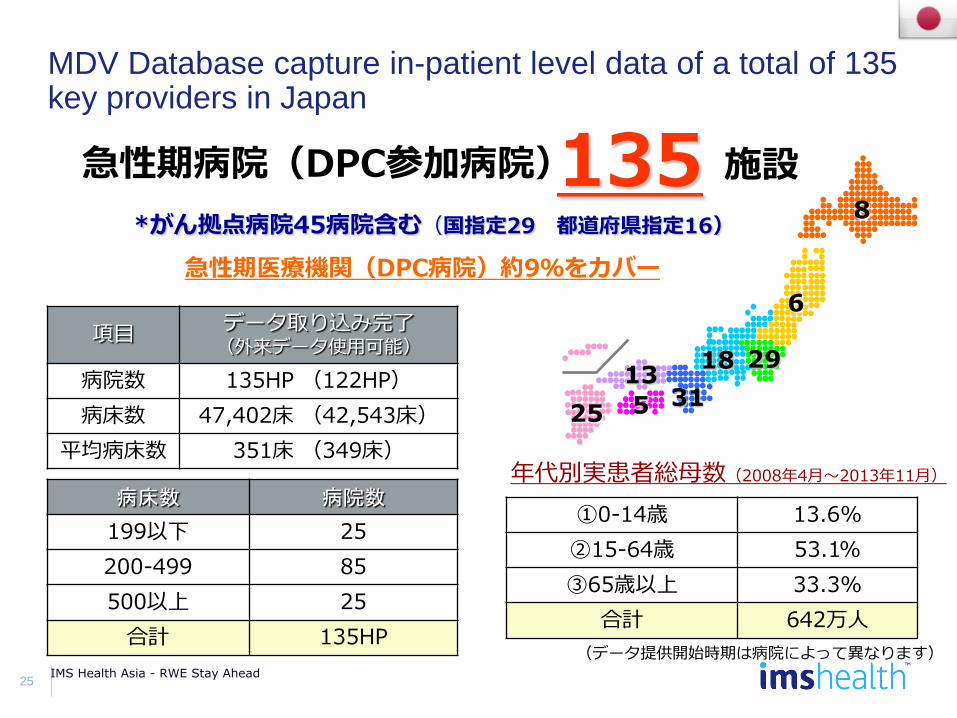
MDV Database capture in-patient level data of a total of 135 key providers in Japan
IMS Health Asia - RWE Stay Ahead
急性期病院(DPC参加病院) 135 施設
項目 データ取り込み完了 (外来データ使用可能)
病院数 135HP (122HP)
病床数 47,402床 (42,543床)
平均病床数 351床 (349床)
①0-14歳 13.6%
②15-64歳 53.1%
③65歳以上 33.3%
合計 642万人
年代別実患者総母数(2008年4月~2013年11月)
*がん拠点病院45病院含む(国指定29 都道府県指定16)
病床数 病院数
199以下 25
200-499 85
500以上 25
合計 135HP
急性期医療機関(DPC病院)約9%をカバー
(データ提供開始時期は病院によって異なります)
29
8
6
18
31 13
5 25

26
Public health insurance data is now open and shared by HIRA for research and analyses
IMS Health Asia - RWE Stay Ahead
• HIRA is a government agency and stands for Health Insurance Review and Assessment Service
• Aligns with the bigger agenda called ‘Government 3.0’ which aims to achieve a common goal by sharing government data where appropriate
− The two main objectives are ‘Providing customized services to individual citizens’ and ‘Creation of new national growth model through job creation’ through opening and sharing information
• All the government departments are to be evaluated by the degree of openness
• There are three data types
available from HIRA
− Treatment information data
− Patient sample data
• HIRA-NPS (National Patient Sample)
• HIRA-NIS (National Inpatient
Sample)
• HIRA-APS (Aged Patient Sample
with age≥65)
• HIRA-PPS (Child & Young people
Patient Sample with age<20)
− Pharmaceutical products distribution
information data (Sales data)
27
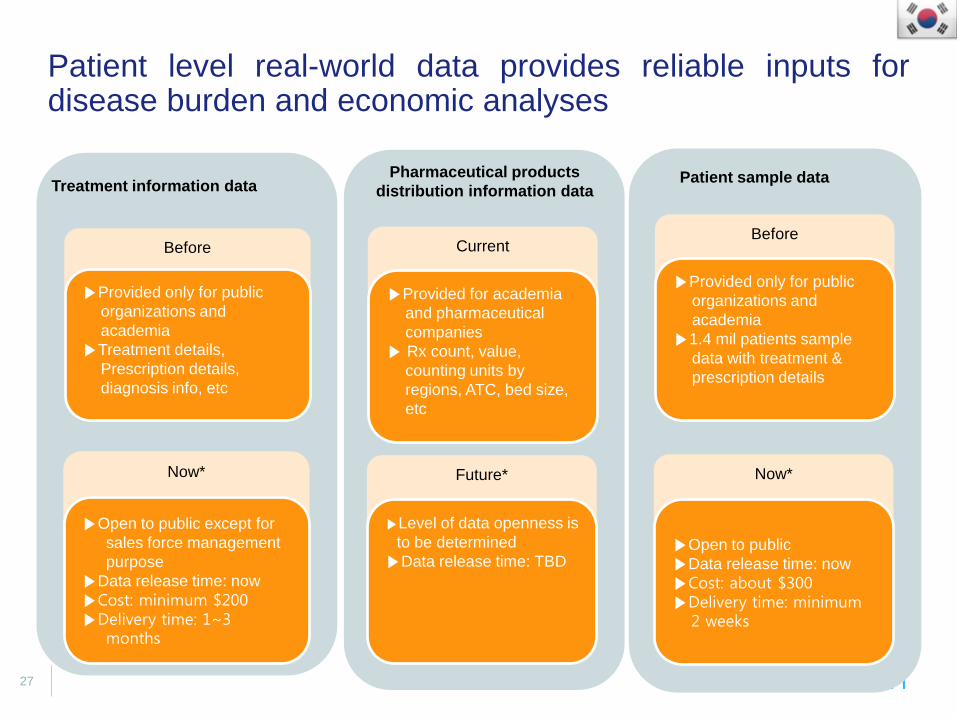
Patient level real-world data provides reliable inputs for disease burden and economic analyses
IMS Health Asia - RWE Stay Ahead
Treatment information data
Before
▶Provided only for public
organizations and
academia
▶Treatment details,
Prescription details,
diagnosis info, etc
Now*
▶Open to public except for
sales force management
purpose
▶Data release time: now
▶Cost: minimum $200 ▶Delivery time: 1~3
months
Patient sample data
Before
▶Provided only for public
organizations and
academia
▶1.4 mil patients sample
data with treatment &
prescription details
Now*
▶Open to public
▶Data release time: now
▶Cost: about $300 ▶Delivery time: minimum
2 weeks
Pharmaceutical products
distribution information data
Current
▶Provided for academia
and pharmaceutical
companies
▶ Rx count, value,
counting units by
regions, ATC, bed size,
etc
Future*
▶Level of data openness is
to be determined
▶Data release time: TBD

28
Patient level sample data is made available annually from NHIRD for research use
IMS Health Asia - RWE Stay Ahead
• Taiwan launched a single-payer
National Health Insurance Program on
March 1, 1995
• As of today, more than 23 million of
Taiwan’s 23.4 million population were
enrolled in this program
• National Health Insurance Research
Database (NHIRD) captured through
the electronic recording system set up
by the Bureau of National Health
Insurance, Taiwan (BNHI)
• The data derived from NHIRD has been increasingly used to provide real world evidence in drug
reimbursement listing as well as other policy decision-making
• Local economic evidence such as budget impact and cost-effectiveness analyses primarily rely
on the inputs reported and derived from the raw patient level NHRID data

29
Different data files and datasets have been created over the years for various research goals
IMS Health Asia - RWE Stay Ahead
Data Files
Monthly claim summary for inpatient claims (DT)
Monthly claim summary for ambulatory care claims (CT)
Inpatient expenditures by admissions (DD)
Details of inpatient orders (DO)
Ambulatory care expenditures by visits (CD)
Details of ambulatory care orders (OO)
Expenditures for prescriptions dispensed at contracted pharmacies (GD)
Details of prescriptions dispensed at contracted pharmacies (GO)
Major Datasets
Longitudinal Health Insurance Database 2010 (LHID2010)
- 1,000,000 beneficiaries, randomly sampled from the year 2010 Registry for Beneficiaries (ID) of the NHIRD
- everyone who was a beneficiary of the National Health Insurance Program during any period in 2010 could be randomly sampled
Specific subject datasets
- Based on a survey of the research community, specific research subjects were selected
- Examples include Traditional Chinese medicine dataset (CM), Cancer dataset (CN), Diabetes dataset (DB) etc

IMS Health Asia - RWE Stay Ahead
Contacts Seng Chuen Tan Director, HEOR IMS Health Asia Pacific Email: [email protected]