Embed Size (px)
Citation preview

Quality Lowers Cost: The Cost Effectiveness of a Multicenter Treatment Bundle for Severe Sepsis and
Septic ShockIntermountain Healthcare
Intensive Medicine Clinical ProgramHealthcare Delivery Research, Institute for Healthcare
LeadershipLydia Dong MD, MS

Disclosures
There is no any conflicts of interest or relevant disclosures for any of the authors

Introduction
• Sepsis occurs in 1% to 2% of all hospitalizations in the U.S.
• Severe sepsis and septic shock are leading cause of morbidity and mortality in Intensive Care Unit
• Published in-hospital mortality rate ranges from 40-60%
• Sepsis resulted in an aggregate healthcare cost of $20.3 billion in 2011
• Requires early detection and treatment for survival• Rapid identification, resuscitation and early evidence
based treatment is critical to best care and improved patient outcomes

Introduction (Cont.)
• A longitudinal quality improvement study in severe sepsis and septic shock patients was Initiated by Intensive Medicine Clinical Program (IMCP) (2004-2010)
• Sepsis bundles and related quality improvement initiatives yield improved bundle compliance and clinical outcomes (notably mortality), but the relationship of bundle compliance to fixed and variable healthcare costs is unclear
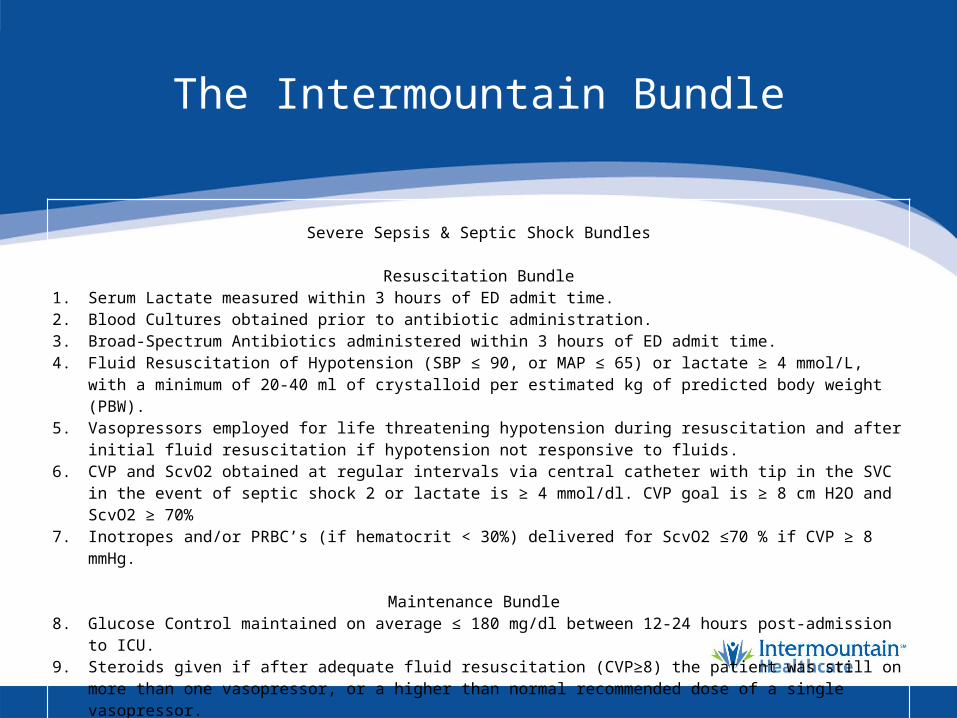
The Intermountain Bundle
Severe Sepsis & Septic Shock Bundles
Resuscitation Bundle
1. Serum Lactate measured within 3 hours of ED admit time. 2. Blood Cultures obtained prior to antibiotic administration. 3. Broad-Spectrum Antibiotics administered within 3 hours of ED admit time. 4. Fluid Resuscitation of Hypotension (SBP ≤ 90, or MAP ≤ 65) or lactate ≥ 4 mmol/L, with a minimum of
20-40 ml of crystalloid per estimated kg of predicted body weight (PBW). 5. Vasopressors employed for life threatening hypotension during resuscitation and after initial fluid
resuscitation if hypotension not responsive to fluids. 6. CVP and ScvO2 obtained at regular intervals via central catheter with tip in the SVC in the event of
septic shock 2 or lactate is ≥ 4 mmol/dl. CVP goal is ≥ 8 cm H2O and ScvO2 ≥ 70% 7. Inotropes and/or PRBC’s (if hematocrit < 30%) delivered for ScvO2 ≤70 % if CVP ≥ 8 mmHg.
Maintenance Bundle 8. Glucose Control maintained on average ≤ 180 mg/dl between 12-24 hours post-admission to ICU. 9. Steroids given if after adequate fluid resuscitation (CVP≥8) the patient was still on more than one
vasopressor, or a higher than normal recommended dose of a single vasopressor. 10. Drotrecogin Alfa Eligibility assessed for use employing hospital guidelines. 11. Use of a Lung Protective Strategy with Vt 6 ml/kg PBW and plateau pressures < 30 cmH20 for
mechanically ventilated patients.

Result and Conclusion from Our Previous Study
1. Miller RR, 3rd, Dong L, Nelson NC, et al. Multicenter implementation of a severe sepsis and septic shock treatment bundle. Am J Respir Crit Care Med. 2013;188(1):77-82.
Objectives
• To access the relationship between bundle compliance and healthcare cost in severe sepsis and septic shock patients

Study Design
• Observational study of a severe sepsis/septic bundle as part of multi-year longitudinal quality improvement study across multiple hospitals of an integrated healthcare organization (IH)
• Fully compliant care was defined as success toward 11 of 11 bundle elements.
Study Population and Data Sources
• Inclusion criteria• Patients 18 years or older• Diagnosed with severe sepsis or septic shock • Admitted to ICUs from the emergency
department (ED) or operating room• 10 IH hospitals with 10 EDs and 13 ICUs
• Web-based sepsis bundle data collection application and Intermountain Healthcare Enterprise Data Warehouse
Intermountain Cost Accounting System
• Consolidated hospital case mix database which is sourced from the corporate AS/400 production system.
• Total costs per patient were obtained through our enterprise charge master. The charge master contains variable and total costs for a standardized set of charge codes. Hospitals conduct annual / biannual costing studies to determine the variable and total cost for charge codes.
1. Roberts RR, Frutos PW, Ciavarella GG, et al. Distribution of variable vs fixed costs of hospital care. JAMA. 1999;281(7):644-9.

Cost Outcomes
• Total costs = Fixed + Variable Costs• Fixed Costs: Those costs that do not change due to
volume in a hospital or service. Examples include electricity, facility maintenance, property and equipment.
• Variable Costs: Those costs that do change with volume including salary, patient care supplies, medication and diagnostic supplies etc.

Primary Outcome
•Standardized total and variable costA weighted adjustment method based on the volume and inflation rate was applied to standardize the costs and charge amounts for each charge code across facilities and years

Statistical Method
• A Generalized Linear Mixed Model with Gamma distribution and log link was independently performed to assess the association between standardized costs (total and variable) and treatment bundle compliance while controlling for patient age and Charlson Comorbidity Index Score (CCIS) stratified by severe sepsis and septic shock sub-groups.
• Facilities were treated as random effects.

Results
• 3910/3997 eligible patients had all data available and were enrolled from the 11 hospitals.
• Patients with bundle compliance had in-hospital mortality of 10.6% (n = 224 of 2118) versus 13.0% (n = 233 of 1792, p = 0.02) for those who did not receive fully compliant care.
• Patient characteristics, outcomes and standardized costs by severity of sepsis are shown in Table 1-4.
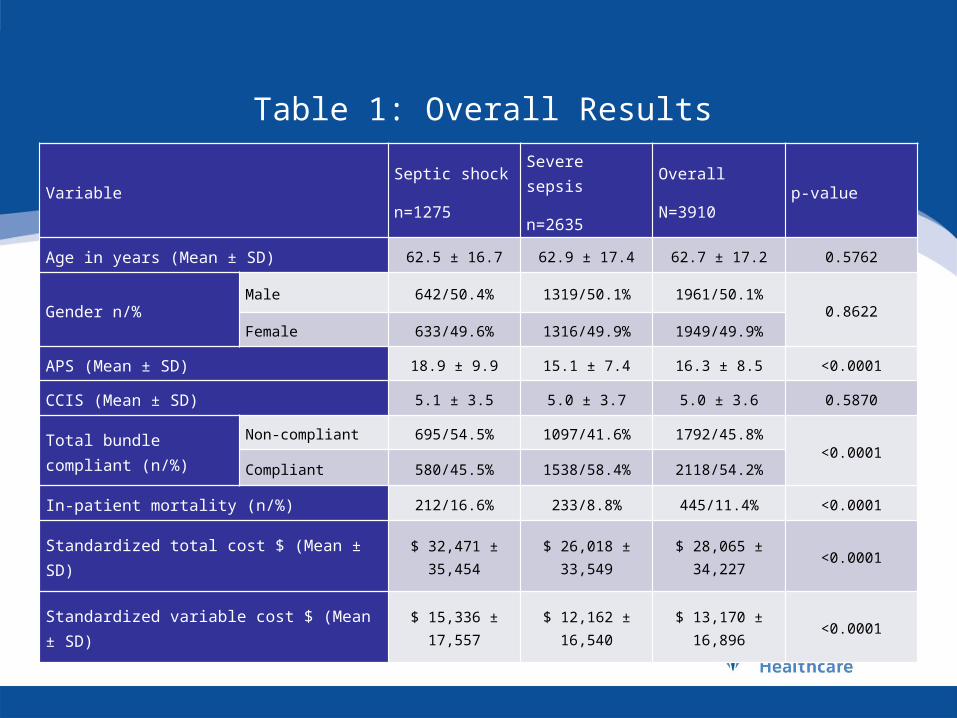
Table 1: Overall Results
VariableSeptic shock
n=1275
Severe sepsis
n=2635
Overall
N=3910p-value
Age in years (Mean ± SD) 62.5 ± 16.7 62.9 ± 17.4 62.7 ± 17.2 0.5762
Gender n/%Male 642/50.4% 1319/50.1% 1961/50.1%
0.8622Female 633/49.6% 1316/49.9% 1949/49.9%
APS (Mean ± SD) 18.9 ± 9.9 15.1 ± 7.4 16.3 ± 8.5 <0.0001
CCIS (Mean ± SD) 5.1 ± 3.5 5.0 ± 3.7 5.0 ± 3.6 0.5870
Total bundle compliant (n/%)
Non-compliant 695/54.5% 1097/41.6% 1792/45.8%<0.0001
Compliant 580/45.5% 1538/58.4% 2118/54.2%
In-patient mortality (n/%) 212/16.6% 233/8.8% 445/11.4% <0.0001
Standardized total cost $ (Mean ± SD) $ 32,471 ± 35,454
$ 26,018 ± 33,549
$ 28,065 ± 34,227 <0.0001
Standardized variable cost $ (Mean ± SD) $ 15,336 ± 17,557
$ 12,162 ± 16,540
$ 13,170 ± 16,896 <0.0001

Table 2: Cost Results by Severity of Sepsis
Cost variable Severity of sepsis
Total bundle compliantp
Non-compliant Compliant
Standardized total cost ($)
Septic shock 32,498 ± 35,487 32,440 ± 35,445 0.9767
Severe sepsis 28,021 ± 40,301 24,589 ± 27,672 0.0096*
Non-Standardized total cost ($)
Septic shock 26,868 ± 29,915 27,278 ± 29,453 0.7604
Severe sepsis 21,940 ± 31,737 20,858 ± 24,211 0.3211
Standardized variable cost ($)
Septic shock 15,304 ± 17,475 15,375 ± 17,670 0.9426
Severe sepsis 13,134 ± 19,892 11,468 ± 13,619 0.0108*
Non-Standardized variable cost ($)
Septic shock 14,236 ± 16,367 14,492 ± 16,551 0.7824
Severe sepsis 11,871 ± 18,212 10,515 ± 12,475 0.0234*

Table3. GLMM with Standardized Total Cost
Model with Total Cost in Severe Sepsis
Model with Total Cost in Septic Shock
Model Estimate p-value Estimate p-value Intercept 9.7884 <0.0001 9.7960 <0.0001Total bundle (not compliant)
0.1092 0.0237* 0.0097 0.8667
Age group
18-29 0.0233 0.8374 0.3075 0.0427
30-39 0.2967 0.0138 0.4017 0.002040-49 0.3693 <0.0001 0.2123 0.051650-59 0.1604 0.0385 0.3667 <0.000160-69 0.2464 0.0007 0.0885 0.003870-79 0.0879 0.2237 0.0888 0.0644>80 Ref. Ref.
CCIS 0.0095 0.1502 0.0217 0.0066Saving with bundle per case
$2,557 (95% CI: $2,110, $3,096)
(~11% saving)
No saving

Table4. GLMM with Standardized Variable Cost
Model with Variable Cost in
Severe Sepsis
Model with Variable Cost in Septic Shock
Model Estimate p-value Estimate p-value Intercept 8.9873 <0.0001 9.0079 <0.0001Total bundle (not compliant)
0.1193 0.0182* 0.0082 0.8908
Age group
18-29 0.0163 0.8909 0.3381 0.0319
30-39 0.3179 0.0116 0.4144 0.002140-49 0.4002 <0.0001 0.2363 0.036950-59 0.1627 0.0448 0.3665 0.000160-69 0.2563 0.0007 0.2614 0.004570-79 0.0893 0.2377 0.1662 0.0716>80 Ref. Ref.
CCIS 0.0125 0.0725 0.0233 0.0049Saving with bundle per case
$1,288 (95% CI: $1,055, $1,572)
~12%
No saving

Results (Cont.)
• Implementation of sepsis bundle in severe sepsis patients saved 11% ($2,557, 95% CI: $2,110 - $3,096) in standardized total cost and 12% ($1,288, 95% CI: $1,055 - $1,572) in standardized variable cost after controlling patient age and CCIS per case. Total $4.6 million saving over the study period
• No savings in septic shock patients after implementing sepsis bundle
Conclusions
• In this study, sepsis bundle compliance is associated with improved mortality and lower costs (total and variable) in hospitalized patients with severe sepsis but not in patients with septic shock.
• While it remains unclear why the effect was only seen in patients with severe sepsis, there appears to be an important correlative relationship between clinical quality and costs even in complex medical treatments.(1,2)
1. Chalupka AN, Talmor D. The economics of sepsis. Critical care clinics. 2012;28(1):57-76, vi.2. Lagu T, Rothberg MB, Shieh MS, et al. Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Critical care medicine. 2012;40(3):754-61.

Limitations
• Single system with unique TD-ABC capabilities• Sub-optimal bundle compliance for the entire six
years of the study• No QALY (Quality-adjusted Life-year) calculations
Acknowledgements
• Todd Allen, MD (ED Development Team Medical Chair )
• Terry Clemmer, MD (IMCP Medical Chair)• Nancy Nelson (IMCP Operation Director)• Danny Probst (IMCP Data Manager)• Andrew Merrill (Statistician)• Russell R. Miller III M((Critical Care Development
Team Medical Chair)

Thank you !





























