Embed Size (px)
Citation preview

Self-Care: An Ethical Imperative
Kimberly Richards, Psy.D.
Jesse Matthews, Psy.D.
Angela O’Neill, B.A.

Introductions
Jesse Matthews, Psy.D.
Licensed psychologist in private practice; contract in community mental health, forensic, and nursing homes; adjunct faculty
Chair, PPA ECP Committee
Kimberly Richards, Psy.D.
Licensed psychologist in private practice
PPA ECP Committee member
Angela O’Neill, B.A.
Psychology doctoral student- Immaculata University

Overview
Self-care
Current research
Distress, burnout, and compassion fatigue risk factors
Self-care and work-life balance
Ethics and self-care
Impaired professionals
Psychologist suicide
Prevention
Intervention
Follow-up
Impact of psychologist suicide on colleague survivors and clients

Self-care
Vital for well-being (and not just for psychologists)
An ongoing process involving trial and error
Many different ways to do it
Needs vary as a function of individual differences
Includes multiple dimensions
“Can be considered in terms of self-awareness and self-regulation in the service of balancing our psychological, physical, and spiritual needs; connection between our self and others; and our personal and professional selves; interacting in infinitely complex ways” (Baker, 2003)
EVERYONE deserves it.

http://livingmorefully.com/3-top-self-care-tips-create-balance-enjoy-life/

http://www.drbeckybeaton.com/uploads/2/1/6/0/21608682/7722006.png?1372969682

http://501resourcemanual.weebly.com/uploads/1/8/9/3/18938345/2493521_orig.gif
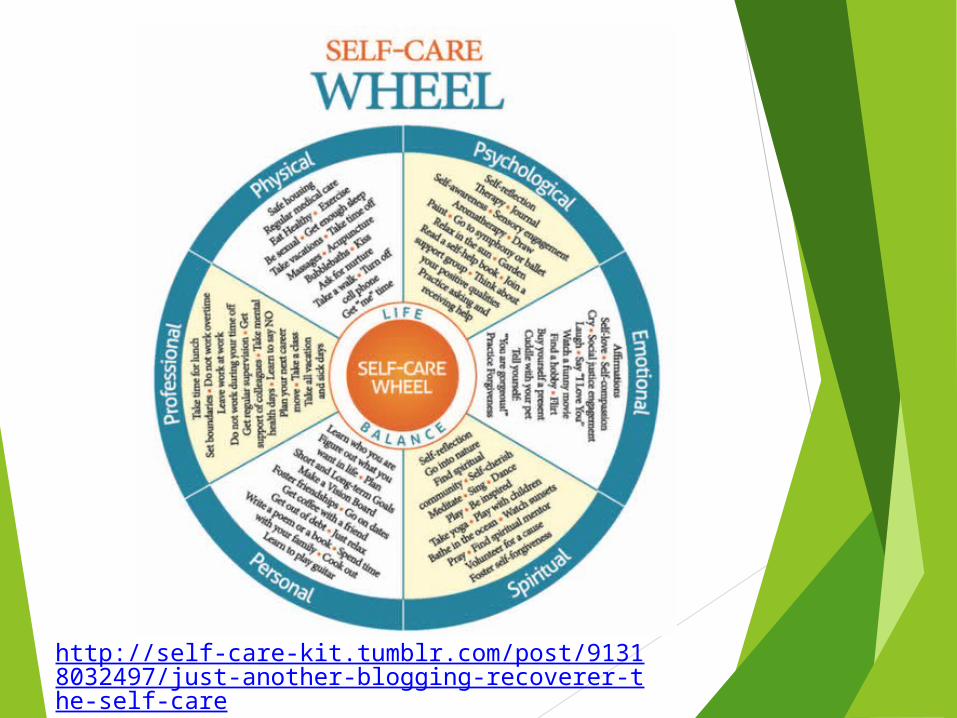
http://self-care-kit.tumblr.com/post/91318032497/just-another-blogging-recoverer-the-self-care

7 Types of Self-Care Strategies for Coping with Stress (Markway, 2014)
1. Sensory
Breathe, snuggle a cozy blanket, take a hot shower, get a massage, listen to music, burn a scented candle
2. Pleasure
Take yourself out to eat, be a tourist in your own city, watch a show or movie, write or draw
3. Mental/Mastery
clean out a drawer or closet, take one small step toward something you have been avoiding, try a new activity, do a crossword puzzle or word search, play a video game
4. Spiritual
meditate, pray, list 5 things you are grateful for, attend a religious service


7 Self-Care Strategies (continued)
5. Emotional
cry when you need to, write your feelings down, accept your feelings, laugh
6. Physical
go for a walk or run, dance, stretch, ride a bike, get enough sleep
7. Social
get lunch with a friend, call or text a friend, join a group (support group, book club, sports team, etc.)

2 Types of Self-Care
Macro self-care
Strategies we typically think of, which often require substantial investment of time, effort, or money
e.g. take a vacation, play golf, work out at a gym, meditate for 40 minutes daily, go to a play or concert
May suggest that self-care needs to be a big, life-changing project- can feel overwhelming and bad
Micro self-care
Available at all times, on demand
Spontaneous, brief practices
Making small changes with reliable frequency
e.g. 5 minutes of mindfulness meditation, progressive muscle relaxation, visualization, push-ups

Self-Care Resources APA Advisory Committee on Colleague Assistance
(ACCA), July 2010. Tips for Self-Care: http://www.apapracticecentral.org/ce/self-care/acca-promoting.aspx
Baker, E. (2003). Caring for ourselves as psychologists. National Register of Health Service Psychologists. http://www.e-psychologist.org/index.iml?mdl=exam/show_article.mdl&Material_ID=1
Boyes, A. (2013). 17 self-care tips from the experts: https://www.psychologytoday.com/blog/in-practice/201302/17-self-care-tips-the-experts
North American Drama Therapy Association (2015). Self-care for therapists. http://www.nadta.org/membership/selfcare-for-therapists.html
Tartakovsky, M. (2013). How clinicians practice self-care & 9 tips for readers. PsychCentral. http://psychcentral.com/lib/how-clinicians-practice-self-care-9-tips-for-readers/

So why would practicing self-care ever be a problem?
We’re busy! (time constraints)
We have many patients counting on us, some more demanding than others.
We’re always multi-tasking- assessing, treating, assisting, doing administrative tasks, researching, teaching, learning, presenting, marketing, networking, etc.
Many of us work more than one job (balancing- one inevitably creeps into another).
Our work is mentally taxing.
We’re perfectionistic.
We have difficulty setting limits.
We have financial obligations (office expenses, mortgages, families, student loans, etc.) or constraints (seeing many low-fee clients, income may be unstable).
It feels selfish
We’re always putting it off

The reality… We are taught in school to care for others, but not
to care for ourselves.
It may get talked about, but the existing system does not support or reward self-care.
The life of an early career psychologist is also not conducive to self-care.
Even for seasoned psychologists, you need to play your cards right to achieve the balance you want.
“Burnout is the rule, not the exception when you aren’t taking care of yourself” …“To enjoy a long, healthy, and satisfying career, you must begin today to practice intentional self-care.” http://careersinpsychlogy.org/experts-discuss-need-self-care/
“If we follow our own advice, everyone benefits.” http://www.apapracticecentral.org/ce/self-care/acca-promoting.aspx

Current Research Bamonti et al. (2014) sampled 177 programs-
handbooks were available online for 136 (76.8%) of them; of these, 15 (11.0%) had an available general psychology department handbook that referenced self-care and 44 (32.4%) had an available clinical psychology training area handbook with such a reference.
A simple reference to psychotherapy or mental health services for impaired students was the most common self-care theme observed.
Researchers suggested that graduate programs adopt clearly articulated and readily accessible self-care statements as well as institutionalized self-care practices that are encouraged and/or supported by faculty and administration.
A call to action urges psychology training programs to consider initiating a shift from cultures of self-care that are reactive in nature to ones that instead are proactive and preventive, with a focus on wellness.

Current Research
Myers et al. (2012) examined self-care practices and perceived stress among psychology graduate students
488 psychology graduate students from across the US completed an anonymous survey of self-care practices and stress.
Multiple regression analyses indicated that sleep hygiene, social support, emotion regulation, and acceptance within a mindfulness framework were significantly related to perceived stress.
Results suggested that educating students about self-care practices can be an integral part of helping students manage stress associated with clinical training.

Current Research Boellinghaus, Jones, and Hutton (2013): 12 trainee
therapists who had previously attended a mindfulness-based cognitive therapy course took part in a six-session loving kindness meditation (LKM) course and were interviewed about their experience.
5 master themes were identified: (a) engaging with the practice, (b) impact on self, (c) impact on relationships, (d) bringing compassion into the therapy room, and (e) integrating LKM into life.
Participants perceived LKM to have led to increased self-awareness, compassion for self and others, and therapeutic presence and skills. At the same time, LKM was experienced as emotionally challenging.
Findings suggest that it may be useful to offer LKM to trainees as an approach to enhancing self-care and compassion, but that it should be taught with care, given its potential emotional impact.

Current Research Pakenham (2015) explored the utility of the acceptance and
commitment therapy (ACT) framework for identifying processes and strategies to enhance self-care in clinical psychology trainees (CPTs).
116 CPTs completed questionnaires in the first year of clinical training.
The ACT processes constituted the predictors: values, defusion (measured as thought suppression), mindfulness, and acceptance. The adjustment criterion variables included: stress, distress, life satisfaction, and clinical training satisfaction.
The ACT processes explained significant amounts of variance in all of the adjustment outcomes, and thought suppression, values, and acceptance each emerged as significant predictors of 1 or more of the outcomes.
With the exception of mindfulness, the ACT processes were related to better adjustment as predicted. The adverse effects of thought suppression were pervasive, whereas the beneficial effects of acceptance and values varied across adjustment outcomes. Acceptance had unexpected suppressor effects on mindfulness in regression analyses on distress and stress.
Findings support the utility of the ACT framework for explaining and enhancing adjustment and self-care in CPTs.

Current Research Wise, Hersh, and Gibson (2012) sought to expand the
conceptualization of psychologist functioning as embodied in the widely promulgated stress-distress continuum.
Through the incorporation of a positive dimension, they envisioned the potential for psychologists to spiral up via their practice of enhanced self-care.
4 foundational principles are interwoven throughout our consideration of effective self-care for psychologists: an emphasis on flourishing (rather than merely surviving), intentionality, an awareness of reciprocity in care of self and others and the benefits of integrating self-care into our daily practices and routines, rather than being added onto existing personal and professional obligations.
A review of literature on psychologist self-care, healthy lifestyles, mindfulness, acceptance-based therapies, and positive psychology informed their endorsement of mindfulness-based positive principles and practice (MPPP’s) for psychologists. These MPPP’s were broadly conceptualized as the how of effective self-care that supports the what (as in what to do) in this realm.

Risk Factors for Distress, Burnout, or Compassion
Fatigue Not setting boundaries- working during time off, constantly checking e-mail or voice mail, being overly flexible with scheduling, etc.
Isolation- spending too many hours doing clinical work, not consulting, not networking or socializing with colleagues, limited social relationships or time spent with loved ones
Working too much- too many clients in a row, too many challenging clients, too much of a single kind of work, not taking time off, etc.
Unhealthy coping mechanisms- relying on quick fixes like food, alcohol, drugs, the Internet, etc. to escape
Unrealistic expectations- believing you should be invulnerable, should be able to work at the highest level all of the time, and other “shoulds”

Risk Factors (continued)
Failing to address issues or to grow as a person- reading, participating in therapy, support groups, etc.
Failing to recognize the hazards of your profession- taking on clients outside of your competence, overdoing it with number of clients or hours, not consulting, feeling like a failure, not seeing blind spots, etc.
Allowing yourself to stagnate professionally- not challenging yourself to continue learning, not reading, staying in a position you dislike/hate, etc.
Neglecting self-care- not exercising or sleeping enough, poor diet, lack of spiritual or intellectual growth, not engaging in fun or replenishing activities, etc.
(Norcross & Barnett, 2007; Barnett, 2008)

What about Ethics?
American Psychological Association Code of Ethics: Standard 2.06: Personal Problems and Conflicts
(a) “Psychologists refrain from initiating an activity when they know or should know that there is a substantial likelihood that their personal problems will prevent them from performing their work-related activities in a competent manner.”
(b) “When psychologists become aware of personal problems that may interfere with their performing work-related duties adequately, they take appropriate measures, such as obtaining professional consultation or assistance, and determine whether they should limit, suspend, or terminate their work-related duties. (See also Standard 10.10, Terminating Therapy.)”
Standard 3.04 Avoiding Harm “Psychologists take reasonable steps to avoid harming
their clients/patients, students, supervisees, research participants, organizational clients, and others with whom they work, and to minimize harm where it is foreseeable and unavoidable.”

More about Ethics… PA Code of Ethics:
Principle 1 (h): “As practitioners, psychologists know that they bear a heavy social responsibility because their recommendations and professional actions may alter the lives of others. They are alert to personal, social, organizational, financial, or political situations and pressures that might lead to misuse of their influence.”
Principle 2 (i): “Psychologists recognize that personal problems and conflicts may interfere with professional effectiveness. Accordingly, they refrain from undertaking activities in which their personal problems are likely to lead to inadequate performance or harm to a client, colleague, student, or research participant. If engaged in the activity when they become aware of their personal problems, they seek competent professional assistance to determine whether they should suspend, terminate or limit the scope of their professional or scientific activities.”

Positive Ethics (Norcross & Barnett, 2007)
Focuses the psychologist on constantly striving to achieve the highest ethical standards of our profession.
Eschews efforts to do the minimum, to get by, to avoid negative outcomes.
Guided by a series of aspirational virtues that we strive toward throughout our careers:
Beneficence
Nonmaleficence
Fidelity
Autonomy
Justice
Self-care- providing adequate attention to our own physical and psychological wellness so that we are effectively able to implement the preceding virtues.

At a more basic level… Why would I want to study for X number of years,
paying (borrowing) Y number of dollars, sacrificing so much along the way… so that I could a) start my career many years later than my peers, b) work all of the time just to survive or to get “caught up”, c) continue to sacrifice, d) be completely miserable, and d) not really help anybody all that much???
I became a psychologist to:
help people (obviously)
have an intellectually stimulating career
do a fun job
lead a lifestyle I can be happy with
be my own boss and do the work that I find most rewarding.

Impaired Professionals

Introduction(Barnett, Baker, Elman, & Schoener, 2007)
As psychologists, we face a number of challenges and stressors that place us at risk for experiencing distress, burnout, vicarious traumatization, and eventually impaired professional competence.
Thus it’s necessary to engage in active attempts to manage these challenges and demand through ongoing self-care efforts. Failure to do so may result in harm to our clients, our profession, ourselves, and others in our lives.

Underlying Concepts
The definitions of impairment are not completely clear The APA has provided a detailed description of colleague
impairment and assistance noting numerous descriptions of “impaired professionals” according to various states’ laws, regulations, or state psychological associations.
These definitions were often vague
i.e. A failure to provide services within reasonable standards of care
They are also restricted in their scope
i.e., noting only impairment due to drugs/alcohol or mental disorder
APA acknowledged this lack of consensus and stated, “A universal definition of distress and impairment in professional functioning has not yet been created, although most definitions demonstrate common themes” (APA, 2006, p. 6).

Underlying Concepts
Distress
Subjective emotional state or reaction experienced by an individual in response to ongoing stressors, challenges, conflicts, and demands (Barnett, Baker, Elman, &Schoener, 2007).
Natural state that cannot be avoided
Does not necessarily lead to impairment
Lack of adequate attention to distress makes more likely to lead to impairment
A result of inadequately dealt with distress over time is what Freudenberger (19975, 1990) termed burnout

Underlying Concepts
Burnout
Characterized by feelings of depersonalization, emotional exhaustion, and lack of feelings of satisfaction and accomplishment
May result in prolonged work with emotional challenging clients

Underlying Concepts
Impairment Also referred to as impaired professional competence
May refer to the harmful impact of untreated distress on the psychologist’s professional competences ell as the negative effects of other personal or profession as well as factors that adversely impact one’s competence
An objective change in the psychologist’s professional functioning that may result in ineffective services or cause harm to those with whom we work (Wise, Hersh, and Gibson, 2011)
Examples: being late for appointments Failing to return phone calls Failing to complete reports on time

Underlying Concepts(Wise et al., 2011)
Improper behavior Refers to professional behaviors that clearly cross ethical boundaries and constitute professional misconduct
i.e. sexual or fiscal improprieties with clients (the more obvious ethical violations)

Distress vs. Impairment Distress and Impairment should not be viewed dichotomously
Munsey (2006a) described distress as “an experience of intense stress that is not readily resolved, affecting well-being and functioning, or disruption of thinking, mood and other health problems that intrude on professional functioning,” while impairment is “a condition that compromises the psychologist’s professional functioning to a degree that may harm the client or make services ineffective” (p. 35).
Despite being distinctive components, the line between what constitutes distress and impairment remains blurred.
Burnout should be thought of as one of the many domains that can lead to distress and distress can lead to impairment

And yet, more terminology . . . Problems with professional competence (PCC) vs.
Impaired professional (Elman & Forrest, 2007)
Impairment suggests a clinical or legal issue such as those covered under the Americans with Disabilities Act
PCC focuses on professional skill development rather than psychological impairment
Problems are described in the following way: Lack of responsiveness to feedback
Minimal self-disclosures and self-reflections regarding therapy cases
Defensiveness when asked about actions
Dismissiveness regarding the importance of documentation
Dissmissiveness regarding importance of transference/counter-transference

Definition Issues The lack of consensus in defining impairment is that it makes
identifying rates of impairment problematic
This likely contributes to the difficulty in locating overall impairment rates in the literature. Understanding specific distress (e.g., depression, substance abuse, burnout, vicarious traumatization) may provide a clearer picture (Smith & Moss, 2009)
It is hoped that psychologists will notice signs of distress as they occur and take needed actions to prevent impairment.
Haas and Hall (1990) recommend, “ psychologists should have the self awareness to know when they are functioning poorly and then pursue options to resolve this problem.”

Why is it not that easy? As individuals trained to attend to others’ emotional
states and difficulties, we are at increased risk for overlooking or ignoring our own emotional needs and reaction.
Many of us may have a blindspot and fail to focus on our own needs, issues, and concerns (O’Connor, 2001).
A blind spot can result in possibly missing signs of distress and burnout which can lead to impaired professional competence.
And even if we are aware of them, we may be likely to minimize or deny them, needing to present the façade of the strong caregiver and not the appearance of a weak person in need of assistance (Barnett, Baker, Elman, &Schoener).

Risk Factors for Impairment Numerous data exists that suggest that many psychologists have
histories and vulnerabilities placing us at an increased risk for distress and impairment
70% of female and 33% male psychologists surveyed acknowledged a history of physical or sexual abuse as children
Additionally more than 1/3 surveyed acknowledged experiencing some form of abuse as an adult (Pope and Feldmean-Summers, 1992)
Compared to women in other professions, female mental health professionals acknowledged far greater history of childhood abuse, parental alcoholism, and dysfunction in family of origin, and were more likely to experience a death of a family member and psychiatric hospitalization of a parent (Elliott and Guy, 1993)
As a result, it is possible that individuals in the mental health profession are more likely to be attracted to this profession because it permits the continuations of a caregiver role and because it may allow the opportunity to address or resolve earlier patterns of difficulty and dysfunction, in of itself putting us at risk for distress (Barnett, Baker, Elman, & Schoener)

Challenges & Stressors in Psychology
The number of challenges and stressors that may add to psychologist’s risk of distress and impairment can include:
Clients who place a great deal of emotional demands on the psychologist i.e. Individuals with personality disorders and those who engage in manipulative high risk
behaviors
Clients with chronic difficulties who do not improve and/or relapse at times Clients who attempt or complete suicide Clients who engage in aggressive or violent acts against themselves or others Clinical work with victims of violence and other traumatic events may lead to
vicarious traumatization or secondary victimization Requirements of insurance and managed care
i.e. paperwork demands, adverse utilization review decisions, and difficulties with receiving payment for services
Professional isolation Being on call during nights and weekends and having to respond to crises Concerns about or the impact of ethics, licensure board, or malpractice
complaints
(Baeger, 2001; Barnett, Baker, Elman, & Schoener, 2007; Gately & Stabb, 2005)

Just Like Everyone Else
Though we may spend time teaching and fostering coping skills in our clients, we are not immune to using maladaptive coping skills.
Impaired professional competence may be the direct result of maladaptive coping responses to ongoing distress in personal and professional lives (Barnett, Baker, Elman, & Schoener, 2007).
Additionally, we are no less likely than the average person to experience the effects of daily stresses or physical and mental health concerns and substance abuse issues.

Just Like Everyone Else It is easy to presume that our education and training as
psychologists insulate us from these forces, in reality we are at a greater risk than the general population.
Personal stressors that can impact work Relationship difficulties
Break-ups
Chronic Illness
Death of friends or loved ones
Financial difficulties
Other stressors experienced by individuals throughout our lives
But unlike the general population, our job is to attend to other’s issues and stressors without letting our personal stuff effect our physical and mental health or out ability to help those with whom we work.
Impairment: What might this look like?
In regard to personal distress, practitioners appear to report greater problems with emotional exhaustion, work-related stressors, fatigue, and disillusionment, depersonalization, and a reduction of personal accomplishment (Jenaro et al., 2007; Mahoney, 1997).

Impairment: What might this look like? (Gilroy et al., 2002; Rupert & Morgan, 2005)
Some symptoms of distress and impairment may be noticeable to the professional, but may not be readily identifiable to colleagues:
reduced energy
impaired concentration
decreased patience
decreased confidence
emotional exhaustion
Depersonalization
low sense of personal accomplishment
feelings of grief, anger, sorrow, hypervigilance, and numbing that may accompany vicarious traumatization/secondary traumatic stress

Impairment: What might this look like?
(Barnett et al., 2007; Barnett et al., 2007 ; Gilroy et al., 2002; Rupert & Morgan, 2005)
Other possible warning signs:
Increased feelings of frustration
Impatience
Anger towards clients
Increased boredom
Lack of focus
Hoping certain clients cancel their appointments
Increased fatigue
Decreased motivation
Decreased fulfillment and enjoyment from one’s work

Impairment: What might this look like?
(Boisaubin & Levine, 2001; Corlin, 2002; Smith & Moss, 2009)
Symptoms of distress and impairment that may be noticeable to others:
Increased isolation from others
Withdrawn or irritable
Quantity and quality of work can suffer
Increase in substance use
Complaints from colleagues or supervisees
Changes in behavior
i.e. arriving late to appointments or meetings, poor self-care or hygiene, and frequent, unexplained absences

You better check yourself… before you wreck yourself
It is essential that we see ourselves as vulnerable to the harmful effects of the numerous personal and professional stressors and challenges we face
We all should be sensitive to these issues and should conduct regular self-appraisals as well as engage in an ongoing preventative care program (Barnett et al., 2007).
Self-assessments should include awareness of and attention to personal risk factors and warning signs.

You better check yourself…before you wreck yourself
Self-Assessments need to address the use of maladaptive or negative coping and professionals need to be aware of and avoid these. Negative coping skills are likely to further compound any current difficulties. Negative coping skills can include
Self-medicating (can be with alcohol, drugs, food, etc.)
Seeking emotional support or gratification from clients
Engaging in minimization, denial, or rationalization
Rather, it is imperative for psychologists to engage in positive career sustaining behaviors:
Striking a balance between personal and professional demands and activities
Seeking diversity in professional demands and activities and caseloads
Taking regular breaks from work
Getting adequate rest and exercise
Balanced and healthy diet
Attending to emotional, physical, relationship, and spiritual needs outside the work setting

You better check yourself…before you wreck yourself
These activities cannot be seen as luxury, but rather essential aspects of our professional role that will increase overall personal and professional wellness (Barnett, Baker et al., 2007).
It is important to be aware of the isolation that our profession can create. As a profession, we need to steer clear of professional isolation and begin viewing it as a significant risk factor for burnout and impaired competence.
The use of peer support and supervision groups, personal psychotherapy, individual supervision, professional associations, and colleague assistance programs all may help promote psychologist self-care and may effectively respond to signs of developing impairment (Barnett, Baker, Elman, &Schoener).
Additionally, it is imperative for our profession to reduce the stigma of help-seeking behaviors, to create an expectation for ongoing self-care that establishes this as a part of professional identity and to establish a professional environment of openness, sharing, peer support, and consultation.
Barriers to Intervention
Good, Thoreson, and Shaughnessy (1995) found that 43% of the psychologists surveyed were aware of a male psychologist with a substance abuse problem, and 28% knew of a female psychologist with a substance abuse problem. Yet, only 19% of those polled acknowledged confronting their colleague about their substance abuse.
Thoreson, Budd, and Krauskopf (1986b) reported similar findings, with 33% of their sample having knowledge of a colleague who misused alcohol, but only 12% intervening with the colleague.
More recent research examining the frequency with which impaired psychologists are identified and confronted by their colleagues is sparse at best (Smith & Moss, 2009).

Back to Ethics…for a brief moment The American Psychological Association Code of
Ethics:
Standard 1.04 Informal Resolution of Ethical Violations
“When psychologists believe that there may have been an ethical violation by another psychologist, they attempt to resolve the issue by bringing it to the attention of that individual, if an informal resolution appears appropriate and the intervention does not violate any confidentiality rights that may be involved. (See also Standards 1.02 and 1.03)”
Standard 1.05 Reporting Ethical Violations
If an apparent ethical violation has substantially harmed or is likely to substantially harm a person or organization and is not appropriate for informal resolution under Standard 1.04 (above), or is not resolved properly in that fashion, psychologists take further action appropriate to the situation. Such action might include referral to state or national committees on professional ethics, to state licensing boards, or to the appropriate institutional authorities. This standard does not apply when an intervention would violate confidentiality rights or when psychologists have been retained to review the work of another psychologist whose professional conduct is in question. (See also Standard 1.02).”
Barriers to Intervention
An overall lack of awareness of signs of distress and possible impairment may be one reason for failing to intervene with a colleague (Smith & Moss, 2009)
If symptoms are present, psychologists may have difficulty differentiating the margin between their colleague’s distress and impairment (i.e., a compromise in the professional role resulting in ineffective or harmful services; Munsey, 2006a).
Early signs can be overlooked, especially when impairment is slow and stealthy in onset. Once the impairment becomes blatant, peers may hesitate to intervene for a multitude of reasons. (Smith & Moss, 2009)

Ethics (continued)
PA Code of Ethics
Principle 7 (i): “When psychologists know of an ethical violation by another psychologist which does not affect the welfare of that psychologist’s clients and which appears to be owing to lack of sensitivity, knowledge or experience, they attempt to resolve the issue informally by bringing the behavior to the attention of the psychologist. Informal corrective efforts are made with regard for the rights to confidentiality involved. If the violation is one which threatens client welfare or is not amenable to an informal solution, psychologists bring it to the attention of the Board. Obligations imposed by this subsection are in addition to the reporting requirements under section 18(f) of the act (63 P.S. § 1218(f).”
Barriers to Intervention Floyd, Myszka, and Orr (1998) asked psychologists what prevented
them from expressing concern over a colleague.
43% did not believe that the colleague’s behavior would affect his or her professional functioning
26% believed that the intervention would result in an adverse outcome
22% were unsure of their professional responsibility to do so.
19% of these psychologists reported that expressing concern about a colleague may result in risk to themselves
13% believed it could result in risk to their colleague
The findings by Floyd et al. (1998) are consistent with additional literature suggesting that psychologists fear potential negative consequences if they intervene with an impaired colleague.

Barriers to Intervention (Good et al., 1995; Sherman, 1996; Smith & Moss, 2009; VandenBos
& Duthie, 1986)
Intervention may be perceived to negatively affect one’s relationship with the impaired colleague, leading to undesirable risks for the colleague
i.e., termination of employment, loss of license
or oneself i.e., fear of litigation, fear of losing friends, fear of being
confronted with one’s own flaws (Good et al., 1995; Sherman, 1996; VandenBos & Duthie, 1986).
Hesitation to intervene can also be due to fear of questioning a peer’s professional judgment, the belief that their evidence is insufficient, fear the impaired peer will deny he or she has a problem or reject help, or the hope that another colleague will intervene

Barriers to Intervention Just as psychologists fail to identify impairment and
intervene with peers, they can fail to identify signs of impairment in themselves.
Throughout training and their professional careers, psychologists are seldom encouraged to express doubts or concerns about themselves. Rather, they are encouraged to maintain a visage of competence at all times (O’Connor, 2001).
This can result in psychologists rationalizing their own behavior.
Regular interactions with trusted and respected colleagues with whom there is explicit agreement to confront one another appear to be useful. Peer consultation groups are a prime example of such an arrangement.
However, many busy professionals do not engage in such groups. These take time, and in our business, time is money.
The result, then, is that we do not have a mechanism to confront our colleagues or to be confronted, further exacerbating impairment.

How to Intervene It is imperative to remember in reference to intervening
with impaired colleagues that every situation is different, and it is not possible to create a set of guidelines that will be appropriate for all people in all situations.
For example, the colleague who is experiencing difficulty with a family transition (loss of a parent, youngest child moves out, etc.)may require a different approach than the colleague who is abusing substances in the workplace.
There are times when simply bringing concerns to the impaired psychologist may be adequate to raise awareness and affect change, and it is up to the intervening psychologist to determine the best approach for addressing these issues.
Role-playing the conversation or consultation with colleagues can assist in making such determinations.
Furthermore, documentation of any discussion with the impaired colleague is appropriate in all situations should early intervention not adequately remedy the situation.

How to Intervene (Elman & Forrest, 2007)
By changing the language from impaired professional to problems with professional competence, allows us to find easier ways to address issues of competence:
Focusing on skills assists in developing specific strategies for remediation.
Therapy does not need to be the automatic recommendation for all problems of competence. For example, scenarios may be provided for
discussion to increase self-awareness and role-play can be used to address appropriate therapeutic responses
Competence includes assessing personal and interpersonal functioning as our ultimate goal is or responsibility to the public. Competency assessment creates a bridge between training competence and professional practice. Professional competence involves, adaptation to change, ability to generate new knowledge, and ongoing professional growth

How to Intervene(O’Connor, 2001)
O’Connor (2001) provided recommendations that might improve psychologists' approach to the impaired professional and those who are so charged, while better protecting the public.
1. Demonizing those among us who are distressed or impaired or who are charged with violations is counterproductive and must stop.
Most psychologists can be vulnerable to distress, impairment, and unethical behavior in the right circumstances. Psychologists can be vulnerable to false charges as well.
Facing the consequences of such circumstances is very frightening, support and direction are often most needed, and these circumstances can be further isolating. All of which are not in the best interest of the psychologist, the profession, or the consumer.
2. Understand that as psychologists, we can be vulnerable to stress, distress, and even inappropriate or impaired behavior in certain circumstances, and we will and do have life crises.

How to Intervene(O’Connor, 2001)
3. Encourage ongoing consultation, peer support, and openness to our students and colleagues. A professional norm of appropriate personal self-disclosure and consultation can be established over time and be beneficial for all parties.
The sense of understanding and support that comes with disclosures of fears and failings to supportive others is beneficial for our clients and can be therapeutic for psychologists.
4. Make isolation a concern for all practitioners.
5. Continue education related to distress and impairment including the impact of life crises and the possible predisposition and role characteristics that may impact the clinician.
Those who are troubled are unlikely to step forward in a punitive climate, education is our primary weapon in combating professional impairment and protecting the public.

How to Intervene(O’Connor, 2001)
6. Use our capacity for empathy, our assessment skills and our authority to identify circumstances, needs and options and to set appropriate limits.
Rather than avoiding the problem, we could all improve upon our active support or confrontation of the troubled psychologist. Ethical guidelines and more protective legislation may assist those who would like to intervene with an impaired colleague but fear the possible legal ramifications of whistle blowing.
7. Recognize that impairment does not negate consequences for unethical behavior or incompetence.

How to Intervene(O’Connor, 2001)
8. Better inform oversight bodies about the dynamics of distress and impairment and the role of client
motivations and transference in the complaint process.
For example, a client with borderline personality disorder may significantly distort the client’s perception of the therapist’s motivations and behaviors (i.e. transferential rage).
9. Expand our understanding of client diagnoses that are more likely to result in complaints, and why.
10. Insist on informed, consistent, and fair treatment from oversight bodies.

Psychologist suicide
Sparse research and literature on this topic
Inconsistent methodologies & disparate findings
Elevated suicide rates for healthcare professionals
Physicians, dentists, nurses
‘Wounded Healer’ (Guggenbuhl-Craig, 1999)
Come into profession already wounded

A Little Bit of Research…
Steppacher and Mausner (1973) 1960-1969: suicide rates for male psychologists slightly below
general population
Female psychologists- suicide rates three times that of general population
Guy and Liaboe (1985) Questioned accuracy of above study
Possible sampling and methodological errors
Accuracy of using death certificates
Deutsch (1985) Sample 264 master’s and doctoral level psychotherapists, 2%
reported a suicide attempt
Pope and Tabachnick (1994) Sample 800 psychologists, 29% reported suicidal ideation, 4%
reported a suicide attempt

A Little Bit of Research… (continued)
Phillips (1999) 1981-1990: Psychologist suicide not above national average
Kleespies et al. (2011) questioned generalizability of these results (sampling)
Gilroy et al. (2002) Surveyed 425 counseling psychologists
21% passive suicidal ideation
18% suicidal ideation without a plan
3% suicidal ideation with a plan
1 clinician had an attempt
2009 APA survey: 40%-60% of psychological practitioners reported some disruption in professional functioning from burnout, anxiety or depression (DeAngelis, 2011).

Impact on Colleagues
Takes 1-2 years on average for colleagues to make sense of and cope with loss
Students and trainees question their career choice
Feeling stunned or shocked
Fear of missed warning signs
Are there longer-term supports available to those who need them?
Individual and group therapy
Support groups within community

Impact on Clients(Chiles, 1974; Ballenger, 1978)
Clients were aware that psychologist had problems prior to the suicide
Some felt they were treating the psychologist
Felt responsible for the psychologist’s death
Self-blame
Concerns about fallibility of therapist
Unable to help oneself, how could they help me?
Ambivalence toward therapy
Reject?
Re-engage?
Shock, loss, abandonment, distrust
Sense of demoralization
Questioned hope for their own mental health recovery

Professional Will The American Psychological Association’s Ethics
Code “Psychologists make plans in advance to facilitate the
appropriate transfer and to protect the confidentiality of records and data in the event of psychologists’ withdrawal from positions or practice.” (Section 10.09)
Pennsylvania’s Code of Ethics Principle 5 (Section b, 6): “The psychologist makes
provisions for the maintenance of confidentiality in the preservation and ultimate disposition of confidential records.”
Principle 7 (Section b): “Psychologists understand the areas of competence of related professions, and make full use of the professional, technical and administrative resources that best serve the interest of consumers. The absence of formal relationships with other professional workers does not relieve psychologists from the responsibility of securing for their clients the best possible professional service nor does it relieve them from the exercise of foresight, diligence and tact in obtaining complementary or alternative assistance needed by clients.”

Professional Will Who should notify clients and colleagues about
situation? Choosing an executor
Back up plan?
Compensation for the executor
How should patients be notified of death and/or serious illness (stroke, heart attack, unexpected extended hospitalization, etc.)? What information about therapist should be disclosed?
How should patient records be handled? Billing and financial records
Who has access to patient information? Appointment book and patient contact information
Email and voicemail access codes; EHR codes
Keys to the office, filing cabinets, storage facility
Liability Insurance

Professional Wills- Additional Info.
Dr. Frankel's presentation on professional wills and why you need one:http://static1.squarespace.com/static/54309a74e4b056843fc5a601/t/5573984ae4b0c6a58c7206b1/1433638986321/Beyond+the+Professional+Will+%282%29.pdf
Dr. Frankel's video on professional wills:https://stevefrankel.adobeconnect.com/_a988445346/p6zqakqhepd/?launcher=false&fcsContent=true&pbMode=normal
www.therapistspostdisaster.com/Professional_will_template.doc

Professional Will Resources
The APA Practice Organization's guide to professional wills, at http://www.apapracticecentral.org/business/legal/professional/secure/will.aspx .
Free materials, including guidelines for preparing a professional will; a professional will format; and guidelines for professional executors, from the San Diego Psychological Association.
A free, downloadable copy of a professional will template from Key West, Fla., practitioner Stephen A. Ragusea, PsyD: http://www.ragusea.com/drsteve/resources.html.
Pope, K.S. & Vasquez, M.J.T. (2005). Preparing a professional will. In Pope and Vasquez, How to survive and thrive as a therapist: Information, ideas and resources for psychologists in practice. Washington, DC: American Psychological Association.

ReferencesAmerican Psychological Association. (2006, February 10). Advancing colleague assistance in professional psychology. http://www.apa.org/practice/acca_monograph.html
Bamonti, P., Keelan, C., Larson, N., Mentrikoski, J., Randall, C., Sly, S., Travers, R., McNeil, D. (2014). Promoting ethical behavior by cultivating a culture of self-care during graduate training: A call to action. Training and Education in Professional Psychology, Vol 8(4), Nov, 2014 Special Section: Ethical Issues in Education and Training. pp. 253-260.
Barnett, J. E., Baker, E. K., Elman, N. S., & Schoener, G. R. (2007). In pursuit of wellness: The self-care imperative. Professional Psychology: Research and Practice38(6), 603-612. doi: 10.1037/0735-7028.38.6.603.
Baerger, D. R. (2001). Risk management with the suicidal patient: Lessons from case law. Professional Psychology: Research and Practice, 32, 359-366.
Boellinghaus, I., Jones, F., and Hutton, J. (2013). Cultivating self-care and compassion in psychological therapists in training: The experience of practicing loving-kindness meditation.Training and Education in Professional Psychology, Vol 7(4), Nov, 2013 pp. 267-277.
Davis Bush, A. (2015). Little and often: Using micro-practices for self-care. Psychotherapy Networker, 39 (3), 24- 27, 45.
DeAngelis, T. (2011). Psychologist suicide: What we know and how we can prevent it. Monitor on Psychology, 42(10), 19
Deutsch, C.J. (1985). A survey of therapists’ personal problems and treatment. Professional Psychology: Research and Practice, 16(2), 305-315.
Eliott, D. M., & Guy, J. D. (1993). Mental health professionals versus non-mental health professionals: Childhood trauma and adult functioning. Professional Psychology: Research and Practice, 24, 83-90.
Elman, N. S. & Forrest, L. (2007). From trainee impairment to professional competence problems: Seeking new terminology that facilitates effective action. Professional Psychology: Research & Practice, 38(5), 501-509. Doi: 10.1037/0735-7028.38.5.501.

ReferencesFreudenberger, H. J. (1975) The staff burn-out syndrome in alterative institutions. Psychotherapy: Therory, Research, and Practice, 12, 73-82.
Freudenberger, H. J. (1990). Hazards of psychotherapeutic practice. Psychotherapy in Private Practice, 8, 31-34.
Floyd, M. Y., Myszka, M. T., & Orr, P. (1998). Licensed psychologists’ knowledge and utilization of a state association colleague assistance committee. Professional Psychology: Research and Practice, 29, 594–598.
Gately, L. A., & Stabb, S. D. (2005). Psychology students’ training in the management of potentially violent clients. Professional Psychology: Research and Practice, 36, 681-687.
Good, G. E., Thoreson, R. W., & Shaughnessy, P. (1995). Substance use, confrontation of impaired colleagues, and psychological functioning among counseling psychologists: A national survey. The Counseling Psychologist, 23, 703–721.
Good, G. E., Khairallah, T., & Mintz, L. B. (2009). Wellness and impairment: Moving beyond noble us and troubled them. Clinical Psychology: Series & Practice, 16(1), 21-23. doi: 10.1111/j.1468-2850.2009.01139.x
Guggenbuhl-Craig, A. (1999). Power in the helping professions. Putnam, CT: Spring Publications.
Guy, J.D. & Liaboe, G.P. (1985). Suicide among psychotherapists: Review and discussion. Professional Psychology: Research and Practice, 16(4), 470-472.

ReferencesGilroy, P. J., Carroll, L., & Murra, J. (2002). A preliminary survey of counseling psychologists’ personal experiences with depression and treatment. Professional Psychology: Research and Practice, 33, 402–407.
Guggenbuhl-Craig, A. (1999). Power in the helping professions. Putnam, CT: Spring Publications.
Guy, J.D. & Liaboe, G.P. (1985). Suicide among psychotherapists: Review and discussion. Professional Psychology: Research and Practice, 16(4), 470-472.
Haas, L. J. & Hall, J. E. (1991). Impaired, unethical, or incompetent? Ethical issues for colleagues and ethics committees. Register and Practice, 20I, 48-50.
Jenaro, C., Flores, N., & Arias, B. (2007). Burnout and coping in human service practitioners. Professional Psychology: Research and Practice, 38, 80–87.
Kleespies, P.M., Van Orden, K.A., Bongar, B., Bridgeman, D., Bufka, L. F., Galper, D. I., Hillbrand, M., & Yufit, R.I. (2011). Psychologist suicide: Incidence, impact, and suggestions for prevention, intervention, and postvention. Professional Psychology: Research and Practice, 42(3), 244-251.
Mahoney, M. J. (1997). Psychotherapists’ personal problems and self-care patterns. Professional Psychology: Research and Practice, 28, 14-16.
Markway, B. (2014). Seven types of self-care activities for coping with stress. Psychology Today. Retrieved on June 16, 2015 from: http://www.psychologytoday.com/blog/shyness-is-nice/201403/seven-types-self-care-activities
Munsey, C. (2006a). Helping colleagues to help themselves. Monitor on Psychology, 37(7), 35
Munsey, C. (2006b). Questions of balance: An APA survey finds a lack of attention to self-care among training programs. GradPSYCH, 4. Retrieved June 6, 2015, from http://www.apa.org/gradpsych/2006/11/cover-balance.aspx
Myers, S., Sweeney, A., Popick V., Wesley, K., Bordfeld, A., and Fingerhut, R. (2012). Self-care practices and perceived stress levels among psychology graduate students. Training and Education in Professional Psychology, 6(1), 55-66.

ReferencesO’Connor, M. F. (2001). On the etiology and effective management of professional distress and impairment among psychologists. Professional Psychology: Research and Practice, 32, 345–350.
Phillips, S.M. (1999). U.S. psychologists’ suicide rates have declined since the 1960s. Archives of Suicide Research, 5(1), 11-26.
Pope, K. S. & Feldman-Summers, S. (1992). National survey of psychologists’ sexual and physical abuse history and their evaluation of training and competence in these areas. Professional Psychology: Research and Practice, 23, 353-361.
Rupert, P. A., & Morgan, D. J. (2005). Work setting and burnout among professional psychologists. Professional Psychology: Research and Practice, 36, 544–550.
Sherman, M. D. (1996). Distress and professional impairment due to mental health problems among psychotherapists. Clinical Psychology Review, 16, 299 -315.
Steppacher, R.C. & Mausner, J.S. (1973). Suicide in professionals. American Journal of Epidemiology, 98, 436-445.
Tartakovsky, M. (2013). How clinicians practice self-care & 9 tips for readers. PsychCentral. Retrieved on June 16, 2015 from: http://psychcentral.com/lib/how-clinicians-practice-self-care-9-tips-for-readers/.
Thoreson, R. W., & Skorina, J. K. (1986). Alcohol abuse among psychologists. In Kilburg, R. R., Nathan, P. E., & Thoreson, R. W. (Eds.), Professionals in distress: Issues, syndromes and solutions in psychology (pp. 77-117). Washington, DC: American Psychological Association.
VandenBos, G. R., & Duthie, R. F. (1986). Confronting and supporting colleagues in distress. In R. R. Kilburg, P. E. Nathan, & R. W. Thoreson (Eds.), Professionals in distress: Issues, syndromes, and solutions in psychology (pp. 211–231). Washington, DC: American Psychological Association
Wise, E. H., Hersh, M. A., & Gibson, C. M. (2011). Ethics and self-care: A developmental lifespan perspective. Register Report, 37, 20-29.