Embed Size (px)
Citation preview

Pediatric Ophthalmic Dispensing in different visual problems
Raju KaitiConsultant Optometrist
M. OptomDhulikhel Hospital, Kathmandu University Hospital

What is Pediatric Dispensing?• Considered to be related with dispensing of children age
ranging below 16 years• Babies to mid-teens
• Not only for the correction of refractive error– Also to correct binocular vision anomalies such as strabismus,
amblyopia, or convergence anomalies
• Challenging task
• Requires great communication skills and fitting techniques and adequate patience

• Frequent prescription change and long term patient-practitioner relationship
• Not only children but also their parents can be influenced and retained as regular clients
• Good practice builder
• Children are still developing; hence require special frames designed for them, not the small adult ones

How it differs from adult dispensing?• More difficult• More fun• Duality of client• Time
• Measurement errors get proportionately more serious than in an adult– Child’s facial size exaggerates the error– More discomfort – Facial disfigurement in severe cases

Pediatric Frames• Must fit correctly (anatomically)
• Should be comfortable and durable
• Must not hamper the natural development of the nose
• Must be aesthetically acceptable
• The practitioner needs to ensure that the pupils and lenses are correctly centered
• Safety is of primary concern

Frames need to have• Children don’t have developed nose– Characteristics of good kids’ frames lower crest
larger frontal angle

larger splay
flatter pantoscopic tilt

– Smaller frontal width– Shorter length to bend– Shorter length of drop– Smaller boxed lens size– Shorter back vertex distance
• Spring hinges to allow for children taking their spectacle off with one hand and general hard wear.
• Over 95% of frames dispensed to children are metal. It should be ensured that the frames have no sharp edges.
• Titanium is an ideal material for children as it is strong, durable and holds its adjustment well.
• Cellulose acetate, polyamide, optyl are plastic materials
• Solidly built frames (plastic or metal)
• Deep lens grooves for more securely seated lenses
• Silicone-based rubber frames for babies and children who require indestructible frames-light and pliable and no metal hinges reducing chances of facial injury.

• Square faces: soft curves• Round faces: angular shapes• Short face: shallow frame• Color matching: consider skin color
• Avoid the desire to supply frames they can “grow into”.• Too wide means that:
– Easily knocked off– Optical quality is compromised (aberrations)– Lens thickness is increased
• Reject like oversized clothes.

Main aspects of frame dispensing:• Frame front/width• Eye size• Nasal Bridge • Temple and joints• Frame height• Pantoscopic tilt• Vertex distance• Face form angle

Frame front/Frame width
• Frame front should not be too wide that may cause frequent falling or loosening.
• Too small frame may make child reluctant to wear the frame and also may mark the soft and delicate skin around the temporal regions.
• Attractive color and beautiful designs may increase compliance among children to wear glasses.

Eye size
• Eye size should be bit smaller.
• High power lenses tend to get heavy, unattractive and changing pantoscopic angle, vertex distance etc. would be difficult with large eye size.

Bridge position• Narrow bridge should be used to avoid frame
from slipping down.
• Bridge should fit properly such that entire weight of the spectacle is not carried by crest.
• Nose bridge for children should have contact surface as large as possible.
• The bridge selected should not allow the eyewires to ride on the cheeks.
• Not only painful can also cause permanent ridge to be formed

• Weight of spectacle can be evenly distributed over large area using larger nose pads
• Saddle, keyhole bridge with accurate fit• Strap bridge
• fitting children needs to be – more support at the bottom of the nose pad area, and – a larger pad splay angle (more flare to the pad). A larger pad or
contact surface area helps the frame sit better

Temple and joints• It is better to use appropriate temple
length.
• Use skull type of temple or riding bow type.
• The curl of the sides must stop just short of the ear lobe and sit along back of the ear.
• Curl of sides should be covered in silicone for comfort and durability.


• temple joint with frame front should be at the middle to avoid frame falling down and child viewing from over frame.
• Temple joint should be flexible or have spring on it or 180 degree.
• Temple shouldn’t touch the side of the head until reaching the ear-point.
• Bend sits at the ear point and the drop should rest along the side of the head.

• Frame height– Children have higher cheek position so ensure appropriate lens height.
• Face form angle– Face form lens are good for children as it not only protects eyes but
also vertex distance can decreased.– Face form lens has good grip on child's face.
• Vertex distance– Fit with as close vertex distance as possible to reduce aberration and
ensure clear vision.

Lens selectionThe ideal lens should be
1.1. Impact resistant and durable (children are heavy handed)
22. Light and comfortable
3.3. Relatively thin
4.4. Ideally should give full UV protection
• Vision Consideration
• Hard coated CR39, Polycarbonates, Trivex and High index plastics
• Glass lenses are too dangerous and inappropriate for this group.

Vision considerations• IPD measurement
• Vertex distance
• Lens type

IPD measurement• Proper measurement to ensure optical clarity and reduce
unwanted prismatic effect.
• For older children can use a pupillometer• For younger children use a PD rule
• For very young children or for strabismic cases (uncooperative to fixate his eye ) can use a PD rule measuring ,inner canthus to outer canthus distance can also be measured.
• Involve them in attentive task

Vertex distance•Vertex distance should be as close as possible:•For good frame stability so that lens doesn’t fall down.•For good Optical clarity by reducing peripheral aberration•For maximizing visual field by removing ring scotoma by thick frame of child.
Centers•Should be as close as possible to the geometric centers, using the principal axis/center of rotation rule
– Drooping the optical center 1 mm below the pupil center for every 2 degrees of pantoscopic tilt

Impact resistance
• Children usually tend to break their frames and in few cases lens also.
• Either hard coated polycarbonate or Trivex ( 10x impact resistance than CR-39) lens can be prescribed.

Scratch resistance
• Children lenses scratch more easily
• Hard coat to prevent from easy scratch
• For good optical quality, anti reflection coating is must….hence multi coated lenses is desired
• Children should be taught about proper frame handling, placement and lens cleaning procedures.

Weight • Weight of a lens depends on prescription and specific gravity
of the material used
• Heavy thick lens in high power not only affect optical clarity but also affects frame stability during wear.
• Lenticular lenses given in high plus lenses.
• High index thin lens are desirable as little thinner lens can be used

Polycarbonate• Refractive index (nd) = 1.586
• Abbe number (vd) = 31
• Specific gravity =1.20 gm/cubic cm
• And require anti-scratch coating
• High impact resistance (absorb a blow and just dent)
• Safer for children

• “polycarbonate lenses should be considered the lens of first choice if the client is a child, toddler or active teenager”- Opticians Association of America.
• National society to prevent Blindness warns that glasses and ordinary plastic lenses don’t provide enough protection for children involved in active sports.
• Polycarbonate “sports specs”- are advised for all children involved in sports such as basketball, squash etc.
Note: Trivex was not available when these quotes were made.
Trivex• Triperformance– Superior optics– Impact resistance– Ultra light weight
Refractive index of 1.532 Abbe value of 43-45 Specific gravity of 1.11 Can be thinned to 1 mm
Thickness and weight are of no issues
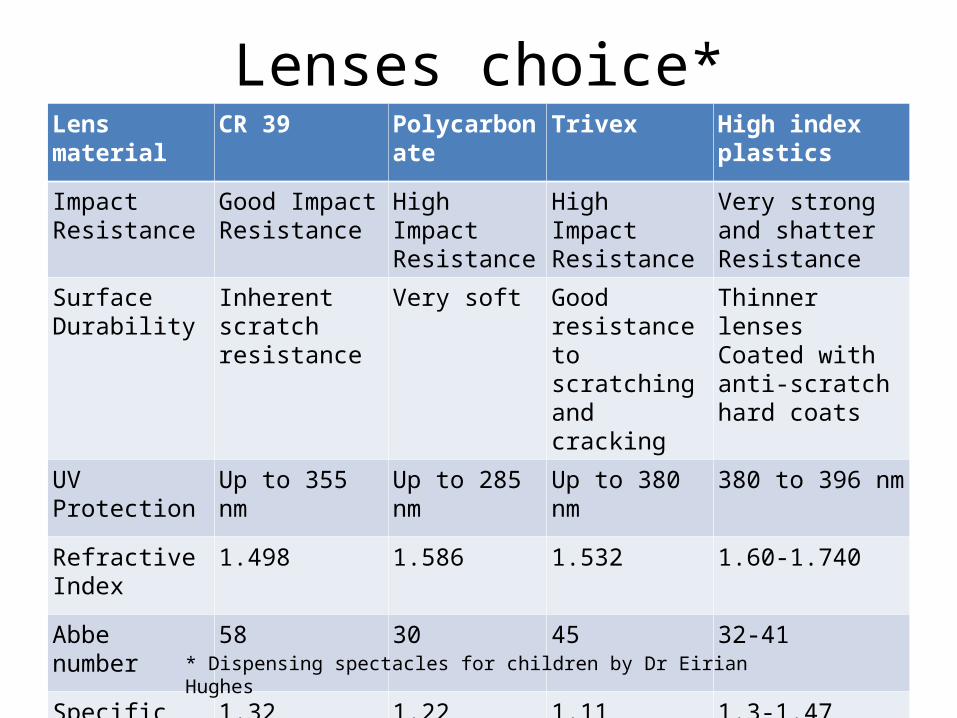
Lenses choice*Lens material CR 39 Polycarbonate Trivex High index plastics
Impact Resistance
Good Impact Resistance
High Impact Resistance
High Impact Resistance
Very strong and shatter Resistance
Surface Durability
Inherent scratch resistance
Very soft Good resistance to scratching and cracking
Thinner lensesCoated with anti-scratch hard coats
UV Protection Up to 355 nm Up to 285 nm Up to 380 nm 380 to 396 nm
Refractive Index 1.498 1.586 1.532 1.60-1.740
Abbe number 58 30 45 32-41
Specific Gravity 1.32 1.22 1.11 1.3-1.47
* Dispensing spectacles for children by Dr Eirian Hughes

Dispensing Pediatric Aphakes• Frame selection
– Small eye size frame– Rounded shape– Shape with small frame difference– Adjustable nose pad– Short vertex distance– Cable or securely fitting temples

• Aim of Lens selection– Reduce lens weight– Reduce lens thickness– Reduce spectacle magnification– Increase field of view– Minimize lens aberration– Offer choice of optimum multifocal style and position– Provide protection from glare and UV radiation.
• Lens selection– High index plastic (since the lenses are heavy and thick)– Aspheric lenses (to counter spherical aberration )– Lenticular lenses ( to counter heavy and thick lens)– Light tints and UV protection (absence of inherent UV
absorption)
• The weight of the lens depends on the volume of material X Specific Gravity
• Antireflection coating is must

• Children's faces does not develop symmetrically, therefore monocular PDs are preferable to binocular PD.
• Consider increasing FOV by vertex reduction.
• Executive Bifocal lens desired but can do with ultex or kryptop to increase near field of view design reduce vertical prismatic effect.
• While marking in dummy lens make sure that bifocal segment cuts child's pupillary margin.
• Less than 6 month old child do not need bifocal and hence corrected for near.

For High Myopes• Frames:
– Smaller eye size– Rounded corners– Flatter or “hidden” bevels– Full frame plastic frames- help hide any edge thickness– Avoid semi-rimless or rimes frames– Heavy frames most likely to slip down causing vertical prismatic
effect, so bridge with good grip and temple little tight.– As small a lens blank size as possible – reduces lens edge
thickness and weight (in myopes) – Avoid using frames with hard temple as child skin is soft and
cause rubbing and irritation.

• Lenses:– High index lens, aspheric, lenticulars– Vertex distance close– IPD can be matched or decentered based on binocular
status.
– Anti-reflection and hard coating.

Dispensing facial deformity or abnormality
• In children with ptosis use frames with lid crutches.
• In crouzans syndrome where eyes seems to be popping out, face form lenses and frames with reduced vertex distance may cause irritation to the eyelids.
• In conditions like treacher Collin syndrome where there is absent or maldeveloped ears use frames with head band.

• Down’s syndrome- typically have a flat, broad bridge to their nose
• standard nose fitting on that average spectacle frame tends not fit properly.
• common sight to see a pair of glasses perched on the end of the nose in Down’s syndrome.
• Metal frames are easier to adapt- more adjustable nosepieces. • nosepieces can be manipulated and angled to fit the shape of a
flat nose better. • slip-resistant pads to give a little more friction and stop the
frame moving so much.

• In downs syndrome where the children tend to have mongoloid feature, use rectangular frame.
• Tomato Glasses produce a frame with adjustable curl sides and a moveable adjustable bridge.
• Erin’s World frames are specifically made for people with Down’s syndrome. They feature a lowered bridge, extra-wide frame fronts and shortened temples.
• specifically to fit flatter faces with a small nose. These are sometimes referred to as Asian-Fit frames.
• For Down’s syndrome- low crest heights, so a strap bridge is a good option
• Down’s syndrome-will innately have a shorter length to bend compared with other- ensure no excessive drop behind the ear-must think in plastic frames as these can’t be cut down

Albinism/Coloboma
• Have extreme photophobia • May be associated with nystagmus, refractive errors,
strabismus and amblyopia• Frames- hypoallergic and UV painted • In albino children use colorful frame (esp. pink in girls) and
any suitable color frames for boys.• prescribe prescriptions tinted lens, photochromic lenses,
Polarized lenses and sunglasses with mirror coating.• Incorporate prisms as per necessity
Ocular misalignment/Nystagmus• Frame choice similar as in other cases
• Prism can be grounded in glasses for up to 8 prism diopters, hence can be used base in (exo) and base out (eso) as relieving prism but opposite for therapeutic purpose.
• Loose prism can be prescribed up to as high as 25 PD• Fresnel prism can be used up to 30 PD
• Tinting of the glasses or sunglasses may decrease the nystagmus of individuals with albinism.
• For the patient with oscillopsia, grinding prism into the spectacles may move the visual field to a point of decreased oscillopsia.
• In nystagmus prism apex towards nystagmus dampening side (null gaze).

Encouragement and maintenance • Encourage them by using spectacles ( family members who have
refractive errors) in front of the children
• Old unused frame to dolls they play with
• Parents to be fully informed
• Frequent monitoring of the fit
• How to take care, clean, put on and off and put their spectacles down without scratching
• Always have spare spectacle in home ( in cases of high error, amblyopes under therapy etc.)
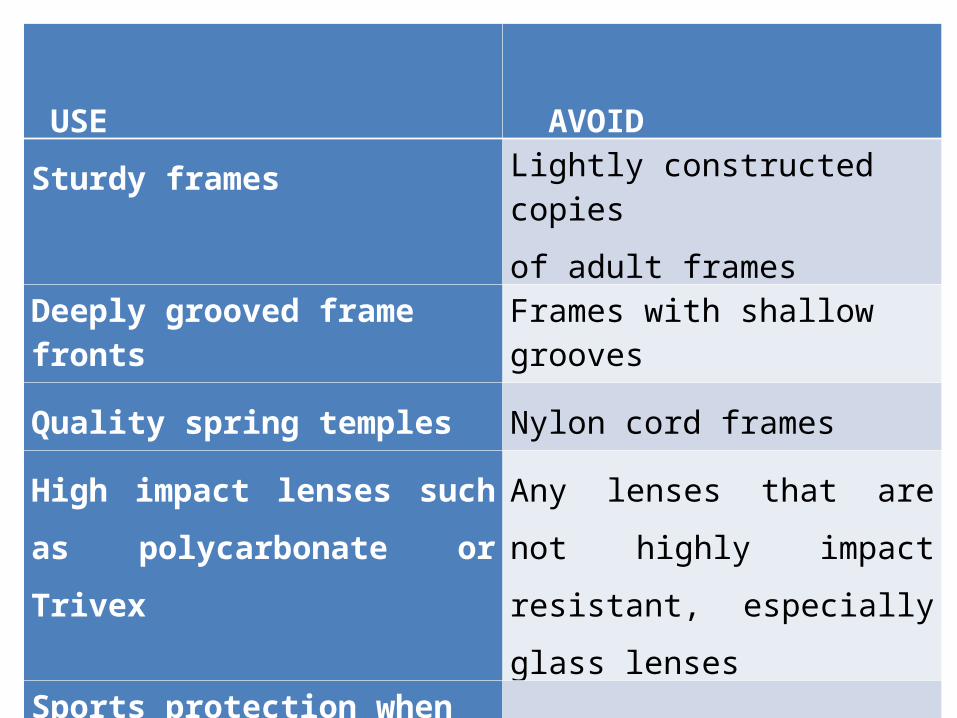
USE AVOID
Sturdy frames Lightly constructed copies
of adult frames
Deeply grooved frame fronts Frames with shallow grooves
Quality spring temples Nylon cord frames
High impact lenses such as
polycarbonate or Trivex
Any lenses that are not highly
impact resistant, especially glass
lensesSports protection when
applicable

Avoid

Thank you!!!