Embed Size (px)
Citation preview

PANEL DISCUSSION ON KNEE OA MANAGEMENT
Maj Gen (Dr) DS BhakuniLucknow, INDIA

OSTEOARTHRITIS

Articular Cartilage - Unique
No Blood Supply No Lymphatic Drainage
No Neural Elements
No immunological Recognition of Chondrocytes
60 – 80% Water

NATURAL HYALURONATE
• Natural polysaccharide component of Cartilage and Synovial fluid
• Combination of Glucornic acid & Glucosamine• Mol Wt 6500-10,900 kDa• 2 ml in normal knee• Conc is 2.5 – 4.0 mg / ml• Helps synovial fluid as Lubricant & Shock absorber• Depolymerized in OA ( 2700-4500 kDa )
• Expert opin Pharmacother 2008;9: 797-804

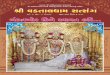
Surgery
COX-2’s
High Dose NSAIDS +Gastroprotectant Corticosteroids
simple analgesics, low dose NSAID’s
Exercise, Physical Therapy, Weight Loss, Orthotics, Nutraceuticals, Bracing
MILD
SEVERE OA
MODERATE
Guidelines for Managing Osteoarthritis
Adapted from Recommendations for the Medical Management of Osteoarthritis of the Hip and Knee, ACR, 2000
Hyaluronic Acid

Dr Rajkiran Dudam MBBS in kakatiya Medical college 1995-2001
MD in General medicine From Gandhi Medical college – Hyderabad 2001-2004
Fellowship in Rheumatology From Nizams Institute of Medical sciences Hyderabad year 2005 – 2007
Consultant Rheumatologist in STAR Hospital , Banjara hills Hyderabad
10 years of experience in Clinical Rheumatology
Secretary - Rheumatology Association of Hyderabad
Faculty at State and National conferences
Assistant Editor Indian Journal of Rheumatology

Q.Initial pharmacological intervention in OA can be all except
1. Acetaminophen & NSAIDs
2. Intra-articular steroids
3. Topical NSAIDs or Capsaicin or topical lignocaine
4. Diacerin

A.Initial pharmacological intervention in OA can be all except
4. Diacerin

Guidelines
• ACR guidelines – 2012 • OARSI – 2014/ last search 2013 march • NICE guidelines – 2014 / last search 2013• EULAR recommendations – 2010• ESCEO – 2016
USE Paracetamol, Topical NSAIDS followed by Systemic

13 RCT For spine pain – ineffective For Knee and Hip – Significant affect on pain and disability / statistically not significant Adverse effects = PBO
Safe option to relive pain at less than 2gms/day
Efficacy and safety of Paracetamol for spinal pain and Osteoarthritis :Syetemic review and meta analysis of randomised placebo controlled trials
BMJ March 2015 ; 250

Lancet May 2016
NSIADS better then Paracetamol PCM ineffective
Effectiveness of NSAIDS for the treatment of pain in knee and hip OA : a network analysisBruno R da Costa
Network meta analysis
Looked into patients from clinical trials May not represent practice setting patient population
Paracetamol very old player

NSAIDS – Choose wisely
• Elderly , Cardiovascular , Renal comorbidity – Avoid
• Stratify patients Low GI and CV risk –any nsNSAIDLow GI , high CV risk – Naproxen High GI risk , low CV risk – COX2 inhibitor or
nsNSAID + PPI Safe prescribing of NSAIDS in patients with OA – an expert consensus addressing benefits as well as gastrointestinal and cardiovascular risk Carmelo scarpignato International NSAID Consensus group BMC Medicine March 2015 ; 13-55

Topical NSAIDS
Pain relief without much systemic adverse effects
60% reduction in pain .
Topical NSAIDS for Chronic musculoskeletal pain in adults Sheena Derry , Philip CongaghanCochrane review

Q Following are useful in OA treatment
1. Glucosamine sulfate + Chondroitin sulphate2. Glucosamine Hydrochloride +Chondroitin
Sulphate3. Both 4. None

Answer
Glucosamine sulfate + Chondroitin sulphate
and
Glucosamine Hydrochloride +Chondroitin Sulphate

Glucosamine & Chondroitin
• Balance of evidence from high-quality trials has shown little to no evidence of clinically meaningful benefit
• Statistically significant improvement in pain scores in studies with < 6 months of follow-up from mostly low-quality trials.

ANNALS OF RHEUMATIC DISEASES JAN 2015
604 patients , grade 2-3 OAGH-CS compared with Celecoxib
At 6 months GH+CS has comparable efficacy with Celecoxib in reducing pain , stifffness and functional limitaion with good safety profile .
Data presented in EULAR 2016 ; London
Combined Chondroitin sulfate and glucosamine for painful Knee OA :A multicenter , randomised double-blind , non inferiority trial verses celecoxib
Marc C Hochberg

Both Glucosamine and NSAIDS are equally effective in reducing pain , stiffness , improving function .Diacerin is linked with GI and Hepatic adverse effects
Efficacy and safety of Glucosamine, diacerin , and NSAIDS in Osteaoarthritis knee Network metanalysis
Jatupon kongtharvonskul European journal of medical research 2015

European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO)
Seminars in Arthritis and Rheumatism 45 (2016) S3–S11
Symptomatic Knee OA
Step 1 : Chronic SYSDOA ( Symptomatic slow acting drugs in OA ) Glucosamine + Chondroitin plus short term Paracetamol rescue analgesia Topical NSAIDS Step 2 : Intermittent or continuous ( Longer cycles of NSAIDS ) - Stratify patients

Q : Clinical case
62 year old women with bilateral grade IV OA and background of CAD / CCF(NYHA IV) and borderline renal dysfunction ( Creatinine :1.9) is suffering with severe knee pain what is your approach
1. TKR 2. I/A steroid injection 3. Analgesics like PCM , Glucosamine + Chondroitin

Answer
• I/A steroid injections


Intraarticular glucocorticoids
• Moderate to severe pain affecting one or a few joints, not adequately relieved by oral drugs.
• Monoarticular or oligoarticular inflammatory OA in whom NSAIDs are contraindicated

Opioid analgesics
• Moderate to severe pain in whom other interventions have failed
• Tramadol (50 to 100 mg max of q6h) alone or in combination with acetaminophen
• Oxycodone - short-term use in patients with acute exacerbations of pain

To summarise
• PCM – still a safe drug in less , 2gms/day • NSAID – use judiciously • Topical NSAID – very effective • Glucosamine + chondroitin – data emerging as
effective • IA steroid can be used for short term pain
relief • Guidelines /recommendations may change

Osteoarthritis Knee
Dr John MathewDM(Rheumatology), MNAMS, DNB, Associate
Prof. RheumatologyCMC Vellore

Question
75 year old lady, has knee pain and restricted mobility due to OA, not benefited from paracetamol, local medications including NSAIDs or Intraarticular steroids. Not willing for a surgery. Next treatment option is
1. Intra articular Platelet Rich Plasma2. Intra articular Hyaluronans3. Tanezumab4. Strontium

Answer
2. Intra articular Hyaluronans

Intraarticular hyaluronans• Improve pain and function#
• Improvement in joint pain was detectable by week four, peaked at week eight, then trended downwards, with some clinically relevant benefit still evident at week 24$
( 54 randomized trials involving 7545 patients)
# Comparative effectiveness of pharmacologic interventions for knee OA: a systematic review and network meta-analysis. Bannuru RR, Schmid CH, Kent DM, et al Ann Intern Med. 2015;162(1):46.
$ Therapeutic trajectory following intra-articular hyaluronic acid injection in knee OA--meta-analysis. Bannuru RR, Natov NS, Dasi UR, Schmid CH, McAlindon TE Osteoarthritis Cartilage. 2011;19(6):611.

DS Bhakuni


05 Feb 2011- 15 Mar 201501Aug2015 – 01 Jun 2016
• Total patients: 418Males: 176 ( 42 % )Females: 241 ( 58 % )Total knees: 640
• Age range: 27-74 years• Mean age: 61.2 years• Failure to respond adequately to non-
pharmacological measures and NSAIDs

“Radiological” Profile
Kellgren-Lawrence Grading of OA knees• Grade 0= none• Grade I= none• Grade II= 263 ( 41 % )• Grade III = 347 ( 54 % )• Grade IV = 30 ( 5 % )
• TOTAL = 640


Adverse effects• Post procedure pain, 24-72 hours: 38 ( 1 – 33% ) 5.93%• Post procedure pain and swelling: 02 ( 3 – 21% ) 0.32%• Pseudo septic reaction : 1 ( 1 – 3% )
0.16%
Over all AE in 19 – 23 % cases ( Ann Rheum Dis 2010:69 ( Suppl 3 ): 702, R Raman et al….
Safe for primary care physician ( Visco Supp for OA- Adv Ther (2013)30:967-986
AE 2.8 -5.8% patients as local knee pain The Open Rheumat Journ,2014,8, 54-68

Details• No Relief – 96 knees ( 15 % )
• Lost to follow up ( Posted out ) 159 ( 25 % )
• Relief 6 months - 1 Year 240 ( 37 % )
• 1 – 2 Years 102 ( 16 % )
• > 2 Years 43 ( 07 % )

REPEAT INJECTIONS - 213 Knees
• After 6 Months - 132 ( 35 % )
• After 1 Year - 62 ( 16 % )
• After 2 Years - 16 ( 4 % )
• Max Injections in Single Joint - 4*
*Max 8 times (clinical Med Insights ( Arthritis & Musculosketel Disorders 2010:3,55-68 )

Knee Repalcement
• Total Knee Replacement 127 / 385 (33%)• ( Excluded 96 with No relief and 159 lost to
follow up ) ? Delayed Replacement ( 67 % )
• Delayed for > 7 years in 72% cases of 1,863 Gd IV (1,342 knees)*
* J Knee Surg. 2014 Oct 28 ( E pub ahead of print) Waddell & Bricker




VISCOSUPPLEMENTEXOGENOUS HYALURONATE
• By bact fermentation or Rooster Comb
• Increases intra articular lubrication which increases Visco - -elastic properties hence called as Viscosupplementation
• Low mol wt (500-700),Intermed (800-1500),High (>6000 kDa) No Evidence of superiority of any brands*• Antiinflammatory, analgesic and possibly chondroprotective**
• Prolong effect due to – Re-establishment of Joint Homeostasis ( increase in endogenous production of Hyaluronate )***
Am J Sports Med 2009:37;1636-44*N Engl J Med 2015;372:1040-7***BMC Musculosketal disorders 2011, 12: 195**

Question
Disease-modifying OA drugs (DMOADs) or Structure-modifying OA drugs (SMOADs) causes which of the following?
1. pain pathways2. inhibition of catabolic processes 3. stimulation of anabolic processes 4. Any of the above

Answer
Disease-modifying OA drugs (DMOADs) or Structure-modifying OA drugs (SMOADs) causes which of the following?
4. Any of the above(pain pathwaysinhibition of catabolic processes stimulation of anabolic processes)

Question
• Which among the following medications has NO evidence for benefit in management of Osteoarthritis?
1. Duloxeteine2. Strontium Ranelate3. Adalimumab4. Both A & B

Answer
• Which among the following medications has NO evidence for benefit in management of Osteoarthritis?
3. Adalimumab

Investigational approaches to the management of OA
Targeting pain in OA
Inhibition of nerve growth factor-Tanezumab reduce knee pain - RCT - 450 patients with moderate to severe knee OA associated with rapidly progressive OA In 2015, phase III trials resumed
Duloxetine - FDA approved for chronic knee pain in OA Milnaciprin

Investigational approaches - Structural modification
Modify inflammatory pathways
TNF α inhibitors
IL-1β inhibitors
Matrix metalloproteinase inhibitors
Mitogen-activated protein kinase inhibitor
Inducible nitric oxide synthase inhibition cindunistat hydrochloride maleate
Bradykinin receptor B2 antagonist Icatibant, fasitibant

Investigational approaches - Structural modification
Cartilage catabolism and anabolism
Bone morphogenetic protein-7
Fibroblast growth factor spriferminPlatelet-rich plasma

Platelet-rich plasma• provide high concentrations of growth factors including
tissue growth factor and platelet-derived growth factors
More large RCTs needed
• Mesenchymal stem cells ± PRP – Active trials recruiting
• Efficacy of PRP injections in OA knee: a systematic review and meta-analysis.Laudy AB, et al Br J Sports Med. 2015 May;49(10):657-72.

Investigational approaches - Structural modification
Bone remodellingCalcitonin
Bisphosphonates BRISK trial Knee OA Structural Arthritis (KOSTAR) study
Strontium

Ayurvedic treatments• Decreased pain for Reumalex (willow bark+ guaiacum resin+ black cohosh+ sarsaparilla+ poplar bark) willow bark alone pine bark green-lipped mussel rose hip stinging nettle Articulin F (Indian frankincense + winter cherry + turmeric + zinc) devil’s claw extract of soybean and avocado unsaponifiables (ASU) Phytodolor (poplar bark+ ash bark+ goldenrod)
Herbal medicines for the treatment of OA: a systematic review. Long L, Soeken K, Ernst Rheumatology (Oxford). 2001;40(7):779.
Comparative effectiveness of a complex Ayurvedic treatment and conventional standard care in OA of the knee--study protocol for a RCT. Witt CM, Michalsen A, Roll S, Morandi A, Gupta S, et al Trials. 2013;14:149. Epub 2013 5 23.

ACR 2012 recommendations

By
Prof. (Dr.) R.N. HaldarWHO Fellow
Head, Dept. of Physical Medicine & RehabilitationIPGME&R, SSKM Hospital, Kolkata
NON PHARMACOLOGICAL MANAGEMENT
OSTEOARTHRITIS OF KNEE

Question 1
Normal knee joint is
1. 5 degree valgus2. 7 degree valgus3. 5 degree varus4. 7 degree varus

Answer
Normal knee joint is
1. 5 degree valgus

BIOMECHANICS• Joint placed between the largest and the
longest levers of the body – high load – liable to injury
• 3 joints within one capsule• Weight of two legs (7+7) =14%• Each knee support 43% (during double
stance)• Each knee support 93% (during swing phase)

BIOMECHANICS CONT.• During ADL force varies 3 to 7 times of body wt.• Medial side loaded 50% more than lateral side
due to adduction moment –so 90% OA in medial side
• 5° Physiological Valgus• > 185°– Knock Knee• < 175°– Bow leg• Compressive & tensile stress- Dynamic activity• Q angle- >20° are abnormal

MECHANICAL AXIS LINE (HKA LINE)
• 3° slanting with vertical line
• 6° with anatomical line

OARSI (OSTEOARTHRITIS RESEARCH SOCIETY INTERNATIONAL) GUIDELINES FOR MANAGEMENT OF OA KNEE (2007) : 12 key non
pharmacologic modalities1. Patient Education2. Self Management3. Social Support4. Weight Loss5. Aerobic Exercise 6. Physical therapy, ROM Exercise
OARSI (2014):
BALANEOTHERAPY
defined as using baths containing thermal mineral waters, was evaluated for the first time and found to be an appropriate therapy for patients with multi-joint OA and comorbidities, as this group has few other treatment options.
7. Muscle Strengthening Exercise
8. Assistive Devices For Ambulation
9. Patellar Taping10. Appropriate Footwear11. Lateral Wedged Insole12. Occupational Therapy

Question 2
Decrease in 5 kg body weight reduces the risk of OA knee by
1. 50%2. 40%3. 30%4. 20%

Answer
Decrease in 5 kg body weight reduces the risk of OA knee by
1. 50%

• Increased body wt. is associated with OA knee• Duration of obesity plays a cumulative role• Women is more in risk • Secretes adipokines from adipose tissue
Exercise – Quadriceps weakness, reduction in body fat, increased physical activitiesDietary Changes – Fat & Caloric restriction
4. WEIGHT LOSS(Decrease in wt by 5kg substantially reduces the risk of OA by 50% )

5. AEROBIC EXERCISE
• Aerobic conditioning – daily walking
• Aquatic therapy

6.PHYSICAL THERAPY , ROM EXERCISE MODALITIES: SURGE FARADIC STIMULATION, TENS, IFT, UST(Restricted)TRACTION: Controvertial
Target the factors which leads to disabilities
• Flexibility –ROM deficits - extension lag – articular changes, shorting of myotendinous structures, joint stiffness• Shorter muscle has biomechanical disadvantage for generating
forces – so stretching is essential prior to exercise• ROM – important functional activity (knee flexion required)
70° for walking83° for climbing stairs93° for getting up from a chair

Question 4
Most preferred muscle strengthening exercise in OA knee is
1. Multi-angle isometric quadriceps exercise 2. Isotonic exercise3. Isokinetic exercise4. None of the above

Answer
Most preferred muscle strengthening exercise in OA knee is
1. Multi-angle isometric quadriceps exercise

7. MUSCLE STRENGTHENING EXERCISE• Mainly quadriceps weakness• Closed kinetic chain exercise (preferable due to less
shear forces and synergistic movements and firing patterns than OKC)
• Isometric - initial painful inflamed joint• Isotonic - eccentric, concentric contraction • Isokinetic – movement done with same speed at a
specified range. CKC and isotonic ex.- most beneficial Multi-angle isometric exercise performed at the knee increase strength throughout the knee range

8. ASSISTIVE DEVICES FOR AMBULATION

9. PATELLAR TAPING
• 25% patellofemoral pain reduced by medial patellar taping
• Immobilization • Pain relief• Unloading brace – 3 point system• Neoprene sleeves • Infra patellar straps

KNEE ORTHOSES• FOR MILD OSTEOARTHRITIS
– Sleeve-style wrap• support and compression
– Knee Sleeve
• FOR MILD to MODERATE OA– Functional knee orthoses
• FOR MILD to MODERATE OA Knee orthoses with patellar hole
• FOR SEVERE OSTEOARTHRITIS with varus deformity at knee and neutral ankle– Unloader knee Orthoses
• 3-Point Off-Loading : shifts joint loads• Hinge: fine-tune the load

10. APPROPRIATE FOOTWEAR
• Shock absorbing insole (visco elastic)
• No genu varum
• Reduces incoming shock wave 42%
• Improves symptoms by 78%

11. LATERAL WEDGED INSOLE
• Genu varum deformity (75%)
• Commonly 5°
LATERAL SUBTALAR WEDGING

12. OCCUPATIONAL THERAPY
• To improve mobility and strength
• To maximize independence
• To educate the patient
• To reduce pain
• Joint protection • Energy conservation
• ADL Training

NONPHARMACOLOGIC RECOMMENDATIONS FOR THE MANAGEMENT OF KNEE OA (ACR 2012)
We strongly recommend that patients with knee OA should do the following:
• Participate in cardiovascular (aerobic) and/or resistance land-based exercise
• Participate in aquatic exercise• Lose weight (for persons who are overweight)

NONPHARMACOLOGIC RECOMMENDATIONS FOR THE MANAGEMENT OF KNEE OA
We conditionally recommend that patients with Knee OA should do the following:• Participate in self-management programs• Receive manual therapy in combination with supervised exercise• Receive psychosocial interventions• Use medially directed patellar taping• Wear medially wedged insoles if they have lateral compartment OA• Wear laterally wedged subtalar strapped insoles if they have medial compartment
OA• Be instructed in the use of thermal agents• Receive walking aids, as needed• Participate in tai chi programs• Be treated with traditional Chinese acupuncture*• Be instructed in the use of transcutaneous electrical stimulation

NONPHARMACOLOGIC RECOMMENDATIONS FOR THE MANAGEMENT OF KNEE OA
We have NO recommendations regarding the following:
• Participation in balance exercises, either alone or in combination with strengthening exercises
• Wearing laterally wedged insoles• Receiving manual therapy alone• Wearing knee braces• Using laterally directed patellar taping

PROPRIOCEPTIVE TRAINING
• Variation in standing• Standing on different surface • Walking• Computer foot game • 10 weeks training • 4 sessions /week

TAI-CHI EXERCISE • Patients with osteoarthritis
of the knee benefit from Tai Chi by increasing lower extremity muscular strength and joint stability
• Tai Chi typically includes a series of dance-like movements that combine to postures or forms. The forms are executed using slow and smooth movements that flow into each other

VIBRATION PLATFORM FOR IMPROVING BALANCE1. Static exercise 2. Dynamic exercise – 2
sessions / week training for 8 weeks
Improve muscle strength and proprioception

IONTOPHORESIS WITH ACETIC ACID
• Reduce calcific deposits and bone spurs
• Insoluble calcium in the form of calcium pyrophosphate reacts with acetic acid to form calcium acetate, which is more soluble and therefore, more easily dissolved by our body fluids (synovial fluid, blood)

CLASS IV LASER THERAPY
• Reduce pain, inflammation, and enhance tissue healing of muscle, ligaments and bones
• Increase circulation and oxygenation of tissues >RBC’s to area and increasing venous and lymphatic return
• Non-invasive use of laser energy to generate a photochemical response (helping cells produce ATP/energy) in damaged or dysfunctional tissue

PILATES BASED REHABJoseph Pilates: exercise format embodying “complete coordination of body, mind and spirit”
Benefits: increases range of motion increases flexibility increases strength increases spine stabilization improves balance improves posture enhances body awarenessdecreases joint stress enhances breathing

Total knee replacement exercise protocol Outline: PRE-OPERATIVE
• ROM Exercises.• Stretching• Strengthening exercise.• Foot-Ankle Exercises• Breathing Exercises• Exercises for DVT prophylaxix

Total knee replacement exercise protocol Outline
• Postoperative day 1 Bedside exercises (e.g. ankle pumps, quadriceps exercises…)
• Postoperative day 2 Exercises for active ROM and terminal knee extension Gait training with assistive device
• Postoperative day 3-5 Progression of ambulation on level surfaces and stairs (if
applicable)• Postoperative day 5 to 4 weeks
Stretching of quadriceps and hamstring muscles Progression of ambulation distance

OA PANEL DISCUSSION
Dr Vinod PadmanabhanConsultant Orthopaedic & Joint Replacement Surgeon
Sree Sudheendra Medical MissionKochi

Surgical Management of OA
• Arthroscopic lavage• Corrective osteotomy• Unicompartmental knee arthroplasty• Total knee replacement

ARTHROSCOPIC DEBRIDEMENT

Arthroscopic Debridement
• Knee Surg Sports Traumatol Arthrosc. 2015Arthroscopy for mechanical symptoms in osteoarthritis: a cost-effective procedure. Hutt et alSignificant improvements in pain and function. The procedure gave good patient satisfaction.
• Saudi Med J. 2009 Jun;30(6):809-12.Arthroscopic joint lavage in osteoarthritis of the knee. Is it effective? Al-Omran AS, Sadat-Ali MBenefits in the extent of pain relief and improvement of joint mobility and delay of definite arthroplasty

High Tibial Osteotomy (HTO)

HTO - Wheel alignment

High Tibial Osteotomy
Indications• Relatively young (<55 years)• Unicompartmental degeneration• Relatively thin• Without ligament instability• Relative sparing of P-F joint• Without Flexion deformity

• Joints. 2016 Jun.Opening-wedge high tibial osteotomy: a seven - to twelve-year study. Pipino et alGood or excellent results were obtained in 94% of the cases ; Still a reliable method for correcting varus deformity ; Satisfactory mid- to long-term results.
• Curr Rev Musculoskelet Med. 2014High tibial osteotomy. Bonasia DE et alExcellent early survivorship and good clinical outcomes were reported ; Correct indications, preoperative workup/planning, and technique selection are essential in achieving good results
High Tibial Osteotomy

Unicondylar Knee Arthroplasty(U.K.A.)
• Partial knee replacement
• Unicompartment OA• Minimally invasive
method• Ligaments intact• Early mobilisation• Short hospital stay

U.K.A.

U.K.A. v/s H.T.O.
• Arch Bone Jt Surg. 2016 Oct.• Unicompartmental Knee Osteoarthritis: UKA
or HTO? Rodriguez-Merchan EC• Eighteen articles were selected and reviewed• In a meta-analysis, the ratio for an excellent
outcome was higher in UKA than HTO• A systematic review has found that with correct
patient selection, both procedures show effective and reliable results

TKR

When shall a Rheumatologist refer a OA knee patient for TKR
1) Grade II2) Grade III3) Grade IV4) None of the above

4) None of the above
• Indications are mulifactorial– Pain– Loss of function of knee joint– Difficulty in performing ADL– Personal factors like funds, relatives support

Absolute contraindication to TKR
1) Active sepsis2) Absence of extensor mechanism3) Neuropathic joint4) All of the above

4) All of the above
Relative contraindications• Very young patient <40 yr• Patient demanding heavy activities• Unreliable patient

50 year old manual labourer with Grade III medial compartment OA ; 15 degree varus
deformity; intact ACL and Post horn medial meniscus injury
What is the best treatment modality?
1) Conservative Management2) Arthroscopic Meniscal surgery3) Arthroscopic debridement + H.T.O.4) Joint Replacement surgery

3) Arthroscopic debridement with High Tibial Osteotomy
• Cost effective• Gives excellent results for at least 10 years • Patient can resume his occupation
– Deep squats– Sitting on floor– Lifting weights
• Can be easily converted to TKR in future (if needed)

POST OP X-Ray

3 months post op
BEFORE AFTER

2 yr post-op

PROFOUND VARUS

55 years old lady with severe varus deformity of both knees, walks with
difficulty with walker support ; X-ray - Severe osteoporosis, Gr IV OA
changes, Femoral and tibial varus
1) Conservative treatment2) Corrective osteotomy of femur and tibia3) Bilateral TKR – Staged (gap of one week)4) Bilateral TKR – single stage

4) Bilateral TKR – single stage
• Single stage – Many advantages– Single anesthesia and OT visit– Cost effective– Safe without added risk of complications– Very effective in severe deformities
• Chance of complications highest if second surgery is done during first two weeks
• Staged TKR - at least a gap of 6 months

Single v/s Two stage• J Arthroplasty. 2014 Mar
Comparison of postoperative morbidity between simultaneous bilateral and staged bilateral TKA: serological perspective and clinical consequences. Niki et al6 months were saved ; a safe and effective procedure in appropriate clinical settings involving anti-bleeding and anti-VTE prophylaxis.
• Acta Orthop Belg. 2015 Dec;81(4):784-9.Comparison of the effectiveness and safety of one-stage versus two-stage bilateral total knee arthroplasty. Zhao YT e alOne-stage BTKA may be safely performed with similar knee function to those of two-stage procedure; Benefit of single anaesthetic, reduced costs and decreased hospital stay when compared to two-stage BTKA.

BEFORE AFTER

Pre-op X-ray
Post-op X-ray

2 years post-op

Most common early complications in post Total Knee Replacement
1) Infection2) DVT leading to Pulmonary embolism3) Neurovascular Injury4) Acute Renal Failure

2) DVT leading to Pulmonary embolism
• Thirty-Day Postoperative Complications and Mortality Following Total Knee Arthroplasty Incidence and Risk Factors Among a National Sample of 15,321 Patients Philip J. Belmont et al JBJS 2014
Infection=0.30%, DVT= 0.78%, NV injury=0.10%, ARF=0.10%
• Lack of registry data from India• In India, Infection has to be kept in mind

10-years implant survival Rate for Primary Total Knee Replacement in OA Knees
1) 60-70 %2) 70-80 %3) 80-90 %4) >90 %

4) >90 %
• 94% survival rate for 10 years • Then onwards 1% reduction every year. • 15 year follow-up of 32476 TKR in Norwegian
Arthroplasty Register • Mona et al 10 June 2015

Most common indication for Revision TKR
1) Infection2) Aseptic loosening3) Dislocation4) Periprosthetic fracture

2) Aseptic loosening
15 year follow-up of 32476 TKR in Norwegian Arthroplasty Register) Mona et al 10 June 2015• Loosening = 28%• Infection = 21%• Dislocation = 20%• Pain = 6%• Others = 25%

CONCLUSION
• Corrective osteotomy has a great role in middle aged patients with early arthritis and deformity
• Joint replacement surgery greatly improves quality of life in elderly
• 15-yr survival rate of implant is 90%• Aseptic loosening is leading cause of revision
TKR.

Take home message
1. Communication and expectations
2. Non Pharmacological & Pharm Treatment
3. I/A Steroids – Frequency
4. Viscosupplementation
5. Surgery