Embed Size (px)
Citation preview

VENTILATION FUNDAMENTAL
S Dr Bikash Shrestha
Fellow Neonatology (NNF, India)MD Paediatrics (AFMC, Pune, India)

OVERVIEW REPSIRATORY PHYSIOLOGY
VENTILATOR BASICS

RESPIRATORY PHYSIOLOGY
Basic characteristics Oxygenation Ventilation Lung volumes Lung mechanics

BASIC CHARACTERISTICS-1 Higher respiratory rate

BASIC CHARACTERISTICS-2 Higher propensity to respiratory failure
–More cylindrical thorax of newborns–Horizontal placing of ribs–Compliant chest wall-lower propensity to
spring out–Closing volume almost equal to FRC

BASIC CHARACTERISTICS-3 Higher propensity to respiratory failure
– Diaphragmatic attachment more horizontal– Low muscle mass and less type I muscle fibers– Liver is relatively larger organ– Dramatic increase in airway resistance (Narrow
airway)– Lung growth takes place in centripetal direction
with relatively larger anatomic dead space

OXYGENATION-1 Extraction of oxygen from the atmosphere
and delivery into the mitochondria Directly correlated with the partial pressure
of oxygen in the alveoli (PAO2) Partial pressure of oxygen in artery (PaO2) Alveolar arterial oxygen gradient (PAO2 –
PaO2) = 5 - 15 mm Hg

ALEVOLAR GAS EQUATION

HYPOXEMIA-1
Hypoxic gas mixture (Low FIO2)
High altitude (Low PB)
Hypoventilation (High PACO2)

HYPOXEMIA-2
Increased alveolar arterial oxygen gradient (PAO2 – PaO2)
Ventilation perfusion mismatch (shunts)

HYPOXEMIA-3Ventilation perfusion mismatch (shunts)

VENTILATION-1 Elimination of CO2 from the blood through the
alveolus
PaCO2 is proportional to minute ventilation (VE)
PaCO2 is accurately correlated to mean alveolar minute ventilation

VENTILATION-2
Problem in ventilation (PaCO2)–Reduced RR–Reduced tidal volume–Increased dead space

LUNG VOLUMES

LUNG MECHANICS Elastic recoil
Compliance
Resistance
Time constant

ELASTIC RECOIL-1The tendency of stretched objects
to return to their original state

ELASTIC RECOIL-2
The forces tending and resisting to collapse are equal at a point close to FRC or resting state

ELASTIC RECOIL-3
Surface tension is correlated with elastic recoil
Surface tension follows Laplace law
P = 2T R

ELASTIC RECOIL-4

ELASTIC RECOIL-5

COMPLIANCE-1Change in volume resulting from a
given change in pressure

COMPLIANCE-2

RESISTANCE Resistance is resulted due to friction Viscous resistance and airway resistance VR-Generated by tissue elements moving
past one another AR-Generated within the respiratory tract
against the gas flow R = P1-P2
V(Flow)

TIME CONSTANT-1 Time necessary for the alveoli to discharge
63% of TV

TIME CONSTANT-2 Pressure changes at alveoli lag behind at the
proximal airway
Inspiratory and expiratory time constants

TIME CONSTANT-3

TIME CONSTANT-4 3 time constants lead to 95% equilibrium
of alveolar and proximal airway
R (Resistance) X C (Compliance)=0.15 secs
3 time constants = 0.45 secs

VENTILATOR BREAKTHROUG
HS

KENNEDY TRAGEDY
1963-Patrick Bouvier Kennedy (34 wks POG/2.1 kg) RDS-succumbed at 39 hrs

VENTILATOR BASICS

VENTILATOR BASICS Introduction
Basic terminologies
Oxygenation-MAP
Modes of ventilation
Pulmonary graphics

INTRODUCTION Movement of gas into and out of lungs by
an external source connected directly to the patient
Supportive, non therapeutic technology
Most neonatal ventilators based on Ayer’s T-piece

AYER’S T-PIECE

BASIC PARTS Pressurized source
Blending chamber
Flow control
Exhalation valve

BASIC TERMINOLOGIES
PIP – Peak inspiratory pressure PEEP – Positive end expiratory pressure Rate - Frequency Ti – Time allowed for inspiration Te – Time allowed for expiration IE ratio – 1:1 to 1:3
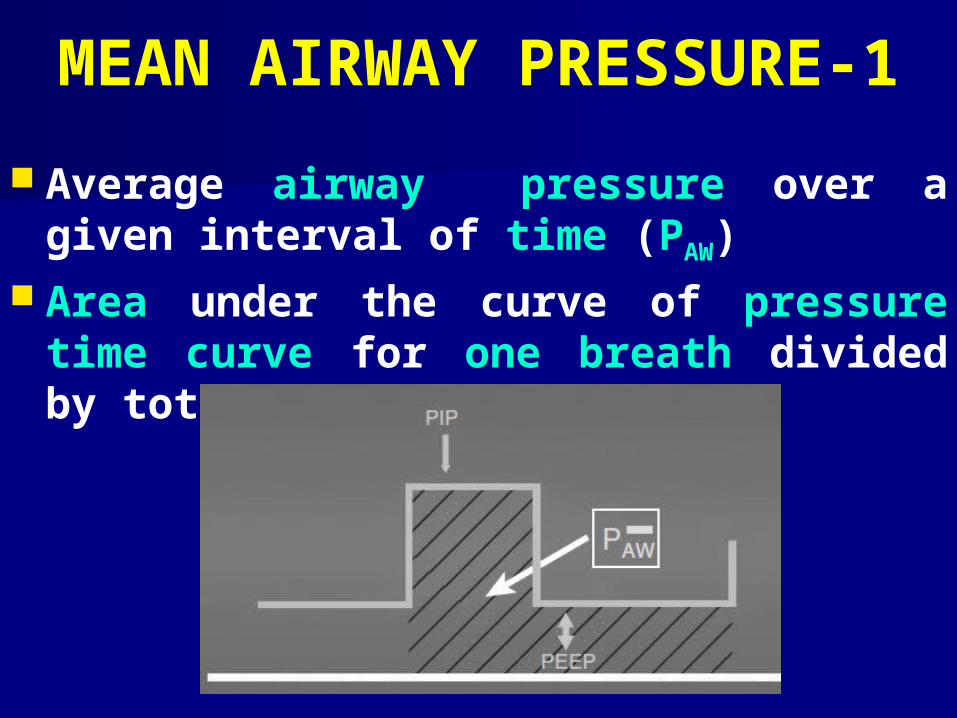
MEAN AIRWAY PRESSURE-1
Average airway pressure over a given interval of time (PAW)
Area under the curve of pressure time curve for one breath divided by total cycle time

MEAN AIRWAY PRESSURE-2

MODES OF VENTILATION-1 Three factors
–How each breath is initiated–How gas flow is controlled during delivery–How the breath is terminated

MODES OF VENTILATION-2
Breath initiation– Controlled– Synchronized or patient triggered
Gas flow control– Pressure– Volume
Flow termination (Cycling)– Volume cycling -Time cycling– Pressure cycling -Flow cycling

MODES OF VENTILATION-3

PULMONARY GRAPHICS-1
Introduction– Relatively new (1980’s)– Microprocessor development (1990’s)
Basis– Sensor with tungsten wire at the proximal airway– Heated wire anemometer technology– Gas flow results in cooling of the wire – Electricity required to bring it back to original temperature is
converted to signals

PULMONARY GRAPHICS-2 Colors
– Inspiration (Red-machine) (Yellow-patient)– Expiration (Blue)– Auto calibrating (Green)
Common signals– Pressure (cm of H2O)– Volume (mL)– Flow (mL/sec)

PULMONARY GRAPHICS-3

PULMONARY GRAPHICS-4
Cyclic phases
– A -Initiation of inspiration
– B -Peak inspiration
– C -End inspiration
– D -End expiration

“Primum non nocere” (First do no harm)
The first tenet of Hippocratic oath

REFERENCESM Keszler. Update on mechanical ventilator strategies. Neoreviews.
2013;14:e237.
AK Ghuman, RG Khemani, CJL Newth. Pediatric applied respiratory physiology-the essentials. Pediatrics and Child Health. 2013;23:7.
PD Sly, RA Collins. Physiological basis of rspiratory signs and symptoms. Pediatric Respiratory Reviews. 2006;7:84-88.
PC Rimensberger. Pediatric and Neonatal Mechanical Ventilation-From Basics to Clinical Practice. Berlin. Springer-Verlag. 2015.
JP Goldmsith, EH Karotkin. Assisted Ventilation of the Neonate. 5th ed. USA. Saunders-Elsevier Imprint. 2015.
SM Donn, MC Mammel. Neonatal Pulmonary Graphics-A Pocket Atlas. New York. Sprigner. 2015.

DESIRABLE CME’S Basics of neonatal ventilation
Pulmonary waveforms fundamentals
Non invasive neonatal ventilation
Newer modes of ventilation
CPAP-Essential tool in NICU’s

THANK YOU














![[PPT]Gentle Ventilation - Neonatal Research · Web viewGentle Ventilation We all want to do it… but what is it? Outline: Avoiding ventilator induced lung injury Permissive Hypercapnia](https://img.dokumen.tips/doc/110x75/5b0504b37f8b9a6c0b8e9bdb/pptgentle-ventilation-neonatal-research-viewgentle-ventilation-we-all-want-to.jpg)














