Embed Size (px)
Citation preview


Prof. Mohamed El Kalioby
Prof. of Pediatrics & Neonatology
Suez Canal University

COMMON NEONATAL
GASRTINTESTINAL PROBLEMS

ITEMSITEMS• Vomiting• Constipation• Diarrhea• Abdominal Colic• NEC • Congenital Anomalies
Cleft lip / palateTEFCHPSAtresia

NEONATAL VOMITINGNEONATAL VOMITING

NEONATAL VOMITINGNEONATAL VOMITING
Vomiting or, more often, regurgitation is a relatively frequent symptom during the neonatal period.

NEONATAL VOMITINGNEONATAL VOMITING
In the first few hours after birth, infants may vomit mucus, occasionally blood streaked. This vomiting rarely persists after the first few feedings.
It may be due to irritation of the gastric mucosa by material swallowed during delivery.
If the vomiting is protracted, gastric lavage with physiologic saline solution may relieve it

NEONATAL VOMITINGNEONATAL VOMITING
Many babies vomit at some time.
In most cases this is unimportant and unlikely to be clinically significant.
Small, frequent vomits are referred to as ‘posits’.

NEONATAL VOMITINGNEONATAL VOMITING
• Spitting up (About 40%)Not forceful. Small volumes (< 5-10 mL) during or shortly
after feeding, often when being burped.Typically caused by rapid/overfeeding and air
swallowing.Gentle patting on the infant's back should be all
that is required during a spitting up episode.

NEONATAL VOMITINGNEONATAL VOMITING
• Infant regurgitation
Vomiting ≥ 2 times/day for at least 3 weeks in the first 1-12 months of life in an otherwise healthy infant.
Often transient in nature and due to immature gastrointestinal tract (GER).

NEONATAL VOMITINGNEONATAL VOMITING
Management of Infant regurgitationReassurance is the only treatment needed.Conservative measures:
Upright positioning after feeding,
Elevating the head of the bed?Domperidone:
Dose: (0.25–0.5 mg/kg/dose (3-4 times/day. Maximum 2.4 mg/kg/d or 80 mg/ d).

NEONATAL VOMITINGNEONATAL VOMITING
WarningWarning• Vomit contains blood (red or black)
(Colour depends upon how long blood has been in the stomach)• Vomit is bile (green, not yellow)• Vomiting is projectile• Baby is unwell• Baby is failing to thrive• Baby has GER (could be aspirating)• Associated diarrhea• Abdomen is distended

NEONATAL VOMITINGNEONATAL VOMITING
Vomiting occurs shortly after birth and persistent:Intestinal obstruction, Metabolic disorders, and ?Increased intracranial pressure.
A history of maternal hydramnios suggests upper gastrointestinal (esophageal, duodenal, ileal) atresia. Bile-stained emesis suggests intestinal obstruction beyond the duodenum.

NEONATAL VOMITINGNEONATAL VOMITING
Abdominal roentgenograms:air-fluid levels, distended bowel loops, characteristic patterns of obstruction (double bubble: duodenal atresia), and pneumoperitoneum (intestinal perforation).
air-fluid levels

NEONATAL VOMITINGNEONATAL VOMITING
• A barium swallow roentgenogram with small bowel follow-through is indicated in the presence of bilious emesis.
• Ultrasonography (CHPS)

NEONATAL VOMITINGNEONATAL VOMITING
A 7 day old baby, born at term, presented to the neonatal unit with a history of vomiting with each feed and 20% weight loss (birth weight 3270 g). Vomiting started soon after birth and it was described by the parents as being projectile; it occurred during or after feeds and was non-bilious. The baby was dehydrated on admission (dry skin and mucous membranes), but was otherwise well. Clinical examination was otherwise unremarkable including no visible peristalsis and no masses palpable. The parents interacted appropriately with the baby and there were no causes for concern among the nursing or medical staff. Initial capillary blood gas analysis showed a metabolic alkalosis.

NEONATAL VOMITINGNEONATAL VOMITING
What is the main diagnosis to exclude?
Hypertrophic pyloric stenosis: ABG classically shows hypochloraemic hypokalaemic metabolic alkalosis.

NEONATAL VOMITINGNEONATAL VOMITING
What investigations would you perform to diagnose this?
Ultrasound scanning:non-invasive, does not use radiation, and can differentiate between several diagnoses (hypertrophic pyloric stenosis, gastro-oesophageal reflux disease, and duodenal anomalies).

NEONATAL NEONATAL CONSTIPATIONCONSTIPATION

Normal bowel habitsFirst bowel movement: within 36 h of birth (later in preterm).90 % of normal newborns pass meconium within 24 h.
During the first week of life: approximately four soft or liquid bowel movements per day (generally more in breast- compared with bottle-fed infants).
During the first three months of life: breastfed infants have about three soft bowel movements per day. Some breastfed infants have a bowel movement after each feeding, whereas others have only one bowel movement per week.

DEFINITIONDefinition of constipation is relative and depends on:•stool consistency, •stool frequency, and •difficulty in passing the stool.
“a delay or difficulty in defecation, present for two or more weeks, sufficient to cause significant distress to the patient”

A normal child may have a soft stool only every 2 or 3 days without difficulty; this is not constipation.
However, a hard stool passed with difficulty every 3rd day should be treated as constipation.

Constipation is common and varies considerably in its severity
The clinician has an important role in identifying the small fraction of children with organic causes of constipation.
ETIOLOGYConstipation may arise from:
I. defects in filling the rectum
II. defects in emptying the rectum or
colonic stasis
excessive drying of stool
failure to initiate reflexes from the rectum
Weak defecation reflex initiated by pressure receptors in the rectal muscle

ETIOLOGY
I. Defective rectal filling (colonic peristalsis is ineffective):hypothyroidism or opiate use and when bowel obstruction (by a structural anomaly or by Hirschsprung disease).

ETIOLOGY
II. Defective emptying the rectum: lesions involving rectal muscles, lesions of sacral spinal cord afferent and efferent fibers, or lesions affecting muscles of the abdomen and pelvic floor. Disorders of anal sphincter relaxation may also contribute to fecal retention

ETIOLOGY
Most children with constipation do not have an underlying medical problem.
WarningWarning Don’t pass meconium after 36 h. Dietetic Causes: Underfeeding /
Cow's milk intolerance. Associating vomiting.

MANAGEMENTBreast FeedingInfants who breastfeed are rarely constipated Glycerin suppositories or rectal stimulation with a lubricated rectal thermometer can be used occasionally if there is very hard stool in the rectum. These interventions should not be used frequently because tolerance may develop; in addition, glycerin may irritate the anus or rectal mucosa.

NEONATAL DIARRHEANEONATAL DIARRHEA

DEFINITION
WHO: passage of three or more loose or watery stools per day.
Nevertheless, absolute limits of normalcy are difficult to define; any deviation from the child's usual pattern should arouse some concern

Ill appearance, Dehydration, Passage of blood or
mucus, regardless of the actual
number of stools or their water content.

NEONATAL COLICNEONATAL COLIC

Colic is commonly described as a behavioral syndrome in neonates and infants that is characterized by excessive, paroxysmal crying. Colic is most likely to occur in the evenings, and it occurs without any identifiable cause.
Possible other causes of excessive crying (eg, having hair in the eye, strangulated hernia, otitis, sepsis); colic remains a diagnosis of exclusion.
ETIOLOGYGastrointestinal causes (eg, GERD, over- or
underfeeding, milk protein allergy, early introduction of solids)
Inexperienced parents (controversial) or incomplete or no burping after feeding
Exposure to cigarette smoke and its metabolites
Food allergyLow birth weightCharacteristic intestinal microflora

ETIOLOGY
Weight loss, Difficult or painful
swallowing, Significant vomiting,Chronic severe diarrhea,Blood in stool Unexplained fever, Urinary symptoms

MANAGEMENT
Rule out common causes of cryingRecommend that the parents not exhaust
themselves, and encourage them to consider leaving their baby with other caretakers for short respites
Consistent follow-up and a sympathetic physician are the cornerstones of management

MANAGEMENT 2
Drug treatment generally has no place in management of colic unless GERD appears likely.
?Anticholinergic agents: effective but has rare serious adverse effects and cannot be recommended.

MANAGEMENT 3
Various benign but unproven treatment modalities are available, including the following:Maternal low-allergen diet (ie, low in dairy, soy, egg, peanut, wheat, shell fish) may offer relief from excessive crying in some infants. Lactobacillus reuteri (Probiotics)SimethiconeOral hypertonic glucoseNutritional supplements and other complementary medicines

Necrotizing Enterocolitis
(NEC)

Necrotizing Enterocolitis 1
Risk Factors:•Premature infants•Feeding of concentrated formulas•GIT infections•Polycythemia, CHD

Necrotizing Enterocolitis 2
C/P•Nonspecific •History of formula feeding•Vomiting, diarrhea, feeding intolerance and high gastric residuals following feedings. •More specific: abdominal distention and frank or occult blood in the stools

Necrotizing Enterocolitis 3
C/P (Cont)GI signs: any or all of the following:•Increased abdominal girth•Visible intestinal loops•Obvious abdominal distention and decreased bowel sounds•Change in stool pattern•Hematochezia•Palpable abdominal mass•Erythema of the abdominal wall
Systemic signs: any of the following:•Respiratory failure•Decreased peripheral perfusion•Circulatory [email protected]
Necrotizing Enterocolitis 4
Management:•NPO•Nasogastric tube to decompress gas•IV fluid•Antibiotics•Extra oxygen•Abdominal x-rays to monitor progress•Measure abdominal girth every four hours
CONGENITAL ANOMALIESCONGENITAL ANOMALIES

Cleft Lip and PalateCleft Lip and Palate

Incomplete Cleft Palate
Unilateral Complete cleft lip & Palate
Bilateral Complete cleft lip & Palate

Treatment 2
Goals of surgery:Close the defectCosmetic: Symmetrical appearance of face
Timing of surgery:2 to 3 months

Treatment 5
Pre Surgery CareConstruction of a plastic obturator to assist in feedings.Use of soft artificial nipples with large openings, a squeezable bottle, and proper instruction

Treatment 6
Post Surgery Care Airway managementPain control Position in infant seat – upright positionElbow restraintsWound careMinimizing cryingFeeding techniques

Treatment 7
Cleft Palate RepairGoals of surgery:Union of the cleft segments, Intelligible and pleasant speech,Reduction of nasal regurgitation, and Avoidance of injury to the growing maxilla.
Treatment 8
Timing of Surgery:Variable according to:size, shape, and degree of deformity.adequacy of the existing palatal segments, morphology of the surrounding areas (e.g., width of the oropharynx), neuromuscular function of soft palate and pharyngeal walls.
Ideally: before 1 yr of age to enhance normal speech development. Babies should be weaned from bottle or breast.When surgical correction is delayed beyond 3rd yr, the child develop intelligible speech.

Treatment 9 Palate Repair
Pre-surgery feedingAlternate nipple design
Breast feeding consultant
ESSREnlarge / stimulate / swallow / rest

Treatment 12
Post Surgery CarePosition on sideNPO for 48 hoursSuction with bulb syringe onlyAvoid injury to palate with syringes, straws, cups etc.
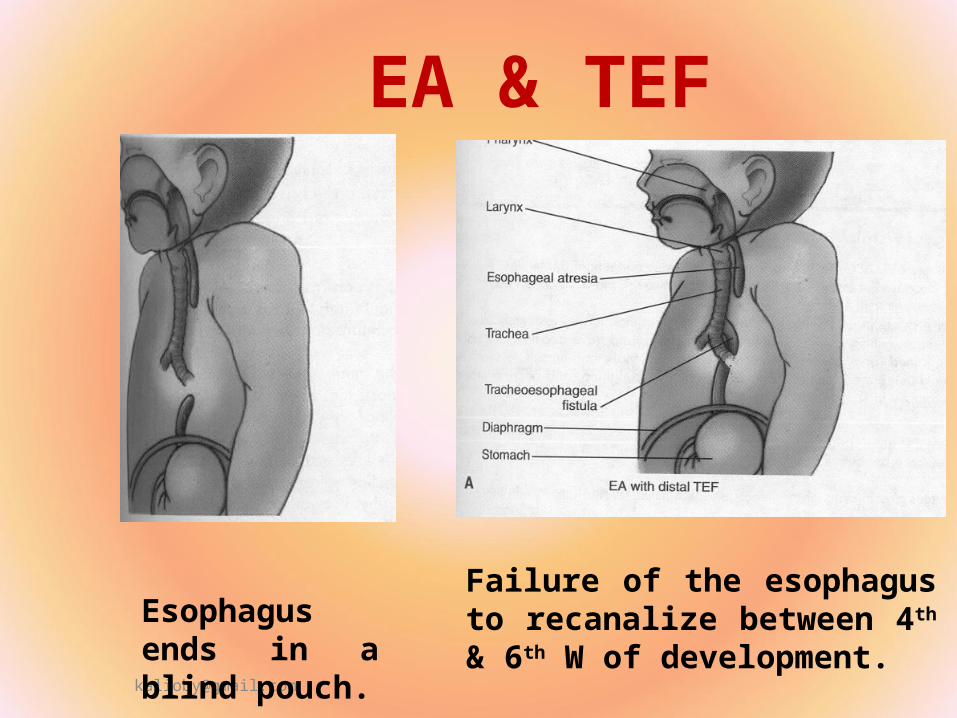
EA & TEF
Esophagus ends in a blind pouch.
Failure of the esophagus to recanalize between 4th & 6th W of development.

ES & TEF 2
Type A – Esophageal atresia without tracheoesophageal fistula (8-10 %)Type B – Esophageal atresia with proximal tracheoesophageal fistula (<1 percent)Type C – Esophageal atresia with distal tracheoesophageal fistula (85-87 %)Type D – Esophageal atresia with tracheoesophageal fistula to both the proximal and distal esophageal segments (<1 percent)Type E – Tracheoesophageal fistula with no esophageal atresia (4 %)

ES & TEF 3
Symptoms and Signs: Excessive salivation / frothy mucus Respiratory Distress Inability to pass NG tube (Except ?) Choking and coughing on feeding (The
rationale for giving sterile water for the first feed).
Diagnosis: – Clinical– CXR