Embed Size (px)
Citation preview

The Nuts and Bolts of Building a Telehealth Program
Jonathan Neufeld, PhD
Georgia Partnership for Telehealth Conference
Savannah, Georgia
March 26, 2015
1
This project is/was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of
Health and Human Services (HHS) under grant number G22RH24745-03-00 under the Telehealth Resource Center
Grant Program for $325,000. This information or content and conclusions are those of the author and should not be
construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.


3

4
Bureau of Primary Care
Maternal and Child Health Bureau
Bureau of Health Workforce
Office of Rural Health Policy
Healthcare Systems Bureau
HIV/AIDS Bureau
HRSAOffice of the
Administrator
Office of the Deputy Administrator
Health Resourcesand Services
Administration (HRSA)

telehealthresourcecenters.org
• Links to all TRCs
• National Webinar
Series
• Reimbursement,
Marketing, and
Training Tools

UMTRC Services
• Presentations & Trainings
• Individual and Group Consultation
• Technical Assistance
• Connections with other programs
• Program Design and Evaluation
• Information on current legislative and policy developments
6

Introduction to Telehealth
• Telehealth refers to a set of methods for delivering health care services
– NOT the services themselves or a specific type of service
• For example, “tele-radiology” is just radiology performed from a remote site
• The provider would do the same thing if they were on site, the patient would receive the same care
– NOT all health care technologies
• EMRs, use of computers and tablets, robotics
7

“Telehealth” vs. “Telemedicine”
• Often used interchangeably (ATA)
• Two types of distinctions are made -
• “Telemedicine” = billable interactive clinical services performed at a distance
• “Telehealth” =• All remote health activities (CME, etc.)
• Clinical remote monitoring (usually at home)

Types of Telehealth• Specialty/Subspecialty
• Allergy/ImmunologyAnesthesiaCardiologyCritical CareDentistryDermatologyOtolaryngology (ENT)EndocrinologyFamily/General PracticeGastroenterologyInfectious DiseasesInternal MedicineMaternal/Fetal MedicineMental/Behavioral HealthNeurologyOncology/HematologyOphthalmology/OptometryOrthopedicsPathologyPediatricsPsychiatryPulmonologyRehabilitative MedicineRheumatologySurgeryUrology
• Services
• Case ManagementCorrectional telehealthDeaf/hearing servicesDiabetic retinopathy screeningDietician servicesDisease managementDoctor-to-doctor consultationEnterostomal therapyForensic/court servicesGenetic counselingLong-term CareNeonatal/Pediatric intensive care unitPain managementPalliative carePre/post-natal careSpeech therapySpine therapyTelestrokeWound careAdult, Individual and Group TherapyBehavioral psychology and healthChemical dependency aftercareChemical dependency therapy (Addiction therapy)Consultation to SchoolsCouples’ counselingDevelopmental (lifespan) counselingPsychiatric medication therapy managementPsychological Assessment
9

1906 - Einthoven’s Telecardiogram
10

1950s - John Mackenzie at Smith Kline
televises over 300 medical and surgical procedures
11

1960s – Dr. Kenneth Bird (Harvard)
12

13

14
Murphy RL, Bird KT. Telediagnosis: a new community health resource. Observations on the feasibility of telediagnosis based on 1000 patient transactions. Am J Public Health. 1974;64(2):113-119.

1965 - Transatlantic Telemedicine
15

1971 – Child Psychiatry (Nebraska)
16

The Bare Necessities
• Clinical Business Model
• Team of Champions
• Solid Partners
• Appropriate Technology
17

Clinical Business Model
• Identifiable need(s)
– Assessment tools
– Consensus value
• Value-bearing service to meet the need(s)
– Reimbursement, cost savings, or other value
• Services that fit within best practices and legal limitations
– Licensing boards (regulations)
– Payers (conditions of payment)18

Legal Limitations
19
• Professionals (doctors, nurses, counselors, etc.) are regulated by state licensing boards
• Medicare: Pays for certain outpatient professional services (CPT codes) for patients accessing care in rural counties and HPSAs in rural census tracts.
*Codified as “conditions of payment”
• Medicaid: Most states (46) cover at least some telehealth services.

Three Domains of Telehealth
• Hospital & Specialty Care• Specialists see and manage patients remotely
• Integrated Primary Care• Mental health and other specialists work in
primary care settings (e.g., PCMH’s, ACO’s)
• Transitions & Monitoring• Patients access care (or care accesses patients)
where and when needed to avoid complications and higher levels of care
**Value proposition differs among these types**
20

Hospital and Specialty Care
21

Three Domains of Telehealth
• Hospital & Specialty Care• Specialists see and manage patients remotely
• Integrated Primary Care• Mental health and other specialists work in
primary care settings (e.g., PCMHs, ACOs)
• Transitions & Monitoring• Patients access care (or care accesses patients)
where and when needed to avoid complications and higher levels of care
**Value proposition differs among these types**
22

Integrated Primary Care
23

Three Domains of Telehealth
• Hospital & Specialty Care• Specialists see and manage patients remotely
• Integrated Primary Care• Mental health and other specialists work in
primary care settings (e.g., PCMH’s, ACO’s)
• Transitions & Monitoring• Patients access care (or care accesses patients)
where and when needed to avoid complications and higher levels of care
**Value proposition differs among these types**
24

Transitions and Monitoring
25

Three Domains of Telehealth
• Hospital & Specialty Care• Specialists see and manage patients remotely
• Integrated Primary Care• Mental health and other specialists work in
primary care settings (e.g., PCMH’s, ACO’s)
• Transitions & Monitoring• Patients access care (or care accesses patients)
where and when needed to avoid complications and higher levels of care
**Value proposition differs among these types**
26

Three Axes of Telehealth
27

Three “Hard Lines” in Telehealth
Encounter Patient Location Service Type
Live videoHealthcare facility
(hospital, clinic, office, etc.)
Individually codedand billed services
Store & Forward (images)
Non-facility(home, etc.)
Monitoring & Management
28
NOT: telephone, email, fax

Multiple Business Models Apply
Strategies Dependent Upon:
• Revenue Stream
• Cost Avoidance
• Added Value
• Shared Savings
**Each may apply to different stakeholders
29

Business Models for Telehealth
• Tele[specialty] Services
• Travel Reduction/Resource Distribution
• Remote Hiring/Recruiting/Retention
• Remote Monitoring & Access
• Kiosks and mHealth
30

Business Models for Telehealth - 1
SPECIALISTS TO REMOTE SITES
• Traditional “Hub & Spoke” arrangement
• Standard Pro-fee Payment (CPT-based) goes to Specialist or Hub (“remote site”)
• Facility fee goes to Patient or Spoke Site
– Called “originating site”
– Commonly $22-$25 per encounter
– NOT the same as “facility fee” in Part A
31

Telemedicine - The Standard Model
Professional Fee(Part B)
Facility Fee(Part B)
Rural “originating
site”
Specialist at “distant
site”

Business Models for Telehealth - 2
TRAVEL REDUCTION/SERVICE DISTRIBUTION
• Site-to-site within an organization
• No real “hub” or “spoke”
• Facility fees excluded (?)
• Goals:
– Reduced travel
– Increased capacity
– Increased efficiency
33

Business Models for Telehealth - 3
REMOTE HIRING, RECRUITMENT & RETENTION
• Recruit from anywhere to anywhere
• Recruit from lower cost locales
• Retain staff when they move
• Key consideration: Licensure
– Services occur at the site of the patient
– Providers must be licensed and credentialed at the patient's location
34

Business Models for Telehealth - 4
REMOTE MONITORING & ACCESS
• Moving the care site to the home (or street)
• Multiple privacy/confidentiality issues
– Informed consent is critical
• Tremendous potential for cost savings
• Overall quality of life improvements
– Staying out of the hospital = better
35

Business Models for Telehealth - 5
HEALTH KIOSKS AND mHEALTH
• Standalone diagnostic centers and smart phone/tablet apps
• Developed and distributed by providers, payers, or third parties
• Targeted directly to consumers
– Enhanced access, self-care, motivation
• Used doctor to doctor or hospital
– Image distribution, diagnosis, consultation36

Business Models for Telehealth - 5
HEALTH KIOSKS AND mHEALTH
• FDA has moved to regulate health apps
– Regulated if it measures or calculates data
• Direct patient payments are a small part of all health care dollars
• Goals are varied (and sometimes unclear)
– Access (to doctors, labs, charts, etc.)
– Outreach (to patients)
– Health behavior change (diet, exercise)37

The Triple Aim - A Realistic Approach
• Services done right will improve Patient Experience (Better Care)
38
• Providing the right services will improve Population Health
• Better Health will lead to Lower Cost

Telehealth in a Triple Aim ContextThe right tool changes everything…
39

A Team of Champions
• Leadership must understand and communicate the vision
• Key players must be flexible and open to new ideas, processes, and technologies
• Knowledgeable support – The TRCs
40

Key Players
• Key players must be flexible and open to new ideas, processes, and technologies
– Start with those most interested and easiest to work with
– Let excited team members recruit peers
– Leave the last 20%
41

A Note About Physicians
• Trained to lead
• Compliance is their livelihood
• Deathly allergic to “not knowing”
SO…
• Build trust
• Test in “non-critical” environments
• Emphasize relationships not technology
42

The Right Partners
• Multiple types of partnerships are available
• Build on existing relationships
• Ask for what you want –
Be the Hub!
43

Telemedicine - The “Legacy” Model
Professional Fee(Part B)
Facility Fee(Part B)
Rural “originating
site”
Specialist at “distant
site”

Direct Contracting – P2P
• Newer model
• Driven by:
– Accessibility of technology
– More sophisticated primary care
– Demand for services closer to patient
– Breakdown of traditional “Hub & Spoke” spheres of influence
45

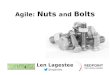
Hub and Spoke Telemedicine
HUB
Spoke
ptpt
ptpt
pt
Spoke
ptpt
ptpt
pt
Spoke
ptpt
ptpt
pt
Spoke
ptpt
ptpt
pt
MD
MD
MD
MD
MD
PhD
DO
NP
Spoke
ptpt
ptpt
pt
Spoke
ptpt
ptpt
pt

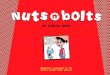
Peer-to-Peer Telemedicine
CLINICpt
pt
pt pt
pt
pt
pt
MD
MD
CSW
NP
DO
PhD
NP
ptpt
ptpt
pt
pt
pt
ptpt
pt
pt
pt
pt
pt
pt
pt
pt
pt
pt
pt
pt
pt
pt
pt
MD

Peer-to-Peer Telemedicine
– Peer-to-Peer Model
• Clinicians anywhere
• Patients anywhere
• Patient site bills, receives payment
• Clinician gets paid by patient site (as an employee or contractor)
• Clinicians anywhere
• Patients anywhere
• Patient site bills, receives payment
• Clinician gets paid by patient site (as an employee/contractor)
• “Telecommuting” (IN)

Wholesale vs. Retail
• Buying specialist time is easier using a Retail provider, but Wholesale is likely to be cheaper
49

Appropriate Technology
• Connectivity
– Site of Service
• Hardware & Software
• Skills & Service Design
50

Connectivity
The Foundation of Telehealth• T-1 (minimum necessary, 1.5 Mbps)
• Business cable internet (3-10 Mbps upload)
• Top-shelf options (fiber, business ethernet)
• Latency and Quality of Service are as important as bandwidth
• Keep the line free of competing demands
51

Site of Service
Hard line: Office vs Home• Privacy & Security
• Connectivity
– Rely on what’s available, or…
– Take connection to the site (4G hotspot)
52

Hardware & Software
53

Equipment
• H.323 Standard Video End Point ($5k-$50k)• LifeSize, Polycom, Cisco/Tandberg
• 32” HDTV (monitor + speakers)
• Desktop stand or rolling cart
• Web-based System ($1k+)• Software (Zoom, Vidyo, etc.)
• Mini computer + HD webcam
• 26-32” HDTV monitor + speakers
• Desktop stand or rolling cart

Equipment
• Web-based System ($500)• All-in-one desktop computer
• HD webcam
• Software package

Equipment
• Key considerations for DIY telemedicine• Good USB webcams beat built-in (laptop) webcams
• USB speakerphones beat built-in mics and speakers
• Wired beats wireless internet
• Monitors need only 720p (“low HD”)
• Keyboard/mouse inputs needed

Peripherals
Exam Camera – Dermatology, wound evaluation
• Tremendous detail, resolution, lighting options
• Unnecessary for many applications
Stethoscope –
• Several very good models available
• Bluetooth (wireless) connections, excellent audio
Otoscope –
• Multiple models available
• Modular, easy to use
57

Stethoscope
58

Otoscope
59

60

Skillsets
• Technology + Skillsets = Capabilities
• Capabilities + Practice = Execution
Training without practice is (mostly) wasted
61

Skillsets
• Rollout schedule that includes practice
• Low-pressure exposure (meetings, training)
• Mock codes/encounters with debriefing
• Process helpers/kits (laminated cards, etc.)
The biggest hurdle in implementation is
fear of the unknown
62

Technology Considerations
● High speed internet at both sites– 1-3 Mbps or more (nominal) for HD
– Test at www.internetfrog.com/mypc/speedtest/
● Endpoints – Two Major Classes– H.323 – Standalone system
● Hardware based, often older and/or larger
● Tandberg, Polycom, LifeSize, Sony, etc.
– SIP/Web-based – Client/server system● Software based (using a host computer)
● Skype, Oovoo, Vsee, ClearSea, Zoom, etc.
● Mobile apps
63

InternetH.323 H.323
Encrypted session
InternetSIP/WEB SIP/WEB
computer
webcam
Server
Encrypted sessions
???
webcam
computer

HIPAA Considerations
• Communications involving PHI (including live video) must be encrypted
• Any entity that stores PHI must sign a Business Associate Agreement (BAA)
• As long as live video is encrypted and not stored, BAA is not technically required
Some type of signed agreement to enforce this is likely to be helpful and is recommended
65

Peripherals
Exam Camera – Dermatology, wound evaluation
• Tremendous detail, resolution, lighting options
• Unnecessary for many applications
Stethoscope –
• Several very good models available
• Bluetooth (wireless) connections, excellent audio
ENT Scope –
• Multiple models available
• Modular, easy to use
66

Staff Training & Integration
Manipulation of peripherals
• Document training in equipment use
Professional Skills (within scope of licensure)
• Telemedicine (in general)
• Palpation, other specific techniques “under direct supervision” (up to licensed providers pending rule)
Key Strategies
1. Trust – Develop strong working relationships
2. Documentation– Policies & Procedures for TM (“same standard of care”)
– Case/Progress Notes (start & stop times, locations, consent)
67

Technology Resource - TTAC
Telehealth Technology Assessment Center
– HRSA-funded technology-focused TRC
http://www.telehealthtechnology.org/toolkits
● Objective introductions to technologies
**Information ages quickly, newest and most expensive equipment isn’t covered
68

Special Considerations
• Almost any client will adapt quickly to technology, given sensitive guidance (providers take longer)
• Clinical skills are the same – rapport is key
• Recognize and foster client understanding
• Refer to technology experiences outside TM
• Involve family/caregivers throughout
69

Conclusions
• Telemedicine is a complex and rapidly changing field
• Telemedicine offers a range of potential benefits to a variety of stakeholders
• Careful examination of business models, clinical strategies, and technologies is necessary to maximize benefit
70

Questions
• Introduction to UMTRC
• Introduction to Telehealth
• Business Models for Telehealth
• Telehealth Regulation and Reimbursement
• Telehealth Technology Considerations
• Conclusions
• Questions
71

Contact Information
Jonathan Neufeld, PhD
Upper Midwest Telehealth Resource Center
(574) 606-5038
72