Embed Size (px)
Citation preview

How you can overcome the barriers
to treating ARLD in primary and secondary care
Stephen Ryder NIHR Biomedical Research Unit in
Gastrointestinal and Liver Diseases at Nottingham University Hospitals NHS Trust and
The University of Nottingham

Dataset Updated
0
100
200
300
400
500
600
700
800
9000
1/0
1/2
00
8
01
/04
/20
08
01
/07
/20
08
01
/10
/20
08
01
/01
/20
09
01
/04
/20
09
01
/07
/20
09
01
/10
/20
09
01
/01
/20
10
01
/04
/20
10
01
/07
/20
10
01
/10
/20
10
01
/01
/20
11
01
/04
/20
11
01
/07
/20
11
01
/10
/20
11
01
/01
/20
12
01
/04
/20
12
01
/07
/20
12
01
/10
/20
12
01
/01
/20
13
01
/04
/20
13
01
/07
/20
13
01
/10
/20
13
01
/01
/20
14
01
/04
/20
14
01
/07
/20
14
01
/10
/20
14
01
/01
/20
15
01
/04
/20
15
01
/07
/20
15
01
/10
/20
15
01
/01
/20
16
01
/04
/20
16
01
/07
/20
16
01
/10
/20
16
Co
un
t o
f P
atie
nts
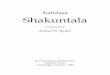
Alcohol or Cirrhosis Diagnoses
Patients per Month
Had Cirrhoses
Had Procedure

Who dies from alcoholic liver disease and where are potential therapeutic
interventions missed? An analysis of 755 deaths in a Health Community 2007-
2010
S Ryder, T Coles, K Bash, T Allen.
Nottingham University Hospitals NHS Trust and Public Health Intelligence and Information NHS
Nottinghamshire County

Aims
1. Who dies from Alcohol Liver Disease?
2. What are possible points for healthcare intervention efforts prior to death?
3. Communities where these people lived – which ones carry disproportionate burden of ALD deaths?

Methods
• Identified deaths in 2 PCT areas via death certification, HES and hospital coding
• Looked at attendances in the years prior to death
• Information from area of residence and demography
• Data available from 2006 but complete from 2007

Results
• 755 deaths identified
• Primary or underlying cause of death recorded as alcoholic liver disease

Deaths from ALD in Nottinghamshire

DSRs by Area of Residence
0
10
20
30
40
50
60
Newark andSherwood
Rushcliffe Bassetlaw Gedling Broxtowe Ashfield Mansfield Nottingham
Deaths from Alcohol Liver Disease 2007 - 2009 Annualized DSRs per 100,000 resident population

0
5
10
15
20
25
30
35
40
45
Rushcliffe Broxtowe Gedling N&S Ashfield Bassetlaw Mansfield Nottingham
Ave IMD2007 Scores by Region People died from ALD versus Ave LA ID 2007 Score (Higher score
reflects higher level of deprivation) Sources: Data warehouse IMD 2007 scores and
Communities.gov.uk - LA Summaries ID 2007
Ave for ALD deaths Ave IMD score for district resident population

Impact on secondary care services
• 755 patients died from ALD
• 95% of these patients were admitted to
hospital prior to dying
–6,954 total admissions
–Average of 7.06 per patient in 5 years
prior to death
• 80% patients had A&E visits prior to dying
–1,215 total A& E visits

0
100
200
300
400
500
600
<1 1 to 6 6 to 12
Num
ber
of
adm
issio
ns
No of admissions
No ALD

Digestive
Abnormal
signs/tests
Circulatory
Neoplasms
Injury/poisoning
Mental/behavioural
Disorder of blood
Other
32%
Diagnoses in previous admission

Place of death
• 72% hospital
• 24% home
• 0.13% hospice

Conclusions
• Mortality from ALD is high and liked to deprivation
• High risk groups can be identified in populations
• People who die from ALD have multiple contacts with secondary care
• Only a minority have ALD recognised/coded

Why are mortality rates continuing to rise?
• Identification of at risk population
• Interventions
• Tools to diagnose early
• Perceptions of healthcare workers and reality of effectiveness of interventions
• Stigmatisation
• NHS and Social care structures

Identification of those at risk
• Primary care
• Secondary care
Q. Why is identification of high risk drinkers a key priority? A. Because we have a highly effective intervention


What can we do: early diagnosis
• No reliable test for alcohol excess
• If we don’t ask we don’t find
• Primary care awareness of liver disease low
• Standard LFTs unhelpful

How good is alcohol screening in primary care?
• No systematic data
• Ballets study

BALLETS study
• 8 practices in Birmingham
• 2006-2008
• Abnormal test in liver panel
• No symptoms of liver disease
• No history of liver disease/alcohol/ivdu
Armstrong MJ et al. J Hepatol 2012;56:234

Cause of Abnormal LFTs
• 54.9% had a cause identified
0
5
10
15
20
25
30
35
40
45
50
NAFLD ALD Screen + unexplained

Potential solutions
• RCGP have identified liver disease as priority area for primary care education (Dr Jez Thompson) linked with Lancet commission
• Local solutions needed (STP/CCG)
• There are good models
– Nottingham City AUDIT C in all new registrations
– Local targets for alcohol/tobacco histories

16/02/2017
The Scarred Liver Project: a novel diagnostic pathway to detect significant liver disease in
the community
Harman DJ et al. BMJ Open2015;5:e007516 doi:10.1136/bmjopen-2014-007516 Direct targeting of risk factors significantly increases the detection of liver cirrhosis in primary care: a cross-sectional diagnostic study utilising transient elastography

Practice based screening for risk
• Four representative GP practices; >20,000 adult patients – Initial pilot phase in 2 suburban GP centres – Validation phase in 2 Inner City GP centres
• GP systems searched for codes for Type 2 DM and alcohol excess • 12 % have risk factors for significant liver disease
• All invited for fibroscan

Novel community pathway
• Diagnostics performed in the community • Point of care diagnostics in primary care
• Diagnostics/brief intervention delivered by nurses
• Specialists placed in the community • Integrated primary and secondary care
• Hepatology clinics in primary care
McCorry et al., QIM 2012; Dolman et al., Liv Int 2013

General Practice Population Risk Factors
Group Population Type 2 Diabetes
Alcohol
Practice A 7,612 304 522
Practice B 2,867 86 136
Practice C 6,412 391 482
Practice D 3,977 226 298
TOTAL 20,868 1,007 1,438

Changing our Approach to Liver Disease
Current approach:
•Lacks accuracy
•Late detection
•Hospital based
•Costly and invasive
Alternative approach:
•Focus on risk factors
•Early detection
•Community testing
•Cost saving
NHS innovations award winners 2013 BMJ team of the year finalists 2015

ALT Liver Enzyme Performance
• 68.3% of patients with elevated liver stiffness had normal liver function enzymes
• 73.1% of patients with proven cirrhosis had normal liver function enzymes


Secondary care: ED screening
• Key part of “every contact counts”
• Evidence base strong for identification and brief advice
• Many models of how to implement



ED screening
• Many challenges to doing it
• Perception in staff that “extra task with no reward”
• Perceived as complex and “no time for brief advice”
• Client group are “unattractive as recipients of care”
• No national data on brief advice in ED

Nottingham ED and screening
0
10
20
30
40
50
60
70
80
90
100
20062007200820092010201120122013201420152016
% SCREENED
CQUIN

Nottingham ED screening
• Two questions mandated:
– Have you drunk 6u or more on any occasion in the last month?
– Was this attendance related to alcohol?
• Answers go back to GP
• Primary care to provide brief advice/intervention
• Audit set up to see if it happens

Hospital beyond ED
• 50% of liver disease still presents with decompensation
• Admissions increasing
• Must have appropriate services for patients who get beyond ED

Alcohol liaison

Models for alcohol teams
Good community services
95%
Hospital Liaison

Nottingham model
• 5 WTE in reach (Framework)
• 1 WTE employed by the Trust
• All patients identified in Trust seen by ALN assessed and referred into community treatment as required
• Trust employee works on hepatology ward and runs clinics with consultants
• 1 High volume service user (band 7) in ED

High Volume service user
• Identified “top 50” high volume users of ED
• Average number of ED attendances 36 per year
• Average cost >£30,000
• Alcohol is the cause or a significant cofactor in 67%

High Volume Service Users
• ED nurse coordinates care
• MDT with community services-housing, finances, medical
• Alert on hospital system flags any attendance
• Care plan available on hospital and community systems
• Data sharing agreements (consent)

HVSU: impact
0
100
200
300
400
500
600
Q1 12 Q2 12 Q3 12 Q4 12 Q1 13 Q2 13 Q3 13 Q4 13 Q1 14 Q2 14 Q3 14 Q4 14
Series2
Series1

Community care
• Range of services required
• Includes detoxification in-patient beds (Mental Health Trust)
• About to have nursing facility for alcohol related brain injury patients

Challenges in provision
• Commissioning fragmentation
• Retendering of services
• Public Health support vital to achieve anything
• Support from local government essential

Improving Liver Health in the East Midlands – A Call to Action
This report has been prepared by: Ben Anderson, Ann Goodwin, Sean Meehan and Natalie Cantillon – Public Health England East Midlands
In collaboration with: Dr Stephen Ryder – Consultant Hepatologist, Nottingham University Hospitals and Chair of East Midlands Clinical Liver Network
Jonathan Gribbin – Consultant in Public Health, Nottinghamshire County Council East Midlands Directors of Public Health including Elaine Michel, Lead for Alcohol and DPH Derbyshire County Council and Mike Sandys, Lead for Obesity and DPH Leicestershire County Council.

RAID model
• Birmingham Mental Health Initiative
• Included alcohol services
• Attractive concept for some clients:
– Severe physical disease
– Told to go home and drink and access community services
– Access to detox beds 3 months
– Not very helpful if you have cirrhosis

Cirrhosis and end of life care
0
20
40
60
80
100
120
0 5 10 15 20 25 30
Drinking
Not

Blue Light Project: treatment resistant drinkers





Gaps in our knowledge • Final order of priority of Alcohol-related Liver Disease questions,
agreed at James Lind Alliance Priority Setting Partnership workshop 16 September 2016
• What are the most effective ways to help people with alcohol-
related liver disease stop drinking? • What are the most effective ways of delivering healthcare
education and information about excessive alcohol consumption, the warning signs and the risks of alcohol-related liver disease to different demographics (including young people)?
• What is the most effective model of community-based care for patients with alcohol-related liver disease?
• What is the patient's experience of alcohol-related liver disease?

• Do attitudes to perceived 'self-induced illness' amongst healthcare professionals affect treatment, care provision and compassion for individuals with alcohol-related liver disease?
• What are the most effective strategies to reduce the risk of alcohol-related liver disease in heavy drinkers?
• Does the stigma associated with alcohol misuse affect the willingness of people with alcohol-related liver disease to ask for help?
• What interventions improve survival in individuals with complications of advanced alcohol-related cirrhosis?
• How should depression be managed in the context of alcohol-related liver disease?
• What models of involvement of palliative care services in advanced alcohol-related liver disease are most beneficial?