Embed Size (px)
Citation preview

Improving Critical Care Intubation at a Community Hospital:
A Prospective Quality Improvement Project
Dr. Samuel Kohen
Comox, BC
BC Quality Forum March 2, 2017 – 14:30 to 15:30
Breakout Session – C4

St Joseph’s General Hospital

Disclosure: Emergent Intubation Experience
• Overall risk of complications is high (39%)
– 19% Severe hypoxemia (SaO2 < 80%)
– 10% Severe hypotension (sBP < 70 mmHg)
– 7% Esophageal intubation
– 6% Frank aspiration
• Associated with high mortality
– ICU 15%, Hosp 29%

Critical Care Intubation 2014 Audit
• Documentation
– Data spread between MD, RN, RT notes
– 25% did not have a MD note at all
• Procedural Efficiency
– Time from meds to CXR = 43 min
• Procedural Safety
– Life threatening complication rate = 35%


Procedural Documentation
Documentation Requirement Points
Was there a signed physician intubation note? 1
Was the indication for intubation documented? 1
Were the drugs used in the intubation listed? 1
Were the airway tools used listed? 1
Was the airway difficulty documented? 1
Was ETT placement clinically confirmed with ETCO2? 1
Were complications listed? 1
Total /7
Objective 1: Improve CCI documentation

Procedural Efficiency
Objective 2: Reduce procedural time

Life Threatening Complications
Complication Definition
Severe Hypoxemia New SpO2 < 80%
Severe Hypotension New sBP < 70 mmHg
Esophageal Intubation ETT mistakenly placed in the esophagus
Frank aspiration New vomitus in airway that requires suctioning
Cardiac Arrest Procedural cardiac arrest
Objective 3: Reduce life threatening complications

Documentation Time Objective 4: No increase in documentation time.

Study Methodology
2014 2015
Exclusion criteria:
Inclusion criteria:
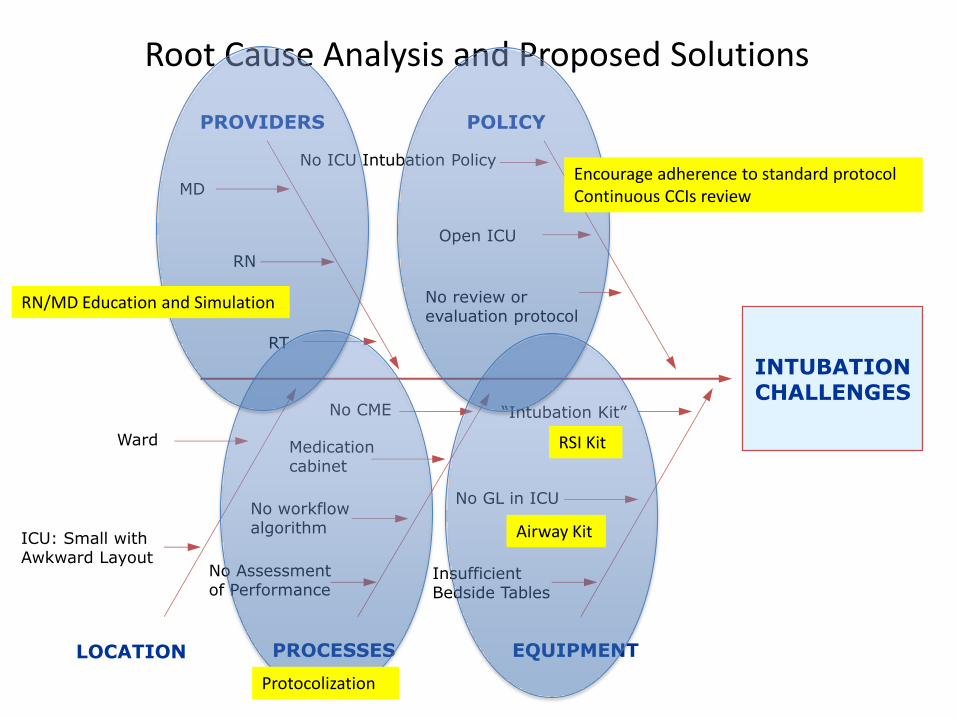
INTUBATION CHALLENGES
EQUIPMENT
PROVIDERS POLICY
No Assessment of Performance
No CME
RT
RN
MD
Ward
ICU: Small with Awkward Layout
PROCESSES LOCATION
No review or evaluation protocol
“Intubation Kit”
No GL in ICU No workflow algorithm
Medication cabinet
Insufficient Bedside Tables
Root Cause Analysis and Proposed Solutions
No ICU Intubation Policy
Open ICU
Protocolization
RSI Kit
RN/MD Education and Simulation
Airway Kit
Encourage adherence to standard protocol Continuous CCIs review
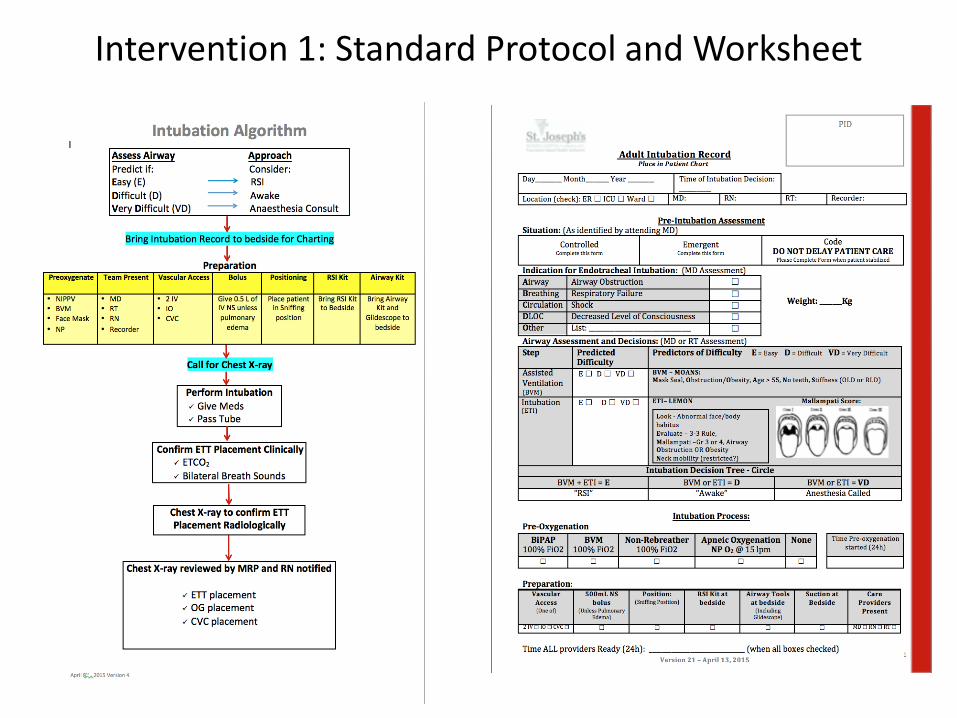
Intervention 1: Standard Protocol and Worksheet

Intervention 2: Airway and Medication Boxes
Standard Adult RSI Kit
Standard RSI Kit Standard Adult Airway Kit

Intervention 3: Multidisciplinary Simulation Course

Results: Patient Demographics

CL 5.3
6.5
2
3
4
5
6
7
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
Do
cum
en
tati
on
sco
re (
/7)
CCI #
17% improvement in documentation (Significant)
CL 5.3
6.5
2
3
4
5
6
7
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
Do
cum
en
tati
on
sco
re (
/7)
CCI #
Critical Care Intubation Documentation (C-chart)
Results: Documentation

1
3
UCL 116.5
54.9
CL 43.1
26.8
0.0
20.0
40.0
60.0
80.0
100.0
120.0
140.0
1 2 3 4 5 6 7 8 10 11 12 13 17 18 20 3 4 5 6 8 9 10 13 14 15 18 19 20 21 22 23 24 26
Tim
e f
rom
Me
dic
atio
n A
dm
inis
tati
on
to
CX
R (
min
)
CCI #
38% improvement in process efficiency (Significant)
Results: Procedural Efficiency

57% relative reduction in life threatening CCI complications (Not significant)
35%
15%
0%
5%
10%
15%
20%
25%
30%
35%
40%
2014 2015
Results: Complications

Documentation Time

Successes and Challenges

Future Directions:































