Embed Size (px)
Citation preview

GDM: EXERCISE & TECHIRIS THIELE ISIP TAN MD, MSC Director, UP Manila Interactive Learning Center Chief, UP Medical Informatics Unit Professor, UP College of Medicine @endocrine_witch

NOTHING TO DISCLOSE

EXERCISE
TELECARESMS
POSTPARTUM

EXERCISE
TELECARESMS
POSTPARTUM

Several international guidelines recommend exercise in GDM management
No supporting evidence from a systematic review
Harr ison et al Journal of Physiotherapy 2016; 62:188-196

Exercise improves glycemic control in women diagnosed with gestational diabetes mell i tus: a systematic review. Harr ison et al Journal of Physiotherapy 2016; 62:188-196.
EXERCISE AND GLYCEMIC CONTROL GDM
P Pregnant women with GDM
I Exercise performed more than once a week, sufficient to achieve an aerobic effect or changes in muscle metabolism
O Postprandial blood glucose, FBS, HbA1c, requirement for insulin, adverse events, adherence
M Systematic review (8 RCTs qualitative n=588, 7 RCTS quantitative n=544)

Harr ison et al Journal of Physiotherapy 2016; 62:188-196
Can adjunctive exercise improve acute postprandial blood glucose in women with GDM vs standard care? Does adjunctive exercise improve FBS and HbA1c? What kind of exercise programs are effective in lowering postprandial blood glucose levels? What variables affect adherence?

Circuit type resistance training n=2
Upright cycle ergometer n=2 (one trial combined with walking)
Recumbent cycle ergometer n=1
Arm ergometer n=1
Brisk walking n=1
Yoga n=1
Image from hammer-fitnes.ch
Image from runningonhungry.com
EXERCISE
Harrison et al Journal of Physiotherapy 2016; 62:188-196
Harr ison et al Journal of Physiotherapy 2016; 62:188-196
Frequency 3-7 sessions per week
Intensity Variable Predicted HR max 50-70% Between “moderate” and “somewhat hard”
Duration 20-45 min Including short warm-up and cool down periods 6 weeks or until 38 wks AOG or to end of pregnancy
EXERCISE
Delivery Individual session Center-based with direct supervision Home-based with direct, indirect supervision (phone) or unsupervised Both center- and home-based
Harr ison et al Journal of Physiotherapy 2016; 62:188-196
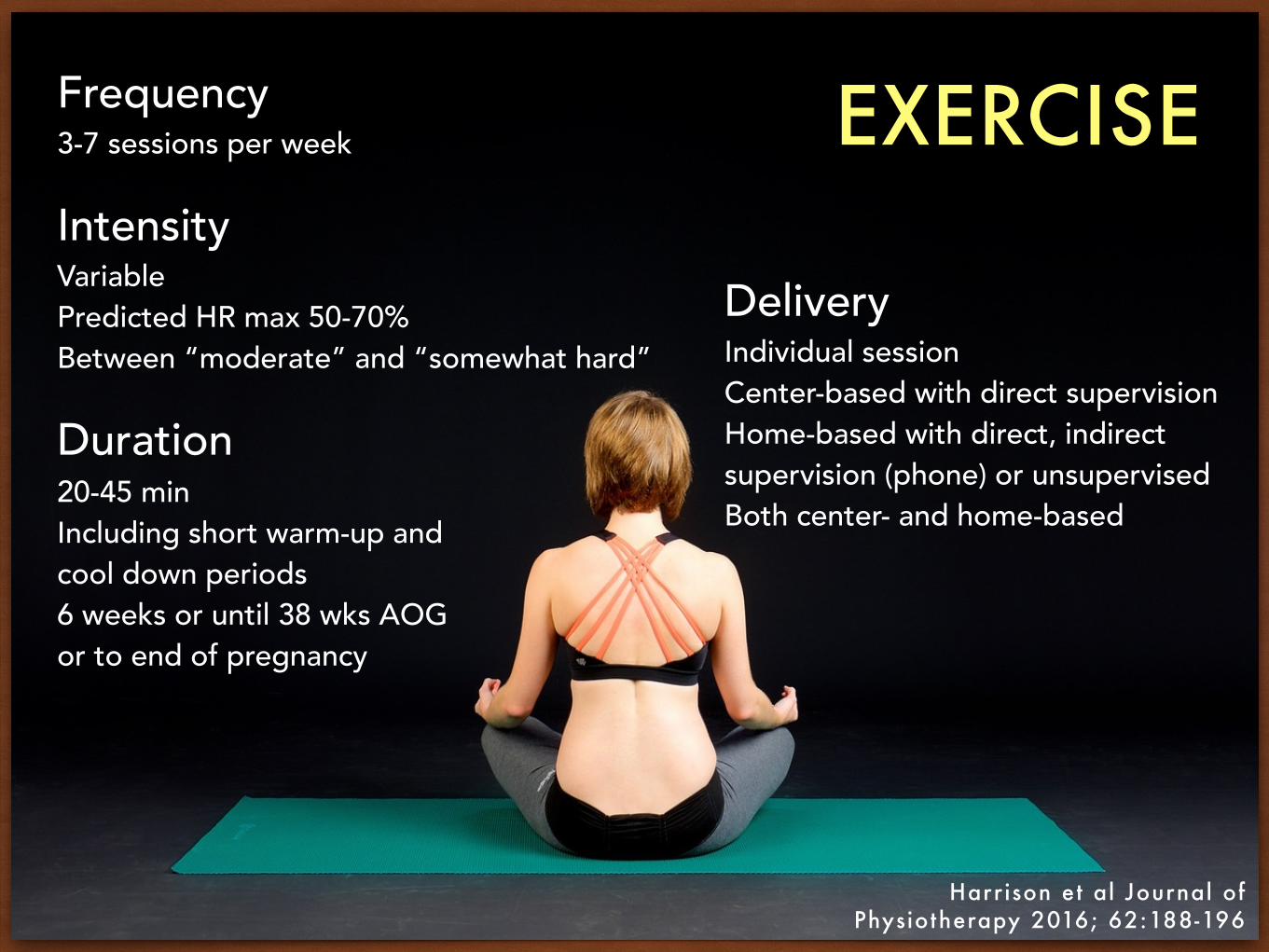
POSTPRANDIAL BLOOD GLUCOSE
Harr ison et al Journal of Physiotherapy 2016; 62:188-196
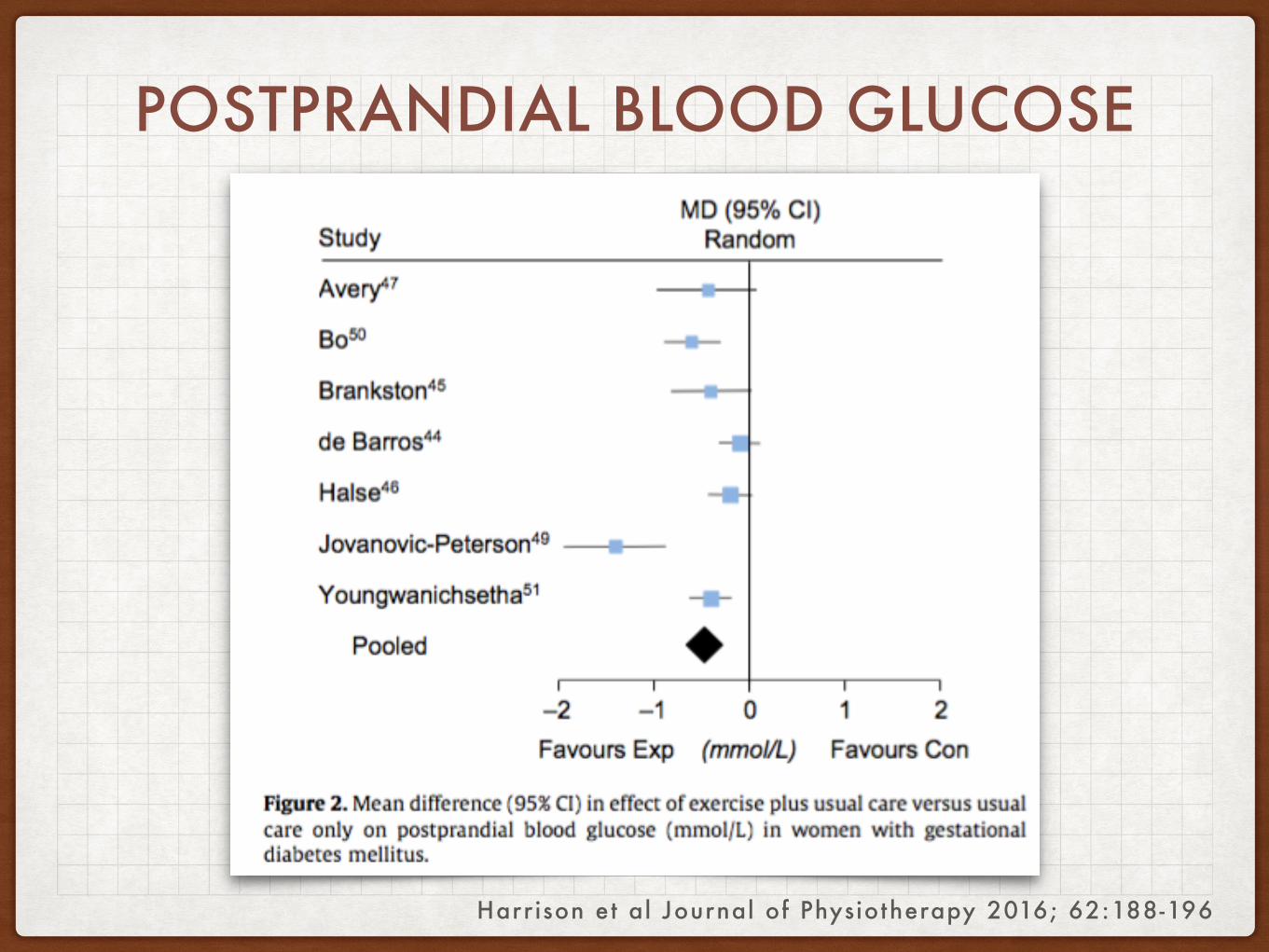
FASTING BLOOD GLUCOSE

HBA1C
Harrison et al Journal of Physiotherapy 2016; 62:188-196

INSULIN REQUIREMENT
Harrison et al Journal of Physiotherapy 2016; 62:188-196
Harr ison et al Journal of Physiotherapy 2016; 62:188-196
Can adjunctive exercise improve acute postprandial blood glucose in women with GDM vs standard care? YES Does adjunctive exercise improve FBS and HbA1c? YES

Harr ison et al Journal of Physiotherapy 2016; 62:188-196
What kind of exercise programs are effective in lowering postprandial blood glucose levels? Moderate intensity, minimum of 3x a week
What variables affect adherence? Not reported by the trials

Harr ison et al Journal of Physiotherapy 2016; 62:188-196
Adding exercise to usual care of GDM reduces postprandial BG, FBG and HbA1c.
Exercise is safe.

EXERCISE
TELECARESMS
POSTPARTUM
Diabetes Res Clin Pract (2015), http://dx.doi.org/10.1016/j.diabres.2015.07.007
Included 3 RCTs only Convenience of reducing face-to-face and unscheduled consultations More trials that include cost evaluation are required

TELECARE APPROACH TO GDM
Perez-Ferre et al Int J Endocr inol 2010
P 100 pregnant women with GDM
I Telemedicine system for transmission of capillary glucose data and SMS with weekly professional feedback
C Traditional face-to-face outpatient clinic visits O Percentage of women with HbA1c <5.8%, normal vaginal delivery and LGA infants
M Randomized parallel group
Perez-Ferre et al Int J Endocr inol 2010
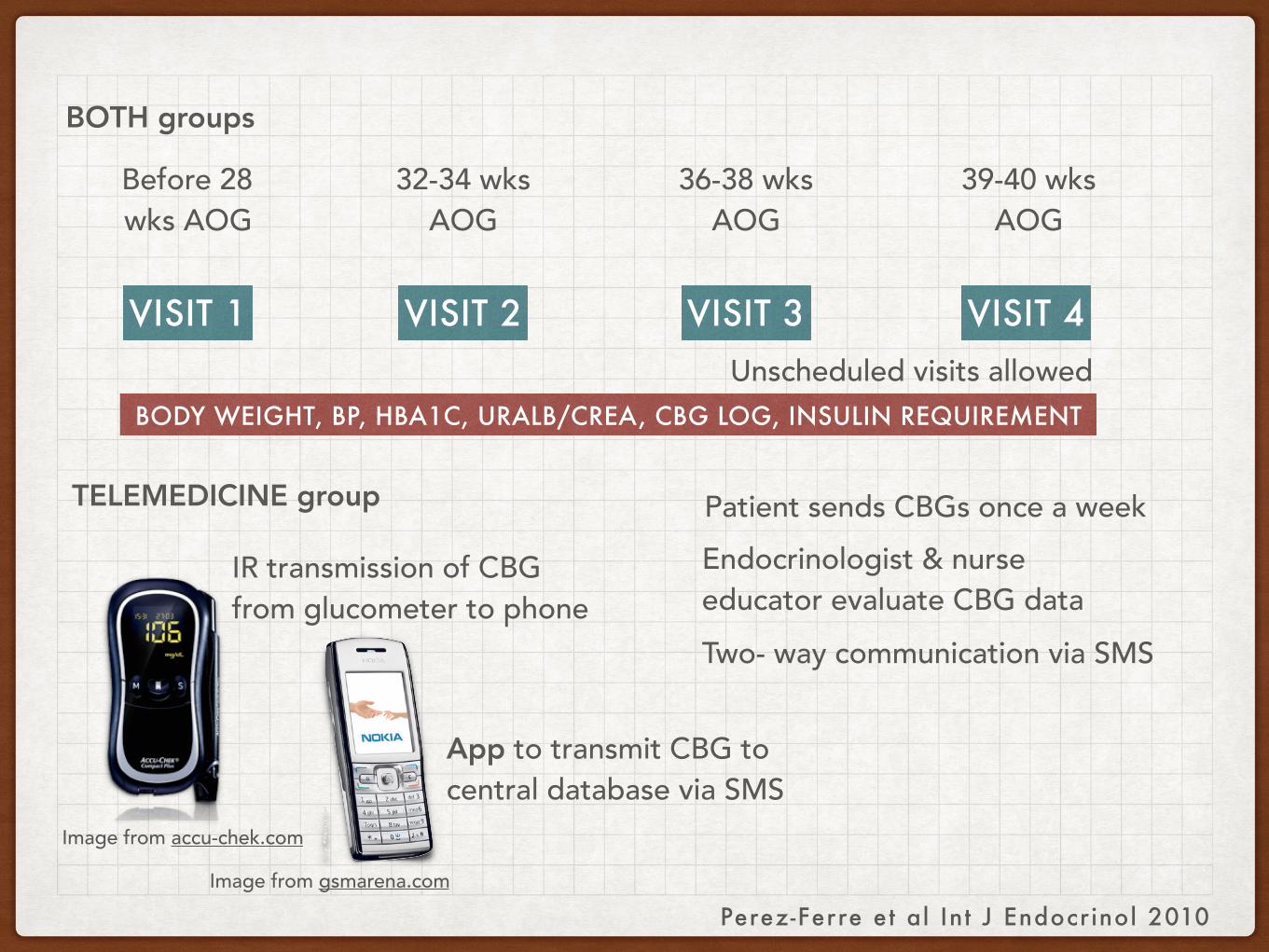
VISIT 1 VISIT 2 VISIT 3 VISIT 4
Before 28 wks AOG
32-34 wks AOG
36-38 wks AOG
39-40 wks AOG
BODY WEIGHT, BP, HBA1C, URALB/CREA, CBG LOG, INSULIN REQUIREMENT
TELEMEDICINE group
BOTH groups
Image from accu-chek.com
Image from gsmarena.com
App to transmit CBG to central database via SMS
IR transmission of CBG from glucometer to phone
Patient sends CBGs once a weekEndocrinologist & nurse educator evaluate CBG dataTwo- way communication via SMS
Unscheduled visits allowed
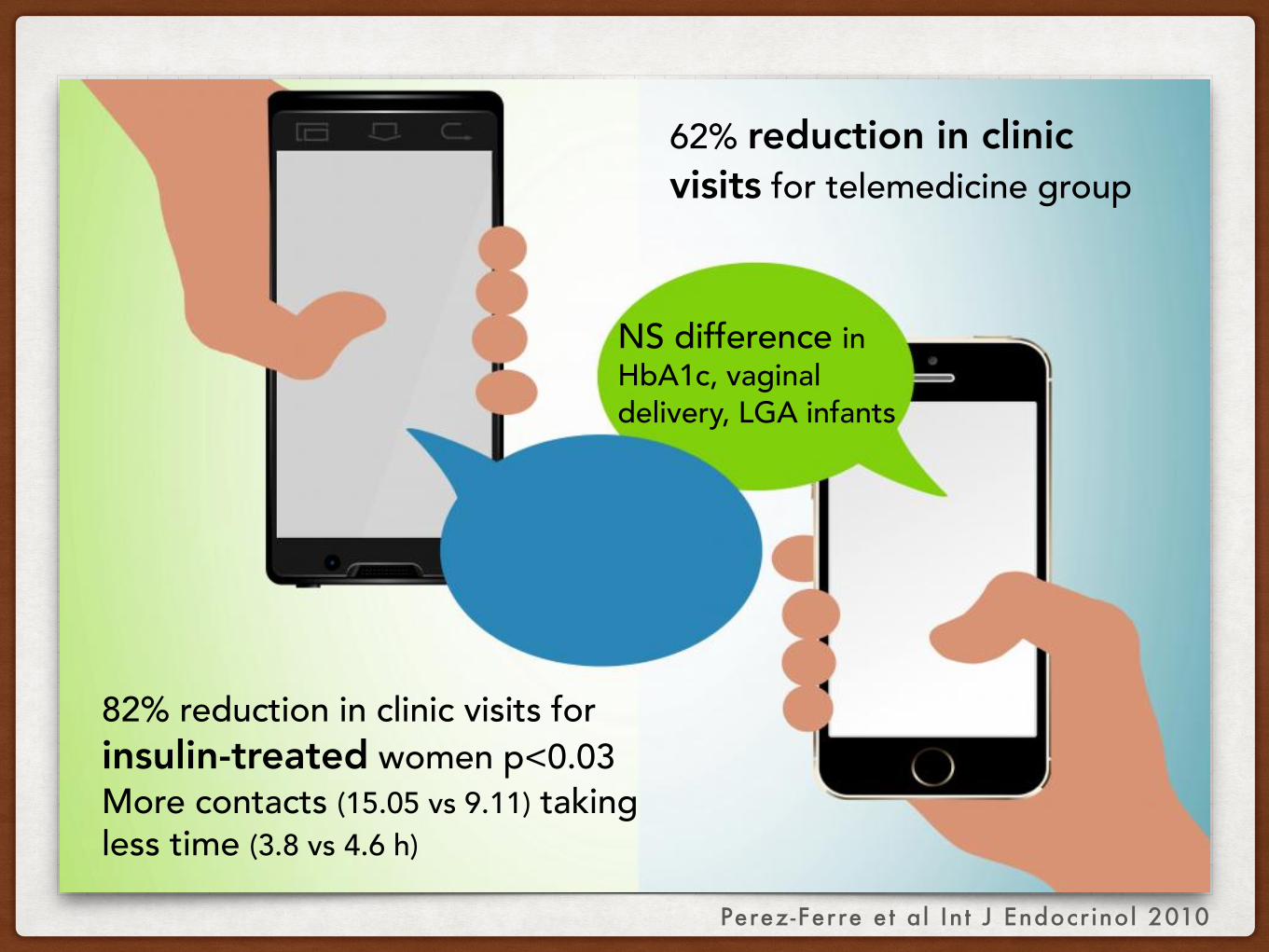
62% reduction in clinic visits for telemedicine group
82% reduction in clinic visits for insulin-treated women p<0.03 More contacts (15.05 vs 9.11) taking less time (3.8 vs 4.6 h)
Perez-Ferre et al Int J Endocr inol 2010
NS difference in HbA1c, vaginal delivery, LGA infants

Perez-Ferre et al Int J Endocr inol 2010
Reduction in number of clinic visits saves time for both patient & health professional
Telemedicine connection increases accessibility to health team, at convenience
Reduces transportation, clinic waiting times
Minimizes intereference with woman’s work schedule
Particularly useful for insulin-treated who require more contacts to adjust insulin dose

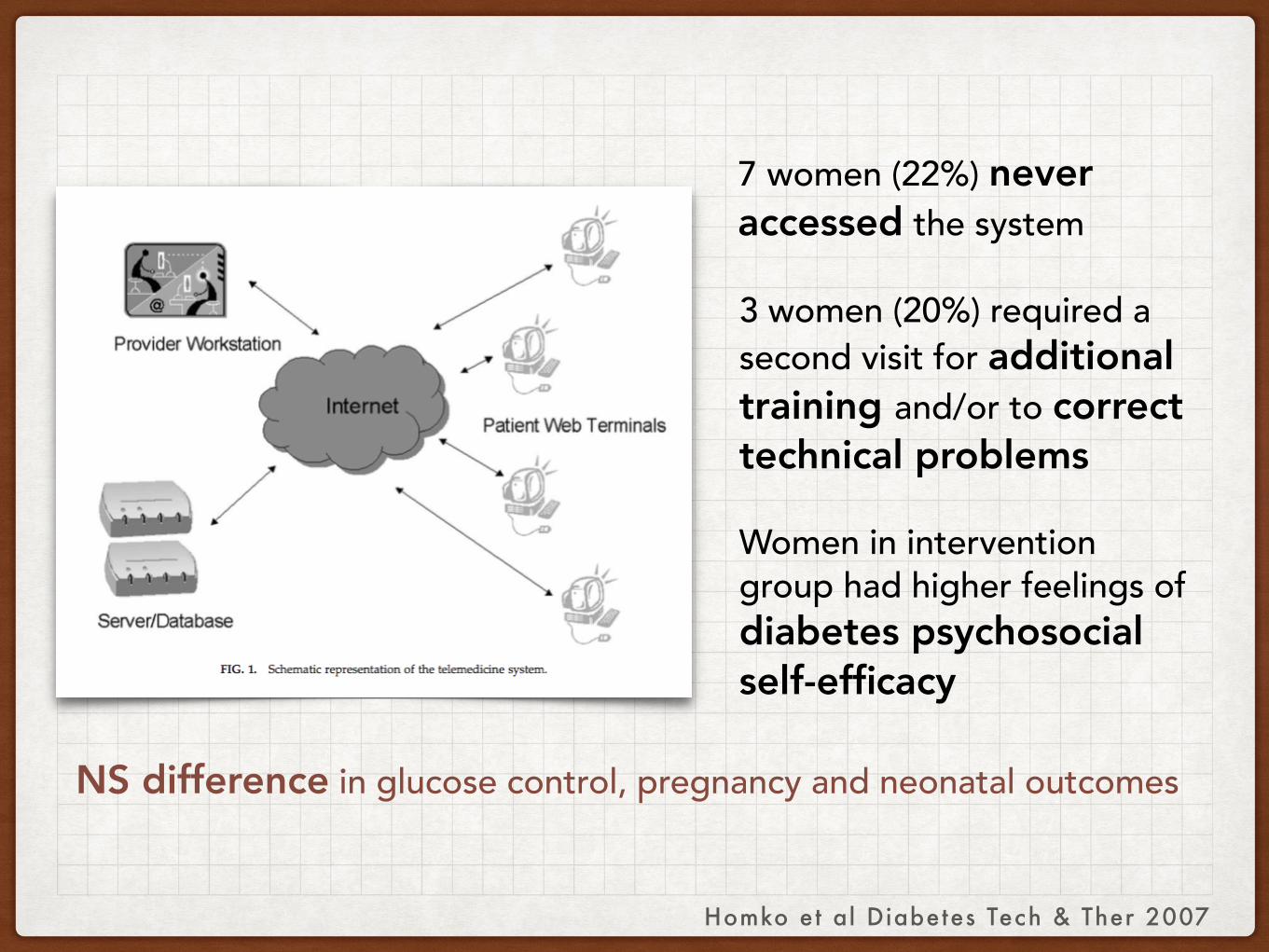
INTERNET-BASED TELEMEDICINE FOR UNDERSERVED WOMEN WITH GDM
Homko et al Diabetes Tech & Ther 2007
P Pregnant women with GDM
I Internet group (n=32); provided computers & internet access for communication via website
C Control group n =25; maintained paper logbooks reviewed at each visit
O Use of system, self-efficacy, maternal glucose control, pregnancy and neonatal outcomes
M Randomized trial

Homko et al Diabetes Tech & Ther 2007
Homko et al Diabetes Tech & Ther 2007
7 women (22%) never accessed the system
3 women (20%) required a second visit for additional training and/or to correct technical problems
Women in intervention group had higher feelings of diabetes psychosocial self-efficacy
NS difference in glucose control, pregnancy and neonatal outcomes

Women sent average of 3 wks data in 8-wk follow-up
Daily responsibility of poor young single mothers with small children limited applicability of
telemedicine approach
Logistics of providing, installing & maintaining hardware was labor-intensive
Homko et al Diabetes Tech & Ther 2007
TELEMEDICINE SYSTEM WITH AUTOMATED REMINDERS FOR WOMEN WITH GDM
Homko et al Diabetes Tech & Ther 2012
P Pregnant women with GDM
I Telemedicine group (n=40); Interactive Voice Response telephone system
C Control group n =40; maintained paper logbooks reviewed at each visit
O Maternal glucose control and infant birth weight
M Randomized trial

Homko et al Diabetes Tech & Ther 2012
IVR system can be accessed from any phone
Asynchronous phone messaging between clinicians and patients
Automated reminders for patients to transmit data

Homko et al Diabetes Tech & Ther 2012
Option of dialing dedicated toll-free number or use Internet with unique log-in and password
Can append message IVR: 45 s speaking Internet: unlimited text input
Data and messages queued for clinician to respond via portal

Homko et al Diabetes Tech & Ther 2012
Patient’s message from IVR plays back as wav file
Nurse can respond by typing IVR: text-to-voice function Internet: text

Homko et al Diabetes Tech & Ther 2012
Automated 3 phone call reminders for missed data transmission
If still no response, the nurse can reset reminders (another 3 calls) or call the patient directly to follow up.

Homko et al Diabetes Tech & Ther 2012
NS difference in maternal blood glucose
NS difference in LGA infants
Adding telephone access and reminders increased transmission rates of data in the intervention group.
Telemedicine system increased contact between women and their health team but had no impact on outcomes.

EXERCISE
TELECARESMS
POSTPARTUM

DIAMIND Randomized Tr ial
POSTPARTUM SMS REMINDERS FOR GDM
P Women with GDM in recent pregnancy, with mobile phone, normal blood glucose before discharge
I SMS group (n=140); SMS reminder for OGTT at 6 wks postpartum and 3 & 6 mos if required
C Control group (n =140); SMS at 6 mos postpartum
O OGTT at 6 mos postpartum
M Randomized parallel groupvan Ryswyk et al Diabetic Medicine 2015

SMS 1 SMS 2 SMS 3
6 wks postpartum
3 mos postpartum
6 mos postpartum
NATIONAL GESTATIONAL DIABETES REGISTER
Sends postal reminders 12-16 weeks after expected due date
SMS GROUP
CONTROL GROUP
if required if required
van Ryswyk et al Diabetic Medicine 2015
SMS sent automatically based on date of birth of baby using Clickatell bulk SMS gateway

DIAMIND Randomized Tr ial
POSTPARTUM SMS REMINDERS FOR GDM
OGTT attendance at 6 mos SMS group: 104 (77.6%) Control group: 103 (76.8%) RR 1.01, 95% CI 0.89-1.15
>83% received postal reminders from National Gestational Diabetes Register
van Ryswyk et al Diabetic Medicine 2015

EXERCISE
TELECARESMS
POSTPARTUM
@ENDOCRINE_WITCHIris Thiele Isip Tan MD, MSc
Director, UP Manila Interactive Learning Center Chief, UP Medical Informatics Unit
Professor, UP College of Medicine