Embed Size (px)
Citation preview
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CLINICAL RESEARCH
Cinaciguat, a soluble guanylate cyclase activator,unloads the heart but also causes hypotensionin acute decompensated heart failure†
Erland Erdmann1*, Marc J. Semigran2, Markku S. Nieminen3, Mihai Gheorghiade4,Rahul Agrawal5, Veselin Mitrovic6, and Alexandre Mebazaa7,8,9
1Herzzentrum der Universitat zu Koln, Cologne, Germany; 2Heart Failure and Transplant Program, Cardiology Division, Massachusetts General Hospital, Harvard Medical School,Boston, MA, USA; 3Division of Cardiology, Helsinki University Central Hospital, Helsinki, Finland; 4Feinberg School of Medicine, Northwestern University, Chicago, IL, USA;5Global Clinical Development, Bayer HealthCare AG, Elberfeld, Germany; 6Kerckhoff Clinic Nauheim, Bad Nauheim, Germany; 7AP-HP, Department of Anesthesiology and CriticalCare Medicine, Hopital Lariboisiere, Paris, France; 8Universite Paris Diderot, PRES Sorbonne-Paris-Cite, Paris, France; and 9U942 Inserm, Paris, France
Received 17 January 2012; revised 2 May 2012; accepted 7 June 2012
Aims Cinaciguat (BAY 58-2667) is a novel soluble guanylate cyclase activator. This study evaluated the haemodynamiceffect and safety of cinaciguat added to standard therapy in patients with acute decompensated heart failure (ADHF).
Methodsand results
In this placebo-controlled, phase IIb study (NCT00559650), 139 patients admitted with ADHF, pulmonary capillarywedge pressure (PCWP) ≥18 mmHg, left ventricular ejection fraction ,40%, and a pre-existing need for invasivehaemodynamic monitoring were randomized 2:1 to cinaciguat:placebo (continuous i.v. infusion). The dose wastitrated for 8 h and maintained for 16–40 h (starting dose: 100 mg/h). At 8 h, mean PCWP changed from25.7+ 5.0 mmHg by 27.7 mmHg with cinaciguat and from 25.0+5.3 mmHg by 23.7 mmHg with placebo(P , 0.0001). The mean right atrial pressure changed from 12.4+ 5.3 mmHg by –2.7 mmHg with cinaciguat andfrom 11.8+4.9 mmHg by –0.6 mmHg with placebo (P ¼ 0.0019). Cinaciguat also decreased the pulmonary and sys-temic vascular resistance and the mean arterial pressure, and increased the cardiac index (all P , 0.0001 vs. placebo).Systolic blood pressure changed by –21.6+ 17.0 mmHg with cinaciguat and –5.0+14.5 mmHg with placebo.Adverse events were experienced by 71 and 45% of patients receiving cinaciguat and placebo, respectively. Noadverse effects on the 30-day mortality were seen; however, the trial was stopped prematurely due to an increasedoccurrence of hypotension at cinaciguat doses ≥200 mg/h.
Conclusion Cinaciguat unloaded the heart in patients with ADHF. However, high doses were associated with hypotension.- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Cinaciguat † Soluble guanylyl cyclase † Heart failure † Clinical trial, phase 2 † Haemodynamics † Vasodilation
IntroductionAcute decompensated heart failure (ADHF) represents new orworsening symptoms of heart failure that necessitate hospitaliza-tion.1,2 As a leading cause of hospitalization in patients olderthan 65 years, ADHF is one of the most costly cardiovascular dis-orders.3,4 Acute decompensated heart failure is associated withsevere cardiac diseases, and comorbidities including diabetes andrenal disease.5
Activation of soluble guanylate cyclase (sGC) is attractingincreasing interest as a therapeutic strategy for cardiovasculardisease. Conventional therapy for ADHF includes diuretics, posi-tive inotropes, and organic nitrates. However, organic nitratesare associated with tachyphylaxis and cytotoxicity from peroxyni-trite production.6,7 There is a need for a therapeutic agentthat will safely improve the haemodynamics in patients withADHF, without adversely affecting the heart and kidneys. Cinaci-guat (BAY 58-2667), a novel, potent sGC activator in clinical
†Some parts of this study were presented as an Oral Contribution at ACC.10, the 59th Annual Scientific Session of the American College of Cardiology. J Am Coll Cardiol2010;55:A16.E147.
* Corresponding author. Tel: +49 221 478 32511, Fax: +49 221 478 32512, Email: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2012. For permissions please email: [email protected]
European Heart Journaldoi:10.1093/eurheartj/ehs196
European Heart Journal Advance Access published July 9, 2012 by guest on O
ctober 25, 2013http://eurheartj.oxfordjournals.org/
Dow
nloaded from
by guest on October 25, 2013
http://eurheartj.oxfordjournals.org/D
ownloaded from
by guest on O
ctober 25, 2013http://eurheartj.oxfordjournals.org/
Dow
nloaded from
by guest on October 25, 2013
http://eurheartj.oxfordjournals.org/D
ownloaded from
by guest on O
ctober 25, 2013http://eurheartj.oxfordjournals.org/
Dow
nloaded from
by guest on October 25, 2013
http://eurheartj.oxfordjournals.org/D
ownloaded from
by guest on O
ctober 25, 2013http://eurheartj.oxfordjournals.org/
Dow
nloaded from
by guest on October 25, 2013
http://eurheartj.oxfordjournals.org/D
ownloaded from
by guest on O
ctober 25, 2013http://eurheartj.oxfordjournals.org/
Dow
nloaded from
by guest on October 25, 2013
http://eurheartj.oxfordjournals.org/D
ownloaded from
by guest on O
ctober 25, 2013http://eurheartj.oxfordjournals.org/
Dow
nloaded from

development for the treatment of ADHF,8,9 acts specifically onoxidized/haem-free sGC independently of nitric oxide by bindingto the enzyme’s haem pocket and mimicking the nitric-oxide-bound haem group.10 In animal studies, cinaciguat exerted potentvasodilation while preserving the glomerular filtration rate(GFR),11 and had antihypertrophic and antifibrotic effects.12 Thefirst clinical study of cinaciguat in patients with ADHF demon-strated strong reductions in preload and afterload, with an increasein cardiac output and preservation of renal function.13 The lack of adeleterious effect on renal and cardiac function despite a loweringof blood pressure in the clinical study suggests that cinaciguat mayhave unique properties. However, as the clinical study was notplacebo controlled, it was unclear how much of the observed clin-ical improvement could be attributed to cinaciguat and how muchwas due to other interventions. The aim of the current placebo-controlled, double-blind, phase IIb study was to evaluate thehaemodynamic effects and safety of i.v. cinaciguat (added to stand-ard therapy) in patients with ADHF.
MethodsThe study enrolled patients at 32 centres in 13 countries over a15-month period from December 2007 to March 2009. The studywas carried out in accordance with the Declaration of Helsinki andadhered to the International Conference on Harmonisation GoodClinical Practice guidelines. The ethics committees of all the participat-ing centres approved the study protocol. All patients providedinformed consent.
PatientsPatients aged ≥18 years were eligible for inclusion if they had acutelydecompensated chronic congestive heart failure, requiring hospitaliza-tion, with a pre-existing need for right heart catheterization, and a pul-monary capillary wedge pressure (PCWP) ≥18 mmHg. Patients had tohave a clinical indication for right heart catheterization, but the deci-sion to use right heart catheterization in each individual patient wasat the discretion of the investigator. Patients had to have had a clinicaldiagnosis of chronic heart failure for ≥3 months before study entry,left ventricular ejection fraction ,40% in the 6 months before studyentry, and a history of heart failure hospitalization or requirementfor i.v. diuretic treatment in the 12 months before study entry. Patientsneeded to have worsening dyspnoea symptoms or clinical evidence ofvolume overload leading to hospitalization at the time of enrolment.
Patients were excluded if they had undergone cardiac surgery withinthe previous month or had any of the following: acute de novo heartfailure; heart failure associated with pulmonary or valvular disease asthe primary cause of heart failure; heart failure associated with con-genital heart disease; pulmonary embolism or myocardial infarctionwithin the previous 30 days; hypertrophic cardiomyopathy; unstableangina; acute inflammatory heart disease; cardiogenic shock; heartrate (HR) ≥120 b.p.m., systemic arterial systolic blood pressure(SBP) ,100 mmHg or .180 mmHg; significant liver disease (e.g.acute clinical hepatitis, chronic active hepatitis, cirrhosis; aspartate ami-notransferase levels more than three times the upper limit of thenormal range), or severe chronic kidney disease or renal failure (esti-mated GFR ,30 mL/min/1.73 m2). A full list of inclusion and exclusioncriteria is available as Supplementary material online.
Study planThis was a multinational, placebo-controlled, double-blind, phase IIbstudy. All patients underwent screening, including physical examinationand laboratory tests. Demographic data, medical history, concomitantmedication use, and adverse events were also recorded. The maximumpermitted length of time between admission to the emergency wardand start of treatment was 48 h. Patients were randomized in a 2:1ratio to receive cinaciguat or placebo. Patients had undergone rightheart catheterization ≥2 h before receiving study drug, and the firststudy measurements were taken ≥1 h after catheter insertion. Afollow-up visit was scheduled for 30235 days after study inclusion.
Patients were valid for safety analysis if they had received at leastone dose of study medication. If they also had at least one valid efficacymeasurement at baseline and post-baseline, they were included in amodified intent-to-treat analysis. Patients were included in a per proto-col titration (PPT) analysis if they were valid for the modifiedintent-to-treat analysis, had a valid PCWP measurement at baselineand at 8 h (or, if withdrawn because of the lack of efficacy, a validPCWP measurement at any time post-baseline up to 8 h), andshowed no major protocol deviations.
Blood pressure, HR, and invasive supine haemodynamic parameterswere measured at baseline and during the study drug infusion (up to48 h or the end of the infusion). Blood pressure and HR were alsomeasured up to 8 h after stopping the study drug infusion. ForPCWP, two separate baseline readings were taken to ensure thatthe haemodynamics were reproducible. Quality checks based onprinted read-outs of haemodynamic recordings were performed byblinded central control. Blood samples were taken at baseline, 24and 48 h or the end of the infusion. Patients also rated their dyspnoeaon a visual analogue scale (VAS) at baseline, 8 and 48 h, and they ratedchanges in dyspnoea on a 7-point Likert scale at 8 and 48 h.
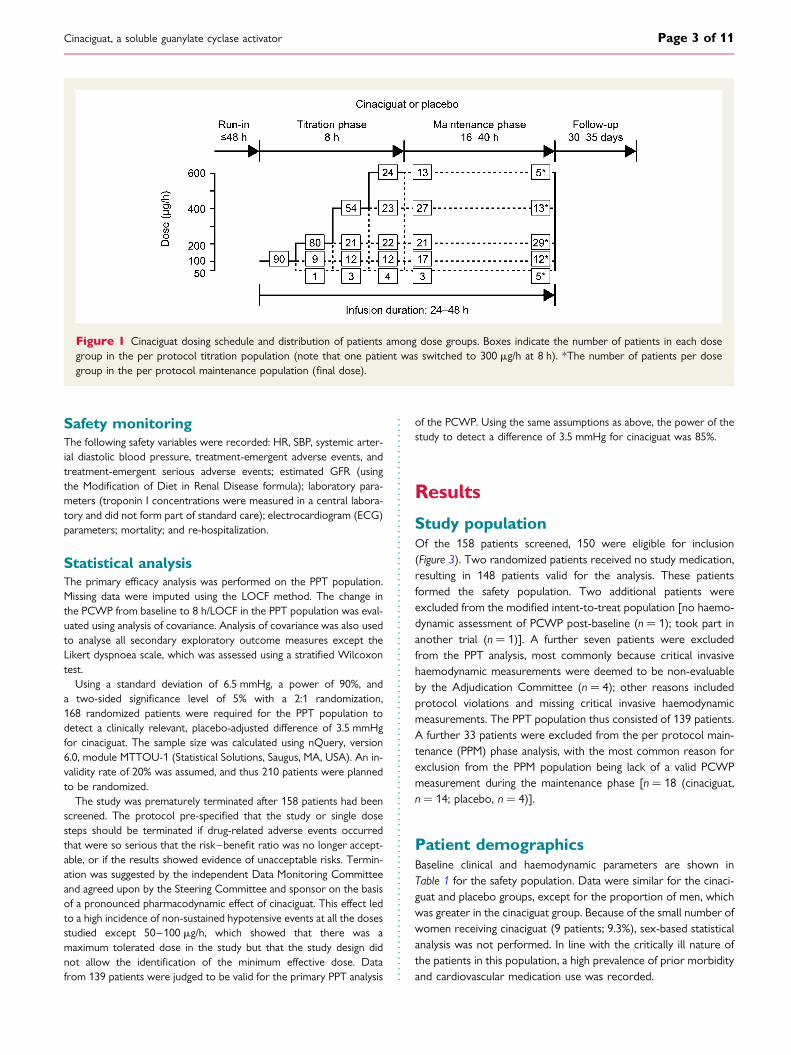
TreatmentPlacebo or cinaciguat at a concentration of 50 mg/mL was administeredas a continuous i.v. infusion for a titration phase of 8 h and a mainten-ance phase of 16–40 h (Figure 1). The starting dose (i.e. initial infusionrate) of cinaciguat was 100 mg/h, and was up- or down-titrated at 2, 4,and 6 h according to tolerability, SBP, and HR (Figure 2).
Concomitant medicationDobutamine at low doses (≤4 mg/kg/min), intravenously administereddiuretics, angiotensin-converting enzyme inhibitors, and beta-blockerswere allowed during the infusion period. Intravenous diuretics were tobe started at an individualized dose depending on clinical conditionsand titrated according to the clinical response.14 Levosimendan, vaso-dilators, vasoconstrictive agents, nitrates, and positive inotropic agents(except dobutamine at doses ≤4 mg/kg/min) were not allowed duringthe study and were to be stopped ≥3 h before the start of the studydrug infusion. Phosphodiesterase type 5 inhibitors were not allowedduring the study or in the 48 h before the start of the infusion.Strong cytochrome P450 2C8 inhibitors were also not allowedduring the study and were to be stopped ≥24 h before the start ofthe infusion.
Outcome measuresThe primary efficacy endpoint was a change in the PCWP from base-line to 8 h or the last post-baseline observation carried forward(LOCF) in the PPT cinaciguat population vs. placebo. Secondary ex-ploratory endpoints included changes from baseline in haemodynamicparameters measured by right heart catheterization and dyspnoea vs.placebo. B-type natriuretic peptide (BNP) levels were also monitored.
E. Erdmann et al.Page 2 of 11
Safety monitoringThe following safety variables were recorded: HR, SBP, systemic arter-ial diastolic blood pressure, treatment-emergent adverse events, andtreatment-emergent serious adverse events; estimated GFR (usingthe Modification of Diet in Renal Disease formula); laboratory para-meters (troponin I concentrations were measured in a central labora-tory and did not form part of standard care); electrocardiogram (ECG)parameters; mortality; and re-hospitalization.
Statistical analysisThe primary efficacy analysis was performed on the PPT population.Missing data were imputed using the LOCF method. The change inthe PCWP from baseline to 8 h/LOCF in the PPT population was eval-uated using analysis of covariance. Analysis of covariance was also usedto analyse all secondary exploratory outcome measures except theLikert dyspnoea scale, which was assessed using a stratified Wilcoxontest.
Using a standard deviation of 6.5 mmHg, a power of 90%, anda two-sided significance level of 5% with a 2:1 randomization,168 randomized patients were required for the PPT population todetect a clinically relevant, placebo-adjusted difference of 3.5 mmHgfor cinaciguat. The sample size was calculated using nQuery, version6.0, module MTTOU-1 (Statistical Solutions, Saugus, MA, USA). An in-validity rate of 20% was assumed, and thus 210 patients were plannedto be randomized.
The study was prematurely terminated after 158 patients had beenscreened. The protocol pre-specified that the study or single dosesteps should be terminated if drug-related adverse events occurredthat were so serious that the risk–benefit ratio was no longer accept-able, or if the results showed evidence of unacceptable risks. Termin-ation was suggested by the independent Data Monitoring Committeeand agreed upon by the Steering Committee and sponsor on the basisof a pronounced pharmacodynamic effect of cinaciguat. This effect ledto a high incidence of non-sustained hypotensive events at all the dosesstudied except 50–100 mg/h, which showed that there was amaximum tolerated dose in the study but that the study design didnot allow the identification of the minimum effective dose. Datafrom 139 patients were judged to be valid for the primary PPT analysis
of the PCWP. Using the same assumptions as above, the power of thestudy to detect a difference of 3.5 mmHg for cinaciguat was 85%.
Results
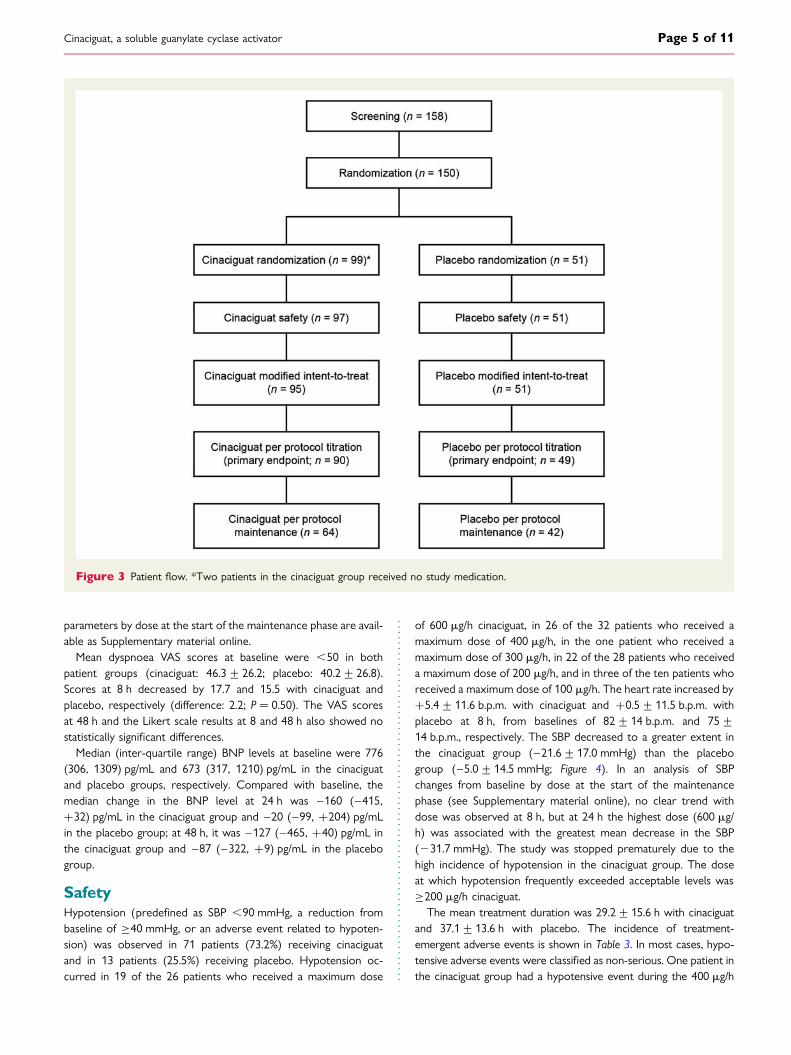
Study populationOf the 158 patients screened, 150 were eligible for inclusion(Figure 3). Two randomized patients received no study medication,resulting in 148 patients valid for the analysis. These patientsformed the safety population. Two additional patients wereexcluded from the modified intent-to-treat population [no haemo-dynamic assessment of PCWP post-baseline (n ¼ 1); took part inanother trial (n ¼ 1)]. A further seven patients were excludedfrom the PPT analysis, most commonly because critical invasivehaemodynamic measurements were deemed to be non-evaluableby the Adjudication Committee (n ¼ 4); other reasons includedprotocol violations and missing critical invasive haemodynamicmeasurements. The PPT population thus consisted of 139 patients.A further 33 patients were excluded from the per protocol main-tenance (PPM) phase analysis, with the most common reason forexclusion from the PPM population being lack of a valid PCWPmeasurement during the maintenance phase [n ¼ 18 (cinaciguat,n ¼ 14; placebo, n ¼ 4)].
Patient demographicsBaseline clinical and haemodynamic parameters are shown inTable 1 for the safety population. Data were similar for the cinaci-guat and placebo groups, except for the proportion of men, whichwas greater in the cinaciguat group. Because of the small number ofwomen receiving cinaciguat (9 patients; 9.3%), sex-based statisticalanalysis was not performed. In line with the critically ill nature ofthe patients in this population, a high prevalence of prior morbidityand cardiovascular medication use was recorded.
Figure 1 Cinaciguat dosing schedule and distribution of patients among dose groups. Boxes indicate the number of patients in each dosegroup in the per protocol titration population (note that one patient was switched to 300 mg/h at 8 h). *The number of patients per dosegroup in the per protocol maintenance population (final dose).
Cinaciguat, a soluble guanylate cyclase activator Page 3 of 11

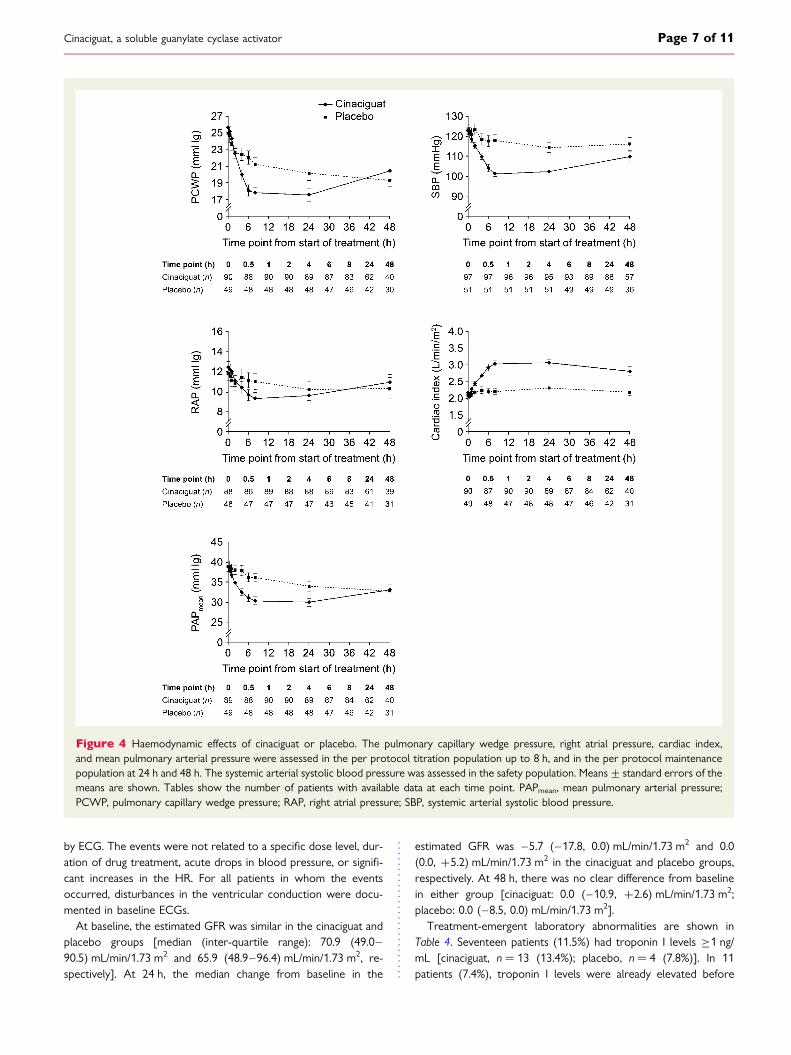
Primary efficacyIn total, 91.1% (82/90) of patients in the cinaciguat group and95.9% (47/49) in the placebo group continued to receive thestudy drug at the end of the 8-h titration phase. The numbersof patients per dose group and planned time point are shownin Figure 1. The mean baseline PCWP was 25.7+5.0 and25.0+5.3 mmHg in the cinaciguat and placebo groups, respective-ly. The administration of cinaciguat resulted in a significant reduc-tion in the mean PCWP from baseline to 8 h/LOCF comparedwith placebo (cinaciguat: 27.7 mmHg; placebo: 23.7 mmHg;difference: 4.0 mmHg; P , 0.0001) (Figure 4). Last post-baseline
observation carried forward was used for seven patients in thecinaciguat group and three patients in the placebo group.
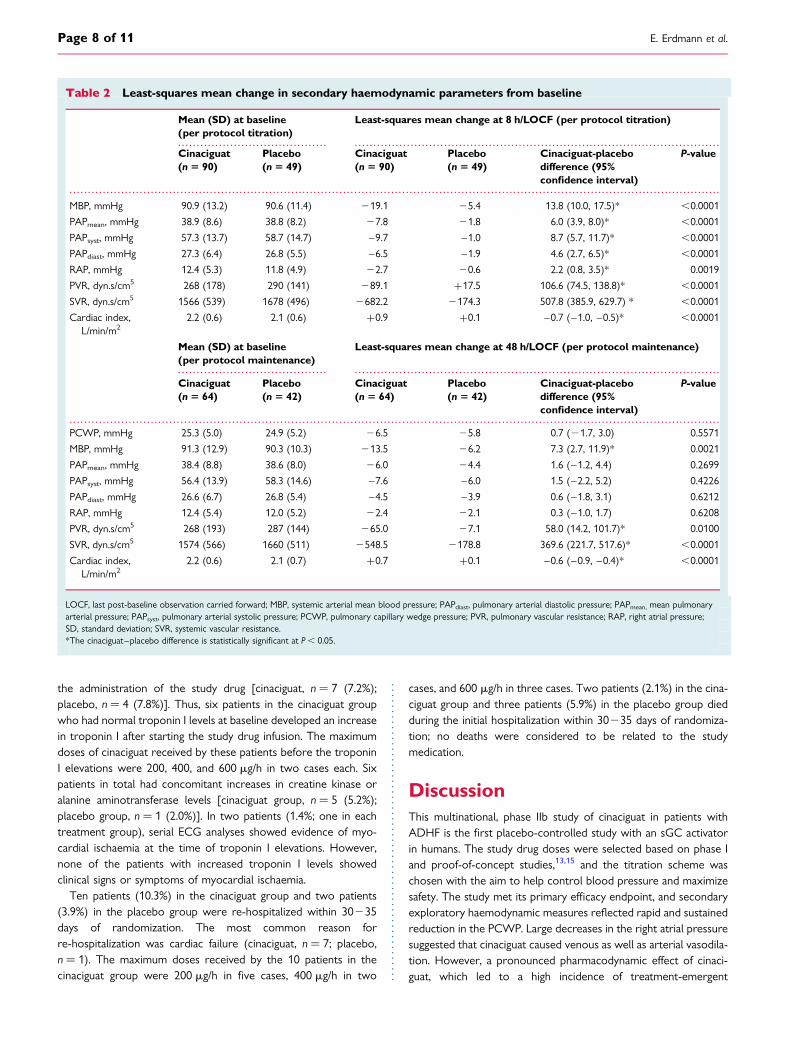
Secondary exploratory parametersThe administration of cinaciguat resulted in statistically significantreductions in the systemic arterial mean blood pressure, rightatrial pressure, mean pulmonary arterial pressure, and systemicand pulmonary vascular resistance (SVR and PVR, respectively)and significant increases in the cardiac index, from baseline to8 h/LOCF compared with placebo (Table 2; Figure 4). These changesfrom baseline were maintained at 48 h/LOCF. Haemodynamic
Figure 2 Dose titration scheme. *Up-titration was only performed during the titration phase. Up-titration from 400 to 600 mg/h was onlyperformed if the SBP was ≥110 mmHg. After down-titration, no up-titration was permitted. †Observed in two consecutive measurements.PCWP, pulmonary capillary wedge pressure; SBP, systemic arterial systolic blood pressure.
E. Erdmann et al.Page 4 of 11
parameters by dose at the start of the maintenance phase are avail-able as Supplementary material online.
Mean dyspnoea VAS scores at baseline were ,50 in bothpatient groups (cinaciguat: 46.3+ 26.2; placebo: 40.2+26.8).Scores at 8 h decreased by 17.7 and 15.5 with cinaciguat andplacebo, respectively (difference: 2.2; P ¼ 0.50). The VAS scoresat 48 h and the Likert scale results at 8 and 48 h also showed nostatistically significant differences.
Median (inter-quartile range) BNP levels at baseline were 776(306, 1309) pg/mL and 673 (317, 1210) pg/mL in the cinaciguatand placebo groups, respectively. Compared with baseline, themedian change in the BNP level at 24 h was –160 (–415,+32) pg/mL in the cinaciguat group and –20 (–99, +204) pg/mLin the placebo group; at 48 h, it was –127 (–465, +40) pg/mL inthe cinaciguat group and –87 (–322, +9) pg/mL in the placebogroup.
SafetyHypotension (predefined as SBP ,90 mmHg, a reduction frombaseline of ≥40 mmHg, or an adverse event related to hypoten-sion) was observed in 71 patients (73.2%) receiving cinaciguatand in 13 patients (25.5%) receiving placebo. Hypotension oc-curred in 19 of the 26 patients who received a maximum dose
of 600 mg/h cinaciguat, in 26 of the 32 patients who received amaximum dose of 400 mg/h, in the one patient who received amaximum dose of 300 mg/h, in 22 of the 28 patients who receiveda maximum dose of 200 mg/h, and in three of the ten patients whoreceived a maximum dose of 100 mg/h. The heart rate increased by+5.4+11.6 b.p.m. with cinaciguat and +0.5+11.5 b.p.m. withplacebo at 8 h, from baselines of 82+14 b.p.m. and 75+14 b.p.m., respectively. The SBP decreased to a greater extent inthe cinaciguat group (–21.6+17.0 mmHg) than the placebogroup (–5.0+14.5 mmHg; Figure 4). In an analysis of SBPchanges from baseline by dose at the start of the maintenancephase (see Supplementary material online), no clear trend withdose was observed at 8 h, but at 24 h the highest dose (600 mg/h) was associated with the greatest mean decrease in the SBP(231.7 mmHg). The study was stopped prematurely due to thehigh incidence of hypotension in the cinaciguat group. The doseat which hypotension frequently exceeded acceptable levels was≥200 mg/h cinaciguat.
The mean treatment duration was 29.2+15.6 h with cinaciguatand 37.1+13.6 h with placebo. The incidence of treatment-emergent adverse events is shown in Table 3. In most cases, hypo-tensive adverse events were classified as non-serious. One patient inthe cinaciguat group had a hypotensive event during the 400 mg/h
Figure 3 Patient flow. *Two patients in the cinaciguat group received no study medication.
Cinaciguat, a soluble guanylate cyclase activator Page 5 of 11
dose step that was deemed by the investigator to be serious anddrug related; the event resolved after discontinuation of the studydrug and infusion of saline. The mean duration of hypotensiveevents was 14.3+29.2 h in the cinaciguat group and 10.5+7.5 hin the placebo group. The mean time to the start of hypotensiveadverse events was 6.3+6.4 h in the cinaciguat group and14.5+14.5 h in the placebo group. In total, 49 patients in the cina-ciguat group had 65 treatment-emergent hypotensive adverseevents. Of these, 1, 8, 18, 2, 21, and 12 events started at cinaciguatdoses of 50, 100, 200, 300, 400, and 600 mg/h, respectively. Theremaining three events started within 1 day after stopping the
cinaciguat infusion. Details of serious adverse events and hypoten-sive adverse events occurring at different cinaciguat dose steps areavailable as Supplementary material online.
Ventricular tachycardia occurred in six patients, all in the cinaci-guat arm (two at a dose of 200 mg/h, one at a dose of 300 mg/h,one at a dose of 400 mg/h, and two after the infusion had beenstopped). Five of the six events were mild or moderate innature. In one of the patients, the ventricular tachycardia requiredtreatment by cardioversion (documented as a serious adverseevent). In the other five patients, non-sustained ventricular tachy-cardia was observed on the monitor but was not documented
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Baseline clinical features and haemodynamic parameters (safety population)
Safety population
Cinaciguat (n 5 97) Placebo (n 5 51)
Demographics
Age, mean (SD), years 62 (12) 61 (10)
Male, n (%) 88 (90.7) 38 (74.5)
Caucasian, n (%) 96 (99.0) 50 (98.0)
Body mass index, mean (SD), kg/m2 29 (5) 29 (6)
NYHA functional class
III, n (%) 65 (67.0) 36 (70.6)
IV, n (%) 32 (33.0) 15 (29.4)
Medical history
Myocardial infarction, n (%) 36 (37.1) 20 (39.2)
Coronary artery bypass, n (%) 14 (14.4) 9 (17.6)
Cardiac pacemaker insertion, n (%) 12 (12.4) 5 (9.8)
Implantable defibrillator insertion, n (%) 15 (15.5) 6 (11.8)
Diabetes mellitus, n (%) 26 (26.8) 12 (23.5)
Non-invasive haemodynamic parameters
Heart rate, mean (SD), b.p.m. 82 (14) 75 (14)
SBP, mean (SD), mmHg 123 (18) 123 (16)
DBP, mean (SD), mmHg 76 (14) 74 (13)
Biomarkers
B-type natriuretic peptide, median (IQR), pg/mLa 776 (306, 1309) 673 (317, 1210)
Estimated glomerular filtration rate, median (IQR), mL/min/1.73 m2 b 70.9 (49.0, 90.5) 65.9 (48.9, 96.4)
Cardiovascular medications
Diuretics, n (%) 92 (94.8) 48 (94.1)
Agents acting on the renin–angiotensin–aldosterone system, n (%) 82 (84.5) 47 (92.2)
Beta-blockers, n (%) 77 (79.4) 44 (86.3)
Serum lipid-reducing agents, n (%) 49 (50.5) 33 (64.7)
Vasoprotective agents other than standard therapy, n (%)c 18 (18.6) 17 (33.3)
Calcium channel blockers, n (%) 10 (10.3) 2 (3.9)
Other antihypertensives, n (%)c 9 (9.3) 2 (3.9)
DBP, systemic arterial diastolic blood pressure; IQR, inter-quartile range; NYHA, New York Heart Association; SBP, systemic arterial systolic blood pressure; SD, standarddeviation.aBaseline data available for 92 and 47 patients in the cinaciguat and placebo groups, respectively.bBaseline data available for 89 and 50 patients in the cinaciguat and placebo groups, respectively.cIn many of the countries included in the study, ‘vasoprotective agents other than standard therapy’ and ‘other antihypertensives’ included a range of treatments that are notclinically approved or widely scientifically acknowledged, for example homeopathic treatments.
E. Erdmann et al.Page 6 of 11
by ECG. The events were not related to a specific dose level, dur-ation of drug treatment, acute drops in blood pressure, or signifi-cant increases in the HR. For all patients in whom the eventsoccurred, disturbances in the ventricular conduction were docu-mented in baseline ECGs.
At baseline, the estimated GFR was similar in the cinaciguat andplacebo groups [median (inter-quartile range): 70.9 (49.0–90.5) mL/min/1.73 m2 and 65.9 (48.9–96.4) mL/min/1.73 m2, re-spectively]. At 24 h, the median change from baseline in the
estimated GFR was –5.7 (–17.8, 0.0) mL/min/1.73 m2 and 0.0(0.0, +5.2) mL/min/1.73 m2 in the cinaciguat and placebo groups,respectively. At 48 h, there was no clear difference from baselinein either group [cinaciguat: 0.0 (–10.9, +2.6) mL/min/1.73 m2;placebo: 0.0 (–8.5, 0.0) mL/min/1.73 m2].
Treatment-emergent laboratory abnormalities are shown inTable 4. Seventeen patients (11.5%) had troponin I levels ≥1 ng/mL [cinaciguat, n ¼ 13 (13.4%); placebo, n ¼ 4 (7.8%)]. In 11patients (7.4%), troponin I levels were already elevated before
Figure 4 Haemodynamic effects of cinaciguat or placebo. The pulmonary capillary wedge pressure, right atrial pressure, cardiac index,and mean pulmonary arterial pressure were assessed in the per protocol titration population up to 8 h, and in the per protocol maintenancepopulation at 24 h and 48 h. The systemic arterial systolic blood pressure was assessed in the safety population. Means+ standard errors of themeans are shown. Tables show the number of patients with available data at each time point. PAPmean, mean pulmonary arterial pressure;PCWP, pulmonary capillary wedge pressure; RAP, right atrial pressure; SBP, systemic arterial systolic blood pressure.
Cinaciguat, a soluble guanylate cyclase activator Page 7 of 11
the administration of the study drug [cinaciguat, n ¼ 7 (7.2%);placebo, n ¼ 4 (7.8%)]. Thus, six patients in the cinaciguat groupwho had normal troponin I levels at baseline developed an increasein troponin I after starting the study drug infusion. The maximumdoses of cinaciguat received by these patients before the troponinI elevations were 200, 400, and 600 mg/h in two cases each. Sixpatients in total had concomitant increases in creatine kinase oralanine aminotransferase levels [cinaciguat group, n ¼ 5 (5.2%);placebo group, n ¼ 1 (2.0%)]. In two patients (1.4%; one in eachtreatment group), serial ECG analyses showed evidence of myo-cardial ischaemia at the time of troponin I elevations. However,none of the patients with increased troponin I levels showedclinical signs or symptoms of myocardial ischaemia.
Ten patients (10.3%) in the cinaciguat group and two patients(3.9%) in the placebo group were re-hospitalized within 30235days of randomization. The most common reason forre-hospitalization was cardiac failure (cinaciguat, n ¼ 7; placebo,n ¼ 1). The maximum doses received by the 10 patients in thecinaciguat group were 200 mg/h in five cases, 400 mg/h in two
cases, and 600 mg/h in three cases. Two patients (2.1%) in the cina-ciguat group and three patients (5.9%) in the placebo group diedduring the initial hospitalization within 30235 days of randomiza-tion; no deaths were considered to be related to the studymedication.
DiscussionThis multinational, phase IIb study of cinaciguat in patients withADHF is the first placebo-controlled study with an sGC activatorin humans. The study drug doses were selected based on phase Iand proof-of-concept studies,13,15 and the titration scheme waschosen with the aim to help control blood pressure and maximizesafety. The study met its primary efficacy endpoint, and secondaryexploratory haemodynamic measures reflected rapid and sustainedreduction in the PCWP. Large decreases in the right atrial pressuresuggested that cinaciguat caused venous as well as arterial vasodila-tion. However, a pronounced pharmacodynamic effect of cinaci-guat, which led to a high incidence of treatment-emergent
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Least-squares mean change in secondary haemodynamic parameters from baseline
Mean (SD) at baseline(per protocol titration)
Least-squares mean change at 8 h/LOCF (per protocol titration)
Cinaciguat(n 5 90)
Placebo(n 5 49)
Cinaciguat(n 5 90)
Placebo(n 5 49)
Cinaciguat-placebodifference (95%confidence interval)
P-value
MBP, mmHg 90.9 (13.2) 90.6 (11.4) 219.1 25.4 13.8 (10.0, 17.5)* ,0.0001
PAPmean, mmHg 38.9 (8.6) 38.8 (8.2) 27.8 21.8 6.0 (3.9, 8.0)* ,0.0001
PAPsyst, mmHg 57.3 (13.7) 58.7 (14.7) –9.7 –1.0 8.7 (5.7, 11.7)* ,0.0001
PAPdiast, mmHg 27.3 (6.4) 26.8 (5.5) –6.5 –1.9 4.6 (2.7, 6.5)* ,0.0001
RAP, mmHg 12.4 (5.3) 11.8 (4.9) 22.7 20.6 2.2 (0.8, 3.5)* 0.0019
PVR, dyn.s/cm5 268 (178) 290 (141) 289.1 +17.5 106.6 (74.5, 138.8)* ,0.0001
SVR, dyn.s/cm5 1566 (539) 1678 (496) 2682.2 2174.3 507.8 (385.9, 629.7) * ,0.0001
Cardiac index,L/min/m2
2.2 (0.6) 2.1 (0.6) +0.9 +0.1 –0.7 (–1.0, –0.5)* ,0.0001
Mean (SD) at baseline(per protocol maintenance)
Least-squares mean change at 48 h/LOCF (per protocol maintenance)
Cinaciguat(n 5 64)
Placebo(n 5 42)
Cinaciguat(n 5 64)
Placebo(n 5 42)
Cinaciguat-placebodifference (95%confidence interval)
P-value
PCWP, mmHg 25.3 (5.0) 24.9 (5.2) 26.5 25.8 0.7 (21.7, 3.0) 0.5571
MBP, mmHg 91.3 (12.9) 90.3 (10.3) 213.5 26.2 7.3 (2.7, 11.9)* 0.0021
PAPmean, mmHg 38.4 (8.8) 38.6 (8.0) 26.0 24.4 1.6 (–1.2, 4.4) 0.2699
PAPsyst, mmHg 56.4 (13.9) 58.3 (14.6) –7.6 –6.0 1.5 (–2.2, 5.2) 0.4226
PAPdiast, mmHg 26.6 (6.7) 26.8 (5.4) –4.5 –3.9 0.6 (–1.8, 3.1) 0.6212
RAP, mmHg 12.4 (5.4) 12.0 (5.2) 22.4 22.1 0.3 (–1.0, 1.7) 0.6208
PVR, dyn.s/cm5 268 (193) 287 (144) 265.0 27.1 58.0 (14.2, 101.7)* 0.0100
SVR, dyn.s/cm5 1574 (566) 1660 (511) 2548.5 2178.8 369.6 (221.7, 517.6)* ,0.0001
Cardiac index,L/min/m2
2.2 (0.6) 2.1 (0.7) +0.7 +0.1 –0.6 (–0.9, –0.4)* ,0.0001
LOCF, last post-baseline observation carried forward; MBP, systemic arterial mean blood pressure; PAPdiast, pulmonary arterial diastolic pressure; PAPmean, mean pulmonaryarterial pressure; PAPsyst, pulmonary arterial systolic pressure; PCWP, pulmonary capillary wedge pressure; PVR, pulmonary vascular resistance; RAP, right atrial pressure;SD, standard deviation; SVR, systemic vascular resistance.*The cinaciguat–placebo difference is statistically significant at P , 0.05.
E. Erdmann et al.Page 8 of 11
hypotensive events at all the doses studied except 50–100 mg/h,was a major concern. It is possible that the concomitant use ofdiuretics and other blood pressure decreasing agents had anadded, synergistic effect on preload, and it is noteworthy thatthe hypotensive episodes occurred despite permitted changes inconcomitant therapy.
Hypotension is a common adverse event in clinical studies oftreatments for ADHF, but the incidence of hypotension in thecurrent study was substantially greater than that observed in pre-viously published studies. In clinical trials of i.v. nesiritide, hypoten-sion was the most common adverse event recorded; in a study ofpatients receiving nesiritide for up to 7 days, 11–17% developedsymptomatic hypotension and 12–24% developed asymptomatichypotension.16,17 Similarly, in the levosimendan Survival of Patientswith Acute Heart Failure in Need of Intravenous Inotropic Support(SURVIVE) trial, hypotension, together with cardiac failure, was themost common treatment-emergent adverse event recorded in
levosimendan-treated patients (15.5%).18 Also, in a randomized,controlled trial of milrinone, sustained hypotension requiring inter-vention was the most common adverse event during the indexhospitalization (10.7%).19 In the Value of Endothelin Receptor In-hibition with Tezosentan in Acute Heart Failure Study (VERITAS)trials, hypotension occurred in 22.7% of tezosentan-treatedpatients up to 5 days after initiating treatment, and was the mostcommon adverse event associated with discontinuation.20 Thehypotensive events suggest that these agents are more potentvasodilators than older, established agents; their use (particularlyin dose-finding studies and at high-dose levels) therefore requireskeen observation and a readiness to commence i.v. fluid adminis-tration when necessary.
No significant differences in dyspnoea were observed betweenthe cinaciguat and placebo groups in the current study. It is pos-sible that this was due to patients being supine and receiving stand-ard therapy including oxygen during the run-in period, and thus notbeing severely dyspnoeic even at baseline. As changes in diureticdoses in the first 8 h were not recorded, it cannot be ruled outthat the similar improvements in dyspnoea might also have beenpartly due to different doses of diuretics.
Ventricular tachycardia was more common in the cinaciguatgroup than the placebo group (though five of the six cases werenot confirmed by ECG). There was no difference in mortalitybetween the cinaciguat and placebo groups at 30–35 days post-randomization. This is in contrast to inotropic agents, which havebeen associated with increased in-hospital mortality.21 However,
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 3 Treatment-emergent adverse events, n (%)
Cinaciguat(n 5 97)
Placebo(n 5 51)
Any treatment-emergenta adverseevent
69 (71.1) 23 (45.1)
Hypotensionb 49 (50.5) 6 (11.8)
Ventricular tachycardia 6 (6.2) 0 (0.0)
Headache 6 (6.2) 0 (0.0)
Nausea 5 (5.2) 2 (3.9)
Vomiting 5 (5.2) 1 (2.0)
Any drug-relatedc treatment-emergentadverse event
58 (59.8) 9 (17.6)
Hypotension 47 (48.5) 4 (7.8)
Ventricular tachycardia 2 (2.1) 0 (0.0)
Headache 2 (2.1) 0 (0.0)
Nausea 2 (2.1) 0 (0.0)
Vomiting 3 (3.1) 0 (0.0)
Any treatment-emergent, seriousadverse eventb
9 (9.3) 1 (2.0)
Hypotension 2 (2.1) 0 (0.0)
Ventricular tachycardia 1 (0.0) 0 (0.0)
Nausea 1 (0.0) 0 (0.0)
Vomiting 1 (0.0) 0 (0.0)
Any drug-related treatment-emergentserious adverse event
5 (5.2) 0 (0.0)
Hypotension 1 (0.0) 0 (0.0)
Ventricular tachycardia 1 (0.0) 0 (0.0)
Nausea 1 (0.0) 0 (0.0)
Vomiting 1 (0.0) 0 (0.0)
aAdverse events starting after the start of infusion of the study drug up to 2 daysfollowing the stop of infusion of the study drug. Specific adverse events occurringin ≥5.0% of any treatment group are shown.bSee Supplementary material online for details of hypotensive adverse events andserious adverse events by the cinaciguat dose group.cAdverse events deemed by the investigator to be related to the study drug.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 4 Treatment-emergent laboratoryabnormalities above the upper limit of normal,% of patients in the cinaciguat and placebo groups
Upper limitof normal
Cinaciguat(n 5 97)
Placebo(n 5 51)
Clinical chemistry
Glucose, unspecified 99 mg/dL 85.7 71.4
Creatinine 1.5 mg/dL 20.9 14.6
Blood urea nitrogen 26 mg/dL 22.0 28.0
AST 40 U/L 8.0 2.3
GGT 65 U/La 2.6 8.3
LDH 480 U/L 25.5 56.3
Creatine kinase 204 U/Lb 3.8 8.5
Triglycerides 149 mg/dL 22.1 11.8
Troponin I 0.4 ng/mL 10.8 0.0
Urinalysis
Creatinine, urine 230 mg/dL 16.7 4.8
Microalbumin 20 mg/dL 44.8 29.4
AST, aspartate aminotransferase; GGT, gamma glutamyl transpeptidase;LDH, lactate dehydrogenase.Laboratory tests were performed at baseline, 24 and 48 h or at the end of infusion.Only measurements taken up to 1 day after stopping the infusion were included.Data are expressed as the percentage of patients without the respectiveabnormality at baseline who went on to show the abnormality post-baseline.aUpper limit of normal: 65 U/L for men and 60 U/L for women.bUpper limit of normal: 204 U/L for men and 173 U/L for women.
Cinaciguat, a soluble guanylate cyclase activator Page 9 of 11

the number of deaths in the current study was low overall,meaning that any between-group differences may have been indis-cernible. Re-hospitalization rates during the follow-up period of30–35 days were numerically higher in the cinaciguat group thanthe placebo group.
Elevated troponin I was identified as a predictor of in-hospitalmortality in two large patient populations enrolled in the ADHFNational Registry (ADHERE)22 and the Enhanced Feedback for Ef-fective Cardiac Treatment (EFFECT) study.23 In the current study,more patients had troponin I elevations in the cinaciguat groupthan in the placebo group. None of those patients showed clinicalsigns or symptoms of myocardial ischaemia, but the high incidenceof episodes of hypotension and troponin I elevations may havefavoured an increased rate of re-hospitalizations in the patientsassigned to cinaciguat. Troponin I increases have been observedpreviously in patients with heart failure without myocardial infarc-tion, and may reflect ongoing myocyte injury related to heartfailure.24
Limitations of this study include the fact that diuretic treatmentsduring the study period were not recorded and that laboratorytest data were not available for all patients. In addition, the propor-tion of patients who were on other vasodilators that were stoppedbefore the study drug infusion was not recorded. Another poten-tial limitation is the challenging patient population; compared withpatients hospitalized with heart failure in ADHERE,25 a higherproportion of patients in the current study had a left ventricularejection fraction ,40% or moderate/severe impairment (100 vs.54% in ADHERE).
The use of right heart catheterization implies a differencebetween the studied patients and those hospitalized for acuteheart failure in the real world as, generally, the patients who canbe studied by right heart catheterization are more clinicallystable. However, these types of studies are nevertheless manda-tory to establish the mechanisms of action of the study drug, itseffective doses, and its safety.
To be effective in ADHF, an ideal therapy should maintainthe SBP and decrease the PVR. The results from the presentstudy are consistent with cinaciguat activating sGC independent-ly of nitric oxide, and cinaciguat administration led to a remark-able decrease in the PVR, but with an undesirable decrease inSBP. The next goal would be to identify the dose at whichcinaciguat still decreases vascular resistance, but without alteringthe SBP.
In conclusion, the results of the current study indicate that cina-ciguat is an effective pulmonary and systemic vasodilator in patientswith ADHF, but the increase in hypotension associated with cina-ciguat doses ≥200 mg/h is a major concern. For this reason,several phase II dose-finding studies in patients with ADHF wereinitiated to investigate the safety and efficacy of i.v. cinaciguat atfixed doses ,200 mg/h. However, those studies were also termi-nated recently because of excessive hypotension and recruitmentdifficulties.26 Overall, the clinical results indicate that cinaciguatcannot be developed as an acute haemodynamic agent, but preclin-ical data suggest that sGC activators may also have long-term,pressure-independent organ-protective effects;12,27 these pres-sure-independent effects should become the focus of futureresearch.
Supplementary materialSupplementary material is available at European Heart Journalonline.
AcknowledgementsThe authors would like to thank Dr John Curram for statistical ana-lysis, the site investigators (listed in Appendix), the study coordina-tors, and the Data Monitoring Committee members (listed inAppendix). Dr Anja Becher and Dr Claire Mulligan of OxfordPharmaGenesisTM Ltd provided medical writing assistance.
FundingThis work was supported by Bayer HealthCare AG.
Conflict of interest: E.E. has received consulting fees, and researchand travel support from Bayer HealthCare AG. M.J.S. has received re-search support from Bayer HealthCare AG. M.S.N. has received con-sultation fees from Bayer HealthCare AG. M.G. has been a consultantfor Abbott Laboratories, Astellas, AstraZeneca, Bayer HealthCare AG,CorThera, Cytokinetics, DebioPharm S.A., Errekappa Terapeutici,GlaxoSmithKline, Ikaria, Johnson & Johnson, Medtronic, Merck, Novar-tis Pharma AG, Otsuka Pharmaceuticals, Palatin Technologies, PericorTherapeutics, Protein Design Laboratories, Sanofi-Aventis, Sigma Tau,Solvay Pharmaceuticals, Takeda Pharmaceutical, and Trevena Thera-peutics. R.A. is an employee of Bayer HealthCare AG. V.M. hasreceived consultation fees, speaking fees, and honoraria from BayerHealthCare AG and CardioPep Pharma GmbH. A.M. has received con-sultation fees from Bayer HealthCare AG and honoraria from Alere,Edwards, Brahms, and Orion.
AppendixSite investigators: Germany: Michael Bohm, Saarland UniversityHospital, Homburg/Saar; Georg Nickenig, University of BonnMedical Centre, Bonn; Stephan Felix, Ernst-Moritz-Arndt-University of Greifswald Clinic, Greifswald; Bernhard Brehm, JenaUniversity Hospital, Jena; Harald Lapp, HELIOS Clinic Erfurt,Erfurt. United States: Lynne Wagoner, Mercy Hospital Fairfield, Cin-cinnati. Poland: Lech Polonski, Silesian Centre for Heart Diseases,Zabrze; Zdzislawa Kornacewicz-Ja, Independent Public ClinicalHospital No. 2, Szczecin; Piotr Ponikowski, IV Military Hospital,Wroclaw; Andrzej Rynkiewicz, Independent Public Clinical Hos-pital No. 1, Gdansk. Italy: Laura Scelsi, IRCCS St. Matthew Poly-clinic, Pavia; Roberto Ferrari, University Hospital of Ferrara,Ferrara; Antonello Gavazzi, Riuniti Hospital, Bergamo. Spain:Javier Segovia Cubero, University Hospital Puerta de Hierro,Madrid. Canada: Marie-Helene Leblanc, Lavan Hospital, QuebecCity. Israel: Alon Marmor, Rebecca Sieff Hospital, Safed; BasilLewis, Lady Davis Carmel Medical Centre, Haifa. Hungary:Andras Vertes, Szent Istvan Hospital, Budapest. Russia: VitaliySulimov, 1st Moscow Medical Academy, Moscow; Grigory Arutyu-nov, Municipal Hospital N 4, Moscow. Lithuania: Pranas Serpytis,Vilnius University, Vilnius; Zita Bertasiene, Kaunas University,Kaunas. Slovenia: Marko Noc, Medical Centre, Ljubljana. Croatia:Vejran Nikolic-Heitzler, Sestre Milosrdnice University Hospital,Zagreb. Serbia: Miodrag Ostojic, Petar Seferovic, Clinical Centreof Serbia, Belgrade; Slobodan Dodic, Institute of CardiovascularDiseases Vojvodina, Sremska; Lazar Angelkov, Dedinje
E. Erdmann et al.Page 10 of 11

Cardiovascular Institute, Belgrade. Data Monitoring Committee:Peter Sleight, John Radcliffe Hospital, Oxford; Wilhelm Haver-kamp, Charite Campus Virchow-Klinikum, Berlin; Chris Palmer,University of Cambridge School of Clinical Medicine, Cambridge.
References1. Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJ, Ponikowski P,
Poole-Wilson PA, Stromberg A, van Veldhuisen DJ, Atar D, Hoes AW,Keren A, Mebazaa A, Nieminen M, Priori SG, Swedberg K, Vahanian A,Camm J, De Caterina R, Dean V, Funck-Brentano C, Hellemans I,Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P,Zamorano JL. ESC Guidelines for the diagnosis and treatment of acute andchronic heart failure 2008: the Task Force for the Diagnosis and Treatment ofAcute and Chronic Heart Failure 2008 of the European Society of Cardiology.Developed in collaboration with the Heart Failure Association of the ESC(HFA) and endorsed by the European Society of Intensive Care Medicine(ESICM). Eur Heart J 2008;29:2388–2442.
2. Onwuanyi A, Taylor M. Acute decompensated heart failure: pathophysiology andtreatment. Am J Cardiol 2007;99:25D–30D.
3. Allen LA, O’Connor CM. Management of acute decompensated heart failure.CMAJ 2007;176:797–805.
4. Chung P, Hermann L. Acute decompensated heart failure: formulating anevidence-based approach to diagnosis and treatment (part I). Mt Sinai J Med2006;73:506–515.
5. Alla F, Zannad F, Filippatos G. Epidemiology of acute heart failure syndromes.Heart Fail Rev 2007;12:91–95.
6. Munzel T, Daiber A, Mulsch A. Explaining the phenomenon of nitrate tolerance.Circ Res 2005;97:618–628.
7. Pacher P, Beckman JS, Liaudet L. Nitric oxide and peroxynitrite in health anddisease. Physiol Rev 2007;87:315–424.
8. Evgenov OV, Pacher P, Schmidt PM, Hasko G, Schmidt HH, Stasch JP.NO-independent stimulators and activators of soluble guanylate cyclase: discov-ery and therapeutic potential. Nat Rev Drug Discov 2006;5:755–768.
9. Tamargo J, Duarte J, Caballero R, Delpon E. Cinaciguat, a soluble guanylatecyclase activator for the potential treatment of acute heart failure. Curr Opin Inves-tig Drugs 2010;11:1039–1047.
10. Martin F, Baskaran P, Ma X, Dunten PW, Schaefer M, Stasch JP, Beuve A, van denAkker F. Structure of cinaciguat (BAY 58-2667) bound to nostoc H-NOX domainreveals insights into heme-mimetic activation of the soluble guanylyl cyclase. J BiolChem 2010;285:22651–22657.
11. Boerrigter G, Costello-Boerrigter LC, Cataliotti A, Lapp H, Stasch JP, Burnett JCJr. Targeting heme-oxidized soluble guanylate cyclase in experimental heartfailure. Hypertension 2007;49:1128–1133.
12. Jones ES, Kemp-Harper B, Stasch JP, Schmidt H, Widdop RE. Cardioprotectiveeffects in aged spontaneously hypertensive rats due to chronic stimulation/activa-tion of sGC without hypotension. BMC Pharmacol 2009;9 (Suppl 1):29.
13. Lapp H, Mitrovic V, Franz N, Heuer H, Buerke M, Wolfertz J, Mueck W, Unger S,Wensing G, Frey R. Cinaciguat (BAY 58-2667) improves cardiopulmonary hemo-dynamics in patients with acute decompensated heart failure. Circulation 2009;119:2781–2788.
14. Nieminen MS, Bohm M, Cowie MR, Drexler H, Filippatos GS, Jondeau G, Hasin Y,Lopez-Sendon J, Mebazaa A, Metra M, Rhodes A, Swedberg K, Priori SG,Garcia MA, Blanc JJ, Budaj A, Dean V, Deckers J, Burgos EF, Lekakis J,Lindahl B, Mazzotta G, Morais J, Oto A, Smiseth OA, Dickstein K,
Albuquerque A, Conthe P, Crespo-Leiro M, Ferrari R, Follath F, Gavazzi A,Janssens U, Komajda M, Moreno R, Singer M, Singh S, Tendera M, Thygesen K.Executive summary of the guidelines on the diagnosis and treatment of acuteheart failure: the Task Force on Acute Heart Failure of the European Societyof Cardiology. Eur Heart J 2005;26:384–416.
15. Frey R, Muck W, Unger S, Artmeier-Brandt U, Weimann G, Wensing G. Pharma-cokinetics, pharmacodynamics, tolerability, and safety of the soluble guanylatecyclase activator cinaciguat (BAY 58-2667) in healthy male volunteers. J Clin Phar-macol 2008;48:1400–1410.
16. Colucci WS. Nesiritide for the treatment of decompensated heart failure. J CardFail 2001;7:92–100.
17. Colucci WS, Elkayam U, Horton DP, Abraham WT, Bourge RC, Johnson AD,Wagoner LE, Givertz MM, Liang CS, Neibaur M, Haught WH, LeJemtel TH. Intra-venous nesiritide, a natriuretic peptide, in the treatment of decompensated con-gestive heart failure. Nesiritide Study Group. N Engl J Med 2000;343:246–253.
18. Mebazaa A, Nieminen MS, Packer M, Cohen-Solal A, Kleber FX, Pocock SJ,Thakkar R, Padley RJ, Poder P, Kivikko M. Levosimendan vs dobutamine forpatients with acute decompensated heart failure: the SURVIVE RandomizedTrial. JAMA 2007;297:1883–1891.
19. Cuffe MS, Califf RM, Adams KF Jr, Benza R, Bourge R, Colucci WS, Massie BM,O’Connor CM, Pina I, Quigg R, Silver MA, Gheorghiade M. Short-term intraven-ous milrinone for acute exacerbation of chronic heart failure: a randomized con-trolled trial. JAMA 2002;287:1541–1547.
20. McMurray JJ, Teerlink JR, Cotter G, Bourge RC, Cleland JG, Jondeau G, Krum H,Metra M, O’Connor CM, Parker JD, Torre-Amione G, van Veldhuisen DJ,Lewsey J, Frey A, Rainisio M, Kobrin I. Effects of tezosentan on symptoms andclinical outcomes in patients with acute heart failure: the VERITAS randomizedcontrolled trials. JAMA 2007;298:2009–2019.
21. Mebazaa A, Parissis J, Porcher R, Gayat E, Nikolaou M, Boas FV, Delgado JF,Follath F. Short-term survival by treatment among patients hospitalized withacute heart failure: the global ALARM-HF registry using propensity scoringmethods. Intensive Care Med 2011;37:290–301.
22. Peacock WF, De Marco T, Fonarow GC, Diercks D, Wynne J, Apple FS, Wu AH.Cardiac troponin and outcome in acute heart failure. N Engl J Med 2008;358:2117–2126.
23. You JJ, Austin PC, Alter DA, Ko DT, Tu JV. Relation between cardiac troponin Iand mortality in acute decompensated heart failure. Am Heart J 2007;153:462–470.
24. Roongsritong C, Warraich I, Bradley C. Common causes of troponin elevations inthe absence of acute myocardial infarction: incidence and clinical significance.Chest 2004;125:1877–1884.
25. Sweitzer NK, Lopatin M, Yancy CW, Mills RM, Stevenson LW. Comparison ofclinical features and outcomes of patients hospitalized with heart failure andnormal ejection fraction (. or¼55%) versus those with mildly reduced (40%to 55%) and moderately to severely reduced (,40%) fractions. Am J Cardiol2008;101:1151–1156.
26. Gheorghiade M, Filippatos G, Erdmann E, Ferrari R, Levy PD, Maggioni A,Nowack C, Mebazaa A. Treatment of acute decompensated heart failure withthe soluble guanylate cyclase activator cinaciguat: The COMPOSE program:three randomized, controlled, phase IIb studies. J Card Fail 2011;17:971.
27. Benz K, Orth SR, Simonaviciene A, Linz W, Schindler U, Rutten H, Amann K.Blood pressure-independent effect of long-term treatment with the solubleheme-independent guanylyl cyclase activator HMR1766 on progression in amodel of noninflammatory chronic renal damage. Kidney Blood Press Res 2007;30:224–233.
Cinaciguat, a soluble guanylate cyclase activator Page 11 of 11




![EUROPE AND CENTRAL EURASIA [ADVANCE RELEASE] · EuropE and CEntral Eurasia—2010 [adVanCE rElEasE] 1.1 The Mineral indusTries of europe and CenTral eurasia By Alberto Alexander Perez,](https://img.dokumen.tips/doc/110x75/5fb12128d7f0ba42711cf746/europe-and-central-eurasia-advance-release-europe-and-central-eurasiaa2010-advance.jpg)
























