Embed Size (px)
Citation preview

At the age of 30, the patient presents with a 2 year history of infertility. Her menses are still regular but she has 2-3 days of spotting before her menses are due. She also complains of pain with intercourse and pelvic pain. In reviewing the patient’s history, the gynecologist notes that over the past year the patient was repeatedly treated by her internist with antibiotics for recurrent microscopic hematuria.

What is the most likely diagnosis?What are the main theories regarding the
pathogenesis in this case?How would you evaluate and treat this
patient?

Theories
Retrograde menstruation (Sampson)Hematogenous or lymphatic spread (Halban)Coelomic metaplasia (Meyer/Novack)Iatrogenic disseminationImmunologic defects (Dmowski)Genetic predisposition

Symptoms
Asymptomatic DysmenorrhoeaMenorrhagia Lower abdominal
painInfertilityChronic pelvic painCyclical bleeding
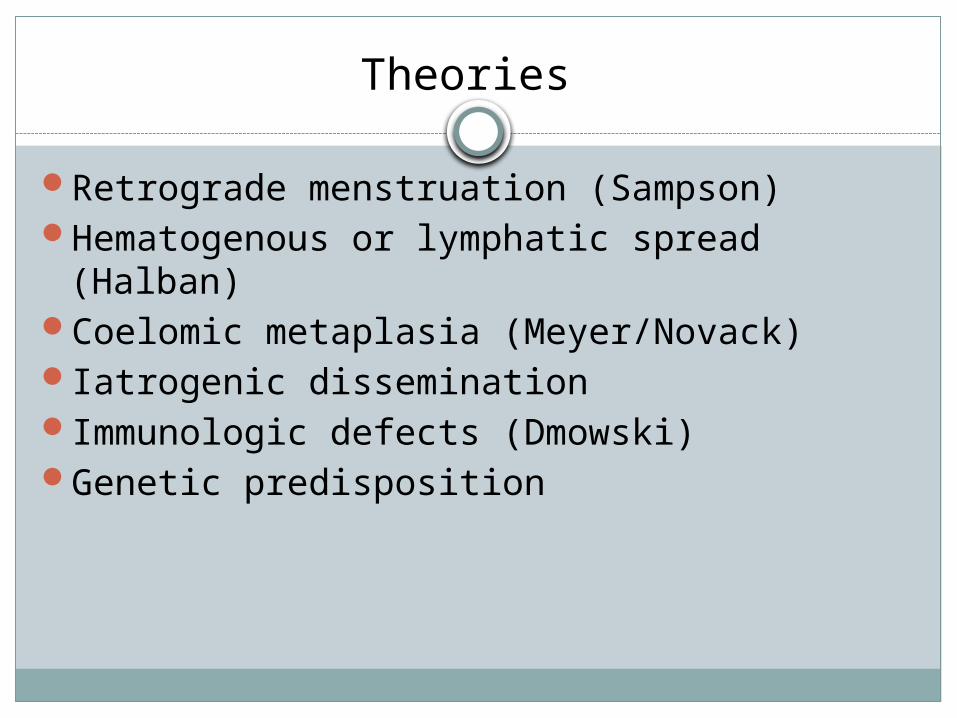
Signs
P/A Cystic swelling Fixed Tender
P/S Bluish or blakish puckered spot
P/V Tender ,fixed, retroverted uterus B/L mass Palpable tender nodules in POD/utero-sacral
Differential diagnosis
PIDUterine myomaMetastatic deposit of malignant ovaryRectal malignancy




Prevention is better than cure
Avoid pelvic examination during / tubal patency test in premenstrual phase
Schedule surgery on genital tract in postmenstrual phase
Age Need for preserving reproductive functionSeverity of symptomsExtent of diseasesResponse to medical management Attitude of the patient towards her problem

Objective of treatment
To eradicate the lesionAvoid recurrence Alleviate the symptomsFacilitate the child bearing Lead a comfortable life

Management
Asymptomatic Expectant
Symptomatic Medical Minimal invasive surgery Surgery

Medical
NSAIDCOCProgestogensGnRH analogues Aromatase inhibitorsRU-486

Minimal invasive surgery
Destruction by cautery, laser vaporizationExcision of cystAdhesiolysisPresacral neurectomyLUNA

Surgery
Incision of cyst and removal of liningSalpingo-oophorectomyHysterectomy +/- BSOScar excision
Assessment
Discuss the C/F and management of pelvic endometriosis in a young nulliparus woman
A woman, P1L1 with dysmenorrhoea , menorrhagia and chronic pelvic pain. A tender mas is felt in right fornix . How will you investigate and manage the case ?
Short notes C/F and management of chocolate cyst of ovary
Reference
Shaw’s Text book of Gynaecology 16th edition