Embed Size (px)
Citation preview

CROUZON SYNDROME: A CASE REPORT
Dr. Asmita A.Indurkar, Dr. V.L.Une, Dr. V.S.NandedkarDepartment of Ophthalmology
Government Medical College & Hospital,Aurangabad

INTRODUCTION Autosomal dominant disorder with complete penetrance and variable
expressivity. Prevalence of 1 in 25,000 live births, and it constitutes 4.8% of all
craniosynostosis. Described by a French neurologist Octave Crouzon in 1912, it is a rare
genetic disorder. Caused by mutation in the fibroblast growth factor receptor 2 (FGFR2)
gene.

CLINICAL FEATURES• Premature closure of cranial sutures results in abnormal skull growth.• This affects development of orbits and maxillary complex,occasionally
causing airway obstruction.• Hypertelorism• Exophthalmos• Strabismus• Short upper lip• Beaked nose• Maxillary hypoplasia and relative mandibular retrognathism
Case report• 9 year old female child presented in OPD with complaint of diminished
vision in both eyes• She was born of non-consanguineous marriage. Her birth was uneventful.
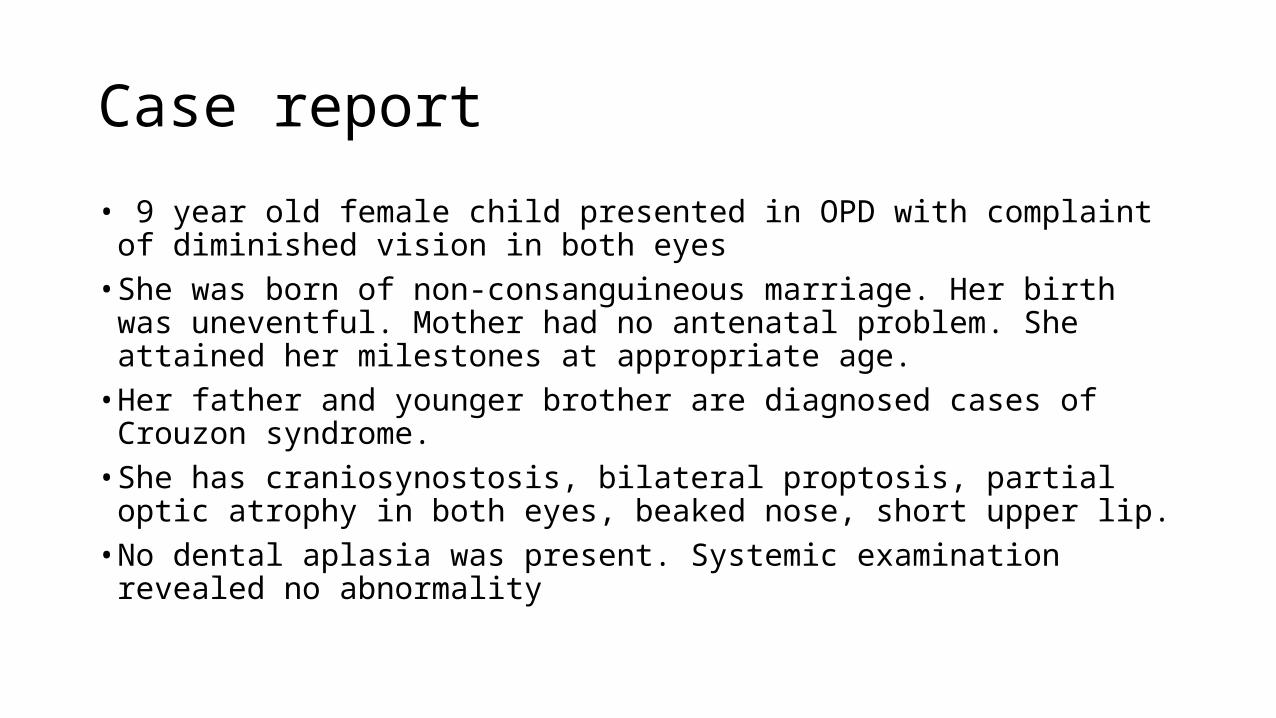
Mother had no antenatal problem. She attained her milestones at appropriate age.• Her father and younger brother are diagnosed cases of Crouzon syndrome.• She has craniosynostosis, bilateral proptosis, partial optic atrophy in both
eyes, beaked nose, short upper lip.• No dental aplasia was present. Systemic examination revealed no
abnormality

Figure 1 : Front view Figure 2 : Lateral view
Patient Profile
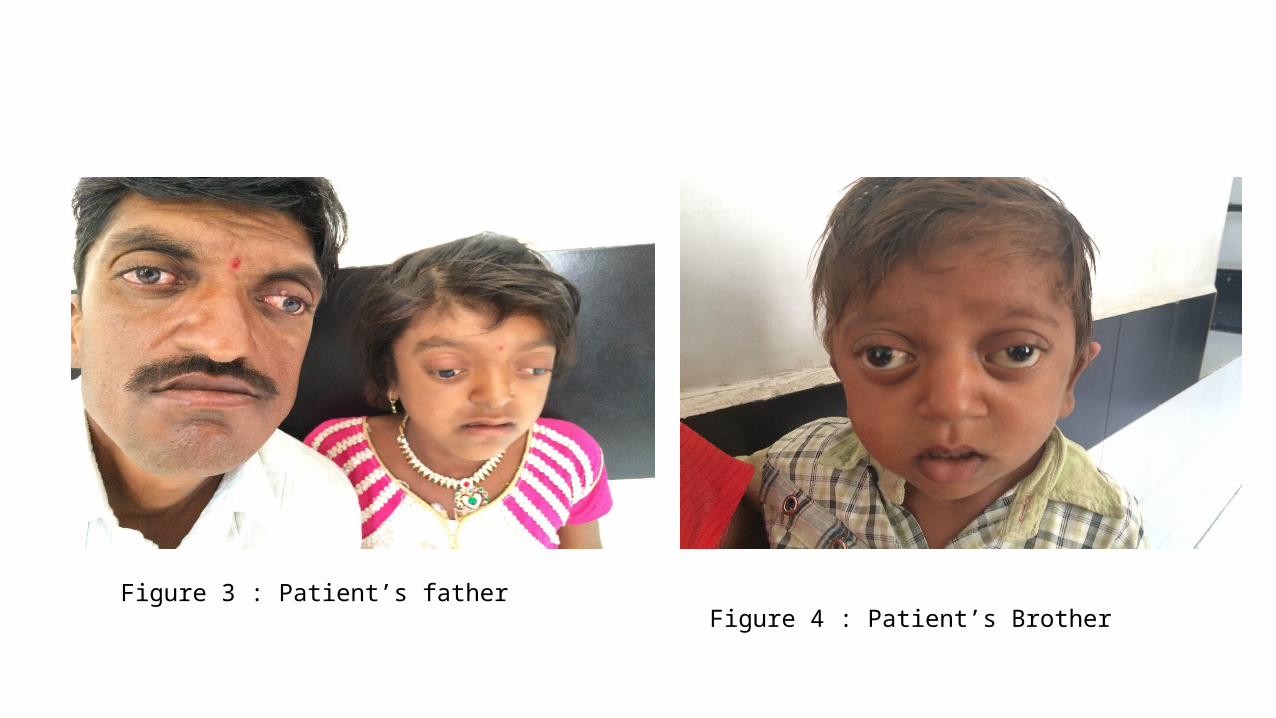
Figure 3 : Patient’s father Figure 4 : Patient’s Brother

OPHTHALMIC EXAMINATION
• Subjective visual acuity is bilaterally poor.• BCVAs (best corrected visual acuity) in the both eyes was 1/60 (O.U).• The objective eye refraction (Sol. Cyclopentolate 2%) indicates +1 D
in both horizontal and vertical axis in both eyes. • Intraocular pressure measured by the Schiotz impression tonometer
was 14.60 mmHg bilaterally. • Interpupillary distance was 68mm. The corneal diameter was 12mm. • Bilateral exophthalmos was observed readings were 22 mm in both
eyes (OU)

• Apart from the bigger diameter of the cornea, biomicroscopic findings of the anterior segment of the eye were normal.• Schirmer's test 1 values were normal (15mm) OU.• The ophthalmoscopic findings were BE Optic atrophy. • Manifest divergent strabismus of 45 degrees in LE in the primary
position was found.

Figure 5 : Left eye Figure 6 : Right eye
Fundus Photographs

• The girl was given artificial tears eye drops and a gel for the future topical use.
• The father was explained the nature of his child's disease and the reason for poorsightedness.
• The girl was recommended consultation of a maxillofacial surgeon.
• Early management would have helped to avoid blindness.

• Early detection of Crouzon syndrome should be done to reduce amblyopia by correction of refractive errors and patching.
• Timely treatment of strabismus.
• Optic atrophy remains an important cause of visual impairment in these patients.

References :1) Gordana Stankovic-Babic,Rade R. Babic.Ophthalmological and radiological picture of crouzon syndrome – a case report.ActaMedica Medianae 2009;48(2):37-40.2) Ahmed I, Afzal A. Diagnosis and evaluation of crouzon syndrome. J Coll Physicians Surg Pak 2009;19(5):318-20.3) Bowling EL, Burstein FD. Crouzon syndrome. Optometry 2006; 77:217-22.4) Horbelt CV. Physical and oral characteristics of Crouzon syndrome, Apert syndrome, and Pierre Robin sequence. Gen Dent 2008;56(2):132-4.





























