Embed Size (px)
Citation preview

Axial Spondyloarthritis2016 Treatment Update
Nigil Haroon MD, PhD, DM
Asst. Professor of Medicine and RheumatologyUniversity of Toronto
Clinician Scientist and Attending PhysicianUniversity Health Network, Toronto
University of Toronto

Nigil Haroon. University of Toronto
Disclosures
• Consultant for Amgen, Abbvie, Celgene, Janssen, MSD, Novartis, UCB.
• Work Supported By CIHR Krembil Foundation TGTW Foundation

Nigil Haroon. University of Toronto
Cardiovascular mortality is increased in
A. Rheumatoid ArthritisB. Ankylosing SpondylitisC. Both A & B

Nigil Haroon. University of Toronto
Objectives
• Pathogenic Basis for Treatment Options in AxSpA
• Window of opportunity in AS treatment
• Interleukin 17A inhibition in AS
• Discuss 2016 update of ASAS/EULAR Recommendations
Nigil Haroon. University of Toronto
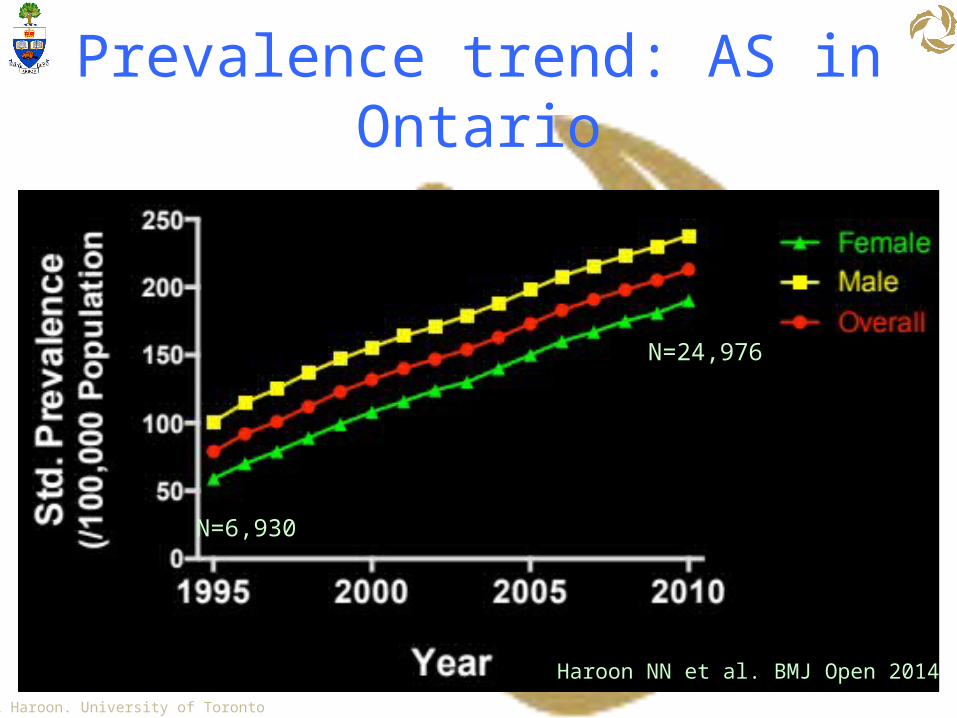
Prevalence trend: AS in Ontario
N=6,930
N=24,976
Haroon NN et al. BMJ Open 2014
Nigil Haroon. University of Toronto
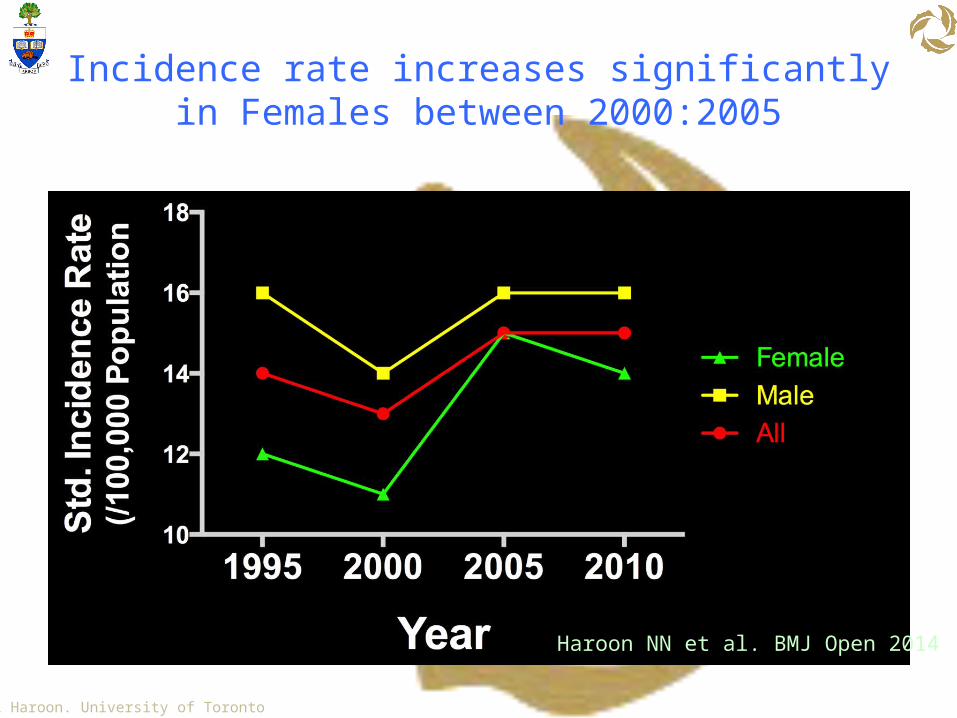
Incidence rate increases significantly in Females between 2000:2005
Haroon NN et al. BMJ Open 2014

Nigil Haroon. University of Toronto
Goals of AxSpA Treatment
Baraliakos et al. Arthritis Research & Therapy 2008, 10:R104

Nigil Haroon. University of Toronto
Goals of AxSpA Treatment
Inflammation
New Bone Formation
Functional Capacity
Vascular Morbidity
Vascular Mortality
Haroon NN, et al. Annals of Internal Medicine: 2014

Nigil Haroon. University of Toronto
AS: Vascular Mortality
Haroon NN, et al. Annals of Internal Medicine: 2014
Favours ASFavours Controls
0
Cardio-V Mortality
Cerebro-V Mortality
HR: 1.35; 1.07-1.70
HR: 1.60; 1.17-2.20
1 2
35%
60%

Nigil Haroon. University of Toronto
STIR +: Inflammation T cells HypertrophicChondrocytes
Inflammatory Infiltrate (T, Fib, Mac)
CalcificationNew Bone
In situ hybridization TNFα mRNA in cellular infiltrate
Inflammatory Infiltrates in SI Joints
Braun J et al. Arthritis Rheum. 1995 Apr;38(4):499-505.
Bollow et al. Ann Rheum Dis 2000;59:135–140

Nigil Haroon. University of Toronto
IL-17+ve cells increased in SpA
Appel et al. Arthritis Research & Therapy 2011, 13:R95

Nigil Haroon. University of Toronto

Nigil Haroon. University of Toronto
Remains active
TNFi
TNFi Contraindication
Active AS
Remains active
Isolated sacroiliitis
Peripheral arthritis
Enthesitis
Monitor validated AS-Specific Disease Activity Measure, CRP, or ESR regularly
LEGENDStrongly recommendConditionally recommendConditionally recommend againstStrongly recommend againstQualifier
NSAIDsUse continuously if active
No preferred drug
No preferred drug
PhysicalTherapy Land-based over aquatic
Active over passive
Alternative TNFi
Local GC
Local GC Consider if ≤2 joints; use infrequently
Local GC Avoid Achilles, patellar, quadriceps
Non-TNFi biologic
Slow-Acting Drugs (SSZ, pamidronate)
Consider if peripheral joint disease or TNFi contraindcations
Systemic glucocorticoidsConsider if peripheral flare, pregnancy, IBD flare
use infliximab or adalimumab
Recurrent iritis
IBDuse TNFi monoclonals
Unsupervised back exercises, formal group or individual self-management education, fall evaluation/counseling

Nigil Haroon. University of Toronto
Delays in starting treatment has significant consequences in the management of AS
A. TrueB. False

Nigil Haroon. University of Toronto
Window of Opportunity

Nigil Haroon. University of Toronto

Nigil Haroon. University of Toronto
Davis JC Jr. et al. Arthritis Rheum 2003;48:3230-6; van der Heijde D et al. Arthritis Rheum 2005;52:582-91; van der Heijde D et al. Arthritis Rheum 2006;54:2136-46; Humira Product Monograph, Abbott Laboratories Ltd., 2009; Inman RD et al. Arthritis Rheum 2008;58(11):3402-12.
Anti-TNFs in AS: ASAS20 at 24 Weeks%
pat
ient
s
p<0.001
GolimumabEtanercept Adalimumab
p<0.001p<0.0001 p<0.001
Infliximab
p<0.001

Nigil Haroon. University of Toronto
31.3
18.812.5 15.0
77.8
61.155.6 60.0
0
20
40
60
80
100
ASAS 20 ASAS 50 Part. Remission BASDAI 50
Placebo Infliximab
Barkham N, et al. Arthritis Rheum. 2009;60:946-954.
P=0.006P=0.012 P=0.009 P=0.006
Perc
enta
ge o
f Pat
ient
sEfficacy of Infliximab in B27+ Patients
With MRI+ Early Sacroiliitis
Week 16

Nigil Haroon. University of Toronto
Nigil Haroon. University of Toronto

Nigil Haroon. University of Toronto

Nigil Haroon. University of Toronto
BASDAI50 response – Wk12
>=40% 20-40% 10-20% <10%
Vastesaeger N et al.Ann Rheum Dis 70:973, 2011.

Nigil Haroon. University of Toronto Alper M van Sijl et al. Ann Rheum Dis 2015;74:119-123
TNFi and progression of subclinical atherosclerosis in AS

Nigil Haroon. University of Toronto
TNFi and progression of subclinical atherosclerosis in AS
No-TNFi TNFI Rx0.59
0.60.610.620.630.640.650.660.670.680.69
PrePost
Correlation of ΔBASDAI & cIMTR = 0.308 (p=0.013)
CAROTID IMT

Nigil Haroon. University of Toronto
Spinal Fusion in AS &Window of Opportunity

Nigil Haroon. University of Toronto
Wide Variability in Progression of SpA
0 10 20 30 40 50 60 70 80 90 10005
1015202530354045
Δ m
SASS
S
Cumulative Probability Plot
© NIGIL HAROON

Nigil Haroon. University of Toronto
Predictors of Progression
Inflammation
Damage
Smoking
p < 0.001
p < 0.001
P = 0.002
Haroon N et al. Arthritis Rheum 2013

Nigil Haroon. University of Toronto
Spondyloarthritis
Inflammation
New Bone Formation
Inflammation New Bone Formation
Inflammation New Bone Formation

Nigil Haroon. University of Toronto
ASDAS and Progression of Spinal Fusion
< 1.3 1.3-2.1 2.1-3.5 >3.50
0.5
1
1.5
2
2.5
3
3.5
Rate
of m
SASS
S Pr
ogre
ssio
n (u
nits
/2yr
s)
Baseline ASDAS
Ramiro S. ARD. 2014

Inflammation and New Bone Formation
Baraliakos et al. Arthritis Research & Therapy 2008, 10:R104

Nigil Haroon. University of Toronto
It is important to continue NSAIDs even if patients are doing well on TNF inhibitors
A.TrueB.False

Nigil Haroon. University of Toronto
Mean daily dose of celecoxib: 243 mg in the continuous-
treatment group and 201 mg in the on-demand group.
Mean difference: 42 mg (P 0.0001).

Nigil Haroon. University of TorontoJoachim Sieper et al. Ann Rheum Dis doi:10.1136/annrheumdis-2015-207897
ENRADAS Study
Continuous GroupN=85
Continuous GroupN=62
On Demand GroupN=60
Baseline
2yr FU
NSAIDS continous group vs On Demand
On Demand GroupN=82
Effects of NSAIDs on RAdiographic Damage in Ankylosing Spondylitis

Nigil Haroon. University of Toronto Joachim Sieper et al. Ann Rheum Dis doi:10.1136/annrheumdis-2015-207897
ENRADAS: NSAID Index
Mean daily dose: 112mg
Mean daily dose: 66mg

Nigil Haroon. University of Toronto
Cumulative probability plot of X-ray Progression

Nigil Haroon. University of Toronto
ACR Abstract # 758. Sieper et al.
CONCLUSION
NSAIDs have no disease modifying effect
IMPLICATIONS
NSAIDs should be used for symptom modification in ASIf patients are stable on TNFi, NSAID continuation is
not warranted

Nigil Haroon. University of Toronto
OASIS data: mSASSS rate (p=ns)*
infliximab OASIS OASIS meeting study criteria)0
0.2
0.4
0.6
0.8
1
1.2
1.4
Infliximab*
Etanercept OASIS OASIS meeting study criteria)0
0.2
0.4
0.6
0.8
1
1.2
1.4
Etanercept*
.91 .951.27
.9 1.01.2
van der Heijde D et al., Arthritis Rheum 2008;58: 1324-31
van der Heijde D et al., Arth Res Ther 2008;58: 1324-31
van der Heijde D et al., Arthritis Rheum 2008;58: 3063-70
Adalimumab OASIS OASIS meeting study criteria)0
0.2
0.4
0.6
0.8
1
1.2
Adalimumab*
.81.0 .9
Credit: Lianne Gensler

Nigil Haroon. University of Toronto
Study Centers
United States
Toronto
Haroon N et al. Arthritis Rheum 2013
Nigil Haroon. University of Toronto
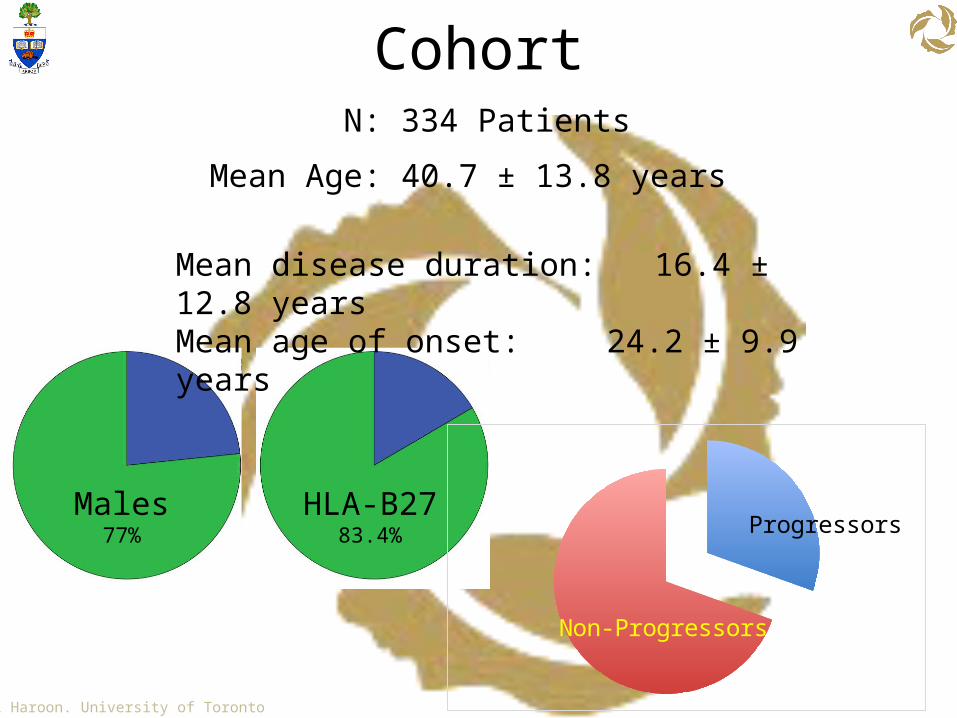
CohortN: 334 Patients
HLA-B2783.4%
Males77%
Mean Age: 40.7 ± 13.8 years
Mean disease duration: 16.4 ± 12.8 yearsMean age of onset: 24.2 ± 9.9 years
Progressors
Non-Progressors

Nigil Haroon. University of Toronto
Early use of TNF-inhibitors reduces rate of radiographic progression
N=120N=42N=39
OR: 0.36; CI:0.15-0.91; p=0.03
Haroon N et al. Arthritis Rheum 2013

Nigil Haroon. University of Toronto
Best results when TNF-inhibitors started within 10 years of disease onset
60%
20%
Haroon N et al. Arthritis Rheum 2013

Nigil Haroon. University of Toronto
The Effect of TNF Inhibition on Radiographic Progression inAnkylosing Spondylitis: An Observational Cohort Study of
374 Patients. Maksymowych WP. et al.
• FOllow-up Research Cohort in AS (FORCAST)• 374 patients with AS from Northern Alberta• Mean FU of 3.1 years
ABSTRACT NUMBER: 975
Std Rx(n=147)
TNFi(n=227)

Nigil Haroon. University of Toronto
The Effect of TNF Inhibition on Radiographic Progression inAnkylosing Spondylitis: An Observational Cohort Study of
374 Patients. Maksymowych WP. et al.
ABSTRACT NUMBER: 975
Significant variables in multiple propensity analysis
Coefficient 95% CI p
Baseline mSASSS 0.018 0.003 – 0.032 0.015
Baseline ASDAS 0.24 0.031 – 0.45 0.024
Time between disease onset and anti-TNF start:
No anti-TNF Ref
<5 years -1.41 -2.56 – -0.25 0.017
5-10 years -0.34 -1.30 – 0.62 0.49
>10 years -0.17 -0.70 – 0.36 0.53
Maksymowych et al. ACR 2015

Nigil Haroon. University of Toronto
TNFi + High Dose NSAIDs decrease risk of progression in AS
Gensler L. et al. ACR 2016

Nigil Haroon. University of Toronto
Secukinumab Significantly Improves Signs and Symptoms of Active Ankylosing Spondylitis: 52-
Week Data From MEASURE 2, a Randomised, Double-Blind, Placebo-Controlled Phase 3 Trial With
Subcutaneous Loading and Maintenance Dosing
J. Sieper1, J. Braun2, X. Baraliakos2, D. Baeten3, M. Dougados4,
P. Emery5, A. Deodhar6, C. Wei7, B. Porter8, M. Andersson9,
S. Mpofu9, H. Richards9
1Charité University Medicine Berlin, Berlin, Germany; 2Rheumazentrum Ruhrgebiet, Herne, Germany; 3Academic Medical Centre, Amsterdam, The Netherlands; 4Université Paris René
Descartes and Hôpital Cochin, Paris, France; 5University of Leeds, Leeds, UK; 6Oregon Health & Science University, Portland, USA; 7Chung Shan Medical University Hospital,
Taichung, Taiwan; 8Novartis Pharmaceuticals Corporation, East Hanover, USA; 9Novartis Pharma AG, Basel, Switzerland
MED/COSas/0002

Nigil Haroon. University of Toronto
MEASURE 2: Study Design
Randomisation was stratified according to whether subjects were anti–TNF-naïve or had previous intolerance or inadequate response to anti-TNF therapy. BL, baseline; i.v., intravenous; q4wk, every 4 weeks; PBO, placebo; R, randomisation; s.c., subcutaneous; TNF, tumour necrosis factor; Wk, Week.- MED/COSas/0002
TreatmentLoading
PrimaryEndpoint
Secukinumab 75 mg s.c.Wk 4 and q4wk
Secukinumab75 mg s.c. BL, Wks 1, 2, 3
Secukinumab 150 mg s.c. Wk 4 and q4wk
Secukinumab150 mg s.c.BL, Wks 1, 2, 3
PBO s.c. BL, Wks1, 2, 3
PBO s.c. Wks 4, 8, 12
Secukinumab 150 mg s.c. Wk 16 and q4wk
Secukinumab 75 mg s.c. Wk 16 and q4wk
1 8 12 163 4Week 2BL
FinalInjection Wk 256
FinalAssessment/
Wk 260/Wk 268
R1:1:1
R1:1
46
N=72
N=73
N=74

Nigil Haroon. University of Toronto
Rapid Improvements in ASAS20 Response Through Week 16 (Primary Endpoint)
0 4 8 12 160
20
40
60
80
100
28.4%
41.1%
61.1%
Secukinumab 150 mg s.c. (N = 72) Secukinumab 75 mg s.c. (N= 73)Placebo (N = 74)
*
*
†
*P < 0.0001; †P < 0.001; §P < 0.01; ‡P < 0.05 versus placebo (P-values at week 16 were adjusted for multiplicity of testing); NRI data presented through Week 16.ASAS, Assessment of Spondyloarthritis International Society criteria; NRI, nonresponder imputation.- MED/COSas/0002
1 2 3
Per
cent
age
of R
espo
nder
s
§
‡
§
† †
‡
†
Weeks
†
47

Nigil Haroon. University of Toronto
ASAS20 Response in Anti–TNF-Naïve and Anti–TNF-IR Subjects at Weeks 16 and 52
†P < 0.001; ‡P < 0.05 vs. placebo at Week 16.ASAS, Assessment of Spondyloarthritis International Society criteria; s.c., subcutaneous; IR, inadequate response; TNF, Tumour necrosis factor.Anti–TNF-IR subjects had an inadequate response to, or intolerance of anti-TNF therapy. Missing data were imputed as non-responses through Week 16 (NRI, non-responder imputation); Week 52 data are as observed - MED/COSas/0002.
anti–TNF-naïve anti–TNF-IR0
20
40
60
80
100
68.2
50.051.1
2531.124.1
Secukinumab 150 mg s.c. Secukinumab 75 mg s.c. PlaceboP
erce
ntag
e of
Re-
spon
ders
‡
†
N = 44 N = 45 N = 45 N = 28 N = 28 N = 29
anti–TNF-naïve anti–TNF-IR0
20
40
60
80
10082.1
59.171.4
47.4
Per
cent
age
of
Res
pond
ers
N = 45
N=28 N=28
N = 44 N = 28 N = 28
At Week 16
At Week 52
48

Nigil Haroon. University of Toronto
Crohn’s Disease Worsening with Secukinumab
Nigil Haroon. University of Toronto
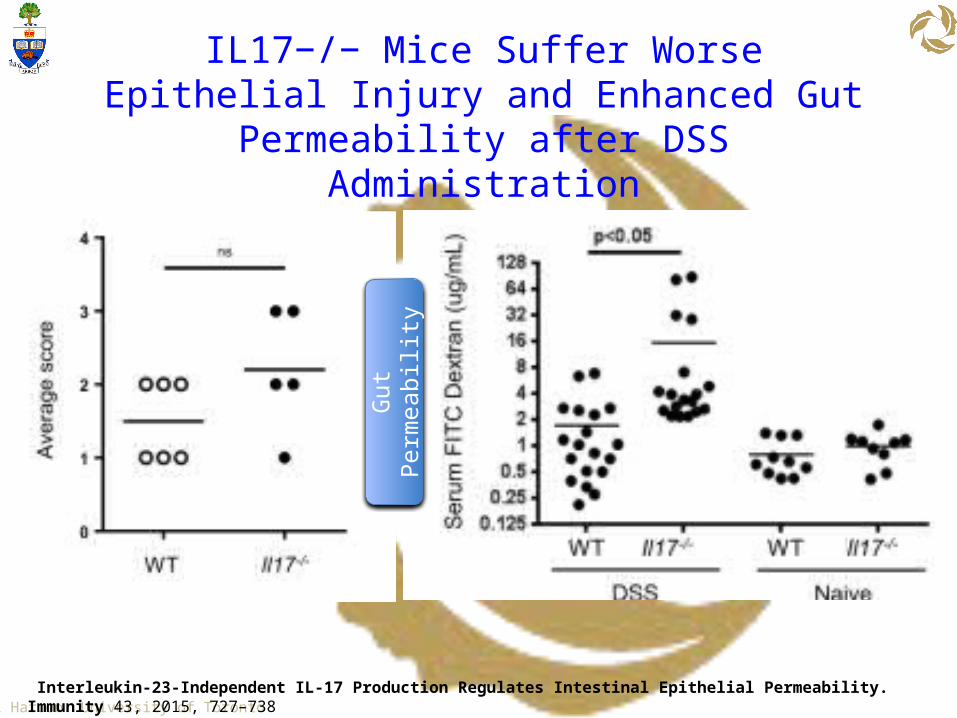
IL17−/− Mice Suffer Worse Epithelial Injury and Enhanced Gut Permeability after DSS
Administration
Interleukin-23-Independent IL-17 Production Regulates Intestinal Epithelial Permeability. Immunity 43, 2015, 727–738
Gut P
erm
eabi
lity

Nigil Haroon. University of TorontoImmunity 2008 28, 445-453DOI: (10.1016/j.immuni.2008.03.001)
Different Faces of Th17 Cells
Nigil Haroon. University of Toronto
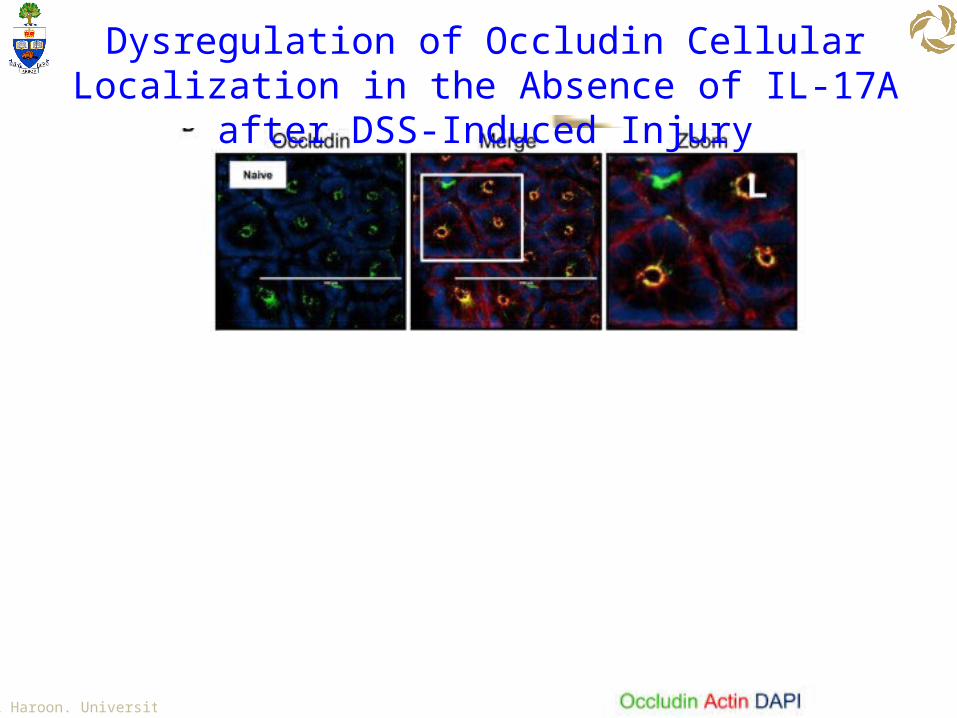
Dysregulation of Occludin Cellular Localization in the Absence of IL-17A after DSS-Induced Injury

Nigil Haroon. University of Toronto
No Increased Risk of IBD Among Secukinumab-Treated Patients with Pso, PsA or AS: Data from 14 Phase 2 and Phase 3 Clinical Studies. Atul
A. Deodhar et al.
ACR 2016: ABSTRACT NUMBER: 962

Nigil Haroon. University of Toronto
Secukinumab Phase II Study
Xenofon Baraliakos et al. Ann Rheum Dis 2015

Nigil Haroon. University of Toronto
Distribution of MRI inflammatory and fatty lesions in VEs in subjects (N=10) treated with secukinumab from core study baseline to week 94.
Xenofon Baraliakos et al. Ann Rheum Dis doi:10.1136/annrheumdis-2015-207544
©2015 by BMJ Publishing Group Ltd and European League Against Rheumatism
Nigil Haroon. University of Toronto
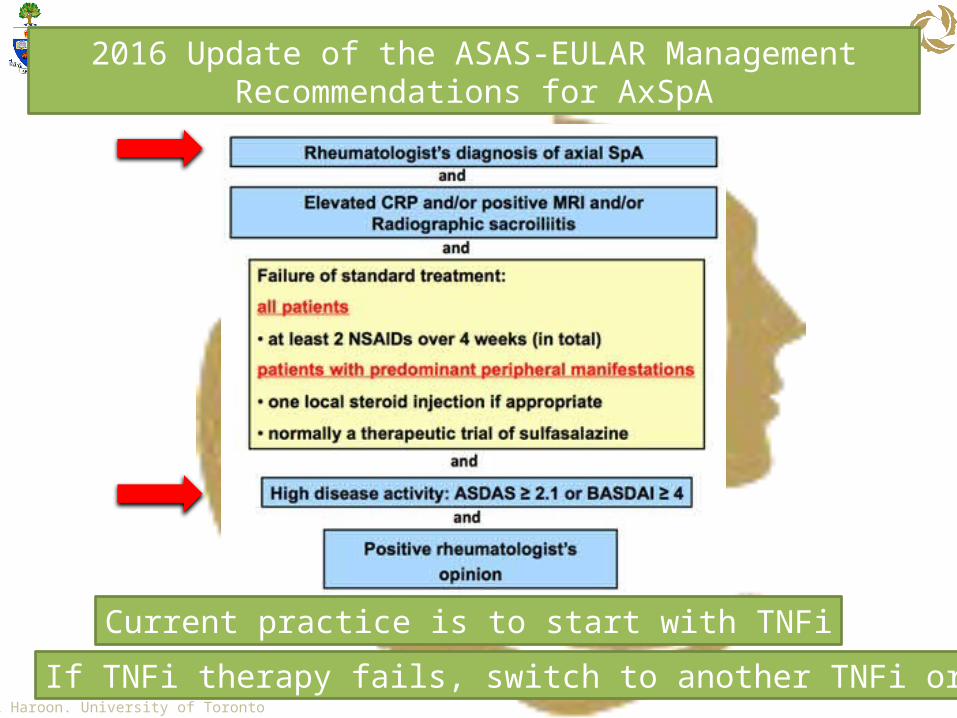
2016 Update of the ASAS-EULAR Management Recommendations for AxSpA
Current practice is to start with TNFi
If TNFi therapy fails, switch to another TNFi or IL-17i

Nigil Haroon. University of Toronto
Summary

Nigil Haroon. University of Toronto
The Team
Zhenbo Zhang
Kelly Thickett
Hasan Abdullah
Kirby Yee Matthew He Jano Muralitharan
Vidya Ranganathan
P Rahman D Philpott B WoutersMike Zeng
Archita Srinath





























