Embed Size (px)
Citation preview

Clinical Decision Support By Clinicians, For Clinicians
{S}caffold: A toolset for making it so
Jason Jones, PhD
Kaiser Permanente
• What is it and what was the problem?
• Technical framework
• New era of choices
Overview
• Fit decision support into workflow
• Speed ideation to deployment
• Creative control for clinicians and informaticists
• Advance technical (prediction & protocol) capability
Development Goals
Almost 90 year old very pleasant male with history of stroke presented with presyncope at 16:39. Felt like he was going to faint at church. Vital signs normal upon arrival. History of diarrhea 3 days ago. Initial labs normal except for WBC 13.5K. Patient felt well and wanted to leave. Advised him to stay for telemetry monitoring considering his age and prior medical history. He was transferred to our ED observation unit at 20:14.
Developed fever and altered mental status around 23:00. Hospitalist ordered lactate, blood and urine cultures, and gave a dose of ceftriaxone and azithromycin for presumed pneumonia. The internist, Dr Lu, informed me of what was happening. I
placed patient back on "My Patients" trackboard and saw the SIRS symbol which had not been there previously and the time when it started. I went over to our observation unit, ordered 3L intravenous fluid, and stayed at beside to ensure that
the nurses aggressively resuscitated the patient using pressure bags for fluid boluses. Patient started to develop some
tachypnea and crackles so I ordered a repeat chest x-ray ordered which showed pulmonary congestion and bipap was ordered.
Patient's mental status improved dramatically with the fluid and bipap and by the next morning he was off bipap. Lactate went from 4.9 to 2.9 mmol/L. He did not end up on vasopressors. His infection source ended up being urine. Length of stay was 3 days.
The SIRS symbol was helpful because it informed me that patient met SIRS criteria, and more importantly what time this occurred. With that knowledge, I knew I was within the time frame to initiate EGDT and aggressively resuscitate this patient. It would have been helpful to the nurses as well if they had this since they were the ones monitoring him in the observation unit. We had good nurses at that time, some other nurses may not have been as alert or aware.
A Patient Story (Mimi Lee, MD)
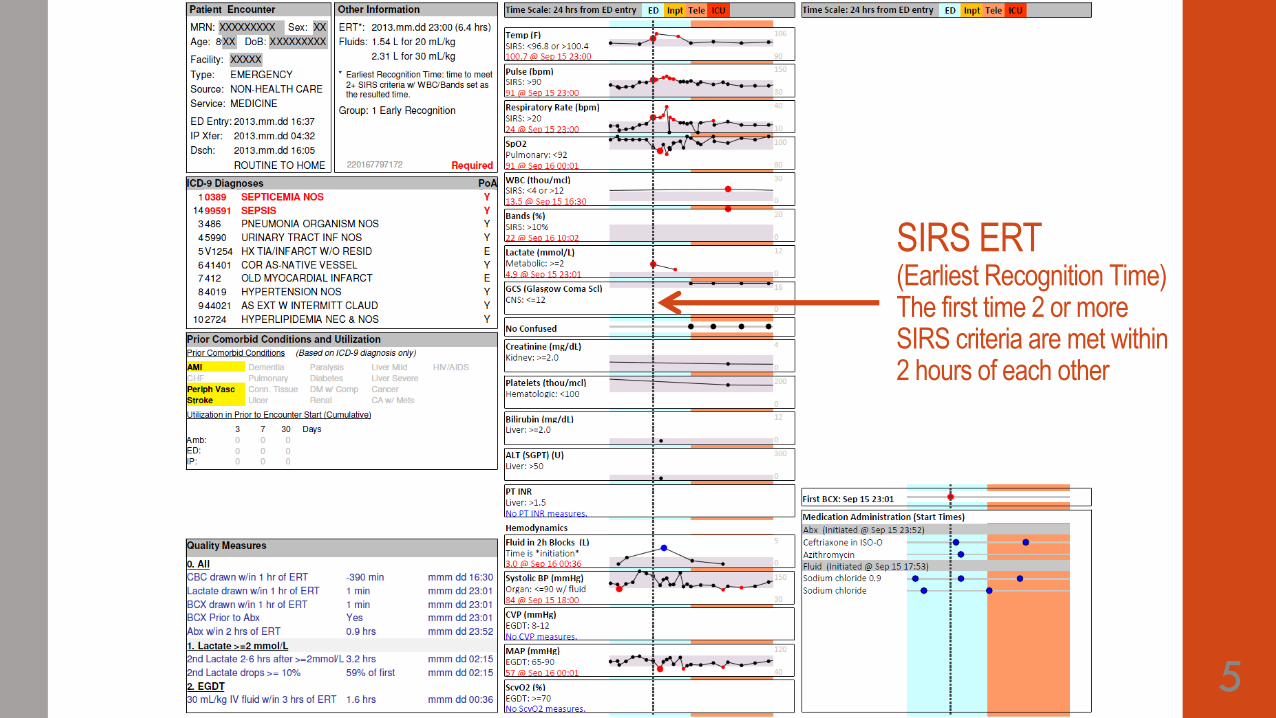
5
SIRS ERT (Earliest Recognition Time) The first time 2 or more SIRS criteria are met within 2 hours of each other
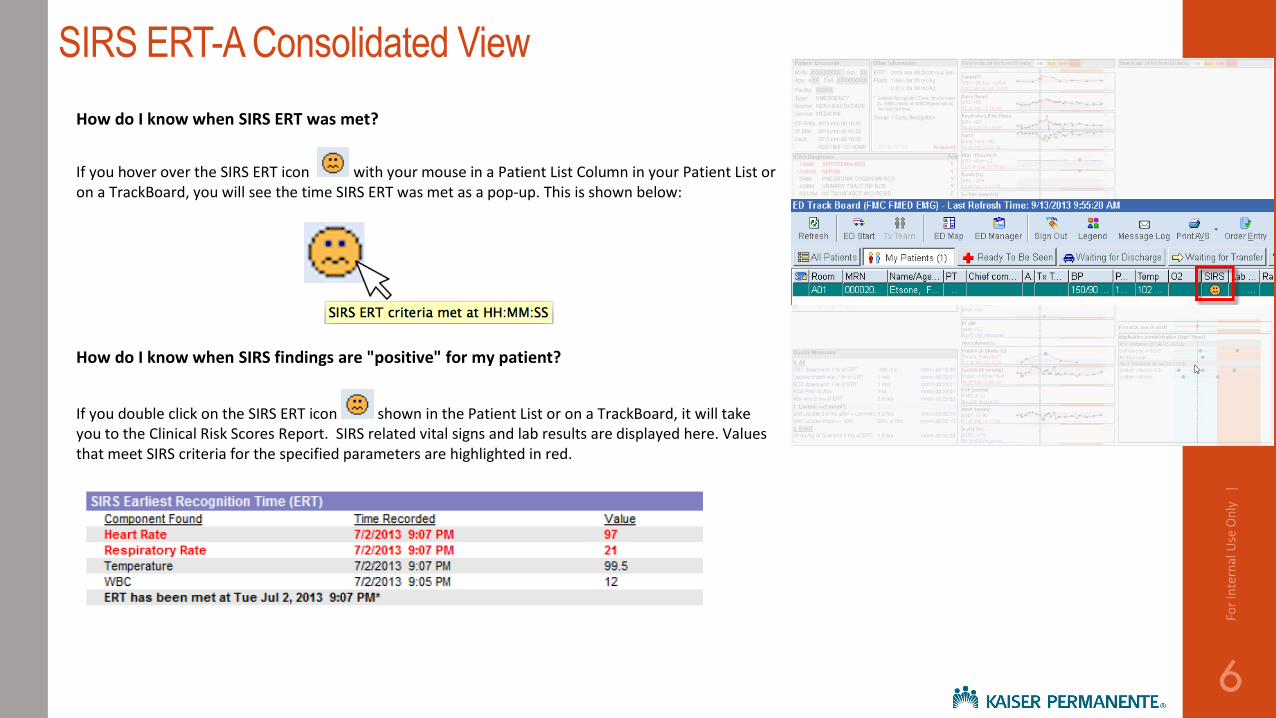
SIRS ERT-A Consolidated View
How do I know when SIRS ERT was met?
If you hover over the SIRS ERT icon with your mouse in a Patient List Column in your Patient List or on a TrackBoard, you will see the time SIRS ERT was met as a pop-up. This is shown below:
How do I know when SIRS findings are "positive" for my patient?
If you double click on the SIRS ERT icon shown in the Patient List or on a TrackBoard, it will take you to the Clinical Risk Scores Report. SIRS related vital signs and lab results are displayed here. Values that meet SIRS criteria for the specified parameters are highlighted in red.
6
For
Inte
rnal
Use
On
ly
|
7
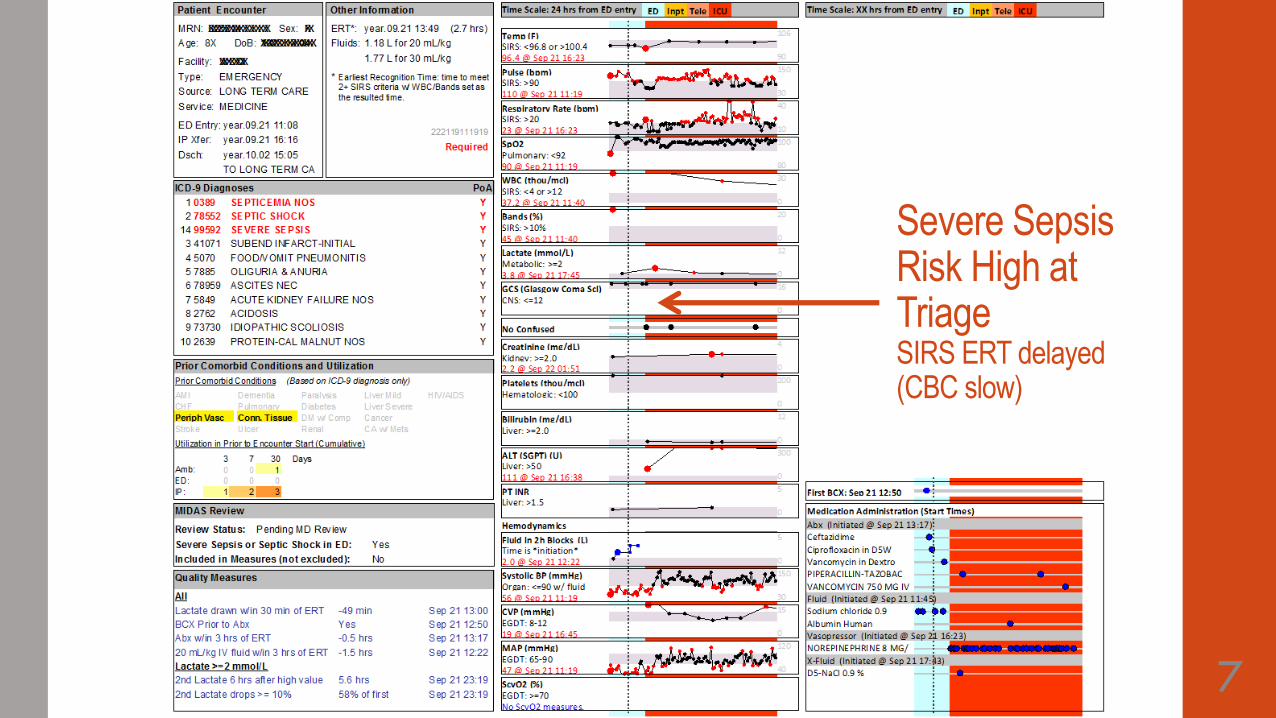
Severe Sepsis Risk High at Triage SIRS ERT delayed (CBC slow)
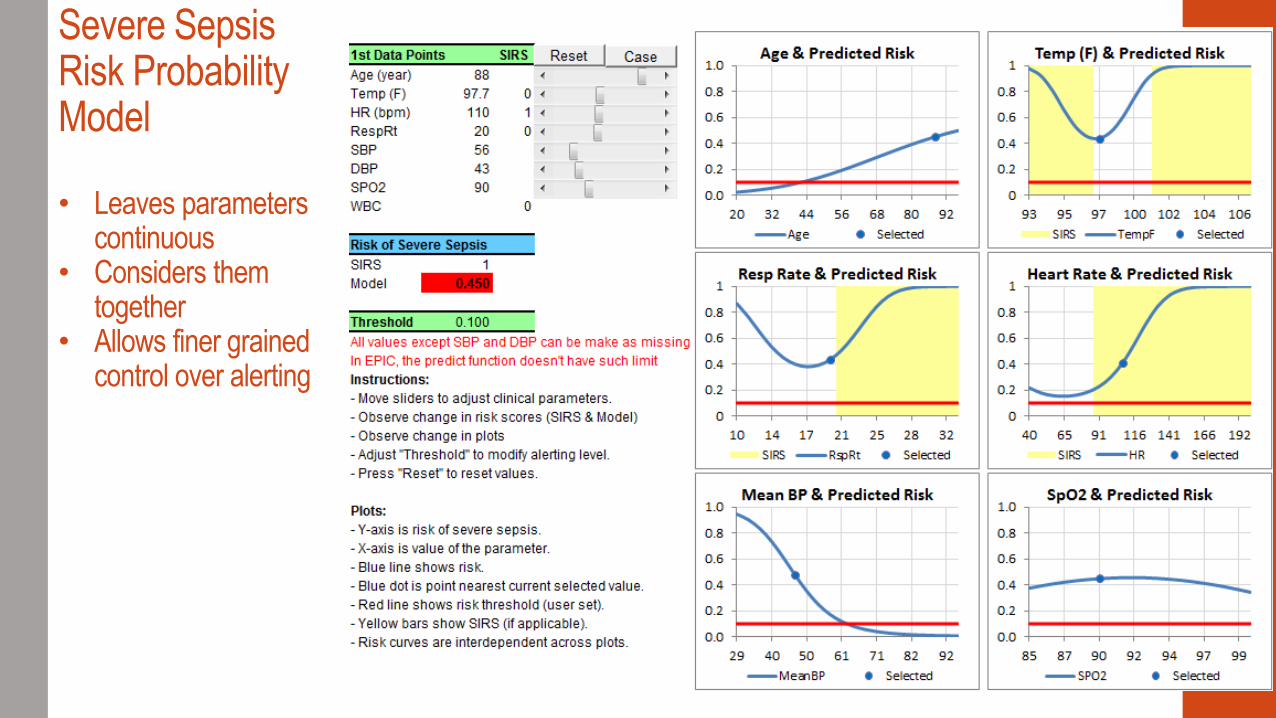
Severe Sepsis Risk Probability Model • Leaves parameters
continuous • Considers them
together • Allows finer grained
control over alerting
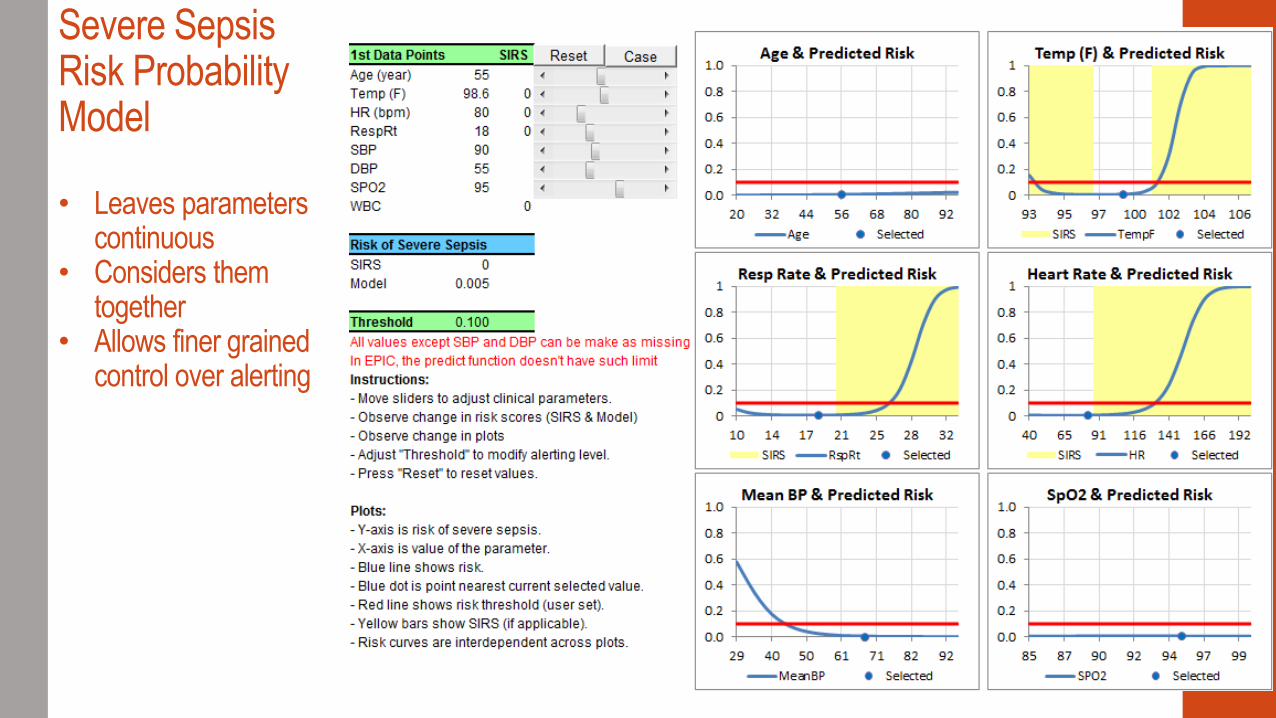
Severe Sepsis Risk Probability Model • Leaves parameters
continuous • Considers them
together • Allows finer grained
control over alerting
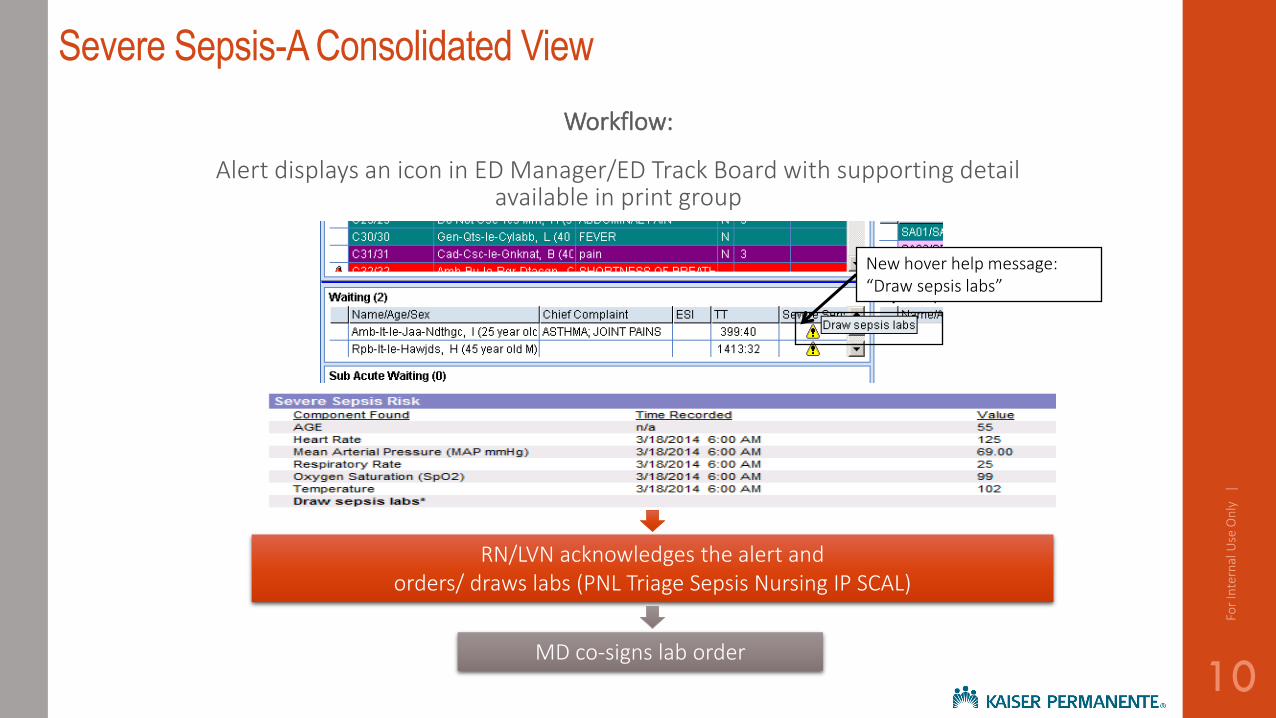
Severe Sepsis-A Consolidated View
Workflow:
Alert displays an icon in ED Manager/ED Track Board with supporting detail available in print group
RN/LVN acknowledges the alert and orders/ draws labs (PNL Triage Sepsis Nursing IP SCAL)
MD co-signs lab order
New hover help message: “Draw sepsis labs”
10
For
Inte
rnal
Use
On
ly
|
• What is it and what was the problem?
• Technical framework
• New era of choices
Overview
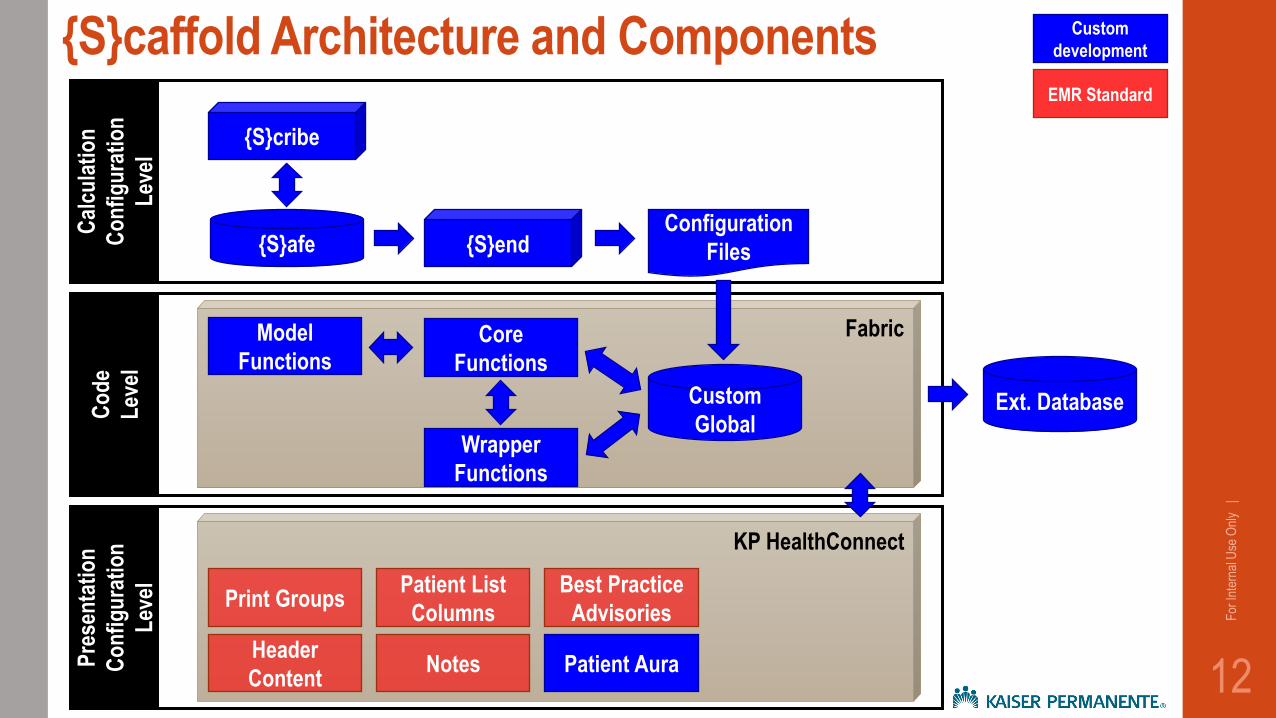
{S}caffold Architecture and Components
12
For
Inte
rnal
Use
Onl
y |
KP HealthConnect
Best Practice
Advisories
Patient List
Columns
Notes
Print Groups
Header
Content Patient Aura P
rese
nta
tio
n
Co
nfi
gu
rati
on
Lev
el
Fabric
Co
de
Lev
el
Model
Functions Core
Functions
Wrapper
Functions
Custom
Global
Cal
cula
tio
n
Co
nfi
gu
rati
on
Lev
el
{S}cribe
{S}end {S}afe Configuration
Files
Custom
development
EMR Standard
Ext. Database
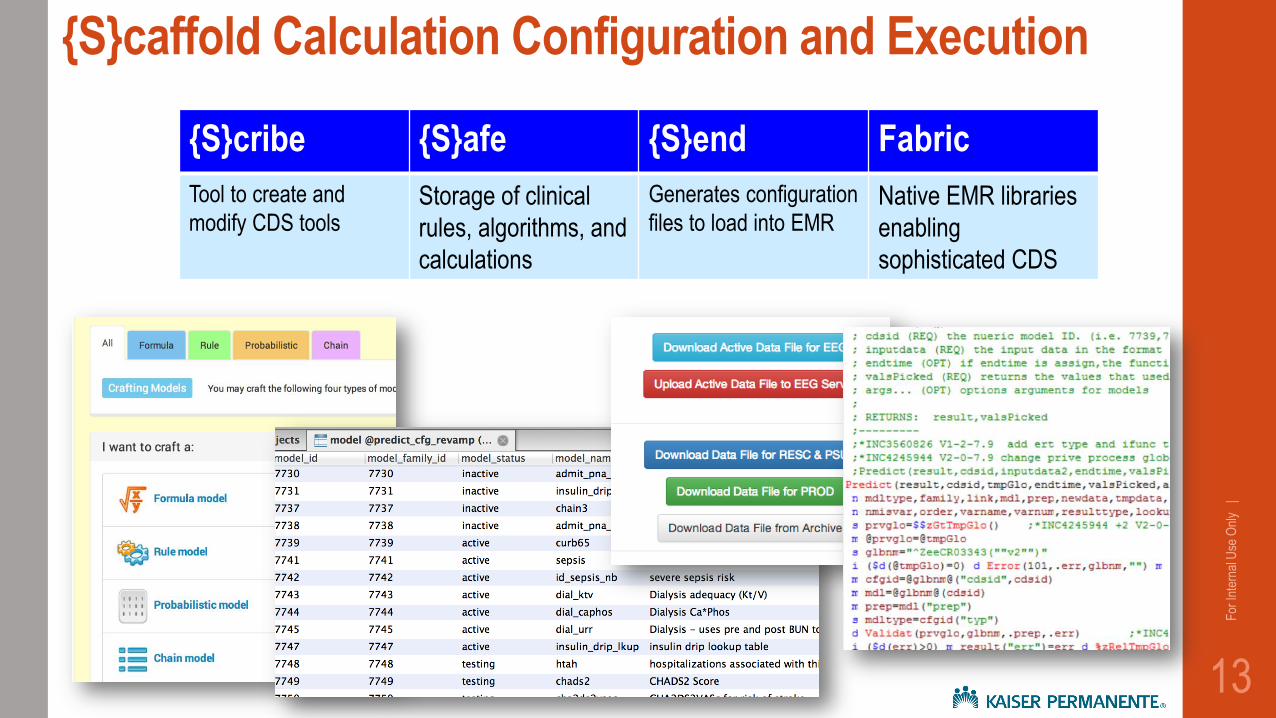
{S}cribe {S}afe {S}end Fabric
Tool to create and
modify CDS tools Storage of clinical
rules, algorithms, and
calculations
Generates configuration
files to load into EMR Native EMR libraries
enabling
sophisticated CDS
13
For
Inte
rnal
Use
Onl
y |
{S}caffold Calculation Configuration and Execution
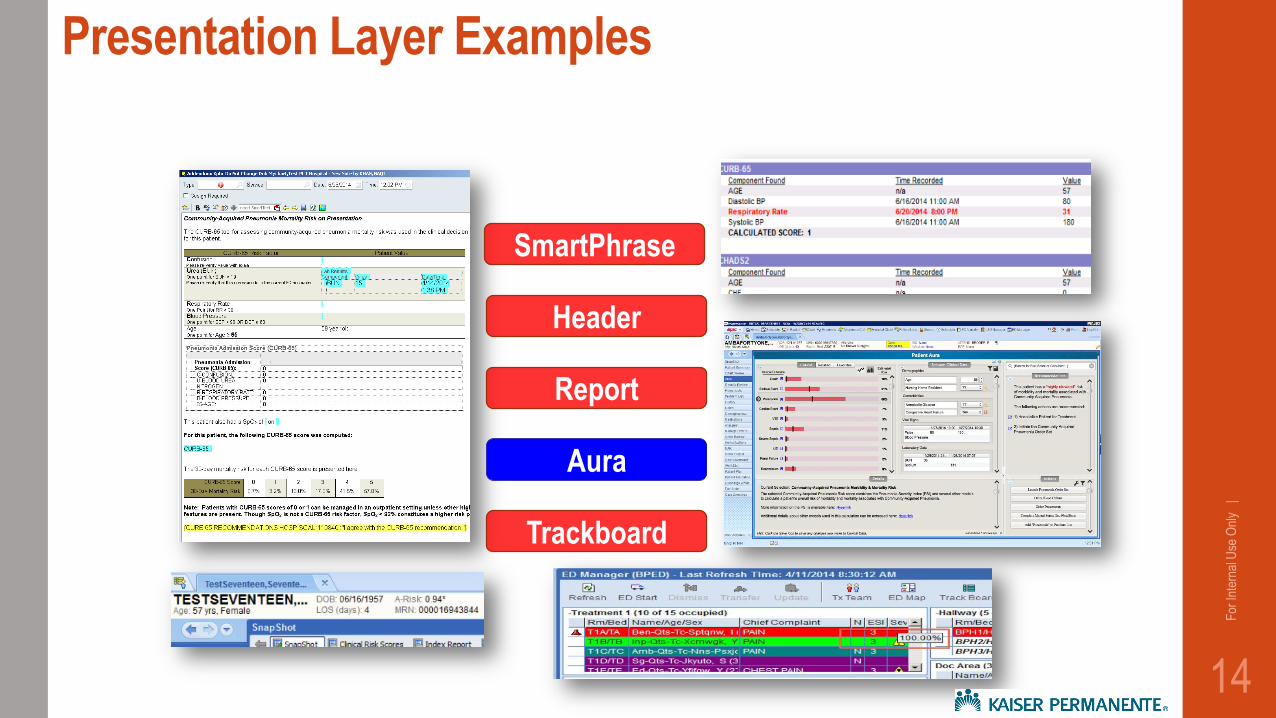
SmartPhrase
Header
Aura
Trackboard
Report
14
For
Inte
rnal
Use
Onl
y |
Presentation Layer Examples
15
For
Inte
rnal
Use
Onl
y |
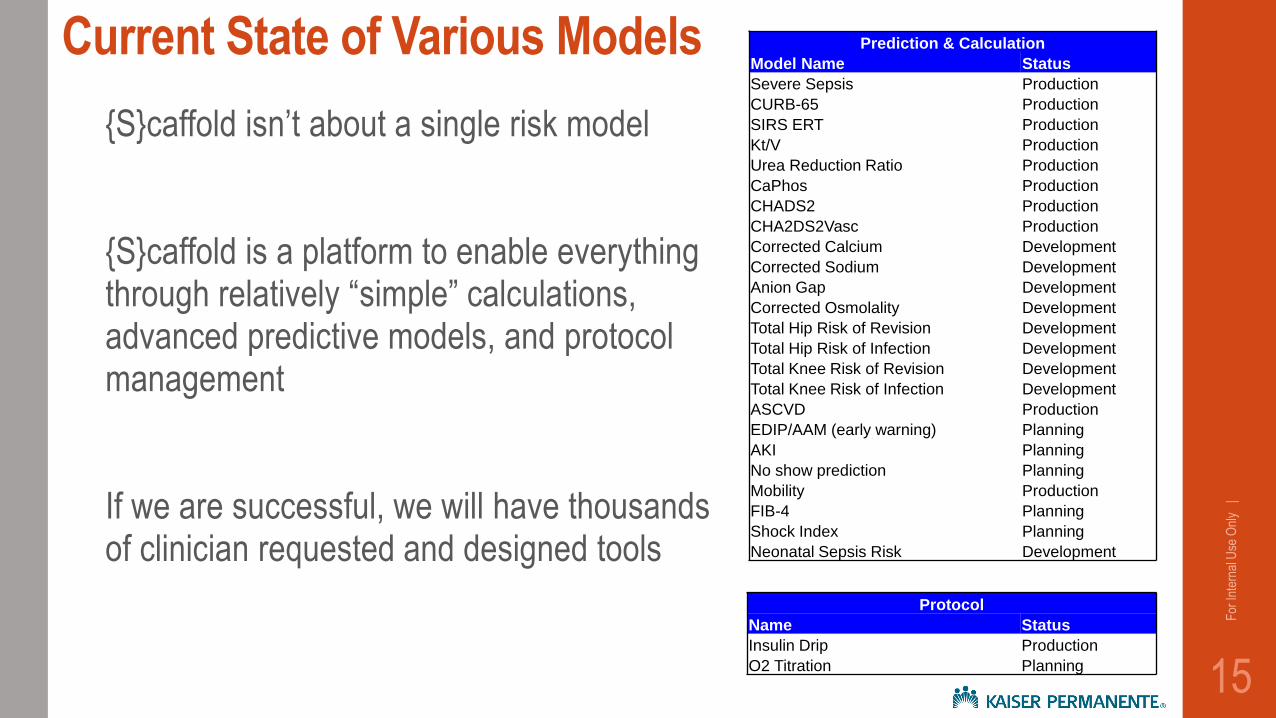
Current State of Various Models Prediction & Calculation
Model Name Status
Severe Sepsis Production
CURB-65 Production
SIRS ERT Production
Kt/V Production
Urea Reduction Ratio Production
CaPhos Production
CHADS2 Production
CHA2DS2Vasc Production
Corrected Calcium Development
Corrected Sodium Development
Anion Gap Development
Corrected Osmolality Development
Total Hip Risk of Revision Development
Total Hip Risk of Infection Development
Total Knee Risk of Revision Development
Total Knee Risk of Infection Development
ASCVD Production
EDIP/AAM (early warning) Planning
AKI Planning
No show prediction Planning
Mobility Production
FIB-4 Planning
Shock Index Planning
Neonatal Sepsis Risk Development
Protocol
Name Status
Insulin Drip Production
O2 Titration Planning
{S}caffold isn’t about a single risk model
{S}caffold is a platform to enable everything through relatively “simple” calculations, advanced predictive models, and protocol management
If we are successful, we will have thousands of clinician requested and designed tools
16
For
Inte
rnal
Use
Onl
y |
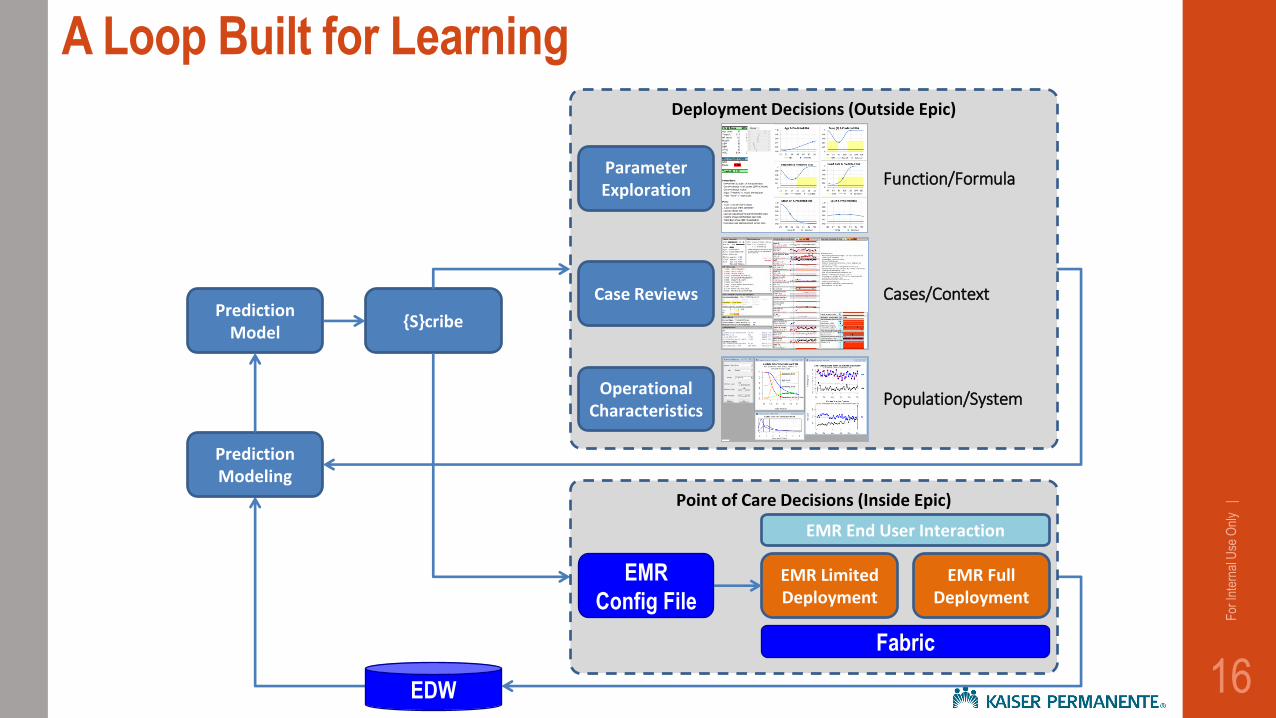
A Loop Built for Learning
Prediction Model
{S}cribe
Prediction Modeling
Point of Care Decisions (Inside Epic)
EMR
Config File
EMR Limited Deployment
EMR Full Deployment
Fabric
EMR End User Interaction
Deployment Decisions (Outside Epic)
Parameter Exploration
Function/Formula
Case Reviews Cases/Context
Operational Characteristics
Population/System
EDW
• What is it and what was the problem?
• Technical framework
• New era of choices
Overview
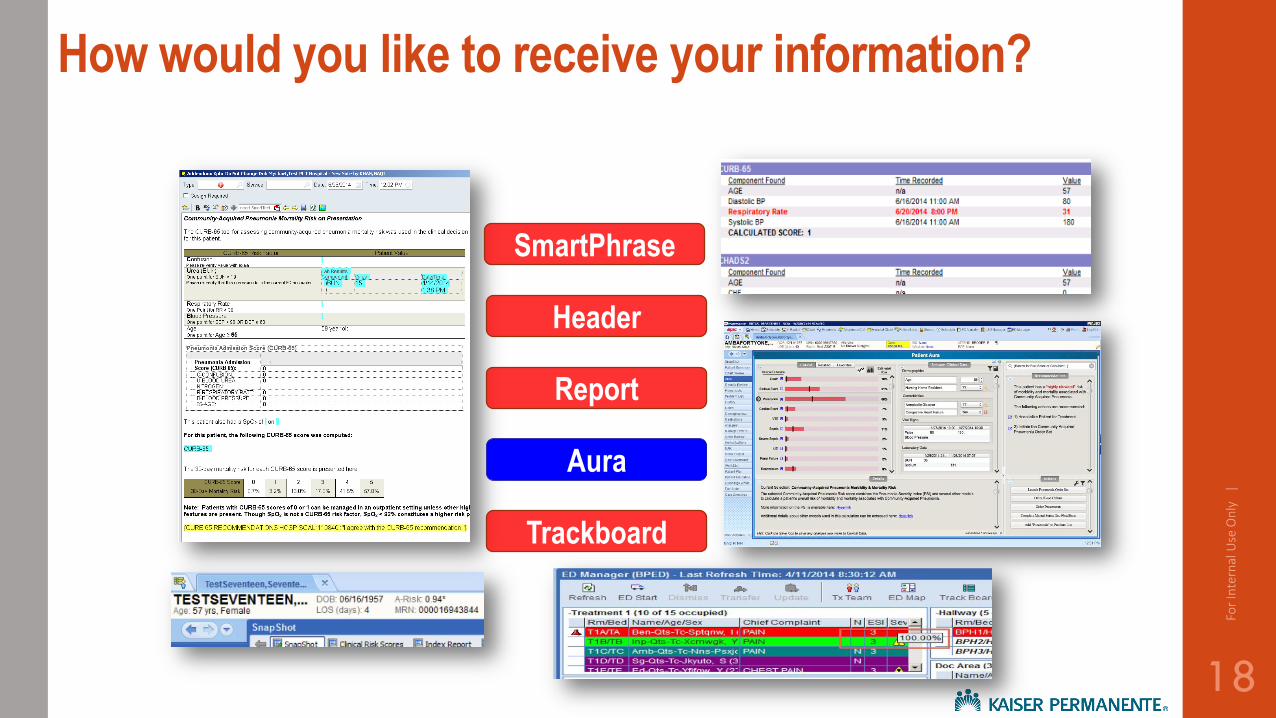
How would you like to receive your information?
18
For
Inte
rnal
Use
On
ly
|
SmartPhrase
Header
Aura
Trackboard
Report
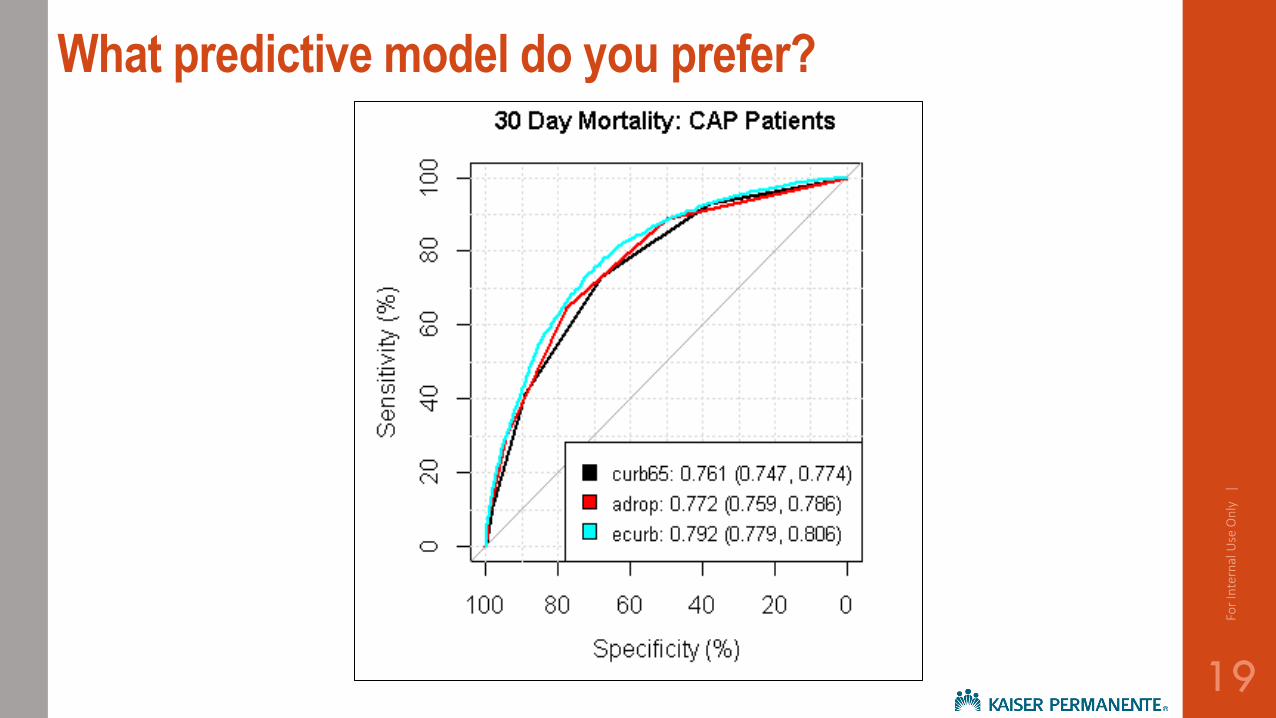
What predictive model do you prefer?
19
For
Inte
rnal
Use
On
ly
|
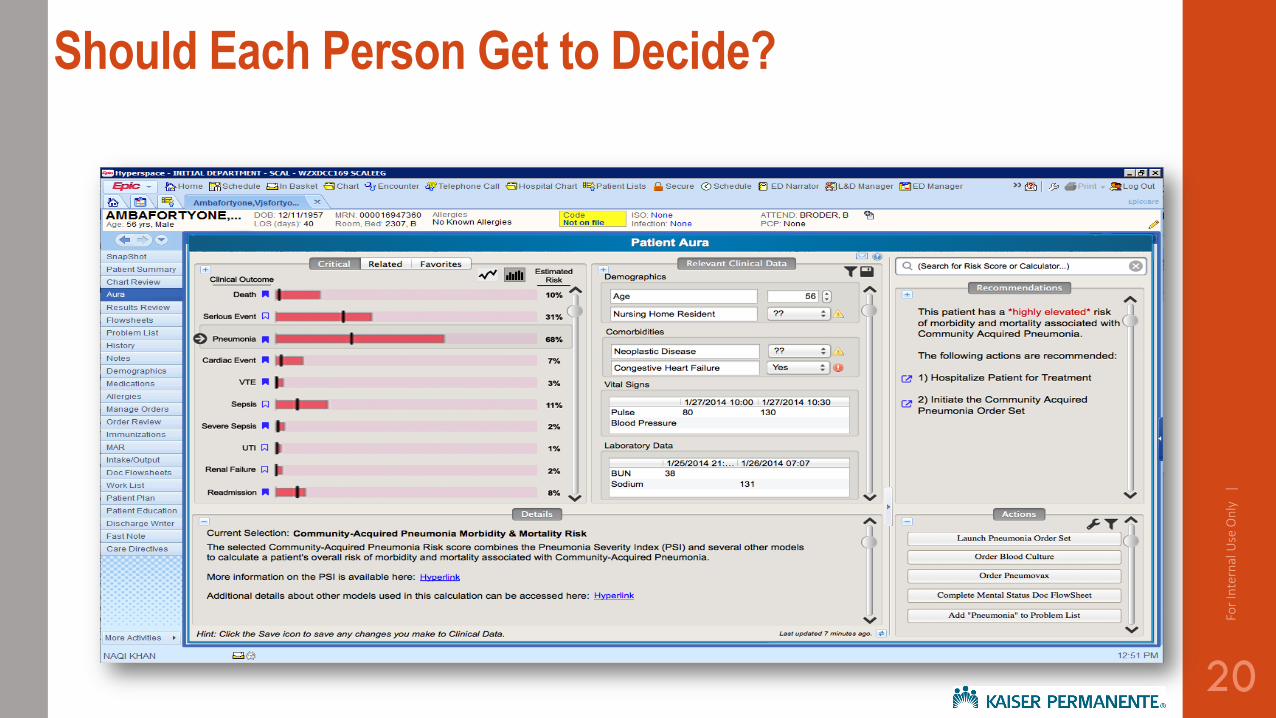
Should Each Person Get to Decide?
20
For
Inte
rnal
Use
On
ly
|
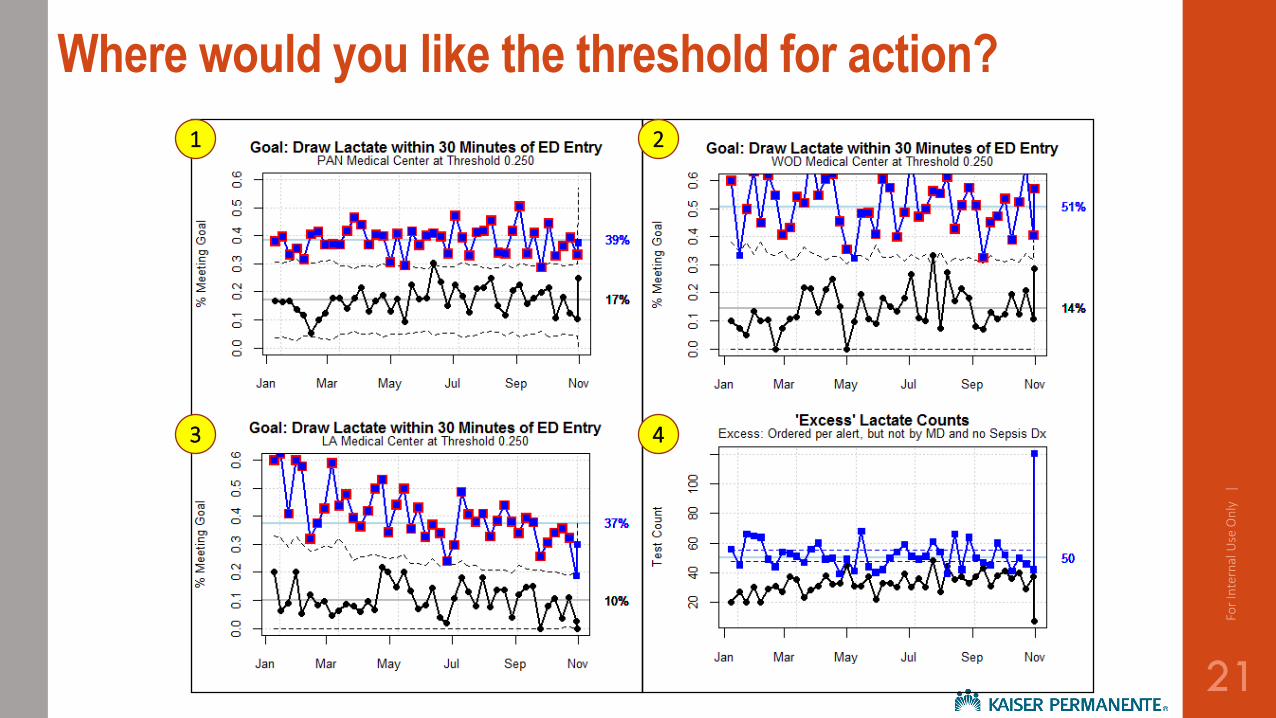
Where would you like the threshold for action?
21
For
Inte
rnal
Use
On
ly
|
1 2
3 4
Questions or Thoughts?
For
Inte
rnal
Use
On
ly
|
22





























