Embed Size (px)
Citation preview

HEPATOBLASTOMA AND BONE TUMOR

#
HEPATOBLASTOMA

#
DEFINITIONS
• Hepatoblastoma: A type of liver cancer that usually does not spread outside the liver. This type usually affects children younger than 3 years old.
• Hepatocellular carcinoma: A type of liver cancer that often spreads to other places in the body. This type usually affects children older than 14 years old.
#
Two less common types of childhood liver cancer are:
• Undifferentiated embryonal sarcoma of the liver (UESL): The third most common liver cancer in children and adolescents. It usually occurs in children between the ages of 5 and 10 years.

#
• Infantile choriocarcinoma of the liver: Choriocarcinoma of the liver is a very rare tumor that appears to originate in the placenta and presents with a liver mass in the first few months of life. Infants are often unstable due to hemorrhage of the tumor. Clinical diagnosis may be made without biopsy based on tumor imaging of the liver associated with extremely high serum beta-hCG levels and normal AFP levels for age.
#
ETIOLOGY• Although the exact cause of liver cancer
is unknown, there are a number of genetic conditions that are associated with an increased risk for developing hepatoblastoma. They include:
• Beckwith-Wiedemann syndrome: This syndrome is characterized by a combination of Wilms' tumor, kidney failure, genitourinary malformations and gonad (ovaries or testes) abnormalities.

#
INCIDENCE • primarily affects children from infancy to
about 5 years of age.
• Most cases appear during the first 18 months of life.
• Hepatoblastoma affects white children more frequently than black children, and is more common in boys than girls up to about age 5, when the gender difference disappears.
• It occurs more frequently in prematurely born with very low birth weights.

#
• Familial adenomatous polyposis: This is a group of rare inherited diseases of the gastrointestinal tract.
• Hemihypertrophy: This condition is the faster growth of one limb on one side of the body in comparison with the other side.
• Children who are exposed to hepatitis B infection at an early age, or those who have biliary atresia, are also at increased risk for developing liver cancer.

#
RISK FACTORS • Being male.
• Having the hepatitis B virus that was passed from mother to child at birth.
• Certain genetic changes linked with childhood hepatocellular carcinoma.
• Having one of the following conditions:– Biliary cirrhosis,Alagille syndrome, Glycogen
storage disease, Progressive familial intrahepatic disease, Tyrosinemia.

#
CLINICAL FEATURES
• The signs and symptoms of pediatric hepatoblastoma often depend on the size of the tumor and whether it has spread to other parts of the body.
#
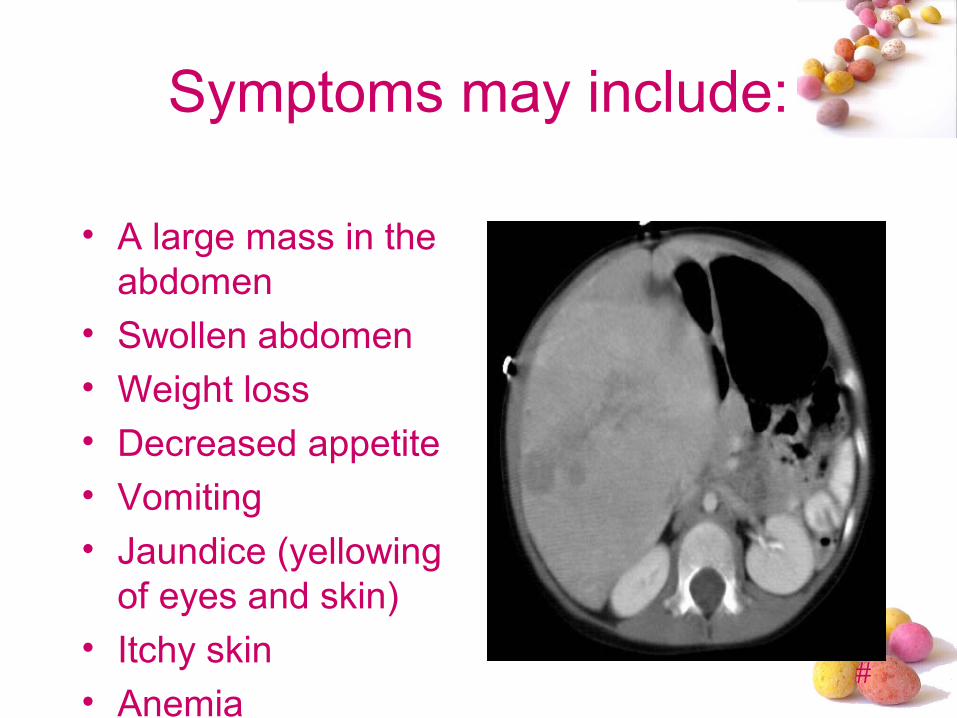
Symptoms may include:
• A large mass in the abdomen
• Swollen abdomen• Weight loss• Decreased appetite• Vomiting• Jaundice (yellowing
of eyes and skin)• Itchy skin• Anemia
#
Other Symptoms
• Fever
• Back pain
• Decreased urination

#
DIAGNOSTIC MEASURES
• Physical exam and history : An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient's health habits and past illnesses and treatments will also be taken.
#
• Alpha-fetoprotein (AFP) test. AFP levels in the blood can be used both to diagnose hepatoblastoma and to monitor its response to treatment.
• Computerized tomography scan (CT or CAT scan). It can show a mass in the liver and whether the cancer has spread to other organs such as the lungs.

#
• Magnetic resonance imaging (MRI). An MRI scan uses radio waves and strong magnets with computer technology. MRI shows more detailed images than CT and ultrasound and can help doctors see if the cancer has invaded one of the major blood vessels located near the liver.

#
• Complete blood count (CBC): The number of red blood cells, white
blood cells, and platelets.The amount of hemoglobin (the protein
that carries oxygen) in the red blood cells.
The portion of the blood sample made up of red blood cells

#
• Liver function tests : A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by the liver. A higher than normal amount of a substance can be a sign of liver damage or cancer.

#
• Biopsy. A biopsy (a sample of tissue that is removed and examined under a microscope) will help confirm the diagnosis and help plan treatment.
• Bone scan. This imaging test uses a special radioactive material that is injected into a vein. The substance collects in areas of diseased bone and is sensed by special cameras that pick up radioactivity.
#
• Abdominal x-ray : An x-ray of the organs in the abdomen. An x-ray is a type of energy beam that can go through the body onto film, making a picture of areas inside the body

#
• Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. The picture can be printed to be looked at later. In childhood liver cancer, an ultrasound exam of the abdomen is usually done.

#
• Hepatitis assay : A procedure in which a blood sample is checked for pieces of the hepatitis virus.
• Epstein-Barr virus (EBV) test: A blood test to check for antibodies to the EBV and DNA markers of the EBV. These are found in the blood of patients who have been infected with EBV.

#
STAGING • “Staging” is a process of testing and
analysis to determine how far the cancer has spread. Once doctors know the stage of the disease, they can choose the most effective way to treat it. Additional tests such as a CT scan, an MRI, an ultrasound, or even surgery may be required.There are two staging systems for childhood liver cancer: presurgical and postsurgical.
#
• Presurgical (before surgery) staging: The stage is based on where the tumor has spread within the four parts (sections) of the liver, as shown by imaging procedures such as MRI or CT. This staging system is called PRETEXT.
• Stage I: Cancer is found in one section of the liver. Three sections of the liver that are next to each other do not have cancer in them.
• Stage II: Cancer in one or two sections of the liver. Two sections are next to each other do not have cancer in them.

#
• Stage III: One of the following is true:– Cancer is found in three sections of the liver and one section does not have cancer.
– Cancer is found in two sections of the liver and two sections that are not next to each other do not have cancer in them.
• Stage IV: Cancer is found in all four sections of the liver.
#
• Postsurgical (after surgery) staging: The stage is based on the amount of tumor that remains after the patient has had surgery.
• Stage I: The tumor was in the liver only and all of the cancer was removed by surgery.
#
• Stage II The tumor was in the liver only and all of the cancer that can be seen without a microscope was removed by surgery. A small amount of cancer remains in the liver, but it can be seen only with a microscope, or the tumor cells may have spilled into the abdomen before surgery or during surgery.

#
• Stage III: One of the following is true:– The tumor cannot be removed by surgery.– Cancer that can be seen without a microscope remains after surgery.
– The cancer has spread to nearby lymph nodes.
• Stage IV: The cancer has spread to other parts of the body.
• Recurrent childhood liver cancer is cancer that was once treated but has now come back, either in the liver or in other parts of the body.

#
TREATMENT
• Chemotherapy
• Surgery
• Radiation therapy
• Percutaneous ethanol injection

#
Chemotherapy
• It is a key part of treatment for nearly all infants and children with hepatoblastoma. Chemotherapy is used to both shrink the primary liver tumor and to treat any hepatoblastoma that has escaped outside the liver. This is important for patients with all stages of the disease, because cancer cells might have traveled to other parts of the body

#
Surgery
• Doctors will operate to remove the cancer whenever possible. Chemotherapy may be given before surgery to shrink the tumor, or after surgery to destroy any remaining cancer cells.
• The different types of surgery performed are:• Cryosurgery: Also known as cryotherapy, this treatment uses an instrument, possibly guided by ultrasound, to freeze and destroy abnormal tissue, such as carcinoma in situ.

#
• Partial hepatectomy: The cancerous part of the liver is removed in this surgery. The part removed may be a wedge of tissue, an entire lobe, or a larger part of the liver, along with a small amount of normal tissue around it.

#
• Total hepatectomy and liver transplant: The entire liver is removed and replaced with a healthy liver from a donor in this surgery. A liver transplant may be possible when cancer has not spread beyond the liver and a donated liver can be found. If the patient has to wait for a donated liver, other treatment is given as needed.

#
• Resection of metastases: This is surgery to remove cancer that has spread outside of the liver, such as to nearby tissues, the lungs, or the brain.
#
Radiation therapy
• This treatment uses high-energy x-rays or other types of radiation to kill or stop cancer. The radiation may come from a machine, or it may come from a substance sealed in needles, seeds, wires, or catheters placed directly into the cancer.
#
Percutaneous ethanol injection
• A small needle is used to inject ethanol (alcohol) directly into a tumor to kill cancer cells for this treatment.

#
PROGNOSIS• There has been dramatic improvement in outcomes over the last 20 to 25 years, with overall survival rates reaching 70 percent.
• Survival is dependent upon staging at diagnosis.
• Patients with completely resected tumors have a greater than 85 percent chance of survival.
• For those with unresectable disease that responds to chemotherapy, survival rates are about 60 percent.

#
• The prognosis for an individual depends on the stage of the disease:
• Stage I and II: When tumors are located only in the liver and can be surgically removed at diagnosis, the published cure rate is greater than 85 percent when surgery and chemotherapy are used together.

#
• Stage III: When tumors are located only in the liver but cannot be surgically removed at diagnosis, the published cure rate is not as high, approximating 60 percent to 70 percent. The cure rate is higher if complete surgical removal of all tumors becomes possible. Anecdotally, the cure rate appears to be increasing for children with Stage III disease, at least in part due to increasing availability of liver transplantation as a surgical option.

#
• Stage IV: When tumors are located in several places in the body, the published cure rate is 20 percent to 30 percent using surgery and chemotherapy. There is preliminary evidence to suggest that the cure rate may be increasing for children with Stage IV disease, possibly due to more aggressive chemotherapy options and the increasing availability of liver transplantation.
#
NURSING MANAGEMENT
• Risk for Infection related to immunosuppression, chemotherapy, and presence of invasive lines
• Pain related to the abnormal growth of tissues and compression of the adjacent structures by the tumor

#
• Imbalanced Nutrition: Less Than Body Requirements related to inability to ingest or digest adequate quantities of food or absorb adequate nutrients
• Ineffective Management of Therapeutic Regimen related to complex therapy.
• Impaired Growth and Development related to serious illness.
• Fatigue related to disease state• Impaired Family Processes related to situational crisis

#
BONE TUMOR
#
• Osteosarcoma and Ewing's sarcoma are the most common malignancies of bone tissues in children. Osteosarcoma, the more common of the two types, usually presents in bones around the knee. Ewing's sarcoma may affect bones of the pelvis, thigh, upper arm, or ribs.

#
OSTEOSARCOMA

#
Definition
• Osteosarcoma is a type of cancer that produces immature bone. It is the most common type of cancer that arises in bones, and it is usually found at the end of long bones, often around the knee.

#
INCIDENCE• Most people diagnosed with osteosarcoma
are under the age of 25, and it is thought to occur more often in males than females.
• In children and young adults, osteosarcoma usually develops in areas where the bone is growing quickly, such as near the ends of the long bones

#
• Most tumors develop in the bones around the knee, either in the distal femur or the proximal tibia
• The proximal humerus is the next most common site.
• However, osteosarcoma can develop in any bone, including the bones of the pelvis (hips), shoulder, and jaw. This is especially true in older adults.
#
ETIOLOGYAND RISK FACTORS
• The exact cause of osteosarcoma is unknown. However, a number of risk factors are apparent, as follows…
• Rapid bone growth: Rapid bone growth appears to predispose persons to osteosarcoma, as suggested by the increased incidence during the adolescent growth spurt , and osteosarcoma's typical location in the metaphyseal area adjacent to the growth plate (physis) of long bones.

#
• Environmental factors: The only known environmental risk factor is exposure to radiation. Radiation-induced osteosarcoma is a form of secondary osteosarcoma
• Genetic predisposition : Bone dysplasias, including Paget disease, fibrous dysplasia, enchondromatosis, and hereditary multiple exostoses and retinoblastoma (germ-line form) are risk factors.
#
• Osteosarcoma tends to occur in the bones of the:
• Shin (near the knee)
• Thigh (near the knee)
• Upper arm (near the shoulder)
• Osteosarcoma occurs most commonly in large bones in the area of bone with the fastest growth rate. However, it can occur in any bone.
#
TYPES OF OSTEOSARCOMA
• Several subtypes of osteosarcoma can be identified by how they look on x-rays and under the microscope. Some of these subtypes have a better prognosis (outlook) than others.
• Based on how they look under the microscope, osteosarcomas can be classified as high grade, intermediate grade, or low grade.

#
• High-grade osteosarcomas: These are the fastest growing types of osteosarcoma. When seen under a microscope, they do not look like normal bone and have many cells in the process of dividing into new cells. Most osteosarcomas that occur in children and teens are high grade.

#
There are many types of high-grade osteosarcomas :
• Osteoblastic
• Chondroblastic
• Fibroblastic
• Mixed
• Small cell
• Telangiectatic
• High-grade surface (juxtacortical high grade)

#
• Other high-grade osteosarcomas include:
• Pagetoid: a tumor that develops in someone with Paget disease of the bone
• Extra-skeletal: a tumor that starts in a part of the body other than a bone
• Post-radiation: a tumor that starts in a bone that had once received radiation therapy

#
• Intermediate-grade osteosarcomas: These uncommon tumors fall in between high-grade and low-grade osteosarcomas.
• Periosteal (juxtacortical intermediate grade)

#
• Low-grade osteosarcomas: These are the slowest growing osteosarcomas. The tumors look more like normal bone and have few dividing cells when seen under a microscope.
• Parosteal (juxtacortical low grade)
• Intramedullary or intraosseous well differentiated (low-grade central)

#
SIGNS AND SYMPTOMS
• Bone fracture (may occur after a routine movement)
• Bone pain• Limitation of motion• Limping (if the tumor is in the leg)• Pain when lifting (if the tumor is in the
arm)• Tenderness, swelling, or redness at the
site of the tumor

#
STAGINGMusculoskeletal Tumor Society (MSTS) Staging
System
• One system commonly used to stage osteosarcoma is the MSTS system, also known as the ENNEKING system. It is based on 3 key pieces of information:
• The grade of the tumor (G)• The extent of the main (primary) tumor (T)• If the tumor has metastasized (spread) to
nearby lymph nodes (bean-sized collections of immune system cells) or other organs (M)

#
Stage Grade Tumor Metastasis
IA G1 T1 M0
IB G1 T2 M0
IIA G2 T1 M0
IIB G2 T2 M0
III G1 / G2 T1 / T2 M1

#
• In summary:• Low-grade, localized tumors are stage
I.• High-grade, localized tumors are stage
II.• Metastatic tumors (regardless of grade)
are stage III.
#
DIAGNOSTIC MEASURES
• Physical exam and history
• X-ray
• CT scan (CAT scan):
• MRI (magnetic resonance imaging)
• Biopsy: Core biopsy , Incisional biopsy
• Light and electron microscopy
#
TREATMENT• Treatment of osteosarcoma in children
includes chemotherapy (the use of medical drugs to kill cancer cells and shrink the cancer) followed by surgery (to remove cancerous cells or tumors) and then more chemo (to kill any remaining cancer cells and minimize chances of the cancer coming back).
• Surgery often can effectively remove bone cancer, while chemotherapy can help eliminate remaining cancer cells in the body.

#
Surgical Treatment
• Surgical treatments for osteosarcoma consist of either amputation or limb-salvage surgery.
• Limb-salvage surgery- the affected bone and muscle are removed, leaving a gap in the bone that is filled by either a bone graft or more often a special metal prosthesis.

#
• The risk of infection and fracture is higher with bank bone replacement and therefore metal prostheses are more commonly used for reconstruction of the bone after removal of the tumor.

#
Amputation
• If the cancer has spread to the nerves and blood vessels surrounding the original tumor on the bone, amputation is often the only choice.
• When osteosarcoma has spread to the lungs or elsewhere, surgery might be done to remove tumors in these distant locations.

#
Chemotherapy• Chemotherapy is usually given both before
and after surgery. It eliminates small pockets of cancer cells in the body, even those too small to appear on medical scans.
• A child or teen with osteosarcoma is given the chemotherapy drugs intravenously or orally.

#
EWING'S SARCOMA

#
• Ewing’s sarcoma (ES) was first described by James Ewing in 1921 as a "diffuse endothelioma of bone" (Ewing 1921).
• Ewing sarcoma is a malignant (cancerous) bone tumor that affects children.

#
INCIDENCE
• Ewing sarcoma is the second most common type of bone cancer in children, but it is very rare. About 200 children and young adults are found to have Ewing sarcoma each year in the United States.
• About half of all Ewing sarcoma tumors occur in children and young adults between ages 10 and 20.

#
• This type of cancer is rarely found in African-Americans and Asian-Americans.
• It affects slightly more boys than girls.
• It does not appear to be inherited (passed down in families).
• Although not often seen, Ewing sarcoma can occur as a second cancer, especially in patients treated with radiation therapy.

#
CAUSES
• The exact causes of primary bone cancer are unknown.
• The development of Ewing’s sarcoma may be related in some way to times of rapid bone growth
• Genetic exchange -- Most cases of Ewing's sarcoma (85%) are the result of a translocation between chromosomes 11 and 22.

#
CLINICAL FEATURES
• Swelling and soreness around the tumor area
• A low fever that at first may seem to be caused by an infection
• Bone pain, especially pain that worsens during exercise or at night
• Limping, which is caused by a tumor on a leg bone
#
DIAGNOSTIC MEASURES
• A variety of tests and investigations are needed to diagnose Ewing’s sarcoma, including:
A physical exam and medical historyX-rays to locate and identify a potential
bone tumor, and chest x rayMagnetic resonance imaging (MRI) scanComputed tomography (CT or CAT) scan
#
• Bone scan, which uses an injected radioactive material and a special camera to identify potential spots in the skeleton where the cancer may have spread
• Positron emission tomography (PET) scan, which also uses a radioactive material and special camera to identify other spots in the body that may have a tumor
• Biopsy of the tumor

#
TREATMENT MEASURES
• A combination of various treatments is used to treat Ewing's sarcoma. Treatment will depend on a number of factors, including the size and position of the tumour. These include chemotherapy, surgery and radiotherapy.

#
Chemotherapy
• They are often given before surgery and continued afterwards in order to destroy any remaining cancer cells and prevent the sarcoma from spreading. Chemotherapy given in this way is called adjuvant chemotherapy.

#
Surgery
• Amputation
• Limb-sparing surgery
• replacing the bone with a prosthesis (a specially designed artificial part)
• replacing the bone with bone taken from another part of the body (a bone graft).

#
Radiotherapy
• External radiation uses machines outside the body to deliver the X-ray dose.
• Internal radiation uses needles, seeds, wires or catheters (tubes) to deliver the radiation directly into or close to the cancer.

#
SIDE EFFECTS OF TREATMENT
• Side effects can include:
• feeling sick (nausea) and being sick vomiting
• hair loss
• increased risk of infection
• bruising and bleeding
• tiredness
• diarrhea

#
NURSING MANAGEMENT
• Nursing Assessment
• Nursing Diagnoses• Nursing Interventions
• Evaluation

#

#
Sample Graph (3 colours)
0
10
20
30
40
50
60
70
80
90
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
East
West
North

#
Picture slide
• Bullet 1• Bullet 2
#
Examples of default styles
• Text and lines are like this
• Hyperlinks like this• Visited hyperlinks
like this
Table
Text box Text boxWith shadow
Text boxWith shadow

#
Colour scheme
BackgroundText &Lines
ShadowsTitleText
Fills AccentAccent &Hyperlink
FollowedHyperlink

#
Use of templatesYou are free to use these templates for your personal and business presentations.
Do Use these templates for your
presentations Display your presentation on a web
site provided that it is not for the purpose of downloading the template.
If you like these templates, we would always appreciate a link back to our website. Many thanks.
Don’t Resell or distribute these templates Put these templates on a website for
download. This includes uploading them onto file sharing networks like Slideshare, Myspace, Facebook, bit torrent etc
Pass off any of our created content as your own work
You can find many more free templates on the Presentation Magazine website www.presentationmagazine.com
We have put a lot of work into developing all these templates and retain the copyright in them. They are not Open Source templates. You can use them freely providing that you do not redistribute or sell them.