Embed Size (px)
Citation preview

BONE REGENERATION IN DEFECTS COMPROMISED BY RADIOTHERAPY
W. W. HU, B.B. WARD, Z. WANG, AND P.H. KREBSBACHJ DENT RES 89(1):77-81, 2010
Summarized by: Majd Hasanin

W. W. Hu, B.B. Ward, Z. Wang, and P.H. KrebsbachJ Dent Res 89(1):77-81, 2010
INTRODUCTIONAND BACKGROUND

Radiotherapy
Radiotherapy is commonly used as primary treatment and as an adjuvant to the surgical excision of oral squamous cell cancer in the head and neck.
3
Radiotherapy – Effect on Tissues
1. Damage to normal epithelial, dermal, and endothelial cells
2. Hypocellular and hypoxic environment leads to scarring and fibrosis
3. Osteoradionecrosis4. Difficulty in making secondary reconstruction of the
surgical site5. Require the removal of large amounts of bone in a
previously irradiated field
4
Tissue Engineering
¨ The regeneration of new tissues through the recapitulation of key events that occur during tissue formation and growth
¨ A multidisciplinary field still in relative infancy but with great potential to significantly impact patient care
Nussenbaum B et. al. 2005
5

¨ Tissue engineering was initially introduced to describe the technology for producing tissue in vitroLanger R et al. Tissue Engineering. Science 1993
¨ Recently, regenerative medicine is used to describe technology and surgical procedures for regeneration of tissue in vivo
Tissue Engineering6
¨ Tissue-engineering approaches are being developed to regenerate large skeletal defects§ Delivery of cell-signaling factors such as growth factors
or genes from biomaterial scaffolds
¨ Potential advantages to these approaches include the possibility of mirroring normal form and function of original tissues
Tissue Engineering7

Allografts:¨ Calcified freeze dried bone¨ Decalcified freeze dried bone
Alloplasts:¨ Hydroxyapatite, Dense hydroxyapetite, Porous
hydroxyapetite, Resorbable hydroxyapetite¨ Calcium Phosphate, Tricalcium phosphate ¨ Bioactive glass ( Silicon dioxide, calcium oxide, sodium
oxidase, phosphorous pentoxide)¨ Coral derived calcium carbonate
Xenografts:¨ Bovine mineral matrix¨ Bovine -derived
hydroxyapatite
Biomaterial's used in hard tissue engineering 8

Polymers:¨ Collagen¨ Poly
(lactide,coglycolide) ¨ Methylcellulose ¨ Hyaluronic acide ester¨ Chitosan¨ Propylene glycol
alginate
Composite and nanocomposite:¨ PLLA/ HAP¨ PLGA/ HAP
Biomaterial's used in hard tissue engineering 9

1- Natural:¨ Naturally occurring polymers, e.g. Hydrogels; such as
gelatin, agar, collagen, elastin, and fibrin; hyaluronic acid, chitosan/chitin, and alginate
¨ Naturally occurring ceramics, e.g. coral
2- Synthetic:¨ Synthetic bioresorbable polymers, e.g. PGLA,
polycaprolactone (PCL)¨ Porous ceramics, e.g. bioglass and calcium phosphate
structures
Scaffold materials10
1. Are extracellular matrix proteins of different tissues providing a scaffold for cellular support in body.
2. Excellent biocompatibility3. High affinity to and compatibility with the other
matrix proteins
Natural-derived polymers 11

1. A thermal-denatured collagen2. Made of bovine or porcine skin, bone or tendon3. Prepared either by acidic (type A) or alkaline (type B)
treatments (extraction)4. Flexibility in shape5. Biocompatibility6. Affinity to proteins7. Biodegradability8. Excellent candidates for bone graft scaffolds in low-
load areas or as drug delivery materials
Rohanizadeh et al. J Mater Sci: Mater Med (2008) 19:1173–82
Gelatin12
Tissue-engineering approach to the regeneration of bone involves the delivery of cell-signaling factors such as:
1- Growth factors:¨ Such as VEGF, TGF-β1, and BMPs have been delivered to
defects and have significantly improved bone repair in irradiated sites
¨ Did not demonstrate complete regeneration of critical-sized defects
¨ Extremely expensive
13

2- Gene Therapy:
¨ Commonly used in reference to any clinical application of the transfer of a foreign gene
¨ Defined as the correction of a disease phenotype through introduction of new genetic information into the affected organism
¨ Not limited to genetic diseases; in fact most involve acquired diseases (cancer and others)
Tissue-engineering approach to the regeneration of bone involves the delivery of cell-signaling factors such as:
14

Methods of Gene Transfer
Viral methods:
¨ Generally more efficient
¨ consider the tissue target, desired stability of gene expression, size of the gene that is to be transferred
Non-viral or physical methods:
¨ Safer, but less efficient¨ Uses liposomes or
other polymer, or other stimulus-such as sonication or electroporation
15
The principle vectors in clinical use are based on modified adenoviruses, retroviruses and adeno-associated viruses.
An ideal vector: should be targeted to specific cells - express the transgene product at a therapeutic level and under tight regulation for the required amount of time - show essential no toxicity. To be administered with minimal invasiveness
Different vectors will be needed for different clinical applications.
Vectors16
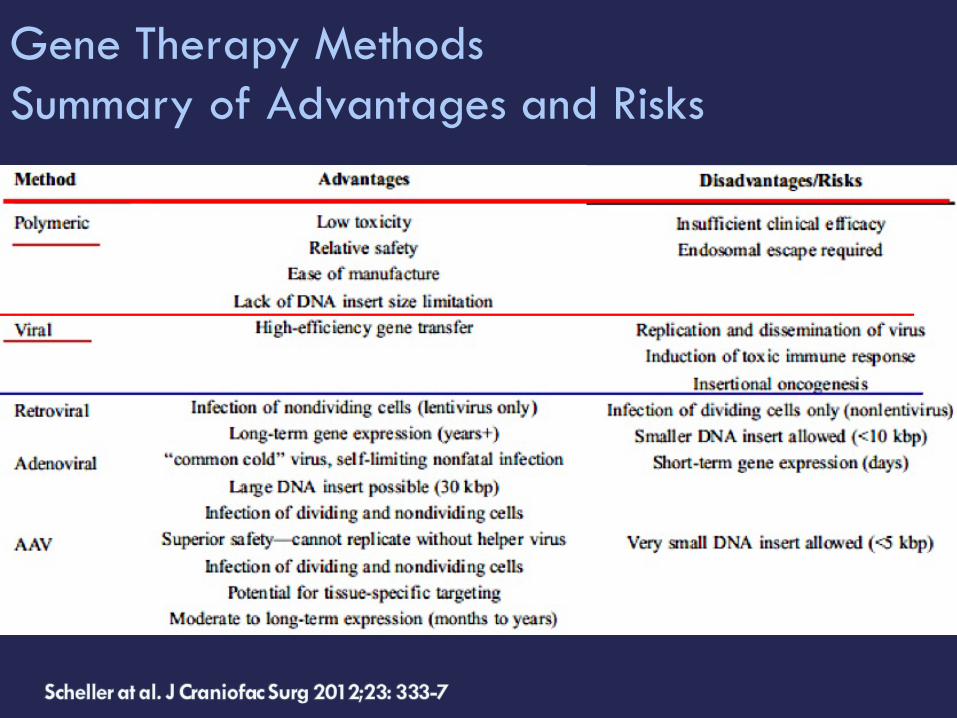
Gene Therapy MethodsSummary of Advantages and Risks
17

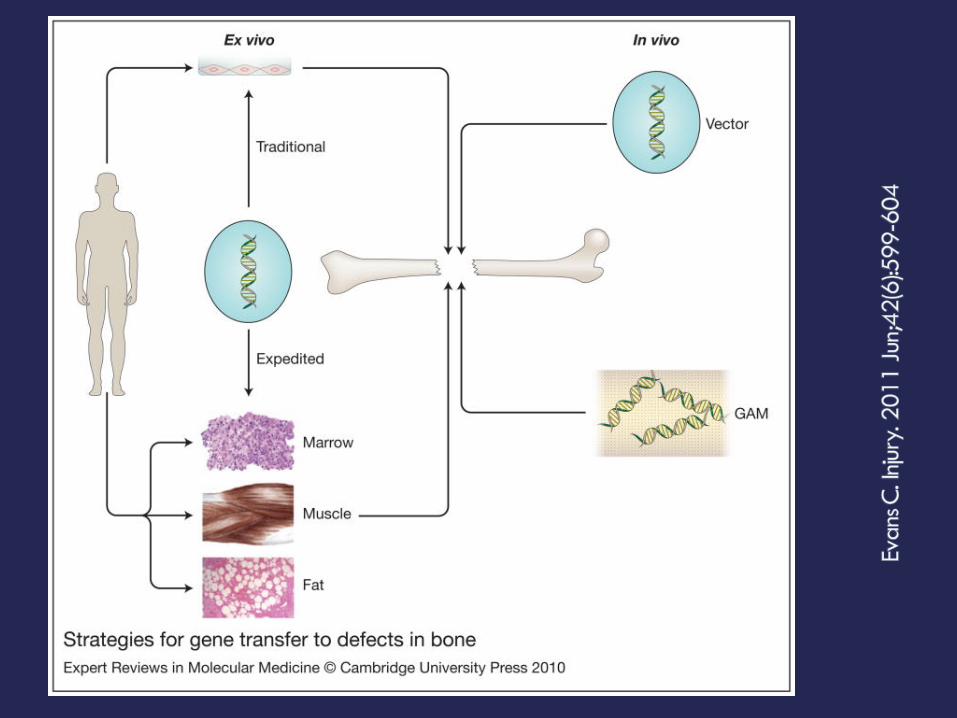
in vivo gene therapy:
¨ Directly delivered from biomaterials so it would circumvent the need for the harvest and transplantation of autologous cells
ex vivo gene therapy:¨ Requires the harvest of
autologous cells from patients for in vitro transduction followed by in vivo transplantation
¨ Very laborious and expensive
¨ Increases the risk of infection
18

Evans C. Injury. 2011 Jun;42(6):599-604
in vivo gene delivery:
the vector is introduced directly into the site of the osseous lesion, either as a free suspension or incorporated into a gene activated matrix (GAM)
ex vivo delivery:¨ they are used to genetically
modify cells, which are subsequently implanted
¨ Traditional ex vivo methods usually involve the establishment of cell cultures, which are genetically modified in vitro
¨ The modified cells are then introduced into the lesion, often after seeding onto an appropriate scaffold.
19
20

W. W. Hu, B.B. Ward, Z. Wang, and P.H. KrebsbachJ Dent Res 89(1):77-81, 2010
MATERIALSAND METHODS

¨ To facilitate bone regeneration, we delivered adenovirus-encoding BMP-2 either as a free suspension or lyophilized within gelatin scaffolds before being implanted into calvarial defects compromised by pre-operative irradiation
¨ Adenovirus-encoding LacZ was used as a negative control, to illustrate the effects of AdBMP2 on bone formation
¨ The cranial specimens were harvested for μ-CT scanning to reconstruct 3-D images and processed for histological analysis
22
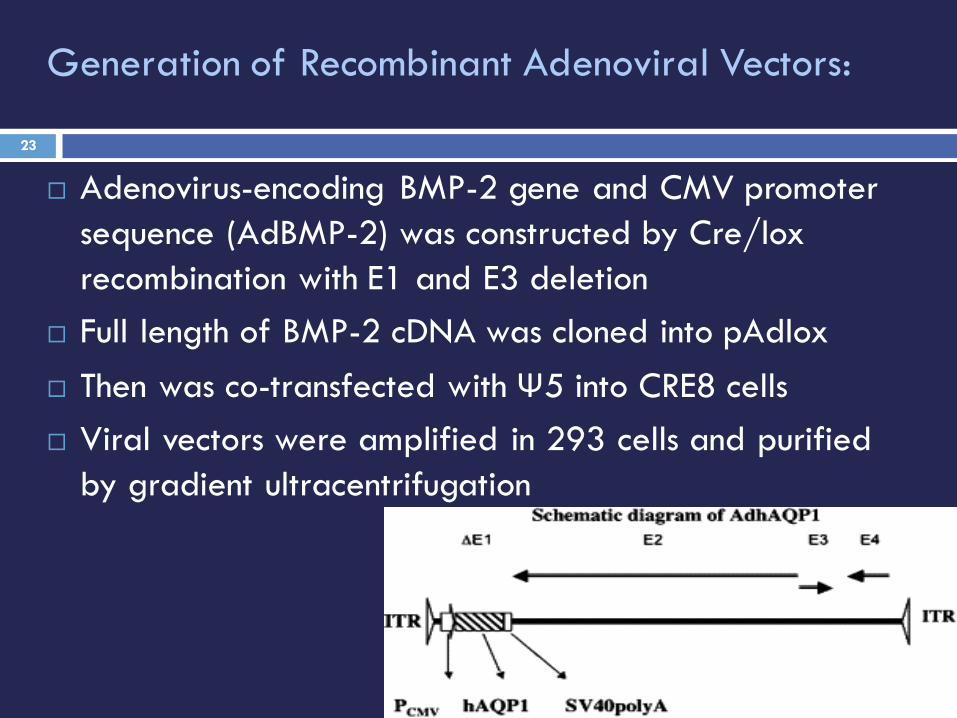
¨ Adenovirus-encoding BMP-2 gene and CMV promoter sequence (AdBMP-2) was constructed by Cre/lox recombination with E1 and E3 deletion
¨ Full length of BMP-2 cDNA was cloned into pAdlox¨ Then was co-transfected with Ψ5 into CRE8 cells¨ Viral vectors were amplified in 293 cells and purified
by gradient ultracentrifugation
Generation of Recombinant Adenoviral Vectors:
23

¨ Fisher rats were anesthetized¨ A single 12-Gy dose was delivered to Dmax at a
source-to-skin distance of 80 cm in an 11.47-minute exposure to the surgical site
¨ The rest of the body was shielded¨ The radiation dose was administered 2 weeks
before the surgical procedure, to mimic a clinical pre-surgical radiation protocol
Animal Irradiation24

Gelatin sponges (Pfizer) were used as scaffolds to deliver AdBMP-2.
¨ Virus lyophilization groups:108 PFU adenoviral vectors were loaded in scaffolds before being freeze-dried for 24 hours
¨ Free AdBMP-2 group:Was also prepared with the same virus concentration in PBS.
Polymer Matrix Loaded with Adenovirus for BMP-2 Gene Delivery
25
¨ To Evaluate the extent to which pre-operative radiotherapy retarded bone regeneration, rats without radiation treatment (No-XRT) were implanted with gelatin sponges containing lyophilized AdBMP-2
¨ To investigate the stability of freeze-dried adenovirus, we stored one group of AdBMP2 lyophilized in scaffolds at -80°C for 1 month prior to implantation.
26
¨ Critical-sized defects were created in calvariae with the use of an 8-mm-diameter trephine bur
¨ viral-loaded scaffolds or controls were placed in the defects
¨ Five animals per group were implanted for 5 weeks¨ All specimens were fixed in 10% buffered formalin
phosphate and stored in 70% alcohol prior to analysis
Calvarial Defect Model and Specimen Harvest
27

¨ Specimens were scanned by μ-CT on a MS8-CMR-100 μ-CT scanner
¨ Reconstructed images were analyzed with Microviewv2.1.0 software
¨ Circular regions of 8 mm in diameter were cropped as the region of interest (ROI)
¨ The bone volume fraction (BVF) and bone mineral density (BMD) of the regenerated bone were evaluated in the ROI, respectively
¨ The superficial views were captured, and the bone coverage in defects was evaluated as bone area fraction (BAF)
Micro-CT 3D Reconstruction28
W. W. Hu, B.B. Ward, Z. Wang, and P.H. KrebsbachJ Dent Res 89(1):77-81, 2010
RESULTS

Negative controls:¨ No regenerated bone in the defects except in the
immediate vicinity of the surgical margins.
AdLacZ was incapable of inducing new bone formation
3-D Images Reconstructed by μ-CT Scanning
30

Scaffolds with AdBMP2 suspensions:¨ A few bony islands were distributed throughout the
defects¨ Newly formed bone did not significantly cover the
defects
3-D Images Reconstructed by μ-CT Scanning
31

AdBMP2 delivered in a lyophilized formulation:¨ Significant regeneration was achieved, nearly
spanning the entire defect
3-D Images Reconstructed by μ-CT Scanning
32

Quantitative Assessment of Regenerated Bone
BVF and BMD by μ-CT scanning of newly formed bone:Suspended AdBMP2 compared with the negative control group¨ Suspended AdBMP2 enhanced the BVF from 14.2 ±
5.3% to 44.6 ± 8.5%¨ There was no
significant difference in BMD between these two groups (77 ± 16 mg/cc vs. 88 ± 13 mg/cc)
33
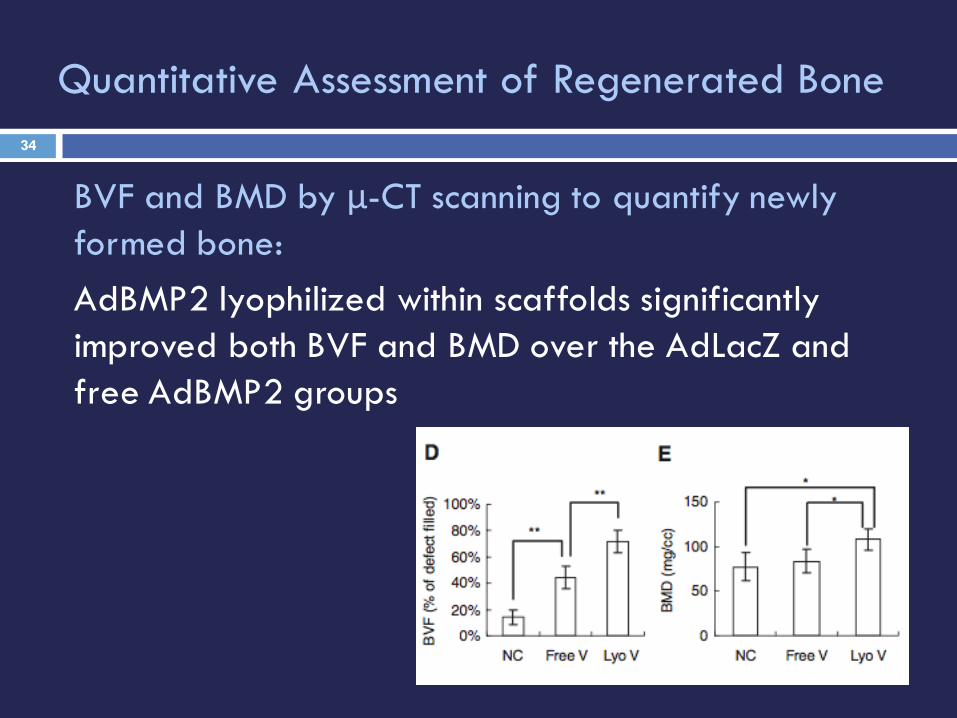
BVF and BMD by μ-CT scanning to quantify newly formed bone:AdBMP2 lyophilized within scaffolds significantly improved both BVF and BMD over the AdLacZ and free AdBMP2 groups
Quantitative Assessment of Regenerated Bone34

Quantitative Assessment of Regenerated Bone
To judge the extent of regenerated bone in the cranial defects, we determined the BAF of newly formed bone based on 3-D projection images captured by μ- CT:Free AdBMP-2 group:¨ Bone covered only a modest region of the defects (46.4 ± 11.3%)Lyophilized AdBMP2 group:¨ Significantly increased bone formation, and most of the area of the
defects was covered by mineralized tissue (68.7± 7.1%).
à The therapeutic effects ofAdBMP2 were greatly improvedwhen AdBMP was locallydelivered within scaffolds.
35

Histological section without radiation treatment (No-XRT):¨ scaffolds with lyophilized AdBMP-2 induced new bone
growth that nearly filled the entire defect¨ No residual scaffold material was observed¨ The regenerated bone was integrated with the native
bone at the defect margins and supported a robust hematopoietic marrow
The Effects of Bone Regeneration in Critical- sized Defects Compromised by Radiotherapy
36
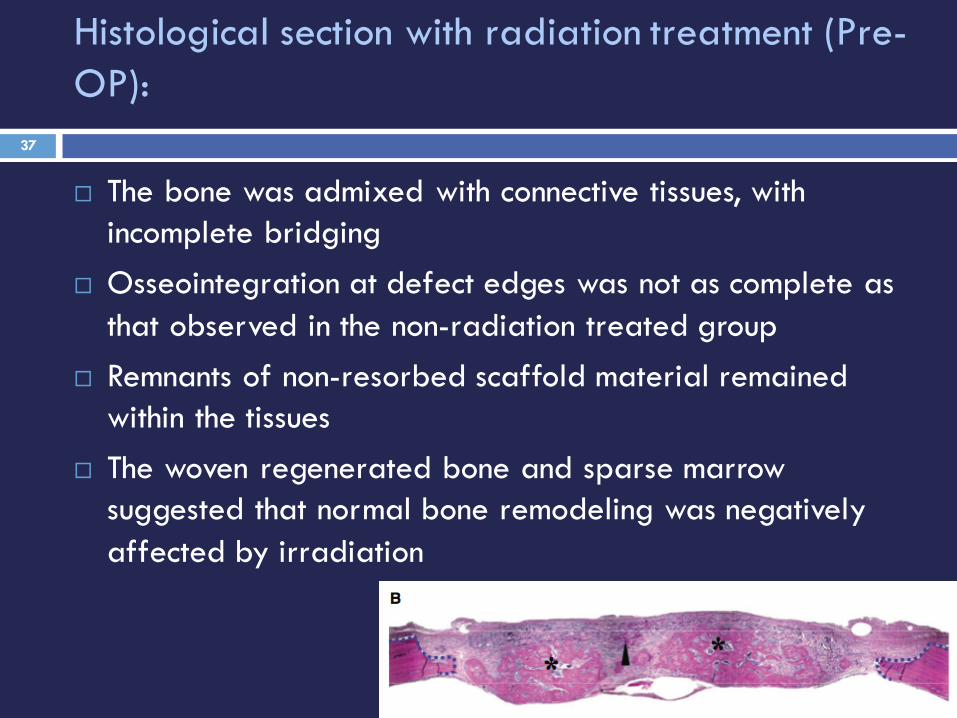
Histological section with radiation treatment (Pre-OP):
¨ The bone was admixed with connective tissues, with incomplete bridging
¨ Osseointegration at defect edges was not as complete as that observed in the non-radiation treated group
¨ Remnants of non-resorbed scaffold material remained within the tissues
¨ The woven regenerated bone and sparse marrow suggested that normal bone remodeling was negatively affected by irradiation
37
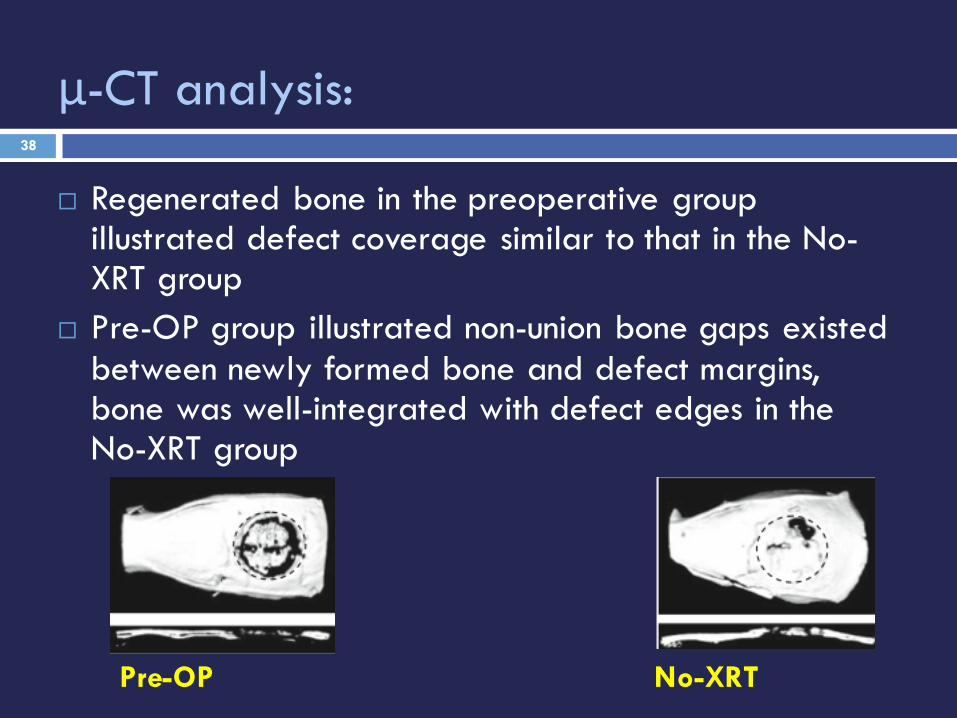
μ-CT analysis:
¨ Regenerated bone in the preoperative group illustrated defect coverage similar to that in the No-XRT group
¨ Pre-OP group illustrated non-union bone gaps existed between newly formed bone and defect margins, bone was well-integrated with defect edges in the No-XRT group
Pre-OP No-XRT
38

Quantified data analysis:
¨ BVF and BAF in these two groups had no significant differences
¨ BMD of the Pre-OP group was significantly less than that of the No-XRT group (108 ± 12 mg/ cc vs. 250 ± 41mg/cc)
Level of mineralization in the Pre-OP group was reduced because of the side-effects of radiation
39

¨ AdBMP2 lyophilized in gelatin scaffolds was stored at -80°C for 1 month and implanted into calvarial defects with pre-operative radiotherapy (1M-PreOP) group
μ-‐CT scanning¨ Bone formation in the 1M-PreOP group had bone defect
coverage similar to that in the Pre-OP group
Adenoviral Bioactivity is Preserved in Lyophilized Gelatin Scaffolds
40
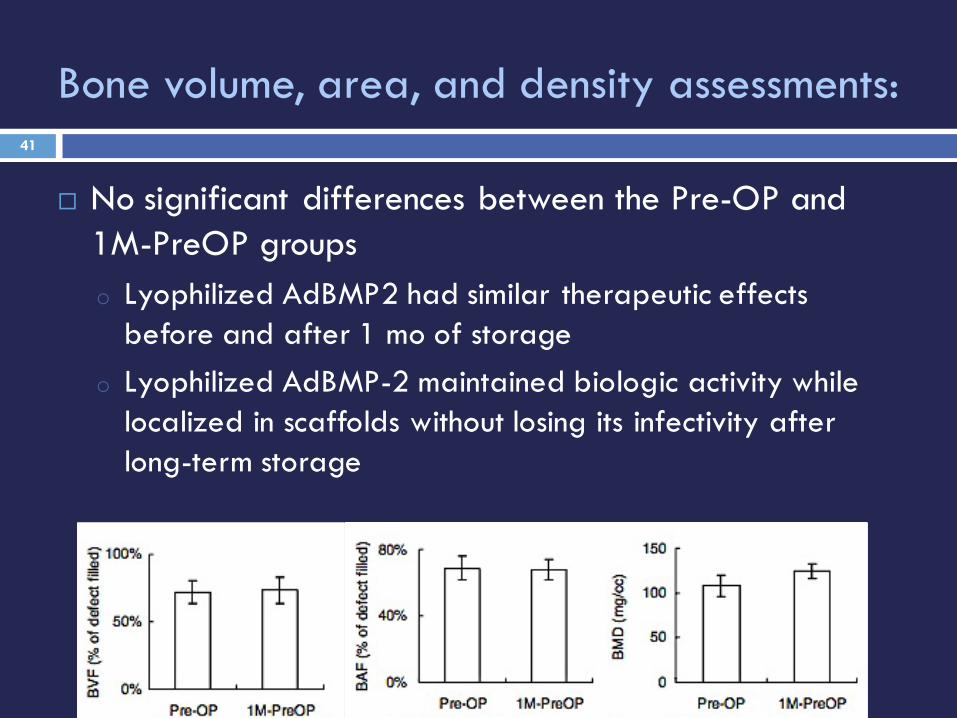
Bone volume, area, and density assessments:
¨ No significant differences between the Pre-OP and 1M-PreOP groupso Lyophilized AdBMP2 had similar therapeutic effects
before and after 1 mo of storageo Lyophilized AdBMP-2 maintained biologic activity while
localized in scaffolds without losing its infectivity after long-term storage
41

W. W. Hu, B.B. Ward, Z. Wang, and P.H. KrebsbachJ Dent Res 89(1):77-81, 2010
DISCUSSION

¨ AdBMP-2 lyophilized demonstrated superior bone formation in bone defects compromised by preoperative irradiation
¨ BVF and BAF in the suspended and AdBMP-2 groups were both higher than in the negative control group
¨ No significant differences in BMD between these two groups
¨ Osteogenesis induced by free AdBMP-2 mainly increased bone quantity (BVF and BAF), but not bone quality (BMD)
AdBMP-2 lyophilized compared with the freely suspended virus group:
43

¨ Lyophilized AdBMP-2 enhanced both bone quantity and quality in irradiated defects
¨ The lyophilization strategy would likely be more appropriate for treating irradiated bone defects than a conventional bolus gene delivery method.¤ Due to sufficient mineral density is important for bone
homeostasis and function
Lyophilized compared with the freely suspended virus group:
44
¨ Newly formed bone in the Pre-OP group had bone volume and defect coverage similar to that in the No-XRT group
¨ Sagittal images from μ-CT scanning and the BMD analysis demonstrated that the mineralized tissue in the Pre-OP group was less dense than in the No-XRT group
¨ The histomorphologic assessments also illustrated that woven bone was mainly formed in the Pre-OP defects.
¨ The sparse marrow suggests a sub-optimal environment caused by radiation, and the bone regeneration period may need to be longer for proper recovery.
The effects of radiotherapy on bone regeneration
45

¨ Biologic activity and therapeutic effects of lyophilized AdBMP-2 were maintained after 1 month of storage at -80°C.
¨ Viral vectors encoding cell-signaling genes can be incorporated within biomaterial scaffolds and stored at low temperatures as pre-made constructs, making clinical application convenient for surgeons to apply in an operating room setting.
The long-term storage experiments46

W. W. Hu, B.B. Ward, Z. Wang, and P.H. KrebsbachJ Dent Res 89(1):77-81, 2010
CONCLUSION

Conclusion
o In vivo gene therapy by locally delivering BMP-2 gene within scaffolds, which effectively repaired defects compromised by radiation damage
o Compared with ex vivo gene therapy, lyophilized adenovirus transduces cells in situ within the wound sites and simplifies the treatment by avoiding repeated surgeries
48

Conclusion
o Reduces the risk of contamination by not using autologous cells
o Virus-scaffold constructs can be prepared and stored in advance of a regenerative procedure and could be applied in an operating room setting
49

Conclusion
o The development of this technology could provide alternative options for bone replacement in irradiated tissue beds without the limitations and side-effects of current reconstructive technique.
o Lyophilized adenovirus in situ could have broad applications to non-irradiated tissues.
50

W. W. Hu, B.B. Ward, Z. Wang, and P.H. KrebsbachJ Dent Res 89(1):77-81, 2010
THANK YOU