Embed Size (px)
Citation preview

Nelson Origa, Pharm.D. Candidate Texas Tech University Health Sciences Center
School of Pharmacy | Dallas Campus February 4, 2015

Learning Objectives By the end of this presentation participants should be able to:1.Describe mechanisms of CINV2.Classify cancer drugs associated with CINV according to their emetogenicity3.Discuss current treatment recommendations for CINV4.Explain mechanism of action of Akynzeo® and its pharmacokinetics/pharmacodynamics5.Analyze trials that led to approval of Akynzeo® based on safety and efficacy
2

Abbreviations CINV-Chemotherapy-induced
nausea and vomiting 5-HT3-Serotonin type 3 receptor HEC-Highly emetogenic
chemotherapy MEC-Moderately emetogenic
chemotherapy AP-Area Postrema CTZ-Chemoreceptor trigger
zone NIDL-No Impact on Daily
Living FLIE-Functional Living Index-
Emesis
NK1 RA-Neurokinin 1receptor antagonist
NEPA-Netupitant + palonosetron EC-Emesis center CR-Complete Response CP-Complete protection NCCN-National comprehensive
cancer network MASCC-Multinational
Association of Supportive Care in Cancer
ASCO-American Society of Clincal Oncology
NTS-Nucleus tractus solitarius
3
Chemotherapy-Induced Nausea and Vomiting: Definitions
Nausea: Inclination that vomiting is imminent
Vomiting: Expulsion of gastric contents due to contraction of muscles of abdomen and diaphragm
Retching: Movement of muscles of abdomen and thorax
CINV Acute 0-24 h Delayed 24-120 h Anticipatory
Learned response Breakthrough
During chemotherapy Refractory Occurs
despite use of antiemetics
4
CINV: Risk FactorsPatient Factors
Age: >6years or <50 Gender: Female>Male Vomiting Previous
cycle Low alcohol use Motion sickness Anxiety Expectation
Treatment factors Emetogenicity of drug Dose of drug Antiemetic
administered
Warr. Eur J Pharmacol. 2014;192-196. 5

CINV: Prevalence & Consequences67 Patients on HEC
60% delayed nausea 50% delayed emesis
231 Patients on MEC 52% delayed nausea 28% delayed emesis
Consequences of CINV↑Length of stay Poor adherence Diminished quality of
life
Jenelsins MC et al .Expert Opin Pharmacother. 2013;14(6):757-66.Grunberg SM et al.Cancer. 2004;100(10):2261-2268.
6

Chemotherapy Emetic Risk ClassificationHigh: > 90% frequency of emesis without antiemetics
Moderate: 31-90% frequency of emesis without antiemetics
Low: 10-30% frequency of emesis without antiemetics
Minimal: <10% frequency of emesis without antiemetics
Hesketh N. Engl J Med. 2008; 358:2482-24947

Emetogenic Potential of Cancer DrugsHigh Moderate Low Minimal
Intravenous Cisplatin Alemtuzumab Bortezomib Bevacizumab
Cyclophospha-mide≥1500
Cyclophosphamide<1500
Cetuximab Bleomycin
Gemcitabine Rituximab
Dacarbazine Doxorubicin Docetaxel Vinblastine
Carmustine Epirubicin Etoposide Vincristine
Oral Procarbazine Imatinib Capecitabine Hydroxyurea
Hexamethyl-melamine
Cyclophosphamide
Etoposide Methotrexate
8Affronti ML. Cancer Manag Res.2014; 6:329-337

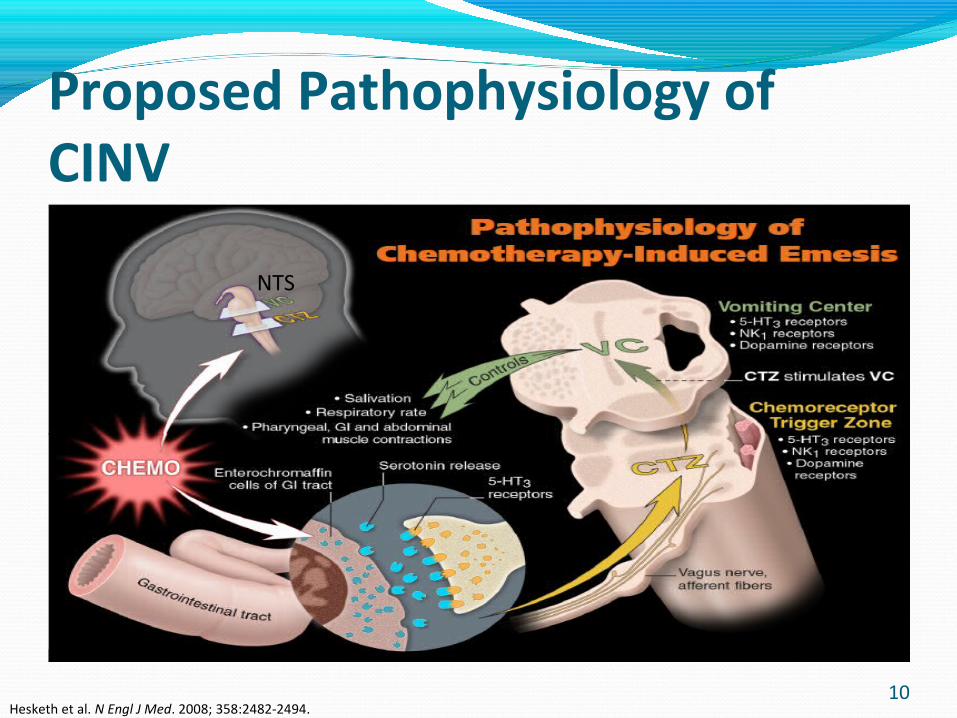
Proposed Pathophysiology of CINVCentral & peripheral regions
Emetic/vomiting center (VC)-neurons in medulla oblongata-coordinate NV-primary structure
Chemoreceptor trigger zone(CTZ) in AP in floor of 4th ventricle of brain activated by chemotherapy
Vagal nerve afferents from GIT to nucleus tractus solitarius (NTS) & dorsal motor nucleus of the vagus nerve
GI tract releases 5-HT, SP,D2,H1 due to irritation, free radicals, damage, and necrosis of GI mucosa by chemo
Jenelsins MC .Expert Opin Pharmacother. 2013;14(6):757-66 Grunberg S. NEJM 1993.329:1790-1796
9
Proposed Pathophysiology of CINV
NTS
Hesketh et al. N Engl J Med. 2008; 358:2482-2494.10
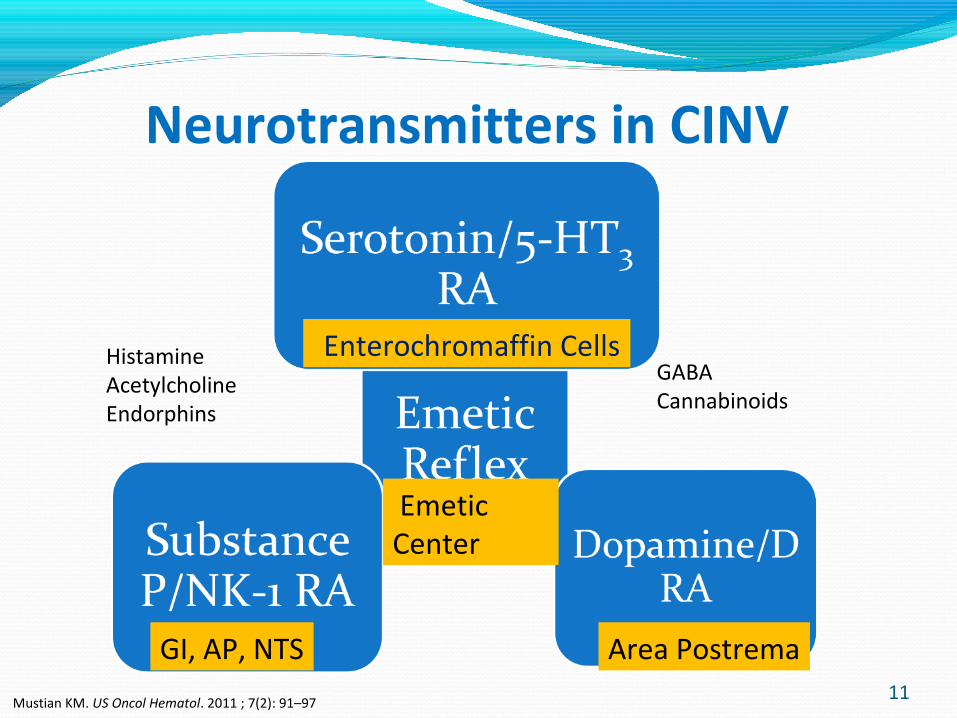
Neurotransmitters in CINV
GI, AP, NTS
Enterochromaffin Cells
Emetic Center
Area Postrema
GABACannabinoids
HistamineAcetylcholineEndorphins
Mustian KM. US Oncol Hematol. 2011 ; 7(2): 91–9711
CINV: Antiemetic Agents5-HT3 RA
Palonosetron(Aloxi®)Ondansetron(Zofran®)Granisetron(Sancuso®)Dolasetron(Anzemet®)
CorticosteroidsDexamethasone(Decadron®)Dopamine RAMetoclopramide(Reglan®)
NK-1 RAAprepitant(Emend®)Fosaprepitant(Emend®)Netupitant/palonosetron (Akynzeo®)
Benzodiazepines Lorazepam(Ativan®) Atypical Antipsychotic olanzapine(Zyprexa®)
Ettinger DS. NCCN Guidelines. Antiemesis.v 2.2014. 12

Antiemetic Agents: Adverse Effects5-HT3 RA
Headache Constipation QT prolongation (FDA
alert) Somnolence Dizziness Elevated transaminases
NK-1 RA Fatigue Hiccups Weakness Dizziness
Corticosteroids Euphoria Insomnia ↑Appetite Hyperglycemia Fluid retention
Ettinger DS. NCCN Guidelines. Antiemesis.v 2.2014. 13

CINV Prophylaxis The NCCN Guidelines for HEC
High Risk Low Risk 5-HT3 RA +Steroid+ NK-1 RA( or
olanzapine)
Palonosetron + dexamethasone + aprepitant
5-HT3 RA + dexamethasone + fosaprepitant
Dexamethasone or
Metoclopramide or Prochlorperazine or
Ondansetron or Dolasetron or Granisetron
Ettinger DS. NCCN Guidelines. Antiemesis.v 2.2014 14

CINV Prophylaxis NCCN Guidelines for MEC
Day 1 Days 2 and 3
5-HT3 RA + Steroid ±NK-1 RA 5-HT3 Monotherapy –No palonosetron Ondansetron 8mg po bid OR Steroid monotherapy: Dexamethasone 8mg po/iv daily OR NK-1 RA± Steroid
Palonosetron 0.25mg iv + Dexamethasone 12mg po/iv±Aprepitant 125mg po/fosaprepitant 150mg IV
OR OR
Olanzapine-based Regimen Olanzapine 10mg PO days 2-4 if given on day 1± Lorazepam 0.5mg-2mg PO/IV q 4h prn± HR2RA or proton pump inhibitor
Olanzapine 10mg po +Palonosetron 0.25mg iv +Dexamethasone 20mg iv
15Ettinger DS. NCCN Guidelines.Antiemesis.V2.2014.

CINV Treatment Summary
Mustian KM et al. US Oncol Hematol.2011;7(2):91-97. 16

Novel NK1 and 5-HT3 Antagonists
Netupitant Palonosetron Highly selective NK1 RA binds
NK1 in abdominal vagus nerve, brainstem, and AP→decreased emesis
Long t1/2~ 90 hours>90% brain receptor
saturation for long-96 hours Enhanced Substance P
inhibition when combined with palonosetron
Allosteric & positive cooperativity at 5-HT3 receptors
T1/2=40hours
5-HT3 receptor internalization= inhibition ↑and efficacy in acute & delayed CINV than 1st Gen 5-HT3 RA
High binding affinity/specificity to 5-HT3 receptors
Navari RM. Drug Design, Development and Therapy. 2015;9: 155-161 Hasketh . Ann Oncol.2014;25(7): 1340-1346 17

Novel NK1 and 5-HT3 Antagonists
Netupitant 300mg Palonosetron 0.5mgPK/PD:Onset 15 min-3h, Vd 1982±906L
99.5% protein binding Metabolized by CYP 3A4, 2C9, 2D6 to metabolites
Receptor occupancy: 92.5%(6h), 86.5%(24h)
Co-administration with netupitant 600mg /palonosetron 1.5mg: No significant effect on QTc intervalFixed-dose combination with netupitant offers: Synergy Convenience Potential guideline ↑ adherence
Akynzeo(R) [package insert]., SA, Lugano, Switzerland: Helsinn Healthcare; 2014. 18

Approved October 10, 2014
19

Akynzeo: A Better or Bitter Pill for the Prevention of CINV ?Dosage: 300mg
netupitant/0.5mg palonosetron capsule
Administration- HEC 1 capsule po 1 hour before
chemotherapy + 12mg dexamethasone 30 minutes prior to chemotherapy on day 1, then 8mg days 2-4
Anthracyclines/Cyclophosphamide: Akynzeo 1 capsule po 1hour and 12mg dexamethasone 30 minutes prior to chemotherapy
Contraindication: NoneAdverse events≥3%:
Headache, constipation, dyspepsia, fatigue, asthenia
Akynzeo(R) [package insert]., SA, Lugano, Switzerland: Helsinn Healthcare; 2014.20
Akynzeo: A Better or Bitter Pill for the Prevention of CINV ?Drug interactions:Netupitant- moderate
inhibitor of CYP3A4 →dexamethasone, midazolam, docetaxel, cyclophosphamide
CYP 3A4 Inducers/Inhibitors
Pregnancy category C
Dose adjustment: Hepatic
Mild-moderate-No dose adjustment; severe- avoid
Renal Mild-moderate
impairment-No dose adjustment
Not studied in ESRD
Akynzeo(R) [package insert]., SA, Lugano, Switzerland: Helsinn Healthcare; 2014.21

NEPA Versus Aprepitant + PALOStudy of 413 patients on
HEC and MEC, NEPA showed small advantage (2-7%) over aprepitant/PALO in primary analysis: No emesis, no rescue therapy
Gralla RJ et al. Ann Oncol. 25(7):1333-1339.22

Study 1
23

Study 1: Study DesignPhase II, Multicenter, Randomized, double blind,
double dummy, parallel group study694 chemotherapy naïve patients2008 29 sites-Russia 15 sites-Ukraine
Hasketh PJ et al . Ann Oncol.2014;25(7): 1340-1346.
24

Study 1:Inclusion Criteria≥18 years oldDx of malignant tumorKarnofsky Performance
Scale score ≥70%Able to follow
procedures and complete patient diary
Naïve to chemotherapyScheduled cisplatin
therapy ≥50mg/m2 alone or in combination
Hasketh PJ et al . Ann Oncol.2014;25(7): 1340-1346. 25
Study 1:Exclusion CriteriaScheduled to receive
HEC or MEC from day 2-5 post chemoModerate/highly emetogenic radiotherapy 1 week before day1
Bone marrow/stem cell transplant
Experienced vomiting, retching or >mild nausea in 24 h before day 1
History of serious CV conduction abnormalities except right bundle branch block
Hasketh PJ et al . Ann Oncol.2014;25(7): 1340-1346.
26
Study 1:Exclusion CriteriaChronic use of CYP 3A4
substrates/inhibitor within 1 week
4 weeks of inducers before day 1
Use of CYP 3A4 substrate/inhibitor within 1 week
Hasketh PJ et al . Ann Oncol.2014;25(7): 1340-1346. 27
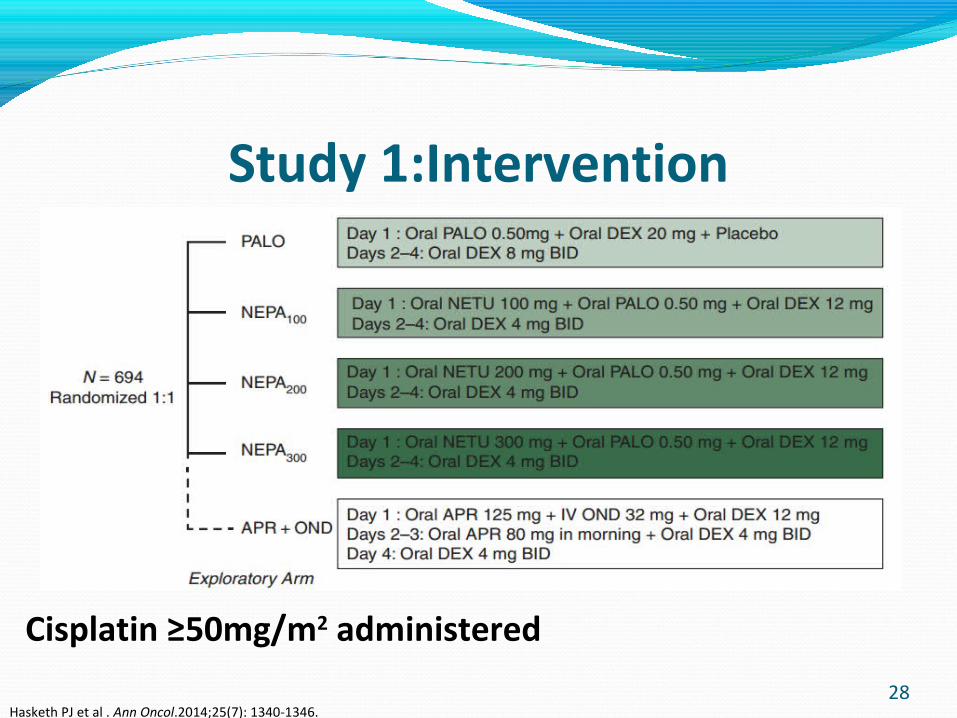
Study 1:Intervention5 Treatment groups:
Hasketh PJ et al . Ann Oncol.2014;25(7): 1340-1346.
Cisplatin ≥50mg/m2 administered
28
Study 1: Intervention Cisplatin ≥50mg/m2 1-4 h infusion Blinding by matching placebos Rescue meds: For refractory/persistent nausea
and vomiting Treatment failure→ NEPA: 60 minutes before chemotherapy Dexamethasone: 30 minutes before
chemotherapy
Hasketh PJ et al . Ann Oncol.2014;25(7): 1340-1346. 29

Study 1: Efficacy EndpointsPrimary Endpoint Secondary Endpoints Complete Response(CR)
No EmesisNo Rescue medication during overall phase post-chemo (0-120h)
CR in acute phase (0-24h)CR during delayed phase(25-
120 h) No emesis No significant nausea:
Visual Analog Scale ≤25mmComplete Protection in all phases:
CR + No significant nausea
Hasketh PJ et al . Ann Oncol.2014;25(7): 1340-1346.
30

Study 1: Statistical AnalysisIntention-to-treatAssumed overall CR
70% NEPA 50% PALO
1-sided α level=0.0166 129 patients/goup 85% →
powerRounded up to
136/group 680 patients →total
Logistic regression-Primary & secondary efficacy adjust for gender
Holm-Bonferroni-to adjust for multiple comparisons
Post hoc logistic regression-compare APR arm and PALO
Hasketh PJ et al . Ann Oncol.2014;25(7): 1340-1346. 31
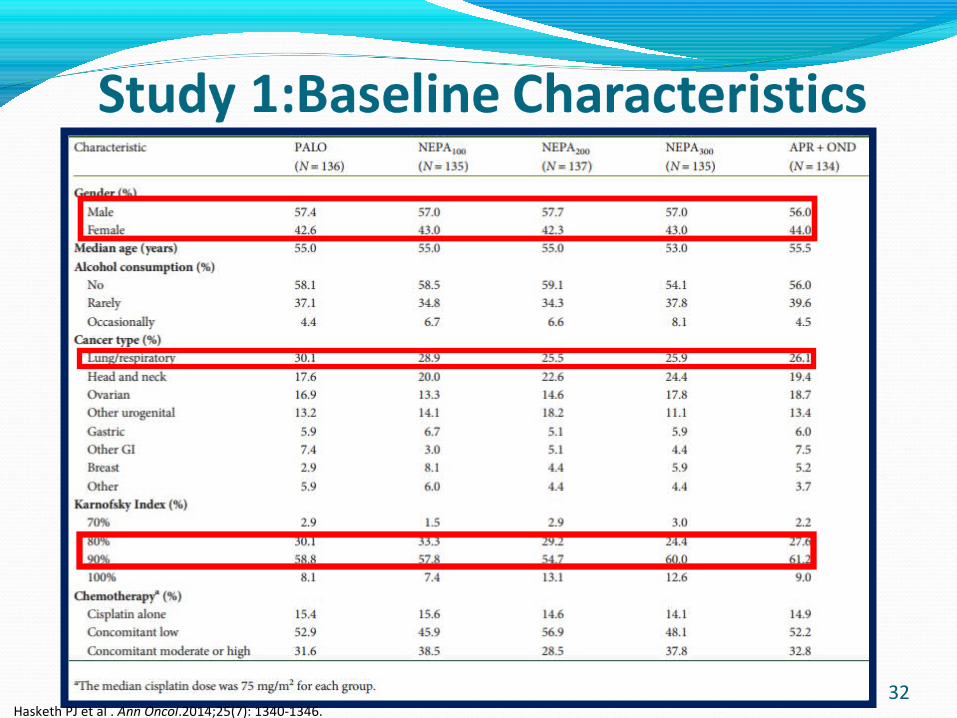
Hasketh PJ et al . Ann Oncol.2014;25(7): 1340-1346.32
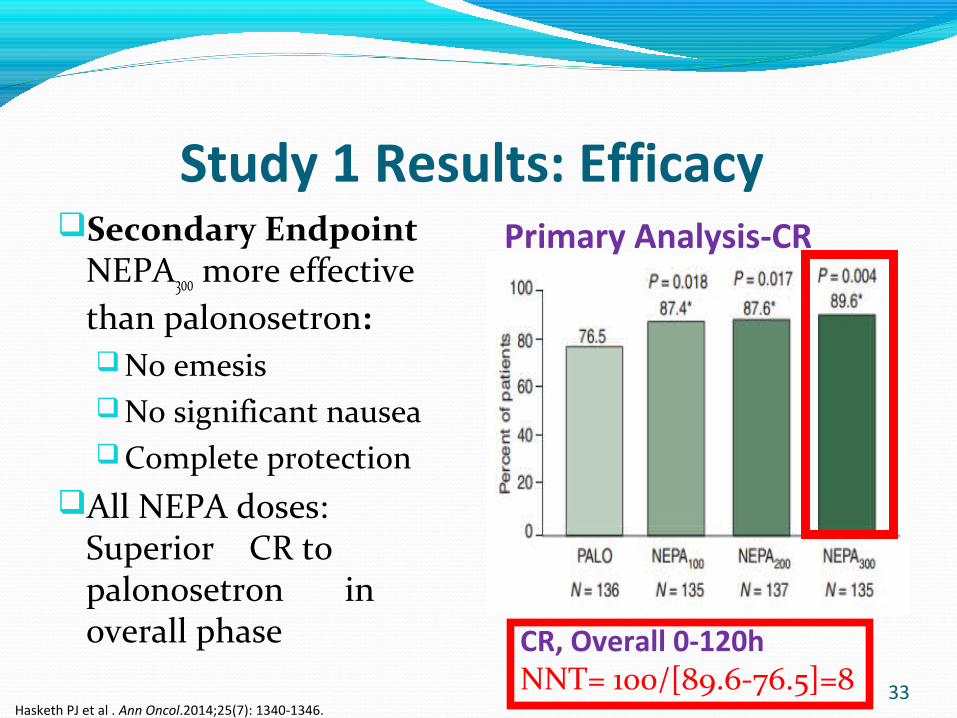
Study 1 Results: Efficacy Secondary Endpoint
NEPA300 more effective than palonosetron:No emesisNo significant nauseaComplete protection
All NEPA doses: Superior CR to palonosetron in overall phase
Primary Analysis-CR
CR, Overall 0-120hNNT= 100/[89.6-76.5]=8
Hasketh PJ et al . Ann Oncol.2014;25(7): 1340-1346.33

Study 1 Results Secondary Analysis
Hasketh PJ et al. Ann Oncol.2014;25(7): 1340-1346.34

Study 1: Safety DataAdverse Effects Authors’ Conclusion Most common Hiccups NEPA300 7(5.1%) NEPA 200 5(3.6% NEPA 100 5(3.7%) PALO 5(3.7%) Headache
NEPA 300 the most Effective dose combination
NEPA regimens significantly improved prevention of CINV in patients receiving cisplatin-based HEC
NEPA arms comparable to APR arm: adverse events & ECG changes
Hasketh PJ et al . Ann Oncol.2014;25(7): 1340-1346.
35

Study 1: CritiqueStrengths WeaknessesRandomized, double blind Multicenter-44 sites Included patients with
different neoplasmsClinically important primary
endpoints
Conducted in one region only-Russia and Ukraine
Relied on patients ability to keep accurate diaries
Male > female yet female gender is a risk factor for CINV
36

Study 2
37
Study 2: Study Design Phase III, Multicenter,
Randomized, double blind, double dummy, parallel group study
1455 patientsApril 2011-November
2012177 sites, 15 countries
Countries:Argentina, Belarus, Brazil,
Bulgaria, Croatia, Germany, Hungary, India, Italy, Mexico, Poland, Romania, Russia, Ukraine, USA.
Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333.
38

Study 2: Treatment
Blinding: Matching PlaceboCyclophosphamide IV 500-1500mg/m2 + doxorubicin IV ≥60mg/m2 ORCyclophosphamide IV 500-1500mg/m2 + epirubicin IV ≥60mg/m2
Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333.39

Study 2 Inclusion/Exclusion Criteria
Inclusion Criteria Exclusion Criteria
≥18 years oldNaïve to chemotherapyScheduled to receive first
AC MEC regimen for a solid malignant tumor
Eastern cooperative oncology group(ECOG) performance status of 0,1, or 2
Scheduled to receive: HEC from day 1-5 or
MEC from day 2-5 post chemo
Radiation therapy to abdomen/pelvis 1 week before day 1 or between day 1 and 5, or 3
Bone marrow/stem cell transplant
Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333.40
Study 2: Exclusion CriteriaExperienced vomiting, retching, mild nausea within
24 hours before day 1Serious cardiovascular abnormalities except
incomplete right bundle branch blockUse of CYP3A4 inducer within 4 weeks or
strong/moderate inhibitors within 1 week or scheduled to receive CYP 3A4 inhibitor/inducer/substrate
Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333.
41

Study 2: Assessments Each patient kept
diary starting day 1- morning of day 6
Emetic Episode: Timing Duration Rescue drug use
Severity of Nausea Visual Analog Scale Impact of CINV on
patients’ lives:Functional Living
Index-Emesis (FLIE)
9 Nausea domains 9 vomiting domains
Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333.42
Study 2: Efficacy EndpointsPrimary Efficacy Endpoints Secondary Efficacy Endpoints
Complete Response (CR) No emesis No rescue drug in
delayed phase of cycle 1
Complete Response(CR) Acute phase Overall phaseComplete Protection (CR + No significant
nausea) No emesis, no significant
nausea, during acute, delayed, and overall phases
Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333.
43

Study 2: Statistical AnalysisPrimary aim: Illustrate
superiority of NEPA over PALO based on CR during delayed phase of cycle 1
Cochran-Maentel-Haenszel (CMH) test to analyze primary efficacy outcome
Assumed responder rate 60% NEPA
50% PALO 2-Sided test of
difference, α level=0.05Sample size of 661
Patients/group 90% →power to detect 9% difference
Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333. 44

Study 2: Baseline Characteristics
Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333.
45
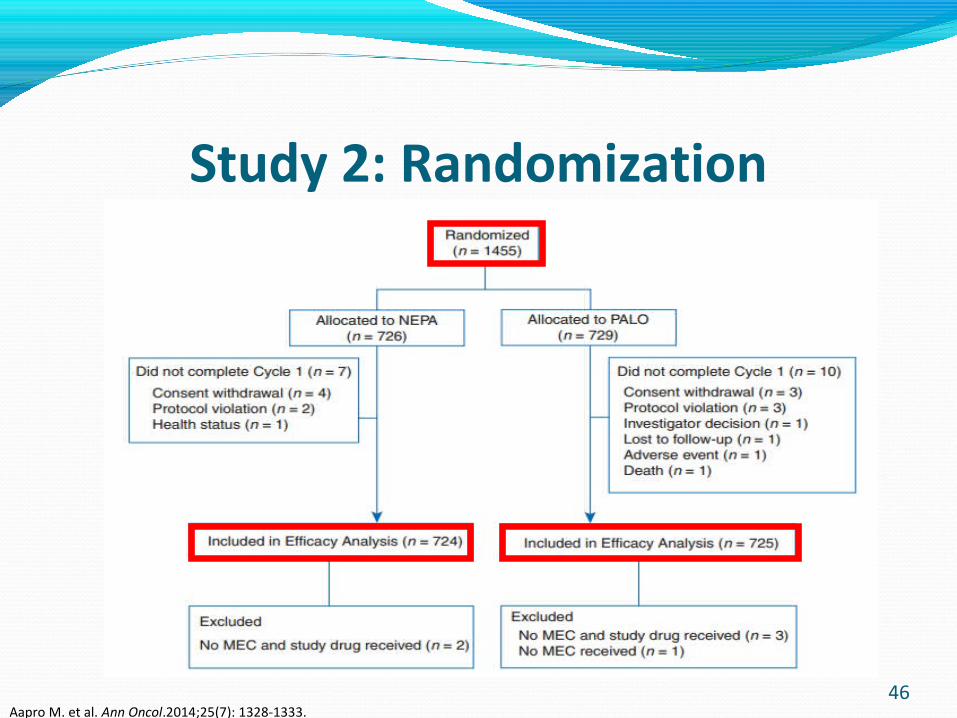
Study 2: Randomization
Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333.46

Study 2 Results: EfficacyPrimary Secondary Delayed Phase
NEPA superior to palonosetron- 76.9% Versus 69.5% (P=0.001)
Acute & Overall Phases
Significantly higher CR rates for NEPA than palonosetron
Delayed & Overall Phases
NEPA consistently more effective than palonosetron: No emesis
No significant nausea Complete protection
Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333.47

Study 2 Results: Primary Efficacy
NEPA superior to PALO in delayed Phase: CR of 76.9% Vs 69.5%NNT: Delayed 100/[76.9-69.5) = 14
CR:No EmesisNo Rescue drug
Study 2 Results: Primary Efficacy
48Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333

Study 2 Results: Impact on LifePatients with NIDL based on FLIE: Overall 0–120 h
Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333.
Study 2 Results: Impact on Patients Life
49
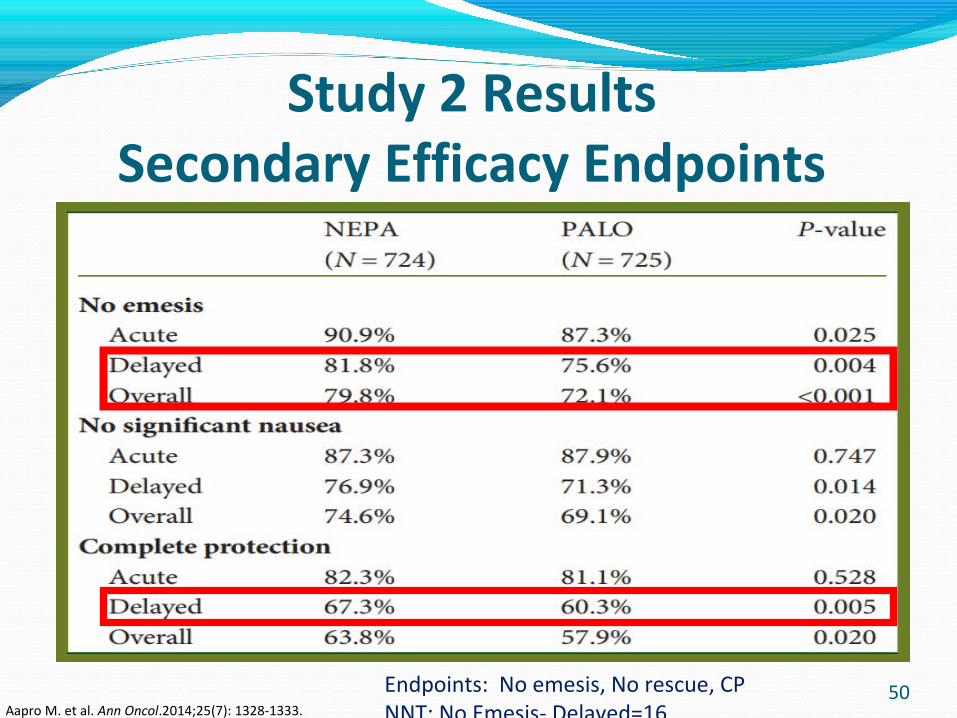
Study 2 Results Secondary Efficacy Endpoints
Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333.
50Endpoints: No emesis, No rescue, CPNNT: No Emesis- Delayed=16
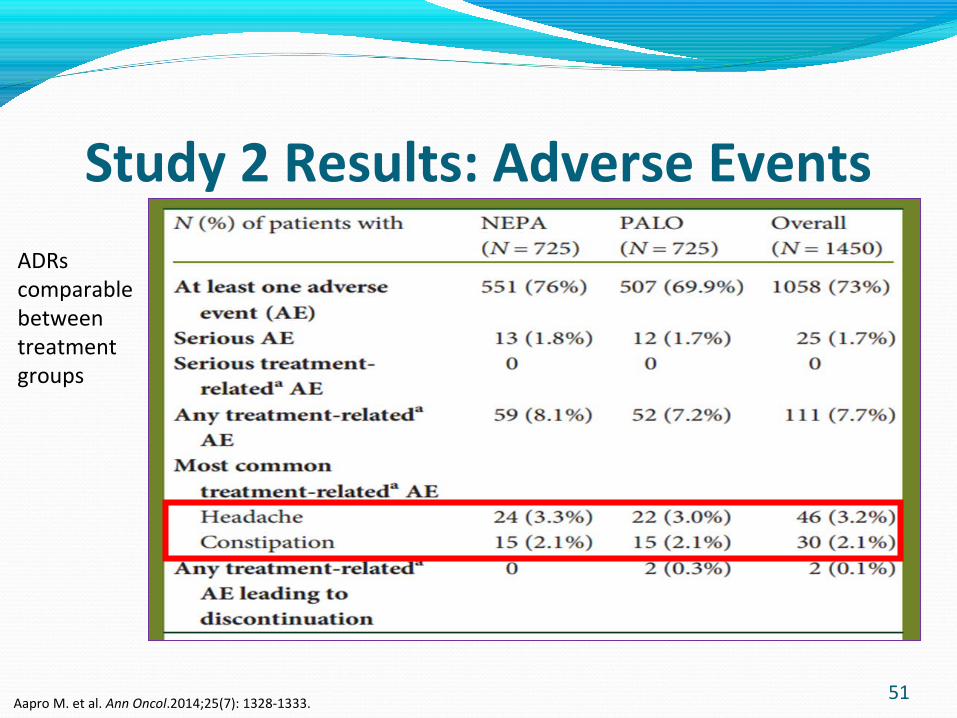
Study 2 Results: Adverse Events
ADRs comparable between treatment groups
Aapro M. et al. Ann Oncol.2014;25(7): 1328-1333.
51

Study 2 Strengths
Randomized, double blind Intention-to-treat Clinically significant primary/secondary endpoints Patients with different neoplasms included Majority of patients fall within age bracket at higher
risk for CINV
LimitationsRelied on Patients to keep accurate diariesStudy included only chemotherapy naïve patients
52
Study 2 Clinical Impact/Author’s Conclusion Akynzeo®, an oral fixed-dose drug, may help
overcome potential barriers to guideline adherence by providing convenience in a single day 1 dose of NEPA plus dexamethasone on day 1 only to prevent CINV for 5 days after therapy.
Akynzeo demonstrated superiority over palonosetron during 5-day period after chemotherapy.
53

Akynzeo: A Better or Bitter Pill? Personal Conclusion
Results from efficacy studies indicate that Akynzeo® is a better pill for the prevention of CINV: It offers an easier to take fixed-dose oral capsule on day 1 of chemotherapy for prolonged prevention of CINV.
Akynzeo (netupitant/palonosetron) may offer better adherence to guidelines for CINV prevention hence improvement in outcomes for patients on HEC/MEC despite higher price.
54
Acknowledgements Dr. Valerie Vuylsteke, Pharm.D., BCACP
Dr. Sachin Shah, PharmD., BCOP
55

Bibliography 1. Warr. Prognostic factors for chemotherapy induced nausea and vomiting. Eur J Pharmacol.2014; 722:192-6.
2. Jenelsins MC, Tejani MA, Kamen C et al. Current pharmacotherapy for chemotherapy-induced nausea and vomiting in cancer patients. Expert Opin Pharmacother. 2013; 14(6):757-66.
3. Grunberg SM, Deuson RR, Mavros P,et al. Incidence of chemotherapy-induced nausea and emesis after modern antiemetics .Cancer. 2004; 100 (10):2261-2268.
4. Hesketh PJ. Chemotherapy-Induced Nausea and Vomiting. N Engl J Med. 2008; 358:2482-2494.
5. Affronti ML, Bubalo J. Palonosetron in the management of chemotherapy-induced nausea and vomiting in patients receiving multiple-day chemotherapy. Cancer Manag Res. 2014; 6: 329–337.
6. Mustian KM, Devine K, Ryan JL et al. Treatment of Nausea and Vomiting During Chemotherapy. US Oncol Hematol. 2011; 7(2): 91–97.
7. Grunberg SM, Hasketh PJ. Control of chemotherapy-induced emesis. NEJM. 1993.329:1790-1796.
56

Bibliography8. National Comprehensive Cancer Network (NCCN). NCCN Clinical Guideline in Oncology Antiemesis version 2.2014.http://www.nccn.org/professionals/physician_gls/pdf/antiemesis.pdf
9. Navari RM. Profile of netupitant/palonosetron (NEPA) fixed dose combination and its potential in the treatment of chemotherapy-induced nausea and vomiting (CINV). Drug Design, Development and Therapy. 2015;9: 155-161
10. Hasketh P, Rossi G, Rizzi G, et al. Efficacy and safety of NEPA, an oral combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting following highly emetogenic chemotherapy: a randomized dose-ranging pivotal study. Ann Oncol.2014;25 (7): 1340-1346.
11. Akynzeo(R) [package insert]. SA, Lugano, Switzerland: Helsinn Healthcare; 2014.
12. Gralla R, Bosnjak S, Hontsa A, et al. A phase III study evaluating the safety and efficacy of NEPA, a fixed-dose combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting over repeated cycles of chemotherapy. Ann Oncol.25(7):1333-1339
13. Aapro M, Rugo H, Rossi G, et al. A randomized phase III study evaluating the efficacy and safety of NEPA, a fixed-dose combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy. Ann Oncol.2014; 25(7): 1328-1333.
57





























