Embed Size (px)
Citation preview
Acute Glomerulonephritis
Soumya Ranjan Parida Basic B.Sc. Nursing 4th year Sum Nursing College
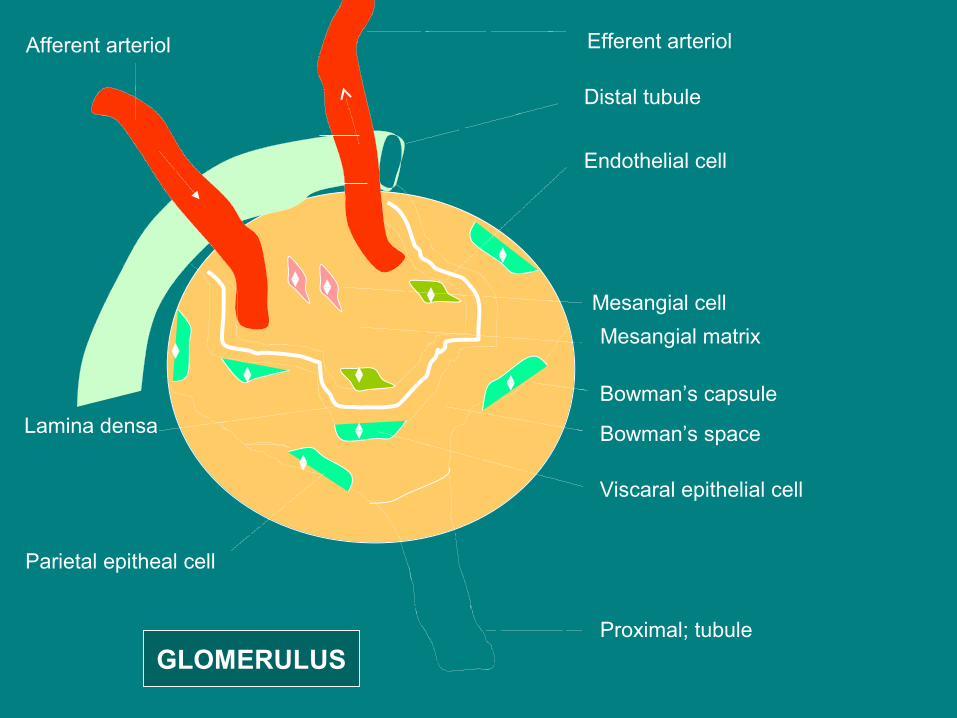
Efferent arteriol
Distal tubule
Endothelial cell
Mesangial cell
Mesangial matrix
Viscaral epithelial cell
Proximal; tubule
Lamina densa
Parietal epitheal cell
Afferent arteriol
Bowman’s capsule
Bowman’s space
GLOMERULUS
Pathogenesis of glomerular diseases
Genetic – • Mutations in exons of DNA• Mutations in the regulatory genes controlling DNA transcription• Abnormal post transcriptional modification of RNA transcripts• Abnormal post translational modifications of proteins
Immunological injury – • AG – Ab – Glomerulus – complement activation – chemtactic and
anaphylatoxin-like factors
Coaglation system activation – • Direct or indirect• Activation of kinin system- chemtactic and anaphylatoxin-like factors

Pathology• Proliferation of glomerular cells –
Generalized – all glomeruli
Focal – some glomeruli
Diffuse – all parts of glomeruli
Segmental – some parts of glomeruli
Endothelial, mesangial cells, mesangial matrix proliferation
Increased glomerular size – norrow the lumens of glomerular
capillaries – renal insufficiency
• Crescent formation in bowman capsule –
Proliferation of parietal epithelial cells
Composition – Fibrin, epithelial cells, BM-like material
macrophages
Fibroepithelial crescent – invasion of connective tissue
Crescent – glomerular cell death – eosinophilic appearance
• Exudation of blood cells –
Neutrophils, eosinophils, basophils, mononuclear cells
• Increase in the width of the BM
• Tubulo interstitial fibrosis –
Injury to the renal tubules – MNC infiltration – soluble factors –
fibrosis – destruction of renal tubules and peritubular capillaries
Pathology

Acute poststreptococcal GN
It is characterized by sudden onset of gross hematuria, edema, hypertension and renal insufficiency
Etiology and epidemiology – • Nephritogenic strains of group-A β hemolytic streptococci –
• Throat serotype – 1,3, 4, 12,25 • Skin serotype – 2, 49, 55, 57, 60 • • Pharyngitis - ( cold weather )• Pyoderma - (warm weather )
Pathogenesis & Pathology
Pathogenesis – Immune complex mediated injury Alternate pathway activation
Pathology - • Light microscopy – All glomeruli enlarged, Bloodless Mesanchymal cell proliferation Mesanchymal matrix proliferation PMN cell infiltration Crescent formation• Immunofluorescence microscopy – Lumpy-bumpy deposits of Ig and complements in BM & mesangium• Electrone microscopy – Electrone dense deposits or ‘humps’ on epithelial side of BM

Clinical manifestations
• Age – 5-12 yrs, uncommon before 3 yrs• Pharyngitis – 1-2 wks• Pyoderma – 3-6 wks• Asymptomatic microscopic hematuria, normal RFT to
ARF• Edema, HT, oliguria, encephalopathy, CHF,nephrotic
syndrome(10 20%)
• Malaise, lethargy, abdominal pain, fever, acute subglottic edema, air way obstruction
• Acute phase – 6-8 wks• Proteinuria and HT – 4-6 wks• Microscopic hematuria – 1-2 yrs
Diagnosis
Normal urine examination -
No cast,except hyaline 1/hpf
RBC – 1-2/hpf
WBC – Male – 0-3/hpf
Female -0-5/ hpf
Epithelial cell few
Bacteria – no organism/oif : unspun
<20/hpf : spun
Urine in AGN –
RBC,
RBC cast,
proteinuria,
PMN cells

Diagnosis
Blood –
Normochromic anemia
C3 level decreased
ASLO – throat infections
2-5 yrs – 120-160 todds unit
6-9 yrs – 240 todds unit
10-12 – 320 todds unit
> 13 yrs - 320 todds unit
DNase B – skin infection
Positive throat culture

Diagnosis
Streptozyme test –
( SLO, DNase B, Hyaluronidase, Streptokinase, NADase )
Renal biopsy –
- ARF
- Nephrotic syndrome
- Absence of evidence of streptococcal infection
- Normal complement level
- Hematuria, proteinuria and low C3 >2 months

Complications
• Hypertension• Encephalopathy• CHF• Hyperkalemia• Hyperphosphatemia• Hypocalcemeia• Acidosis • Seizures• Uremia

Treatment & Prognosis
Treatment –
Diet – Protein, sodium, potassium restricted
Penicillin – 10 days
Fluid restriction
Diuretic
Antihypertensive – CCB, Vasodilators, ACE inhibitors
Prognosis –
95% complete recovery
Recurrences are extremely rare

Membranous Glomerulonephritis
Etiology –
SLE, chronic ITP, neuroblastoma, gonadoblastoma,
syphilis,HBV infection, gold .penicillamine.
Pathology –
LMC – Diffuse thickening of GBM without significant proliferative
changes.
Deposition of membrane-like material by visceral epithelial
cells
Resembles ‘spikes’ on epithelial side of GBM.
IFM – Granular deposits of IgG & C3 on epithelial side.
EMC – Linear staining of IgG,IgA,C3 on tubular BM

Clinical features –
Most common in 2nd decade, nephrotic syndrome (2-6%),
microscopic or gross hematuria, HT (20%).
Diagnosis –
C3 normal except SLE.
Kidney biopsy –
Nephrotic syndrome > 10yrs, Unexplained hematuria and
proteinuria, increased risk of RVT.
Treatment –
Salt restriction, diuretic, prednisone+cyclophosphamide or
chlorombucil
Prognosis –
CRF (20%), Active disease (40%)
Membranous Glomerulonephritis

Pathogenesis – C3 nephritic factors- activates alternative complement pathwayPathology – Type 1 – LMC - most common - Accentuation of lobular pattern - Generalized increased in mesangial cells & matrix - GBM splitting from interposition of mesangial cytoplasm & matrix b/w - endothelial cell and GBM - Formation of crescent IFMC – C3 & lesser amount of Ig in mesangium and along the peripheral capillary in a lobular pattern EMC – immune complex-like deposits in mesangial and subendothelial regionsType 2 – -less common, irregular ribbon-like thickening of GBM, crescent common, splitting rare.
Membranoproliferative (mesangiocapillary) Glomerulonephritis (MPGN)
Type 3 –
Similar to type 1 in LMC & IFMC
EMC – subepithelial and subendothelial
Clinical features –
Most common in 3rd decade, nephrotic syndrome, acute
nephritic syndrome, RFT-normal to decreased, HT.
Diagnosis –
C3 decreased
Renal biopsy – Nephrotic syndrome >10yrs, significant proteinuria
with microscopic hematuria, decreased C3 >8wks.
Treatment –
Long term prednisone EOD
Prognosis –
ESRD (50%), type 2 worst prognosis, recurrent MPGN in kidney
transplant, type 1(13%), type 2(90%)
Membranoproliferative (mesangiocapillary) Glomerulonephritis (MPGN)

SLE Nephritis
Immune complex mediated injury, both T cell and B cell function alteration
WHO classification –
Type 1 – No abnormality
Type 2 – Mesangial lupus nephritis
2a – mild deposit
2b – moderate deposit
Type 3 – FSGN, subendothelial & mesangeal deposits,
necrosis,crescent, sclerosis.
Type 4 – Most common, most severe, diffuse proliferative lupus
nephritis, subendothelial & mesangeal deposits, ‘wire loop
lesions’ necrosis,crescent, sclerosis.
Type 5 – Membranuous lupus nephritis, least common, resembles
membranuous GN except mild to moderate mesangial
proliferation, decreased C3 level.

Clinical features – • Adolescence , female• All type 2 and some type 3 – hematuria, normal RFT, proteinuria <1g/day.
• Some type 3 and all type 4 - hematuria, decreased RFT, proteinuria, nephrotic syndrome, ARF
• Type 5 – nephrotic syndrome.
Diagnosis –
ANA, antibody to double stranded DNA, C3-C4 level decreased.
Treatment – • All patients – prednisone 4-6 months• Type 3 & 4 – 6 monthly IV cyclophosphamide 500-1000mg/m2 followed by
every 3 monthly dosing for 18-36 months.
• Type 1 & 2 – azathioprine single dose daily, 1.5-2mg/kg/day
Prognosis –
Highest risk of progression in type 4
SLE Nephritis

Henoch-schonlein purpura nephritis
Pathology and pathogenesis – • Immune complexes containing IgA1 deposition within the capillaries of the
skin, intestine and glomerulus.• Crescent formation more common and extensive
Clinical manifestations – • 1-3 wks after URI• Gross hematuria (20-30%),• Isolated microscopic hematuria• Hematuria and proteinuria
• Acute nephritic syndrome• Nephrotic syndrome• Renal insufficiency• Ureteritis
Prognosis –
Best - Isolated microscopic hematuria
Poor - Acute nephritic syndrome, Nephrotic syndrome

Rapidly Progressive (crescentic) GN Classification –
1. Immune comlex mediated GN – PSGN, MPGN, lupus, HSP and IgA nephritis.
2. Anti-GBM mediated GN – Goodpasture disease.
3. ANCA mediated GN –Microscopic PAN, Wegner granulomatosis.
Crescent formation.Goodpasture disease – -Pulmonary hemorrage and GN with antibody against type 4 collagen of alveolar BM and GBM. -Continuous linear pattern of IgG along the GBM. Diagnosis –
ANA, Normal C3, anti DNase B,
ANCA to MPO or proteinase-3
Treatment -
According to cause
THANKS





























