Embed Size (px)
Citation preview

Work related musculoskeletal disorders elbow
Dr.Rajeshwari JindalProfessor(Department of PMR)
SMS Medical College Jaipur

Definition
Musculoskeletal disorder (MSD) is an injury or disorder of the muscles, nerves, tendons, joints, cartilage, and spinal disc.
Chronic disease related to manual tasks Source of significant pain, disability and disadvantage
for the injured person and a substantial burden on modern societies.
Statistics suggest that more than 30% of all occupational injuries are musculoskeletal injuries associated with manual tasks (Straker et. al. 2004).

Globally, musculoskeletal conditions are one of the leading causes of morbidity and disability, giving rise to enormous healthcare expenditures and loss of work (WHO 2003), and reducing the quality of life of affected employees and their families.

Work related musculoskeletaldisorders (WMSD)Various synonyms of WMSD – Repeated strain injury Cumulative trauma disorder Over use syndrome
Due to repeated straining body tissue and not allowing enough time to heal are believed to cause progressive discomfort, pain, and ultimately disability to continue regular work.

5
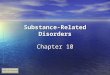
Cumulative Trauma Cycle
irritation to tissue
microtrauma (small tears)
produces scar tissueKeeps repeating
as long as activity continues
Activity
results in: flexibility strength function
adhesions form
adhesions coalesce

6
Risk Factors for Musculoskeletal Disorders
Excessive force Awkward and/or prolonged postures Repetition Direct Pressure Temperature Extremes Vibration Non occupational factor : fitness,
mental status, smoking, hormonal disorder etc

7
Excessive Forces
Common risky problems:• Lifting and carrying• Pushing and pulling• Reaching to pick up
loads• Prolonged holding• Pinching or squeezing

8
Awkward PosturesCommon risky postures: Working overhead Kneeling all day Reaching to pick up loads Twisting while lifting Bending over to floor/ground Working with wrist bent

9
Contact Stress/Poorly Designed EquipmentCommon equipment problems to watch for: Does not have a good grip Too heavy Hard to use Uncomfortable Bad condition Wrong tool/equipment for the job

10
Vibration
Can lead to injury when you are: Using reciprocating tools Using grinding or impact tools Using vibrating tools Working in or on motorized vehicles

Causes of WRMSD How does a musculoskeletal injury occur? Basically, thousands of forceful, awkward and repetitive
movements produce trauma to muscles, tendons and ligaments which eventually leads to pain, inflammation, swelling and deterioration of tendons and ligaments.

12
An Activity is Likely to Become an InjuryWhen:
You perform the activity frequentlyYou do the activity a long time
The work intensity is high
There are a combination of factors

Symptoms of WMSDs?
DiscomfortPainNumbness
BurningSwellingChange in color
.
TinglingTightness, loss of flexibility.

Elbow
Tennis elbow – Lateral epicondylitis Golfer’s elbow – Medial epicondylitis Cubital tunnel syndrome. Bursitis – inflammation of bursa (fluid filled
sacs) Distal bicep tendinitis , tricep tendinitis Pronater teres syndrome

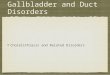
Lateral epicondylitis
15

Causes Tennis elbow is a type of repetitive strain injury, resulting from tendon overuse and failed healing of the tendon. In addition, the extensor carpi radialis brevis muscle plays a key role.

Occupational classification Lateral epicondylitis may be provoked by an exercise involving repeated and forcible extension movements at the wrist. The following three types of occupational group are classified respect to elbow stress Type 1: No or little stress on the elbows
( Driver. Instructor, Office worker, clerk, security guard).
Type 2: Moderate stress on the elbows (e.g. inspectors, electricians. repairmen, unpacker, toolmaker).
Type 3: Heavy stress on the elbows (e.g. Blaster, driller, polishers, welders, carpenter)

Signs and symptoms
Pain tenderness on the outer part of the elbow (lateral epicondyle)
Pain from gripping and movements of the wrist, especially wrist extension and lifting movements
e.g. pouring a container of liquid, lifting with the palm down, sweeping, especially where wrist movement is required

Diagnosis With the elbow fully extended, the patient feels points
of tenderness over the elbow pain with passive wrist flexion and resistive wrist extension (Cozen's test).
Pain with Resisted middle finger extension might indicate the involvement of Extensor Digitorum also.

Treatment
Conservative. Rest, Ice, compression and elevation NSAID Physical therapy, occupational therapy,
orthotics or braces may also be useful. Steroid injections Laser therapy,prolotherapy,us

Counterforce orthosis
Wirst extensor orthosis reduces the overloading strain at the lesion area.
Orthosis is a device externally used on the limb to improve the function or reduce the pain.

Both eccentric loading and extracorporeal shockwave therapy are currently being researched as possible treatments for tendinosis.
Other treatments for which research is on-going includes Platlet Rich Plasma (PRP), and stem cell injections.
Operative treatment

Golfer's elbow
tendinosis of the medial epicondyle of the elbow. Tenderness over the origin of the flexor pronator mass Resisted pronation and/or wrist flexion will reproduce
symptoms in most affected patients Grip strength is decreased in patients with medial
epicondylitis compared with control subjects, although the magnitude of impairment is less than that seen in patients with lateral epicondylitis

The pathogenesis of medial epicondylitis parallels that of lateral epicondylitis, beginning with repetitive microtrauma to the wrist flexors originating at their origin on the medial epicondyle.
The muscles most commonly involved include the pronator teres and flexor carpi radialis but can include any of the other flexor.
Seen in overhead throwing sports,or in occupations requiring repetitive forearm pronation and wrist flexion eg carpenters

Non-specific palliative treatments include: Non-steroidal anti-inflammatory drugs Heat or ice A counter-force brace or "elbow strap" . Therapy for muscle/tendon reconditioning,
starting with stretching and gradual strengthening of the flexor-pronator muscles.
Strengthening slowly begin with isometrics and progresses to eccentric exercises helping to extend the range of motion back to where it once was.

Distal biceps tendonitisDiagnosis: sudden and unexpected forceful extension
against a flexed elbow, or a pop is felt during heavy lifting. Complete ruptures commonly result in Popeye deformity in the upper arm.
Flexion and supination of the elbow are painful and strength is noticed to be decreased in the affected extremity
Magnetic resonance imaging (MRI) helpful diagnostic tool for the diagnosis of a partial tendon rupture

Risk factor More common in male, dominant limb Smoker,chronic steroid use. Occupations with repetitive forearm
motion(plumbers,laborers and athletes)

Treatment
Partial ruptures and tendinosis can be managed with nonoperative options and physical therapy, but early surgical repair is recommended for complete ruptures with postoperative physical therapy.

Triceps Tendonitis Triceps tendinosis is a chronic condition
stemming from overuse and repetitive heavy lifting. Patients routinely describe pain and/or weakness with activities of elbow extension.
Tenderness to palpation occurs at the triceps insertion on the olecranon.
In the setting of chronic repetitive injury, plain radiographs may reveal a traction osteophyte on the olecranon.

Treatment
Nonoperative activity modification, nonsteroidal anti-inflammatory medications, and physical therapy for stretching and ROM ex
Operative management, consisting of olecranon osteophyte excision and triceps repair, is reserved for refractory cases that fail conservative management.

There are several recommendations regarding prevention, treatment, and avoidance of recurrence that are largely speculative including stretches and progressive strengthening exercises to prevent re-irritation of the tendon.

Olecranon bursitis

Olecranon bursitis ( "Smiles' elbow", "elbow bump", "student's elbow", "Popeye elbow", "baker's elbow" or "gamer's elbow"), Characterized by pain, redness and swelling
around the olecranon, caused by inflammation of the elbow's bursa. This bursa is located just over the extensor aspect of the extreme proximal end of the ulna.

Bursitis normally develops as a result either of a single injury to the elbow (e.g., a hard blow to the tip of the elbow)
Repeated minor injuries, such as repeated leaning on the point of the elbow on a hard surface.
Job or hobby involves a repetitive movement (e.g., tennis, golf, or even repetitive computer work involving leaning on one's elbow)

`Non-surgical treatments Icing, a firm compression bandage, and
avoidance of the aggravating activity,NSAIDs .
Treatment for more severe cases may include aspiration of the excess bursa fluid
hydrocortisone injection . In case of infection, the bursitis should be
treated with an antibiotic.Surgical treatments

Pronator syndrome
Compression of the median nerve in the region of the elbow or proximal part of the forearm
Pain and/or numbness in the distribution of the distal median nerve
weakness of the muscles innervated by the anterior interosseous nerve: the flexor pollicis longus the flexor digitorum profundus of the index finger and the pronator quadratus.

Causes
The most common cause is entrapment of the median nerve between the two heads of the pronator teres muscle. Other causes are compression of the nerve from the fibrous arch of the flexor superficialis, or the thickening of the bicipital aponeurosis.
Jobs requiring repeated pronation or supination,lifting, carrying,or placing heavy objects.

Clinical signs Tenderness over the proximal median nerve,
which is aggravated by resisted pronation of the forearm and resisted middle finger flexion.
The flexor pollicis longus and FDP of the index finger are weak.
Sensory changes may be found in the first three fingers as well as in the palm, indicating impairment of the median nerve proximal to the flexor retinaculum.

Treatment
Anti-infammatory medication Injection of corticosteroids into the
pronator teres muscle. Stretching and strengthing ex Massage therapy Surgical decompression can provide benefit
in selected cases.

Diagnosis Conduction velocity of the median nerve
in the proximal forearm may be slow but the distal latency and sensory nerve action potential at the wrist are normal.
MRI may show denervation atrophy of the affected muscles
EMG or the MRI are abnormal for the pronator teres muscle and the flexor carpi radialis, this implies that the problem is at or proximal to the elbow

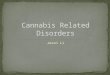
Cubital tunnel Syndrome
The cubital tunnel is a channel which allows the ulnar nerve to travel over the elbow. It is bordered by the medial epicondyle of the humerus, the olecranon process of the ulna and the tendinous arch joining the humeral and ulnar heads of the flexor carpi ulnaris.
Chronic compression of this nerve is known as cubital tunnel syndrome, a form of repetitive strain injury akin to carpal tunnel syndrome.


chronic compression or repetitive trauma Sleeping with the arm folded behind neck,
elbows bent. Pressing the elbows upon the arms of a chair
while typing. Resting or bracing the elbow on the arm rest
of a vehicle. Bench pressing. Intense exercising and strain involving the
elbow.

Ulnar nerve entrapment at the medial aspect of the elbow, causing medial elbow pain and paresthesias in the ring and little finger.
This occurs through repetitive activity requiring flexion or extension of the elbow against resistance.

45
Break the Injury Cycle
Fatigue
Discomfort
Pain
Injury
Disability
re-injury may be
likely

Definition of ergonomics
“Ergonomics is the science and practice of designing jobs and
workplaces to match the capabilities and limitations of the human body.”
Simply put:“fitting the job to the worker”
The goal of ergonomics is to create jobs, tools, equipment and workplaces that fit
people, rather than making people adapt to fit them.

Ergonomic Prevention Approach Engineering approach – Analyze the job it
detail. Various posture evaluation schemes can be used for rough estimation of joint deviation, repetition/duration, and forces involved.
They provide scores for action limit and maximum limits, by which jobs can be selected for improvement.
Internal joint forces can be evaluated by EMG, biomechanical models.

Solution approaches are mechanization, job enlargement, redesign the workstation for adjustability and better working posture, better method to do the work to reduce force, duration, repetition.
Administrative approach – Job rotation, use of part time workers, exercises, stress reduction.

Examples of engineering solutions Counter balance and suspend hand tools -
reduce static load of holding the tool. Tilt the work surface - facilitate better
posture, viewing, reach. Provide hand tools with correct grip
style/diameter/texture – reduce gripping force, improve wrist posture
Maintain sharpness of the knives – reduce force required to cut Hand tools are properly maintained - reduce vibration

More of engineering solutions Use correct work height – better upper body
and hand-arm posture ,Limit reaching motions to minimum
Lower the work area if shoulders needed to be lifted
Provide arm rest if elbows are needed to be raised – reduce static load at shoulder
Consider sitting/standing/sit-stand work posture – reduce static load in lower back
Arrange workplace to minimize twisting, forward or lateral bending – reduce harmful posture of torso
Correct viewing angle - minimize static load on neck muscles, eye strain.

Arrange work to avoid unnecessary motions. Let power tools and machinery do the work. Spread repetitive work out during the day. Take stretch pauses Rotate task with co-workers if possible Change hands or motions frequently
Reducing repetition

Benefits of ergonomicsErgonomics helps to prevent injuriesErgonomics has other benefits
Reduced fatigue and discomfortIncreased productivityImproved quality of workImproved quality of life

53
Conclusions Cumulative trauma occurs over time Applying ergonomics = injury prevention Understand injury risk factors Some situations may have little room for improvement,
but with others you have the control to improve:equipment work practicesbodymechanics

THANK YOU!