Embed Size (px)
Citation preview

VESICO URETERIC REFLUX
AN OVERVIEW

VESICO URETERIC REFLUX
Dr.B.SELVARAJ MS;Mch; FICS;
NEONATAL & PEDIATRIC SURGEON
SVMCH & RC
PONDICHERRY- 605102 INDIA
S
V
M
C
H

VESICO URETERIC REFLUX
Definition & Etiology
Pathophysiology & Clinical Features
Appropriate investigations
Management - Medical & Surgical
OBJECTIVES
S
V
M
C
H

DEFINITION
S
V
M
C
H
Retrograde flow of urine from bladder into upper urinary tract due to incompetent VU Junction
VUR is important because of it’s association with renal dysfunction & parenchymal scarring in UTI

VESICO URETERIC REFLUX
General pediatric population 1 to 2% only
In children with UTI 30 to 50%
30 to 60% of children with VUR have renal scarring
Female: Male ratio= 5:1
Incidence
S
V
M
C
H

Anatomy of VU Junction
Ureter continues as superficial trigone
Waldeyer’s fascia continues as deep trigone
S
V
M
C
H

Paquin’s Urophysiological Law
Urophysiological Law: Submucosal tunnel ureteric length: diameter of ureter should be 5:1
If the ratio is below�Reflux
If the ratio is above�Obstruction S
V
M
C
H

Stephen’s Ureteral Bud Theory
S
V
M
C
H

ETIOLOGY
Primary or Congenital
Lateral ectopy of ureter
Posterior urethral valve
Congenital Neuropathic bladder
Congenital urethral stricture
Secondary or Iatrogenic
Ureteral meatotomy
TURP & TURT
Unroofing of Ureterocele
Failed ureteral reimplantation
S
V
M
C
H

Pathophysiology
VUR�High pressure urine into ureters & Kidneys
Stasis of urine because of postvoidal residual urine
Stasis of urine good nidus for superadded infection
Refluxed infected urine�Pyelonehritis�Renal scarring�Reflux uropathy�ESRD
Reflux,UTI & Pyelonephritis scarring�Well known Triad in Pediatric urology
S
V
M
C
H

VESICO URETERIC REFLUX IRSC Grading
S
V
M
C
H

VESICO URETERIC REFLUX
IRSC Grading
S
V
M
C
H
Clinical Features
In Neonates & Infants usally asymptomatic or 1 or 2 attacks of UTI � Failure to thrive
Fever, chills and costovertebral tenderness in acute pyelonephritis
In cases of obstruction or neurogenic bladder �Palpable hydronephrotic kidney or distended bladder
In oldery chidren� Urgency, frequency and incontinence of urine
S
V
M
C
H
VESICO URETERIC REFLUX
USG abdomen
MCU or VCUG
DMSA Scan & NVCUG
Cystoscopy
INVESTIGATIONS
S
V
M
C
H
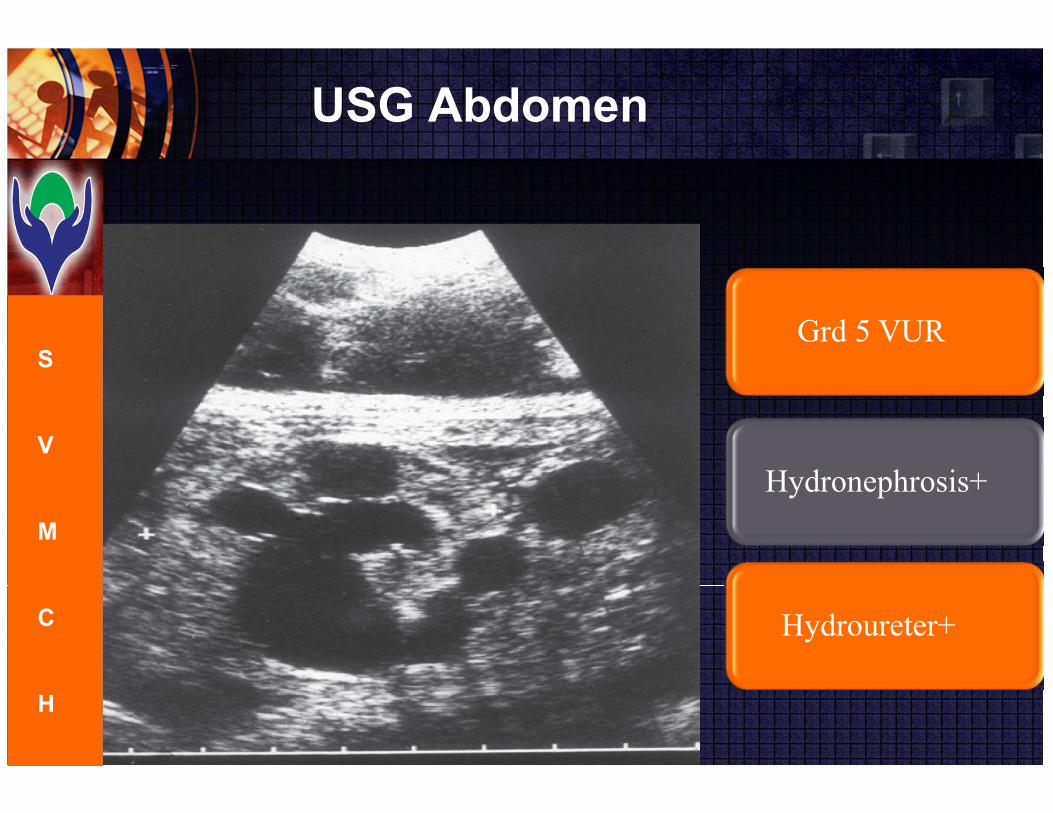
USG Abdomen
Grd 5 VUR
Hydronephrosis+
Hydroureter+
S
V
M
C
H

MCU or VCUG
Gd 1 VUR
Lt VUR Gd 1
S
V
M
C
H

MCU or VCUG
Gd 2 VUR
Bilateral VUR Gd 2
S
V
M
C
H
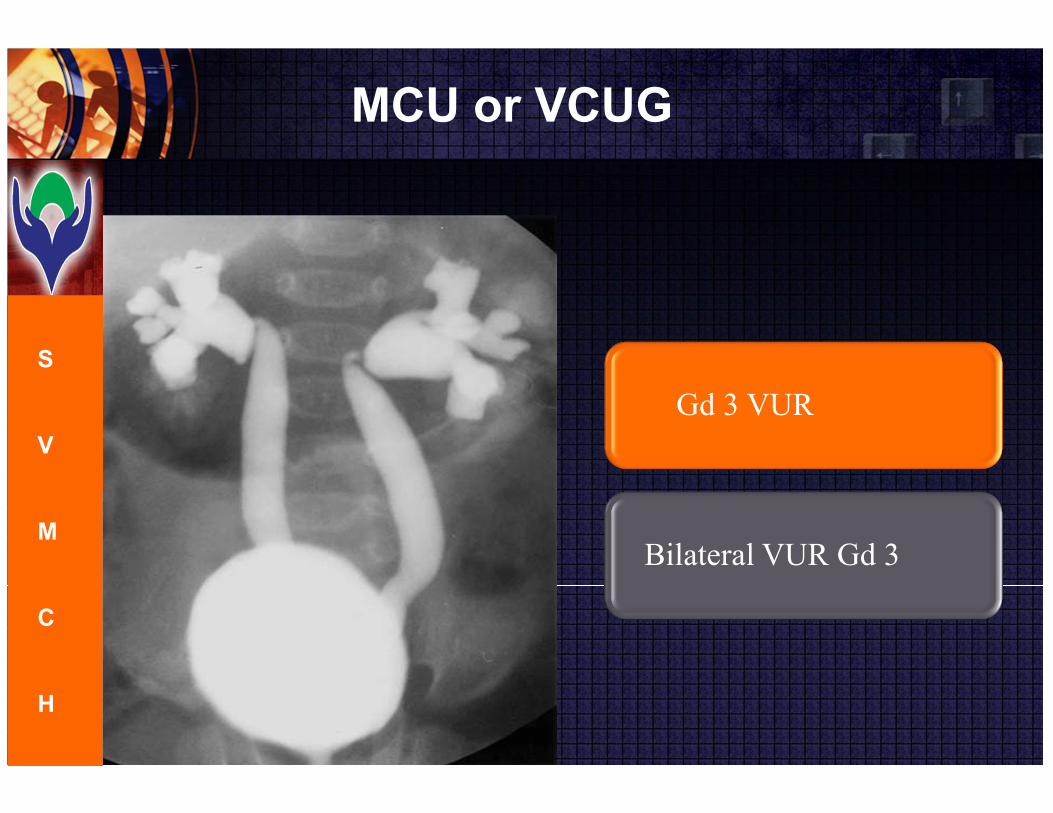
MCU or VCUG
Gd 3 VUR
Bilateral VUR Gd 3
S
V
M
C
H
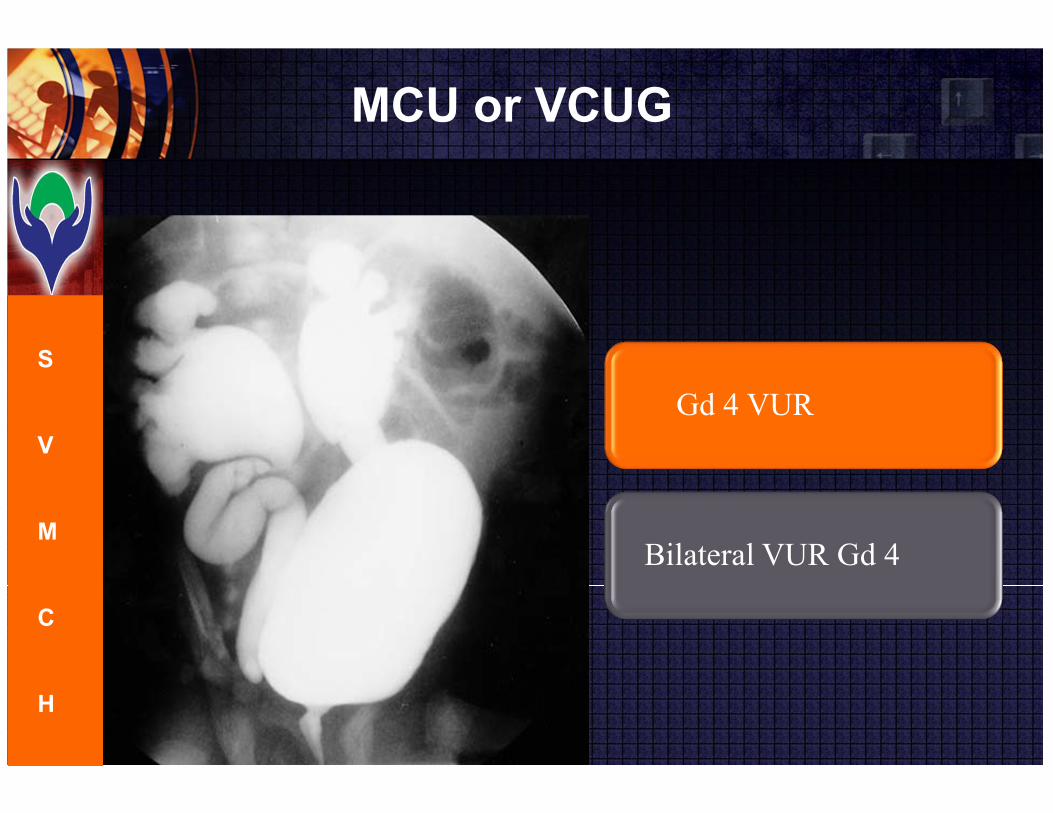
MCU or VCUG
Gd 4 VUR
Bilateral VUR Gd 4
S
V
M
C
H

MCU or VCUG
Gd 5 VUR
Bilateral VUR Gd 5
S
V
M
C
H

PUV with VUR
Gd 4 VUR
PUV with VUR
S
V
M
C
H

Neurogenic Bladder with VUR
Gd 3 VUR
Neurogenic Bladder+
VP shunt+
S
V
M
C
H
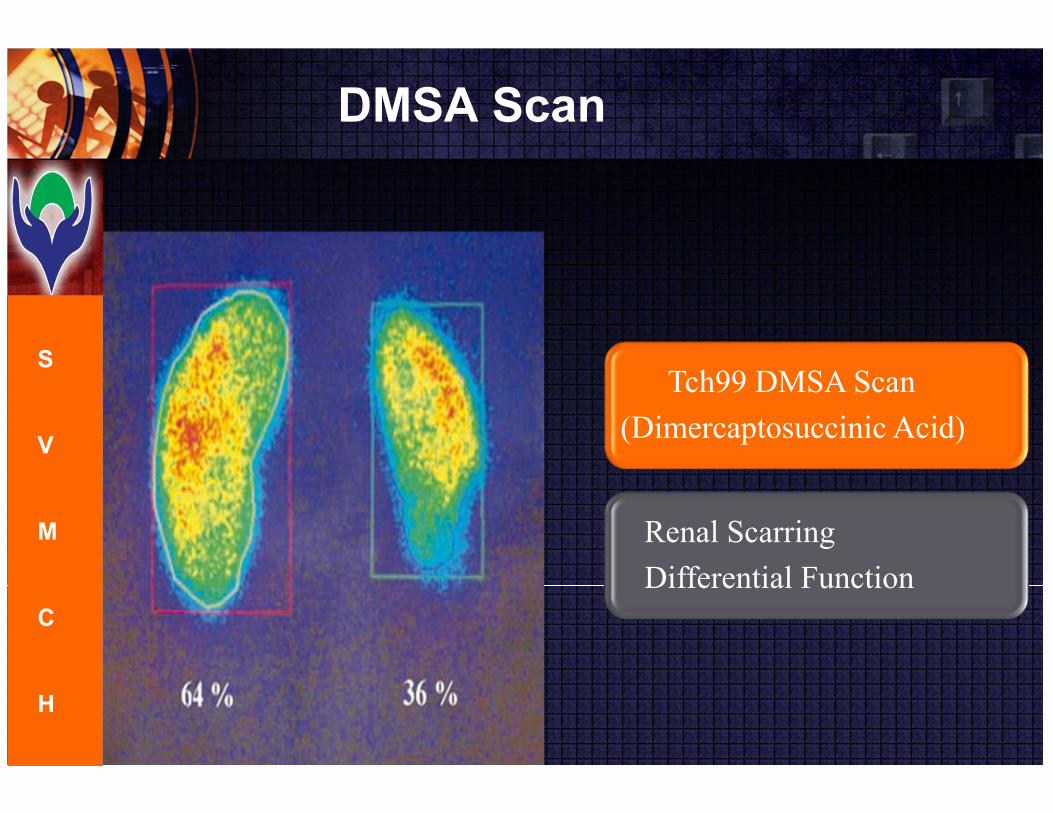
DMSA Scan
Tch99 DMSA Scan
(Dimercaptosuccinic Acid)
Renal Scarring
Differential Function
S
V
M
C
H

NVUCG
Tch 99 Sulfur colloid VCUG
Grading not possible
Suitable for F/U
S
V
M
C
H
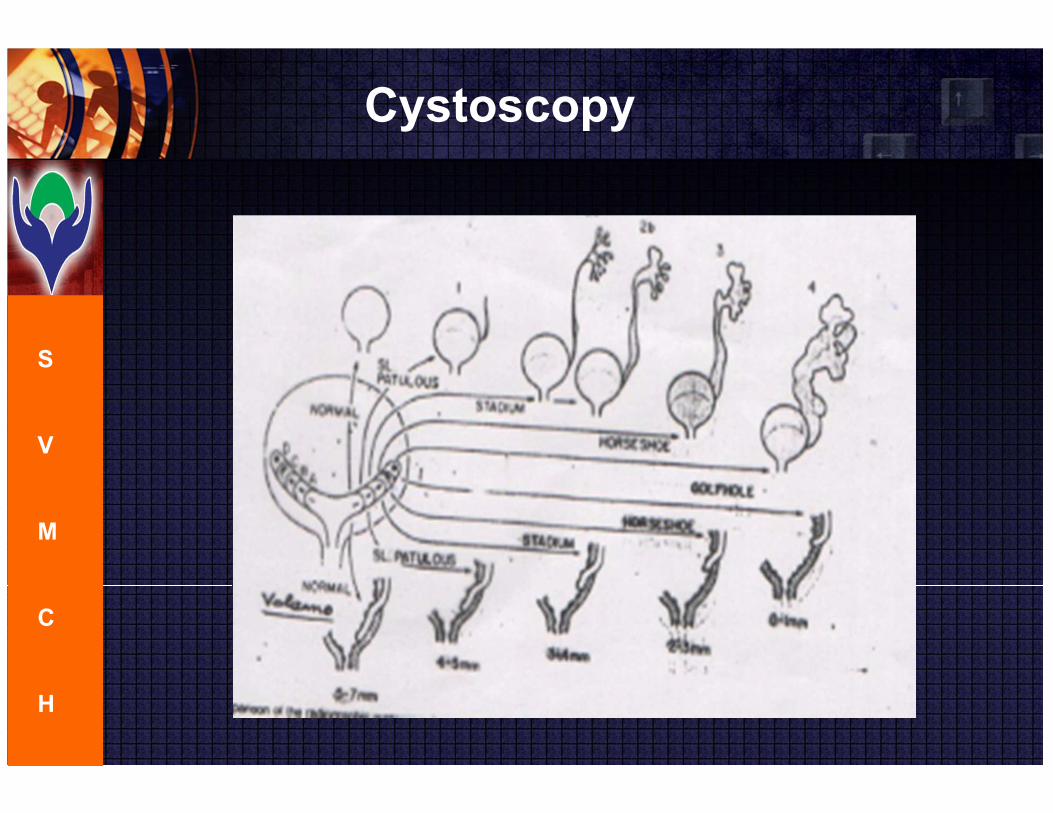
Cystoscopy
S
V
M
C
H

Management- Conservative
S
V
M
C
H
In Gr 1,2&3 Primary VUR
Triple micturition with 2mts interval
Intermittent Antibiotics whenever surveillance culture+ve
In Gr 1,2&3 VUR with LUTO
Clean intermittent catheterisation
Eliminates residual urine & intravesical pressure
Intermittent Antibiotics whenever surveillance culture+ve
Conservatively treated patients should undergo regular VCUG to
R/o failure of treatment

Indications for Surgery
Absent intravesical submucosal tunnel� Lateral ectopic ureter
Persistent or recurrent UTI despite antibacterial prophylaxis
Progressive renal scarring
Renal growth arrest
S
V
M
C
H

Indications for Surgery
Poor patient & parental compliance with non op treatment
Persistent ipsilateral reflux following corrective surgery
Failure of submucosal tunnel growth for 2 to 4 yrs
Intra Renal Reflux Gr 5
S
V
M
C
H

Endoscopic Sting Procedure
S
V
M
C
H

Endoscopic Sting Procedure
S
V
M
C
H

Endoscopic Sting Procedure
S
V
M
C
H

Endoscopic Sting Procedure
S
V
M
C
H

Principles of Antireflux Surgery
S
V
M
C
H
Never a surgical emergency� so urine should be sterilised first
Intravesical ureter newly reconstructed must be compressible
It should be adequately supported posteriorly by detrusor muscle
Intravesical ureter length should be atleast 5 times it’s diameter
� Paquin’s urophysiological Law
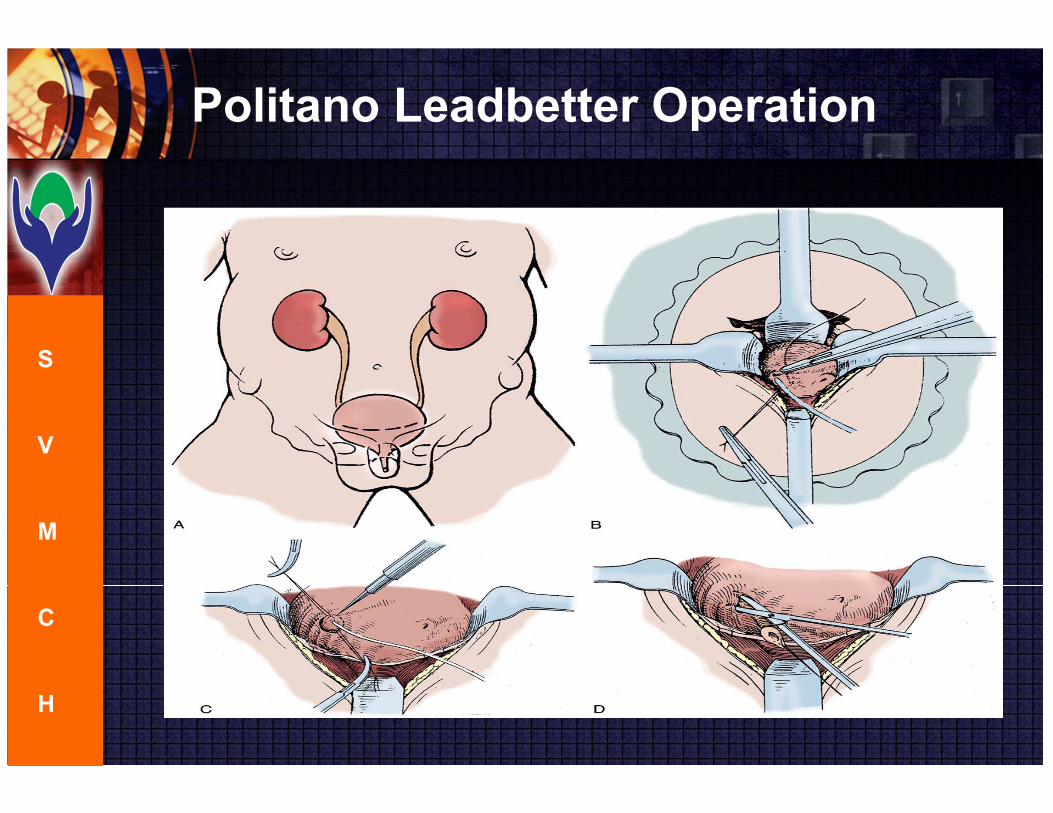
Politano Leadbetter Operation
S
V
M
C
H
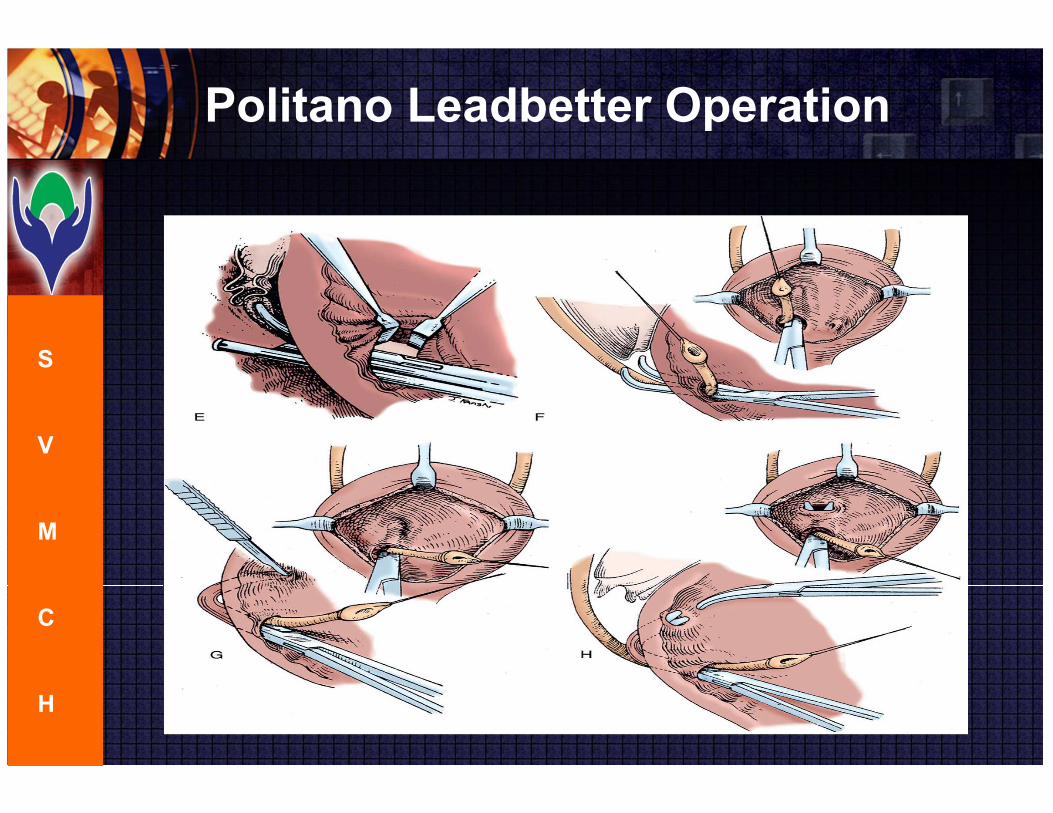
Politano Leadbetter Operation
S
V
M
C
H

Politano Leadbetter Operation
S
V
M
C
H
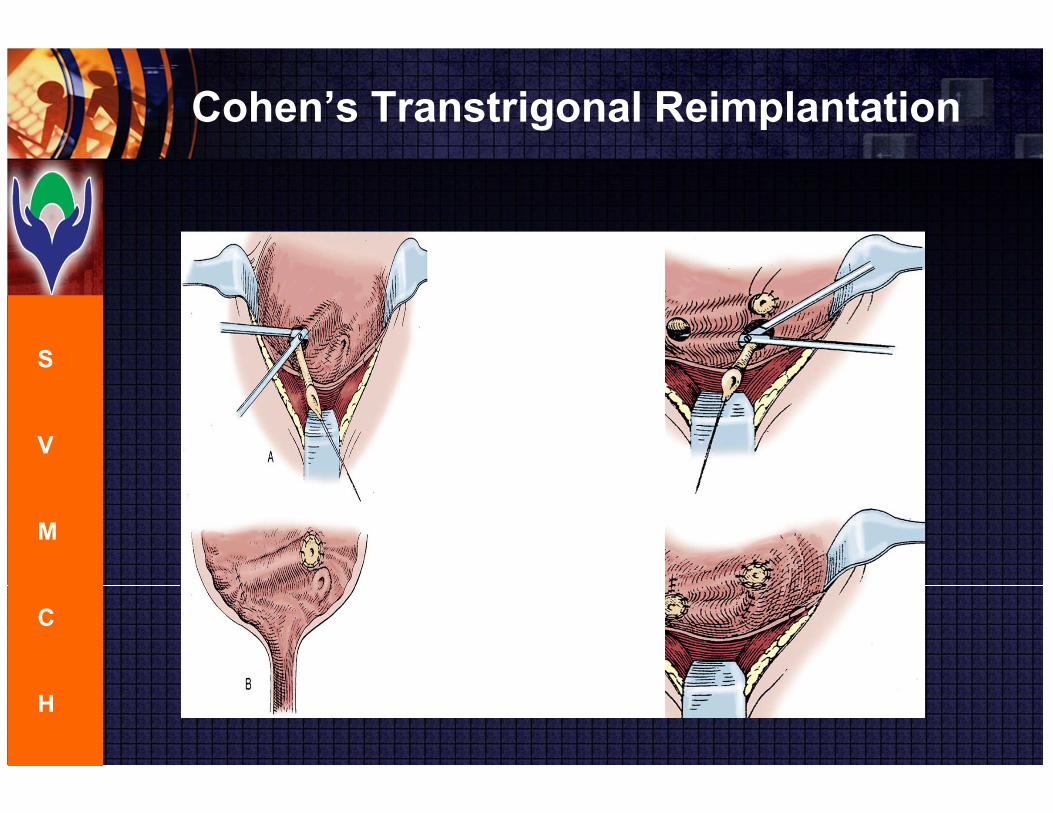
Cohen’s Transtrigonal Reimplantation
S
V
M
C
H
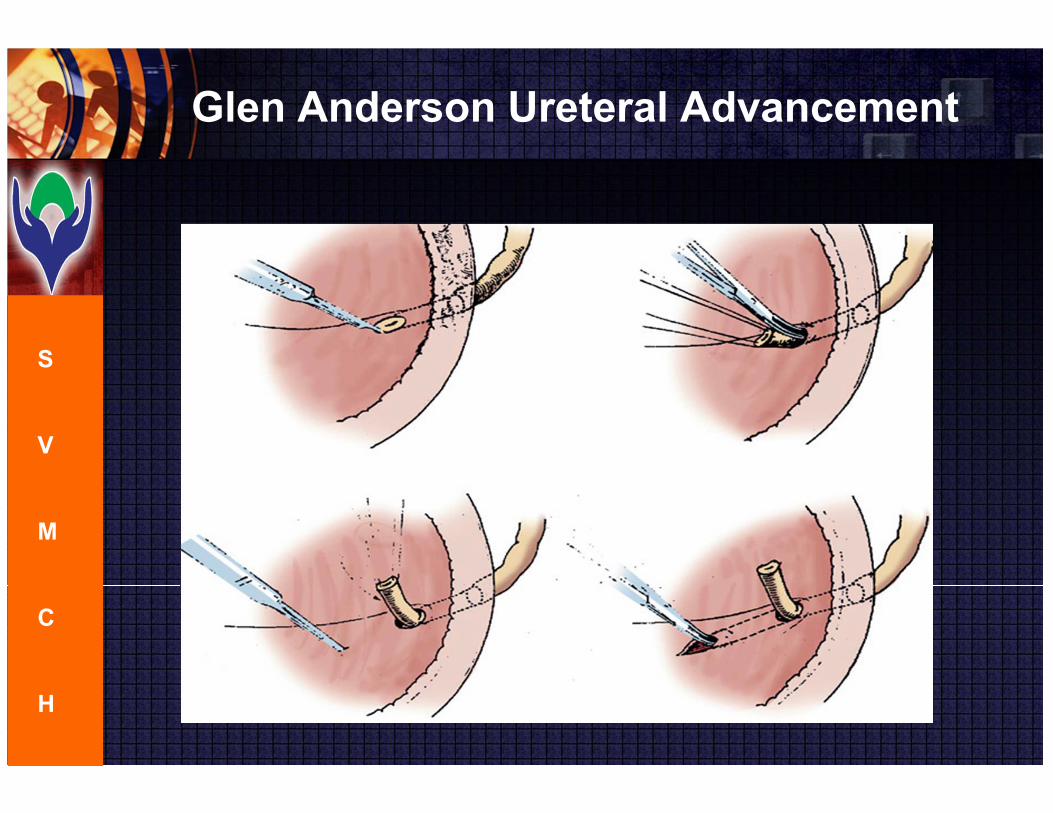
Glen Anderson Ureteral Advancement
S
V
M
C
H

Lich- Gregoir Operation
S
V
M
C
H
Complications after Surgery
S
V
M
C
H
If ureteric hiatus in bladder wall is too wide� Paraureteric Vesical Diverticulum develops
Ureteric stenosis because of ureteric ischemia
Contralateral reflux�division of ureterotrigonal attachment on one side relaxes insertion of opposite ureter
Intravesical ureter length should be atleast 5 times it’s diameter
� Paquin’s urophysiological Law�If not followed recurrence

VESICO URETERIC REFLUX
S
V
M
C
H

TAKE HOME MESSAGE
Male children with one episode of UTI and female children with 2 or more episodes of UTI should be thoroughly investigated to rule out possibility of VUR
In children with repeated episodes of UTIs should do DMSA scan to find out the differential function of both kidneys and to rule out any renal scarring
Treatment options are conservative antibiotic prophylaxis,Endoscopic Sting Procedure or open/Laparoscopic Antireflux surgeries which sould be tailor made for each patient
S
V
M
C
H






























