Embed Size (px)
DESCRIPTION
Citation preview

9/5/2013
1
UNICEF: the equity agenda
and vaccines
Rockville
5 September 2013
Planning for Adult Vaccination in Middle and Low Income Countries,
HIV, TB, and Malaria WorkshopThomas O’Connell, UNICEF NY
Significant progress toward MDG 4, but we’re fast approaching 2015: opportunity to accelerate progress towards MDG4 and sustain the momentum beyond 2015
Despite significant progress, challenges remain – variable progress across regions, populations, and specific causes of mortality requires targeted, high-impact interventions
New data insights, effective technologies, and country innovations enable a sharper, more strategic focus on the countries, diseases, and populations with the highest burden of under-five mortality

9/5/2013
2
Deaths among children under 5 globally;
19,000 die every day from preventable causes
35%
7%
18%11%
5%
2%
2%
1%
18%
•12.4 M
7.6 M
2000
2010
Annual U5 deaths
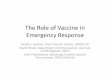
Specifying mortality impacts of inequity...and hence key interventions for scale up
40.7 26.9
50
11
56.3
22.1
6.6
36.7
13.9
4.9
21.6
8.8
0
50
100
150
200
250
Nigeria: Nigeria Q1 Nigeria: Nigeria Q5 (richest)
Under Five Mortality Rate (per 1000 Live Births) in Nigeria
Others
Injuries
AIDS
Pneumonia
Measles
Malaria
Diarrhea
Neonatal
Poorest wealth quintile Richest wealth quintile

9/5/2013
3
Richest 20%
Poorest 20%
Poor, rural Hausa girls
Rich, rural girls
Poor, urban boys
Poor, rural girls
Nigeria
Rural Hausa
Rich, urban boys
Urban
Rural
Urban
Rural
Rich, rural boys
C. A. R.
Chad
Bangladesh
Cameroon
Honduras
Indonesia
Bolivia
Cuba
Ukraine
0
2
4
6
8
10
12
14
Av
era
ge
nu
mb
er
of
ye
ars
of
sch
oo
lin
g
Education poverty
Extreme education poverty
3.3 years
6.4 years
3.5 years
9.7 years
0.5 years
10.3 years
2.6 years
0.3 years
Boys
Girls
6.7 years
10 years
Multiple causes of deprivation (inequity)E.g. Wealth, education, geographic location, and gender inequity in Nigeria
Source: SOWC 2012
Identifying where deprived populations liveUsing district level coverage and outcome “tracers” to identify key districts
88
79 79
7369 68
56 5450
13
20
11 1116
25
34
16
24
0
10
20
30
40
50
60
70
80
90
100
% Full Immunization Coverage
(12-23 months)
% Underweight Children
(6-59 months)
Childhood immunization and nutritional status (%), Uganda
District

9/5/2013
4
Shifting the curve: Hib vaccine introduction
Source: The Lancet 2012; 380:1341-1351 (DOI:10.1016/S0140-
6736(12)61378-6)
Acting upon the data collected –Three strategies to shift the curve, and narrow equity gaps
Narrowing the equity gapsReorienting towards pro-equity delivery and demand
8
1. Delivery
system
2. Demand
Empowerment
3. Legislation &
Policy changes

9/5/2013
5
Shifting the curve: new products, policies and knowledge
Vaccines are essential to equity and child survival
Opportunity
� Unprecedented global support to introduce additional vaccines that target thegreatest killers, which are increasingly concentrated in the poorest, mostmarginalised groups
� Mobilised vaccine industry
� Strong partnership forums , in particular GAVI Alliance Partners
Challenges
� Countries face increased financial burden: higher priced vaccines & increased GAVIAlliance co-financing requirements
� Delivery and logistical challenges as fragile infrastructures are further challengedby more vaccines
� Fragile vaccine industry and constrained supply for most vaccines
� Competition from other priorities for limited funding
Source: 2012 country forecasts received by UNIICEF
Immunization Supplies
VaccinesBCG , DTP, TT/Td/DT, Measles containing, OPV, HepB, YF, DTP-HepB, DTP-HepB/Hib, DTP/Hib, Hib, MR, Meningitis, MMR, PCV, RV IPV, etc.
Safe Injection equipment
Cold Chain Equipment
Vaccines Supplies: US$ 1, 053 million1.895
billion doses
1,946
shipments2012
Countries UNICEF procures
on behalf of
Full schedule
Partial schedule
UNICEF has a key role in vaccine procurement, procuring immunization
supplies on behalf of around 100 countries annually
Source UNICEF Supply Division

9/5/2013
6
UNICEF annual vaccine procurement has increased significantly since
2000 supporting UNICEF Programmes and on behalf of Partners,
Global Programmes, Governments and NGO’s
The arrows indicate the main programme drivers for the increased procurement value.
Source UNICEF Supply Division
Recent increases in value driven by new
vaccine introduction
2010: de Decrease due to price reductions and India self-
self-procurement (OPV), supply shortfalls
Campaign Activities (Polio, Mea), New
vaccine introduction (GAVI) Price
increases, Boosting routine activities
PCV
Penta
OPV
Vaccine Production:
highly regulated and complex, with inherent risks
Product/ Production Profile Impact
Biological products Significant risks of production failures; require
multiple suppliers
Quality is the OVER-RIDING criterion Only WHO pre-qualified vaccines procured;
requiring significant investment and
continuous oversight. Limits the supply base
Highly regulated production
environment
New regulatory requirements can cause
interruptions
Dependency on well functioning NRA Outside of the control of the manufacture –
risk; requires a diverse supplier base
Limited shelf life Quantity and Timing of Forecasts is key
Temperature controlled storage
requirements
Requires to be maintained through to delivery
to the child.

9/5/2013
7
UNICEF’s procurement strategies seek Vaccine Security:
sustained, uninterrupted supply of affordable vaccines, of
assured quality.
Number of qualified suppliers
Price
Pipeline
Availability vsDemand
Major Dependen-
cies
Supply interruptions
UNICEF SD develops strategies to achieve healthy market
objectives within each diversified market situation
• Increasing complexity within procurement as new products become
available
• Competition with high-income markets for production allocation
• Demand reacting to changes and developments in immunization
programmes, vaccine development and funding speculation
• Country preferences on presentation and formulation
• Requires balancing with financial sustainability
• Need for increased flexibility on tendering strategies, maintaining long
time horizons and providing for market flexibility

9/5/2013
8
Forecast
Pentavalent vaccine supply has been impacted by a number of supply interruptions, impacting supply availability and resulting in multiple low volume shipments to maintain supply across all countries
Supply start
De-listing
Suspension
Each instance requiring: Work with WHO QSS, close follow up with manufacturer, work with countries affected or planned ot be supplied from the
interruptions, contingency modeling and planning; internally, with countries and with partners. Communication to market and organization, prepare
press responses etc.
Continued fragile market; since 2010, 2 manufactures with pentavalent vaccines have had their vaccines delisted and 2 new manufactures have
entered with new pre-qualified vaccines. Good response from other suppliers to meet the gaps
Has taken a toll on countries – changes in vaccines, shipment-plans, depleting country stocks
Important: while disruptive, voluntary suspensions of shipments are evidence of functioning QAC and action by manufacturers
Examples of diverse vaccine markets

9/5/2013
9
Forecasts are at the foundation - translating need into funded
demand that will motivate production
New Challenges on the Horizon…
The introduction of new vaccines and increased coverage targets have increased demands on the system in a way that puts business as usual at risk.
Diseases vaccinated against
Vaccine volume per fully immunized child (cm3)
Immunization costper child ($) (including delivery cost) ~6x
4x 4x increasein fridges
between 2001 and 2020,A small but one of the vital
investments in strengthening the supply
chain from end to endAge groups targetedfor immunization
Vaccine doses per child (#) [assuming receives vaccine listed above] ~3x
Acrosslife
course
20050
2010+
$30+
1980
$5
2008
$17
Slide: adapted from McKinsey for BMFG – August 2012
2010+ Realities
1980s Realities
2.5x

9/5/2013
10
Although large in absolute terms, CC equip/OH costs will be
increasingly small as compared to the value of vaccines they support
CC equip/running costs need to be supplemented with HR/transport coststo complete picture of CC support for Vx
1,000
1,500
2,000
2,500 2,415
2,162
234
2012
500
3,000
267
2013
1,740
205
$ M
0
2,846
2015
293
2014
Procurement cost of Vaccines in GAVI Countries
Cost of CC in GAVI Countries
CC costsas a % of
vaccine costs12% 11% 11% 10%
Source: CCL – Country Preparedness: Supply Chain and Logistics Costs in Low and Lower Middle Income Countries, P. Lydon (WHO) (Based on Decade of Vaccines costing work), Feb 2012
Never to early to plan for introduction:
Typhoid conjugate vaccine
August 2013 Bharat Biotech Launches a typhoid
conjugate vaccine for ages from infants 6
months & older to adults . High levels (90+%)
of long lasting protection; One dose schedule
NOTE: this is not a WHO pre-qualified vaccine. UNICEF SD
only procures vaccines with WHO p-q status.
• How will need be forecasted?
• What will be tools and instruments to
measure coverage, & its equity,?
• How will resources (vaccines, funds for
training and advocacy, SC management &
capacity strengthening, etc.)
- 5,000
10,000 15,000 20,000 25,000 30,000
Typ
ho
id
Ro
tavi
rus
Hib
He
pB
Me
nin
giti
s
HP
V
De
ng
ue JE
Morbidity (1'000's)
- 100 200 300 400 500 600
Typ
ho
id
Ro
tavi
rus
Hib
He
pB
Me
nin
giti
s
HP
V
De
ng
ue JE
Mortality (1'000's)
Typhoid morbidity and mortality relative to other vaccine preventable diseases

9/5/2013
11
Some points for the discussion• Hib vaccine: importance of pro-equity introduction policies,
strategies, financing, etc.
• Pentavalent: it takes time to determine suppliers, presentations, end-to-end SCM issues, always in flux
• CC: remember to plan early for this modest investment, essential to protecting large investment in vaccines.
• Innovative Finance: Vaccines are produced in standardized settings, but used in markedly diverse ones. Financing can help inter-country equity of access
• Typhoid: Plan implementation strategies early on:Takes a long time to build SCM capacity, generate demand, assure end to end quality; determine M&E indicators/tools
Thanks to : Ann Ottosen , Katinka Rosenbom of SD, & Gian Gandhi Dmitri Davydov UNICEF HQ
Thank you!

9/5/2013
12
Extra Slides
The Under-five mortality dashboard
Full programme
Partial programme
Insert: Countries procuring
vaccines through UNICEF
Source: 2012 Country forecasts
www.apromiserenewed.org

9/5/2013
13
Procurement context: Global vs. National Buyer
� UNICEF supply strategy is focused on Vaccine Security – the uninterrupted,
sustainable supply of affordable, quality vaccines – with a global
responsibility, acknowledging there is a Vaccine Security Premium.
� UNICEF procurement and tender strategies are developed in support of
the above. Our role in the global market, the characteristics of the
demand market and of the supply market help inform our specific
objectives and strategies.
� While objectives and strategies at a global and national level may vary, we
are dealing with the same vaccine market
UNICEF Vaccines Procurement values on behalf of governments
and partners are increasing
GAVI falls under procurement services but is highlighted separately to show the overall portion of GAVI funded procurement
Source UNICEF Supply Division

9/5/2013
14
Ensuring focus on the whole supply chain
Transparency as a principle and a means of helping markets
be efficient
• Public posting of bid plans and industry consultation
presentations
• Public posting of awards > $100,000
• Posting of prices for product markets where UNICEF has
strategic influence: vaccines, RUTF, medicines, syringes, etc.
• Information notes (eg, Why a 20d BCG vial?, PCV Market
update)
Unicef.org/supply
V3P Project Focus: to broaden the knowledge and
information sharing around vaccine products,
presentation and pricing

9/5/2013
15
Innovative Finance
Increase use of innovative financing and contracting tools
to positively influence the vaccine markets
• Volume Guarantees provide increased (long-term) visibility
to manufacturers and the certainty of a contractual
obligation to purchase
• Prepayments have been exceptionally made in return for
very attractive pricing from manufacturers
• Made possible through partner support
Innovative Finance Achieving Results
Tools Used Transaction Examples Goal
Volume
Guarantee &
Prepayment
Rotavirus Vaccine:
• Volume guarantee provided for a portion of the quantities with some
volumes paid for in advance
• Contract duration of 5-years covering 132M doses
• New vaccine launched and sustained at lower price
• Financing provided by GAVI, with strategic and technical support from
the Gates Foundation (“BMGF”)
• $15 per course � €3.76 per course
• >$400M in savings over 5 years
• Prepayment understood to facilitate
expected expansion of manufacturing
capacity
• Accelerated introduction of Rotavirus
vaccine made possible through certainty
provided by commitment in new markets
Volume
Guarantee
Oral Polio Vaccine (OPV):
• Firm contract signed for 2011-2012 with large bulk and fill-finish
manufacturer who at the time was considering exit of market
• Duration of 2-years originally covering 270M doses per year (540M
doses total)
• Financing provided by BMGF
• Decrease in price offered to <$0.118 per
dose generated significant savings versus
current WAP of >$0.13
• Delayed exit of manufacturer by >2 years
• Increased visibility for manufacturer and
certainty of UNICEF procurement during
fragile OPV market
Volume
Guarantee &
Prepayment
Pentavalent Vaccine (lyophilised):
• Contract signed with new entrant to Pentavalent market with volume
paid for in advance
• Duration for <1 year covering 10M doses
• Financing provided by GAVI
• New entrant to market secured volume
and able to offer extremely attractive
price of $1.80 per dose,
• Expanded vaccine security with expanded
manufacturing capacity in a fragile
market
Volume
Guarantee
PCV
• Volume guarantees for 20/10/5% of quantities or years 1/2/3 of 10 year
contract
• Financing provided by GAVI and WB
• Part of overall AMC structure to achieve
tail price of max. $3.50 and sufficient
production quantities to meet demand