Embed Size (px)
DESCRIPTION
Presentation from the International Congress of the Royal College of Psychiatrists 24-27 June 2014, London
Citation preview

Refractory Mania
David Taylor
Maudsley Hospital
King’s College, London

Refractory mania
Rare as a condition (i.e. longstanding,
unremitting symptoms of mania are rare)
More often manifest as increased cycling
Evidence-based prescribing in short and long
term can reduce likelihood of treatment failure
and cycle acceleration

Where to start?


Meta-analysis of Randomized, Placebo-controlled
Trials in Acute Bipolar Mania: Response*
*Response = at least 50% improvement in Young Mania Rating Scale score
Smith et al. Bipolar Disorders 2007;9:551–560.
0.1 1 10 100
Brecher & Huizar 2003
Smulevich et al. 2005
Pooled effect
Tohen et al. 1999
Tohen et al. 2000
Pooled effect
Brecher & Huizar 2003
Paulsson & Huizar 2003
Pooled effect
Vieta et al. 2002
Smulevich et al. 2005
Hirschfeld et al. 2004
Pooled effect
Keck et al. 2003
Sachs et al. 2006
Pooled effect
Bowden et al. 1994
Paulsson & Huizar 2003
Pooled effect
Pope et al. 1991
Bowden et al. 1994
Pooled effect
Weisler et al. 2004
Weisler et al. 2005
Pooled effect
Haloperidol
Olanzapine
Quetiapine
Risperidone
Aripiprazole
Lithium
Valproate semisodium
Carbamazepine
Favours placebo Relative risk Favours drug

Prophylaxis
Relapse is common –
mania occurs in the context of failed treatment


Olanzapine vs placebo Tohen et al, Am J Psych, 163, 247-256, 2006
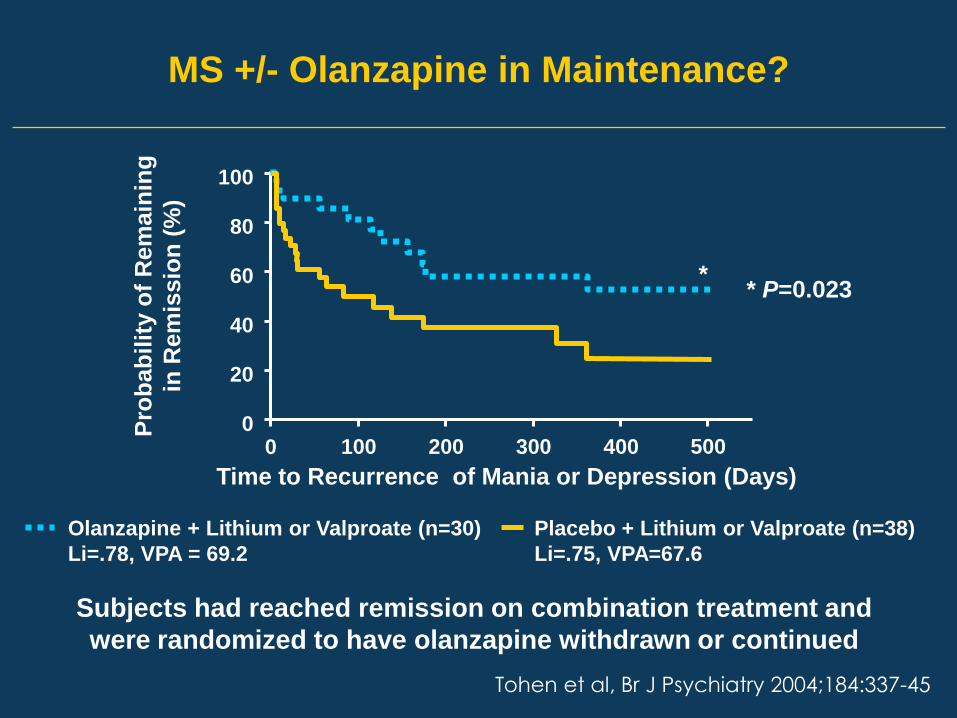
Subjects had reached remission on combination treatment and
were randomized to have olanzapine withdrawn or continued
Tohen et al, Br J Psychiatry 2004;184:337-45
MS +/- Olanzapine in Maintenance?
Time to Recurrence of Mania or Depression (Days)
Placebo + Lithium or Valproate (n=38)
Li=.75, VPA=67.6
Olanzapine + Lithium or Valproate (n=30)
Li=.78, VPA = 69.2
Pro
ba
bil
ity o
f R
em
ain
ing
in R
em
issio
n (
%)
0 100 200 300 400 500
* P=0.023
0
20
40
60
80
100
*


Use the right prophylaxis

Lancet 2010; 375: 385-95

3 6 9 12 15 18 21 24 27 30 33 Months
Time to event outcome measures- first admission or adjuvant treatment for
emerging mood episode
Lancet 2010; 375: 385-95

The problem of drug withdrawal
….choose patients carefully
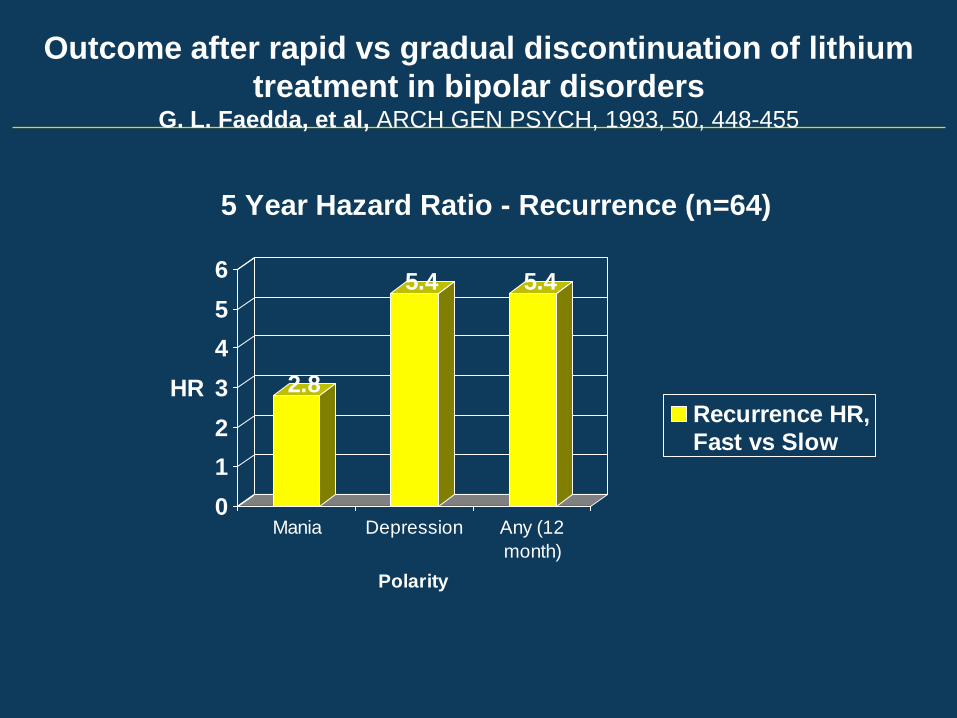
Outcome after rapid vs gradual discontinuation of lithium
treatment in bipolar disorders G. L. Faedda, et al, ARCH GEN PSYCH, 1993, 50, 448-455
2.8
5.4 5.4
0
1
2
3
4
5
6
HR
Mania Depression Any (12
month)
Polarity
5 Year Hazard Ratio - Recurrence (n=64)
Recurrence HR,Fast vs Slow

Baldessarini, R.J. et al. 1997. Reduced morbidity after gradual discontinuation of lithium treatment
for bipolar I and II disorders: a replication study. Am J Psychiatry; 154: 551-553

Combination Therapy in Acute mania
Commonplace – often 3 drugs at once


Combination Therapy Versus Monotherapy in
Patients with Inadequate Mood Stabiliser Response
Response = at least 50% improvement in YMRS score, in randomized controlled trials comparing adjunct therapy with monotherapy.
Smith et al. Acta Psychiatr Scand 2007:115:12–20.
Meta-analysis of response rates*
Risk ratio
Favours monotherapy Favours adjunct therapy
Atypical antipsychotic
Tohen, 2002b (149/220 51/114)
Sachs, 2004 (44/81 29/89)
DelBello, 2002 (13/15 8/15)
Yatham, 2003 (40/68 30/73)
Subtotal
Risk ratio
(95% CI)
Study
1.51 (1.21, 1.89)
1.67 (1.16, 2.39)
1.63 (0.97, 2.72)
1.43 (1.02, 2.01)
1.53 (1.31, 1.80)
%
Weight
51.0
21.0
6.1
22.0
100.0
0.5 1 2 5

Antipsychotic
Brecher, 2003 (55/99 35/101)
Subtotal
Atypical antipsychotic
Tohen, 2000 (35/54 24/56)
Tohen, 1999 (34/70 16/66)
Hirschfeld, 2004 (55/127 29/119)
Brecher, 2003 (43/102 35/101)
Paulsson, 2003 (57/107 27/97)
Subtotal
Mood stabiliser
Bowden, 1994 (32/67 18/72)
Bowden, 1994 (17/35 18/72)
Pope, 1991 (9/20 2/23)
Paulsson, 2003 (51/98 27/97)
Subtotal
Risk ratio
(95% CI)
Study
1.60 (1.16, 2.21)
1.60 (1.16, 2.21)
1.51 (1.05, 2.17)
2.00 (1.23, 3.27)
1.78 (1.22, 2.58)
1.22 (0.86, 1.73)
1.91 (1.33, 2.76)
1.64 (1.38, 1.95)
1.91 (1.03, 3.55)
1.94 (1.00, 3.76)
5.18 (1.26, 21.20)
1.87 (1.29, 2.71)
2.02 (1.52, 2.67)
%
Weight
100.0
100.0
17.7
12.3
22.4
26.4
21.2
100.0
23.6
17.9
3.8
54.7
100.0
Risk ratio
Favours active drug Favours placebo
0.5 1 10 25
Antipsychotic or mood stabiliser in mania
– response rates
2 5

Combination Therapy Versus Monotherapy in
Patients with Inadequate Mood Stabiliser Response
b. Haloperidol + mood stabiliser
Sachs, 2002 (1/53 2/51)
Subtotal
c. Olanzapine + ms
Tohen, 2002b (25/229 2/115)
Subtotal
e. Risperidone + ms
Sachs, 2004 (5/91 6/100)
Sachs, 2002 (2/52 2/51)
Yatham, 2003 (1/75 3/75)
Subtotal
Risk ratio
(95% CI)
0.48 (0.05, 5.14)
0.48 (0.05, 5.14)
6.28 (1.51, 26.04)
6.28 (1.51, 26.04)
0.92 (0.29, 2.90)
0.98 (0.14, 6.70)
0.33 (0.04, 3.13)
0.79 (0.32, 1.95)
%
Weight
100.0
100.0
100.0
100.0
61.6
22.1
16.3
100.0
Risk ratio 0.02 0.2 5 50 1
Favours adjunct therapy Favours monotherapy
Meta-analysis of withdrawal caused by adverse event
Study
Smith et al. Acta Psychiatr Scand 2007:115:12–20.

Use the right drug


www.thelancet.com Published online August 17, 2011 DOI:10.1016/S0140-6736(11)60873-8

www.thelancet.com Published online August 17, 2011 DOI:10.1016/S0140-6736(11)60873-8

Adverse effects and tolerability

Refractory mania
Clozapine
Tamoxifen
Verapamil
? others

Clozapine

All subjects failed
CPZ 500mg + Li

Calabrese JR et al Am J Psychiatry. 1996 Jun;153(6):759-64.
Clozapine for treatment-refractory mania.

Double-blind, randomized, placebo-controlled 6-week study on the efficacy and
safety of the tamoxifen adjunctive to lithium in acute bipolar mania
Journal of Affective Disorders, Volume 129,
Issues 1–3, March 2011, 327-331


Rapid cycling





Thyroxine
Thyroxine
up to
400mcg/day

Quetiapine

Summary
Treat………
Acute mania with MS+AS?
Prophylaxis with MS+AS
Refractory mania with clozapine (? verapamil, etc)
Rapid cycling with quetiapine
Consider tamoxifen, nimodipine, thyroxine, etc.





























