Embed Size (px)
Citation preview

Carolinas HealthCare System
Transforming the Office Management of Heart Failure
Using the Chronic Disease Model in a Family Medicine Residency
ProgramRhett Brown, M.D.
Janice Huff, M.D.Eric Schneider, Pharm.D.
Department of Family MedicineCarolinas Medical Center
Charlotte, NC

Carolinas HealthCare SystemDepartment of Family Medicine
Acute Care Model
Patient Initiated: “Doc, I am sick!”
Brief
Limited planning by the clinician
Works well for the acute limited problem

Carolinas HealthCare SystemDepartment of Family Medicine
Current status of Chronic Illness Care in the U.S.
27% of hypertensives are adequately treated 29% and 26% of diabetics have well controlled
lipid and blood pressure levels, respectively 35% of eligible patients with atrial fibrillation
receive anticoagulation 25% of people with depression are receiving
adequate treatment 50% of discharged CHF patients are
readmitted within 90 days

Carolinas HealthCare SystemDepartment of Family Medicine
Chronic Illness
100 million persons in the US have at least 1 chronic illness
50 Million have more than 188% over age 65 have at least 1
chronic illness22% over age 65 have 4 chronic
illnesses

Carolinas HealthCare SystemDepartment of Family Medicine
Quality Chasm
Institute of Medicine report in 1999 described the “Quality Chasm” in delivery of health care
Institute of Medicine has proposed the redesign of primary care to close the quality chasm between current practices and optimal standards

Carolinas HealthCare SystemDepartment of Family Medicine
System Change ConceptsWhy a Chronic Care Model?
Emphasis on physician, not system, behavior
Characteristics of successful interventions weren’t being categorized usefully
Commonalities across chronic conditions unappreciated.

Carolinas HealthCare SystemDepartment of Family Medicine
Knowledge versus Performance
Physicians know how to treat chronic diseasesThey know what tests should be
ordered and what medications should be prescribed
What services are actually being provided fall far short of best practice standards
We have a systems problem

Carolinas HealthCare SystemDepartment of Family Medicine
The Watchword
Systems are perfectly designed to get the results they achieve

Carolinas HealthCare SystemDepartment of Family Medicine
Remember:
We cannot work harder (systems are perfectly designed to get the results they achieve)
We must work SMARTER! We must work as a TEAM!
We must change OUR system
Carolinas HealthCare SystemDepartment of Family Medicine
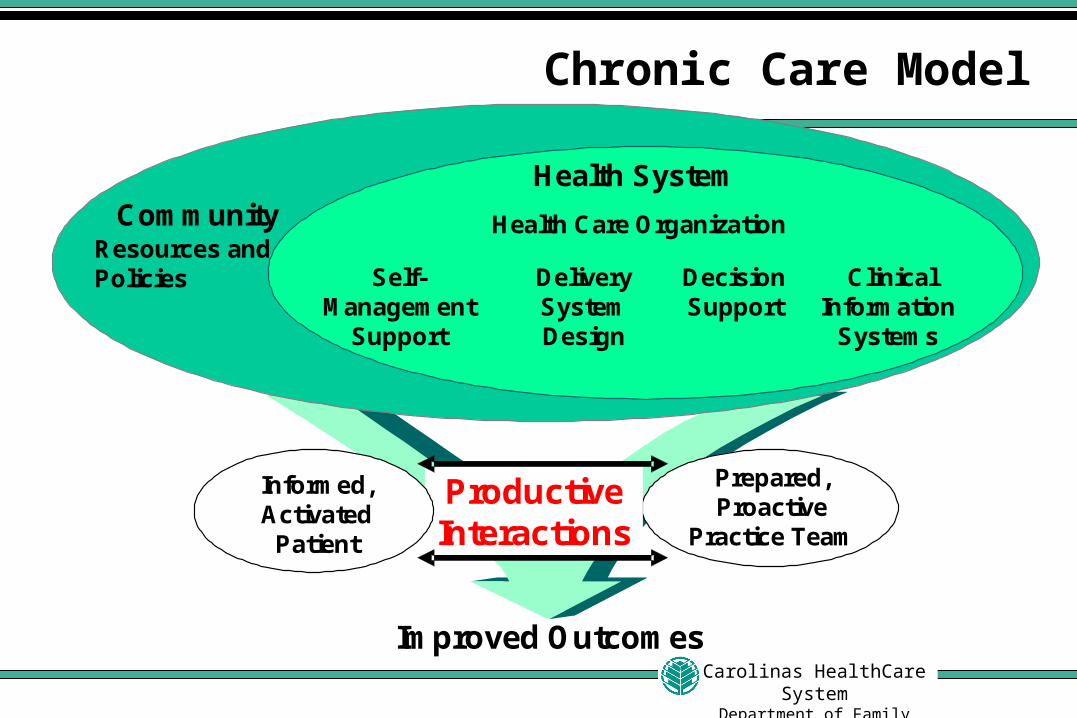
Chronic Care Model
ProductiveInteractions
Prepared,Proactive
Practice Team
Improved Outcomes
DeliverySystemDesign
DecisionSupport
ClinicalInformation
Systems
Self-Management
Support
Health System
Resources and Policies
Community Health Care Organization
Informed,Activated
Patient


Carolinas HealthCare SystemDepartment of Family Medicine
Our Clinical Transformation
Why HFRelatively small populationImpact on our health care system is
largeWell defined and accepted guidelinesEnergy within our hospital system for
improved outpatient management

Carolinas HealthCare SystemDepartment of Family Medicine
Our Clinical Transformation
Determine best practice benchmarks and work to decrease inter-physician variability
Researched published data on best HF outpatient management system design
Developed a concept for an improved healthcare delivery model

Carolinas HealthCare SystemDepartment of Family Medicine
Clinical Transformation Committee
AdministrationClinicians / Support
staff EducationResearch
Information SystemsNursingPharmacyCommunity Resources
Clinical Transformation Committee is multidisciplinary and meets monthly.
Key members:
Steering committee meets weekly to maintain momentum and monitor progress

Carolinas HealthCare SystemDepartment of Family Medicine
Registry Definition
A computerized chronic disease registry is a computer
application to collect and manage condition-specific data
for a group of patients in order to support organized clinical care.

Carolinas HealthCare SystemDepartment of Family Medicine
Critical Features of a Registry
Identification of patients with a common illness
Capture data elements electronicallyReal-time availabilitySearchableLinked to established guidelinesFeedback to providersEnhance generation of letters to patients

Carolinas HealthCare SystemDepartment of Family Medicine
Registry Functions
Patient Informationentered into Registry
Point of care datafor patient visits
Status reports provide clinician feedback
Identify patients needing follow-up
care

Carolinas HealthCare SystemDepartment of Family Medicine
Why Use a Registry?
Institute of Medicine report in 1999 described the “Quality Chasm” in delivery of health care
Institute of Medicine has proposed the redesign of primary care to close the quality chasm between current practices and optimal standards
The registry is one way to narrow the chasm

Carolinas HealthCare SystemDepartment of Family Medicine
Why Use a Registry?
1. Ensure regular follow-up2. Ensure use of evidence-based guidelines3. Provide reminders for clinicians (and patients)4. Facilitate planned care visits5. Monitor performance of practice team6. Enable population management7. Enable task delegation to team members
…TO CHANGE SYSTEMS

Carolinas HealthCare SystemDepartment of Family Medicine
CVDEMS Flow Sheet

Carolinas HealthCare SystemDepartment of Family Medicine
CVDEMS Visit Note

Carolinas HealthCare SystemDepartment of Family Medicine
CVDEMS Visit Note

Carolinas HealthCare SystemDepartment of Family Medicine
CVDEMS Visit Note
History / Physical Examination Assessment of clinical signs/ symptoms of volume overload Cardiac examination Assessment of activity level (NYHA Class) and Disease stage (AHA/ACC Stage)
Tests / Procedures Weight, Blood pressure, Heart rate measurement BMP (q12 months, or as clinically indicated) Assess LVF (Change in clinical status or clinical event/treatment with significant effect on cardiac function)
Education Continue Heart Failure patient education plan Avoidance of patient behaviors that may increase the risk of HF
Medications Review current medication regimen for the presence of medications known to affect HF Heart failure medications as appropriate (see algorithm)
Self Management Training Update Heart Failure action plan Collaborative goal setting
Needs Assessment Assess patient needs and review community resources. Refer as appropriate

Carolinas HealthCare SystemDepartment of Family Medicine
CVDEMS Flow Sheet

Carolinas HealthCare SystemDepartment of Family Medicine
Services Needed/Recommendations

Carolinas HealthCare SystemDepartment of Family Medicine
CVDEMS Decision Rules
LDL Serum creatinine Serum potassium Aspirin therapy ACEI / ARB therapy Beta Blocker therapy Statin therapy Spironolactone therapy Hydralazine/Nitrate
Coumadin in A Fib CTC Study Consent Assessment of LVEF ECHO Heart Failure
Education Pharmacy Consult Pneumovax Influenza Vaccine

Carolinas HealthCare SystemDepartment of Family Medicine
Decision Tools Treat hypertension Encourage smoking cessation Treat lipid disorder
Encourage regular exercise Discourage ETOH & illicit drug use
Stage A Stage B Stage C Stage D
High risk for HF NYHA IVNYHA IIINYHA IINYHA I
consider ACEI ACEI (preferred) or ARB in ALL
patients*
discontinue NSAID’s, CCB, metformin, antiarrhythmics, Actos/Avandia*
Cardiology Referral
consider -Blockers in
select patients*
consider hydralazine
(25mg TID titrate to 100mg QID)
PLUSisosorbide DN
(10mg TID titrate to 80mg TID)
in patients unable to tolerate ACEI/ARB
ACEI (preferred) or ARB*(hydralazine + isosorbide DN in patients
unable to tolerate ACEI or ARB)AND
-Blockers* in ALL patients
Loop diuretic (ALL patients) as needed for fluid control
consider digoxin(target concentration <1.0 ng/ml
consider aldosterone antagonistspironolactone 25 mg daily (preferred) or
epleronone (Inspra®) 25-50mg
ACEI or ARB in ALL patients*
Loop diuretic for fluid control in ALL
patients
consider digoxinand aldosterone
antagonist
may need mechanical assist,transplantation,continuous IV inotrope infusions,HOSPICE care

Carolinas HealthCare SystemDepartment of Family Medicine
Services Needed/Recommendations

Carolinas HealthCare SystemDepartment of Family Medicine
Patient Goal Setting

Carolinas HealthCare SystemDepartment of Family Medicine
Patient Goal Setting

Carolinas HealthCare SystemDepartment of Family Medicine
Patient Goal Setting

Carolinas HealthCare SystemDepartment of Family Medicine
Heart Failure Action Plan
Analogous to an Asthma action plan
Part of patient self management component
Heart Failure Action Plan YOU are the most important person in the management of your heart failure. As part of your medical care team, we will guide you and offer support in the management of your heart failure. The following plan will help you monitor your heart failure and take appropriate actions.
ALL CLEAR CONTINUE YOUR TREATMENT PLAN Your heart failure is stable You should have:
No change in the swelling in your feet/ankles
No change in your breathing No change in your ability to
exercise or perform your daily activities
No more than a 1-2 pound increase in weight since yesterday
Medications: Special Instructions:
CAUTION DO THE FOLLOWING Your heart failure is getting worse You may have:
An increase in the swelling in your feet/ankles
More difficulty breathing, especially when you lie down
More difficulty in your ability to exercise or perform your daily activities
More than a 3-5 pound increase in weight since yesterday
Call your Care Coordinator at 704-446-1000
DANGER CALL YOUR DOCTOR Your heart failure is worse and you need to see your doctor. You may:
Have an inability to catch your breath
Feel severely tired or weak Have more than a 5 pound increase
in weight since yesterday Have chest pain that is new or
worse than usual Be unable to perform daily activities
that you were able to do yesterday
If during business hours: Call your Care Coordinator at 704-446-1000 After hours or weekends: Call the Family Practice Doctor on call at 704-446-1000

Carolinas HealthCare SystemDepartment of Family Medicine
Heart Failure Action Plan
Heart Failure Action Plan YOU are the most important person in the management of your heart failure. As part of your medical care team, we will guide you and offer support in the management of your heart failure. The following plan will help you monitor your heart failure and take appropriate actions.
ALL CLEAR CONTINUE YOUR TREATMENT PLAN Your heart failure is stable You should have:
No change in the swelling in your feet/ankles
No change in your breathing No change in your ability to
exercise or perform your daily activities
No more than a 1-2 pound increase in weight since yesterday
Medications: Special Instructions:
CAUTION DO THE FOLLOWING Your heart failure is getting worse You may have:
An increase in the swelling in your feet/ankles
More difficulty breathing, especially when you lie down
More difficulty in your ability to exercise or perform your daily activities
More than a 3-5 pound increase in weight since yesterday
Call your Care Coordinator at 704-446-1000
DANGER CALL YOUR DOCTOR Your heart failure is worse and you need to see your doctor. You may:
Have an inability to catch your breath
Feel severely tired or weak Have more than a 5 pound increase
in weight since yesterday Have chest pain that is new or
worse than usual Be unable to perform daily activities
that you were able to do yesterday
If during business hours: Call your Care Coordinator at 704-446-1000 After hours or weekends: Call the Family Practice Doctor on call at 704-446-1000

Carolinas HealthCare SystemDepartment of Family Medicine
Care Coordinator
Adapted our current nurse triage positionsTwo RN Care Coordinators provide
continuityAdditional training in HF managementContact all HF patients after office visitsContact all patients on a regular schedule
based on HF severityFollow standing orders for management of
mild exacerbations

Carolinas HealthCare SystemDepartment of Family Medicine
Patient Support Group
Initially held a patient focus groupFrom focus group recommendations
developedMonthly support groupHF disease educationOpportunity for residents to
participate in patient education and facilitating a group

Carolinas HealthCare SystemDepartment of Family Medicine
Measure Outcomes
Hospitalization ratesQuality of life scoresMedication refill compliance

Carolinas HealthCare SystemDepartment of Family Medicine
Lessons Learned
Difficulty and time required to navigate the IRB and RRC process
Communicating and achieving ‘buy-in’ when working with part-time providers
Cultural change takes TIME and PERSERVERANCE
Awareness of subcultures within our office

“Well, I do have this recurring dream that one day I might see some results.”






























