Embed Size (px)
Citation preview

Diagnostic imaging of the
temporomandibular joint
BY : ASHISH RANGHANI
PG STUDENT PART 1
DEPARTMENT OF ORAL MEDICINE & RADIOLOGY
05/11/2015

TRANSCRANIAL VIEW
STRUCTURESHOWN
AREA OF JOINT SEEN
Arthritic changes on the articular surface
Lateral aspect of:Glenoid fossa
Articular eminence
Joint space
Condylar head
It helps to evaluate the joint’s bony relationship
Changes on the central and medial surface are not seen

• Film position: flat against patients ear centered over TM joint of interest against facial skin parallel to sagittal plane
• Position of patient: head adjusted so sagittalplane is vertical & ala tragus line parallel to floor
• View :3 positions
• open, close, rest mouth

Central ray• A) Postauricular/ Lindblom Technique
-1/2 inch behind and 2 inch above auditory meatus
-central ray should be directed posteriorly so
it passes along long axis of condyle.
• B) Grewcock approach
-central ray passes through a point 2 inches above ext. auditory meatus.
• C) Gill’s approach
- ½ inch anterior and 2 inch above EAM

• Central ray aimed downwards at 25 degree to the horizontal, across the cranium, centering through TMJ of interest
• Closed view- size of joint space, position of head of condyle, shape & condition of glenoid fossa & articulareminence
• Open view- range & type of movement
• Comparison of both sides
Disadvantages :
• Superimposition of ipsilateral petrous ridge over the condylar neck

Exposure Parameters Intra Oral X-ray MachinekVp – 70 mA – 07 Seconds – 1.5

Transcranial projections of the left TMJ.closed view (A) and the open view
1
1. articular eminence
2
2 glinoid fossa
3
3 head of condyle
4
4 external auditory meatus
51
2
34
5
5 joint space

TRANSPHARYNGEAL
VIEW/Infracranial/McQueen Dell
INDICATION AREA OF JOINT SEEN
Tmj pain dysfunction syndrome
Medial surface of theCondylar head & neck
Articular surfaceOsteoarthritis & rheumatoid arthritis
Pathology-condylarhead-cyst & tumor
Fracture of neck & condyle

• Film placement-patient holds the cassette flat againstpatients ear centered over TM joint of interestagainst facial skin parallel to sagittal plane½ inch anterior to EAM
Position of patient- occlusal plane parallel to transverse axis of film-soft parts are in a line with nasopharynx and joint
• Patient instructed to inhale slowly through nose, filling of
nasopharynx with air
• Open mouth-condyles move away from base of skull and
mandibular notch is enlarged on opp side.

• Central ray- directed from opp side cranially at angle(-
5 to -10 degrees)
• Beneath the zygomatic arch, through sigmoid notch
posteriorly across pharynx at the condyle
• Comparison of both condylar heads

Exposure ParametersIntra Oral X-ray Machine kVp – 65-70 mA – 7-10 Seconds – 0.8 Using Extra Oral X-ray Machine kVp – 40 mA – 40 Seconds – 1

TRANSPHARYNGEL VIEWMedial profile of the condyle
1 condylar head
2 articular eminence
3 sigmoid notch
4 pterygoid plate
1
2
3
45
5 zygoma

TRANSORBITAL (ZIMMER PROJECTION)
INDICATION AREA OF JOINT SEEN
Trauma Fracture cases
Ant view of TMJ
Medial displacement of fractured condyle
Fracture of neck of condyle

• Film position-behind patients head at an angle of 45 degree to sagittal pane
• Position of patient-
-Sagittal pane vertical
-Canthomeatal line should be 10 degree to the horizontal with head tipped downwards
-The mouth should be wide open
• Central ray-
-tube head-front of patients face
-directed to joint of interest at an angle of +20 degrees to strike cassette at right angles

Point of entry-
- Pupil of the same eye-asking patient to look straight ahead
- Medial canthus of the same eye
- Medial canthus of the opposite eye
- Disadvantage :if the patient cannot open wide, areas of the joint articulating surfaces will be obscured because of mutual superimposition

Transorbital projection showing a frontal
view of the
condyle. The lateral pole is indicated with
an arrow.
Exposure Parameters Intra Oral X-ray Machine kVp – 65-70 mA – 7-10 Seconds – 0.8 Extra Oral X-ray Machine kVp – 40 mA – 40 Seconds – 1
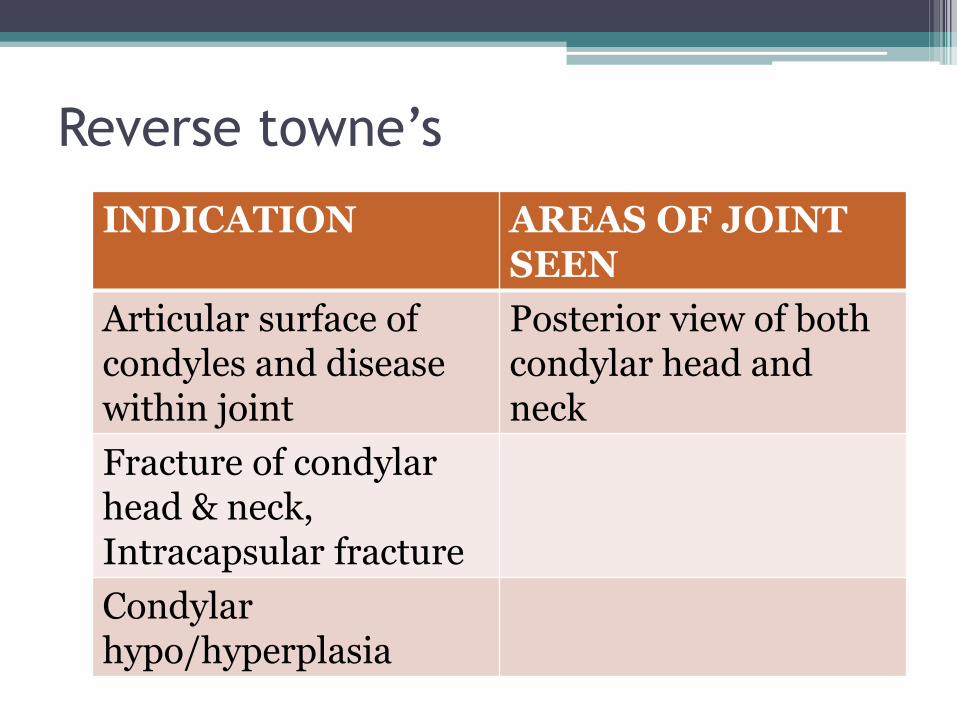
Reverse towne’s
INDICATION AREAS OF JOINT SEEN
Articular surface of condyles and disease within joint
Posterior view of both condylar head and neck
Fracture of condylarhead & neck, Intracapsular fracture
Condylarhypo/hyperplasia

• Film position-cassette placed perpendicular to the floor
Long axis of cassette placed vertically
• Position of patient-
-sagittal plane vertical & perpendicular to film
-lips are centered on the film
-only forehead should touch the film
-mouth wide open
-radiographic base line is at angle of negative 30 degrees to film
• Central ray-directed midsagittal plane at the level of mandible and perpendicular to film

Forehead –nose position
Exposure Parameters Using Extra Oral Machine kVp – 70-80 mA – 60-50 Seconds – 1.6 (Bucky Grid)

Towne’s view/anteroposterior view
• Observe occipital area of skull
• Neck of condylar process
• Film position-cassette perpendicular to floor, long axis-vertically
• Position of patient- A-P view with the back of patients head touching film. canthomeatal line perpendicular to film
• Central ray-30 degree to canthomeatal line & passes it at a point b/n external auditory canals
Exposure Parameters Using Extra Oral Machine kVp – 70-80 mA – 60-50 Seconds – 1.6 (Bucky Grid)

Observe occipital area of skullNeck of condylar process
Towne’s view/anteroposterior view

Structures ShownA full axial view of the base of the cranium showinga symmetrical projection of the petrosa, the mastoidprocess, foramen ovale, spinosum canals, carotidcanals, sphenoidal sinuses, mandible, maxillary sinus,nasal septum, odontoid process of the atlas and theentire atlas, axial inclination of the mandibularcondyles.Helps to study destructive/expansile lesionsaffecting the palate, pterygoid region or base of theskull, sphenoidal sinus.
Submentovertex projection the radiographic base line is parallel to the film,and the X-ray is perpendicular to the film
Film PlacementThe cassette is placed perpendicular to the floor in acassette holding device. The long-axis of the cassetteis placed vertically.
Submentovertex Projection

Position of PatientThe head is centered on the cassette, with thepatient’s head and neck tipped back as far as possible,the vertex (top) of the skull touches the cassette. Boththe midsagittal plane should be perpendicular to theplane of the film and the radiographic base line shouldbe parallel to the film.
Central RayIs directed perpendicular to the film and throughthe midsagittal plane, between the angles of themandible, perpendicular to an imaginary line joiningthe mandibular 1st molars (approximately 1 inch fromthe chin).In order to view the petrous portion, the centralray is directed at right angles (or 5° to the horizontal)to the film midway between the external auditory
Exposure ParameterskVp – 50 mA – 20-30 Seconds – 0.4

Zygomatic archLateral wall of the orbitAnterior arch of the atlas Shenoidal air sinuscondyleUpper & lower teeth suprrimposedOccipital condyleForamen megnumMastoid air sinusShadow of the spine

Panoramic Projection
it provides an overall view of the teeth and jaws, provides a
means of comparing left and right sides of the mandible
Gross osseous changes in the condyles may be identifi ed,
such as asymmetries, extensive erosions, large osteophytes,
tumors or fractures
No information about condylar position or function
is provided because the mandible is partly opened and
protruded
when this radiograph is exposed.
Exposure Parameters kVp – 76 mA–15 Seconds – 15

Panoramic images that revealed rightcondylar hyperplasia (A) and destruction of thecondyle by a malignant tumor (B) (arrows).
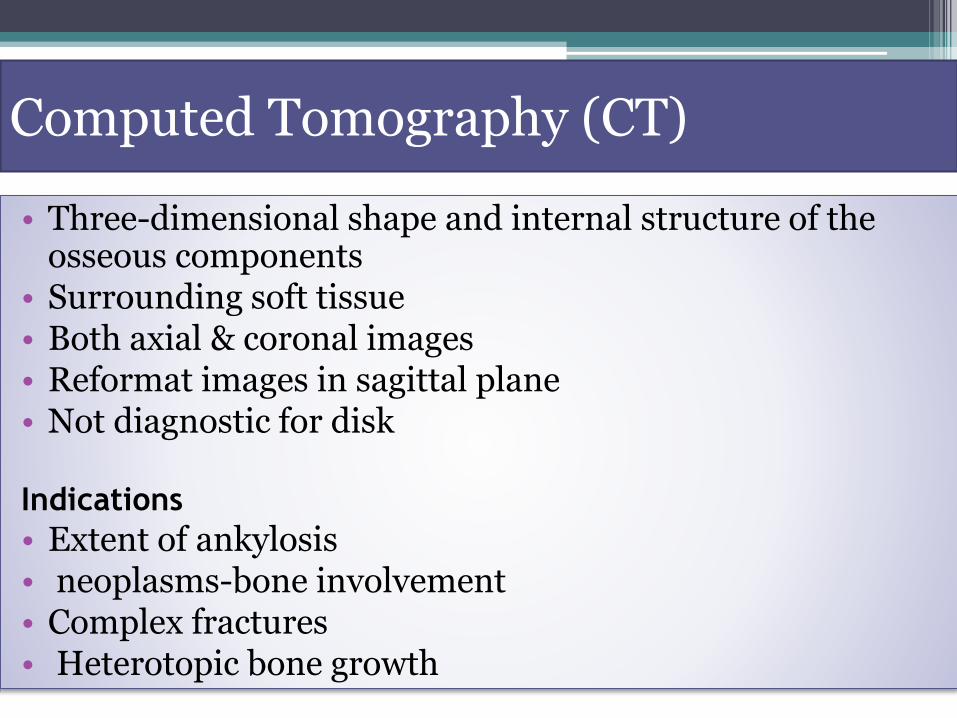
Computed Tomography (CT)
• Three-dimensional shape and internal structure of the osseous components
• Surrounding soft tissue• Both axial & coronal images• Reformat images in sagittal plane• Not diagnostic for disk
Indications
• Extent of ankylosis• neoplasms-bone involvement• Complex fractures• Heterotopic bone growth
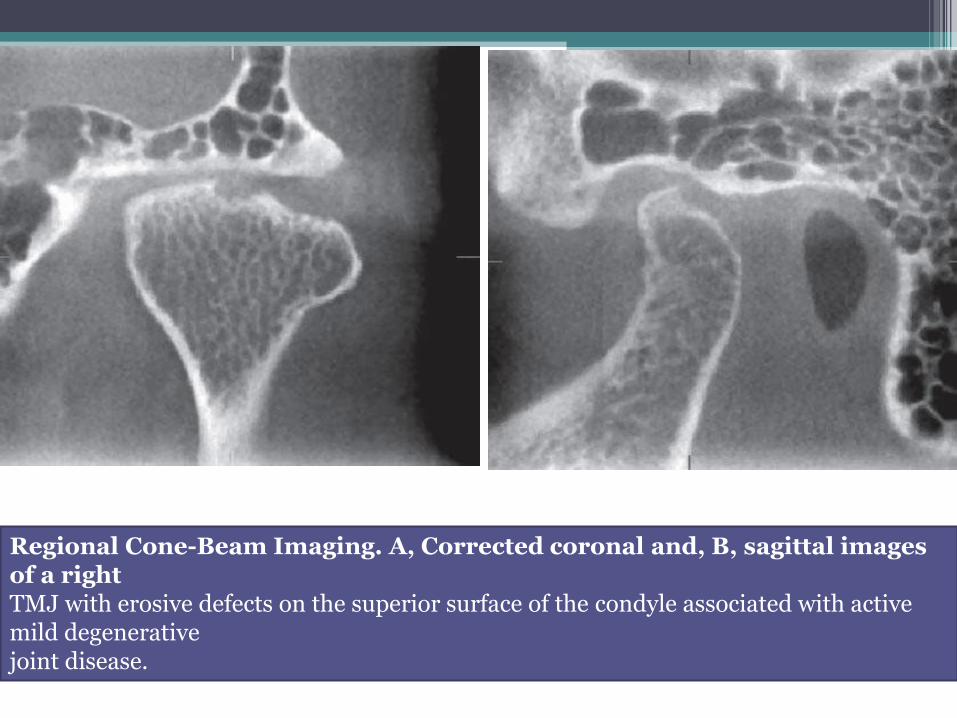
Regional Cone-Beam Imaging. A, Corrected coronal and, B, sagittal images of a rightTMJ with erosive defects on the superior surface of the condyle associated with active mild degenerativejoint disease.

MAGNETIC RESONSNCE IMAGING (MRI)
• Magnetic field and radiofrequency pulses
• Tissue with greater water content emit a higher
signal
• Bilateral dual surface coils- 0.5 to 2 tesla-
Improve image resolution
Oblique sagittal/oblique coronal scans with t1, t2
Closed mouth, partially open and fully open
positions
• images in the sagittal and coronal planes without repositioning the patient
• T1-weighted images best –osseous & diskaltissues
• T2-weighted images-inflammation and joint effusion.
• Motion MRI studies-during opening and closing the patient open in a series of stepped distances
and using rapid image acquisition. ("fast scan ")

MRI of a normal TMJ. A, Closed view showing the condyle and temporal component. The biconcave disk is located with its posterior band (arrow) over the
condyle.B. Coronal image showing the osseous components and disk
(arrows) superior to the condyle.

• Advantages of CT • Advantages of MRI• Direct delineation of bony
structures-surgical anatomy• Reconstruction in all planes• Some soft tissues-lateral
pterygoid muscle• 3-D images from any angle
• Disadvantages--high radiation exposure-soft tissues cant be
appreciated
• Soft tissues-esp disk and its association
• Information in short acquisition time
• Disadvatages--expensive-claustophobia
MRI is contraindicated in pregnant patient or whohave pacemakers, intracranial vascular clips, or metal particles in vital structures. Claustrophobic patient or an inability to remainmotionless.

WHAT ARE THE SIGNS AND SYMPTOMS OF TMD?Pain, discomfort and tenderness of the jaw joint and surrounding muscles
Radiating pain in the face, jaw, or neck,
jaw muscle stiffness,
Reduced mouth opening
painful clicking, popping or grating in the jaw joint when opening or closing the mouth,
A change in the way the upper and lower teeth fit together.
Locking of the jaw on opening
Neck ache, headeche, dizziness, Sleep disturbance

I - Muscular Diagnosesa - myofascial painb - myofascial pain with limited opening
II - Disk Displacementa - disk displacement with reductionb - disk displacement without reduction and with limited openingc - disk displacement without reduction and without limited opening
III - Arthralgia, osteoarthritis and osteoarthrosisa - arthralgiab - temporomandibular joint (TMJ) osteoarthritisc - temporomandibular joint (TMJ) osteoarthrosis
Categories of clinical TMD conditions according to theRDC/TMD.

Disorders of the
Temporomandibular Joint
1- Developmental Abnormalities
2- Soft Tissue Abnormalities

Developmental Abnormalities:
1- Condylar Hyperplasia
2- Condylar Hypoplasia
3- Juvenile Arthrosis
4- Coronoid Hyperplasia
5- Bifid Condyle
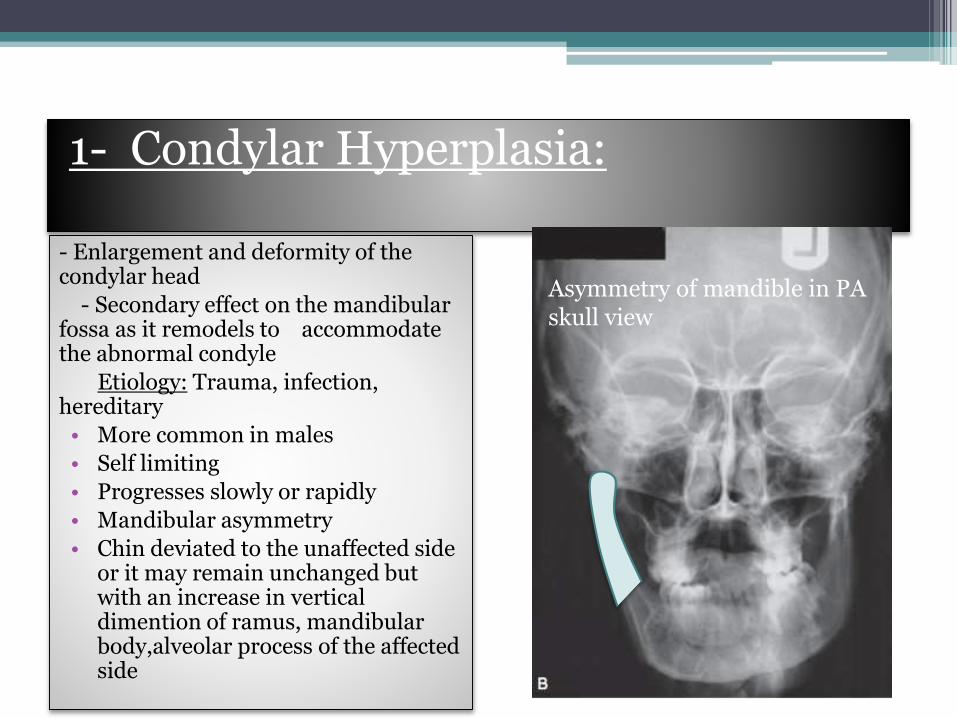
1- Condylar Hyperplasia:
- Enlargement and deformity of the condylar head
- Secondary effect on the mandibular fossa as it remodels to accommodate the abnormal condyle
Etiology: Trauma, infection, hereditary
• More common in males
• Self limiting
• Progresses slowly or rapidly
• Mandibular asymmetry
• Chin deviated to the unaffected side or it may remain unchanged but with an increase in vertical dimention of ramus, mandibularbody,alveolar process of the affected side
Asymmetry of mandible in PA skull view
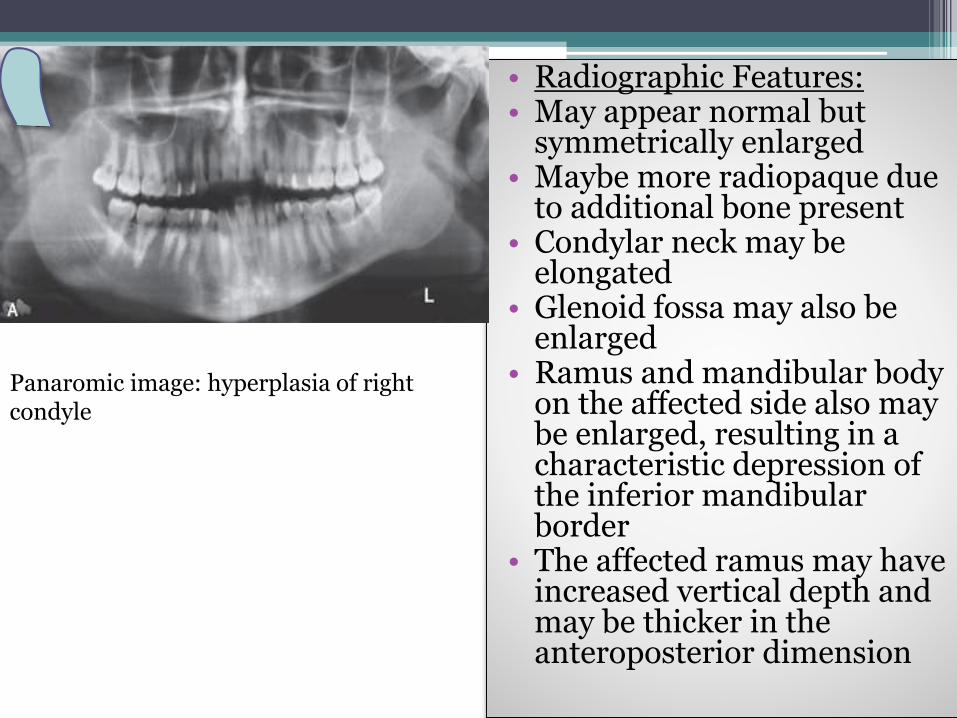
• Radiographic Features: • May appear normal but
symmetrically enlarged • Maybe more radiopaque due
to additional bone present• Condylar neck may be
elongated• Glenoid fossa may also be
enlarged • Ramus and mandibular body
on the affected side also may be enlarged, resulting in a characteristic depression of the inferior mandibular border
• The affected ramus may have increased vertical depth and may be thicker in the anteroposterior dimension
Panaromic image: hyperplasia of right condyle

• Failure of the condyle to attain normal size because of congenital and developmental abnormalities or acquired diseases that affect condylar growth.
• The condyle is small, but condylar morphology is normal• Underdeveloped ramus and occasionally mandibular body• Unilateral or bilateral
2- Condylar Hypoplasia
Hypoplasia of left condyle

• Radiographic Features:
• The condylar neck and coronoid process usually are very slender and are shortened or elongated in some cases

3- Juvenile Arthrosis:
• Manifests as hypoplasia and characteristic morphologic abnormalities
• May be a form of condylar hypoplasia
• It affects children and adolescents during the of mandibular growth
• More common in females
• Incidental finding in a panoramic projection

• Radiographic appearance:
• Condylar head develops a characteristic “toadstool” appearance
• Condylar neck is shortened or even absent in some cases

4- Coronoid Hyperplasia:
• - acquired or developmental
• - elongation of the coronoid process
• - developmental -> bilateral
• acquired -> uni or bilateral
• - inability to open mouth
• - painless

• Radiographic features:
• Best seen in panoramic,
Waters, and lateral tomographic views and on CT scans
• TMJs usually appear normal

5- Bifid Condyle:
• Vertical depression,notch, or deep cleft
in the center of the condylar head• Rare, often unilateral • Incidental finding• Some patients may have sings of TMDs (noises +
pain)• Radiographic Features:• Depression on the superior condylar surface giving a
heart shape

Condylar agenesis
• The absence of all or portions of condylar process, coronoidprocess, ramus or mandible
• other first and second arch anomalies seen
• early treatment maximizes condylar growth
• A costocondral graft may help with facial development
Panoramic view and CT Scan show absence of left condylarhead.

Soft Tissue Abnormalities
Internal Derangements – TMJ in which there displacement of the disc from its normal functional relationship with the
mandibular condyle and the articular portion of the temporal bone. abnormality in the articular disc and may interfere
with normal function• - Cause is unknown• - Internal derangements can be diagnosed by MRI• Clinical Features:• - found in both symptomatic and healthy pts• - symptomatic pts may have a decreased range of
mandibular motion• -displacements may be unilateral or bilateral


• Radiographic Features:• - MRI is the technique of choice• Disc Displacement:• - Anterior displacement is most common• - The articular disc is located anterior to the condylar
head• Disk reduction and nonreduction:• - reduction is when an anteriorly displaced disk may
reduce to a normal relationship with the condylar head during any part of the mouth opening movement
• - nonreduction is when the disk remains anteriorly displaced and will undergo permanent deformation.
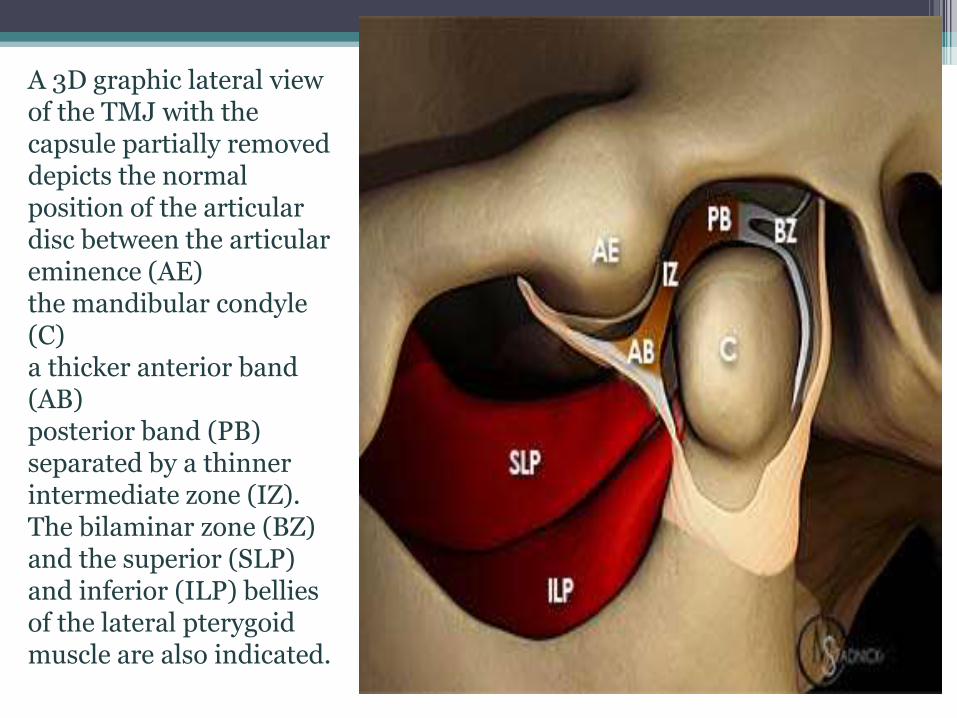
A 3D graphic lateral view of the TMJ with the capsule partially removed depicts the normal position of the articular disc between the articular eminence (AE) the mandibular condyle (C)a thicker anterior band (AB) posterior band (PB) separated by a thinner intermediate zone (IZ). The bilaminar zone (BZ) and the superior (SLP) and inferior (ILP) bellies of the lateral pterygoid muscle are also indicated.
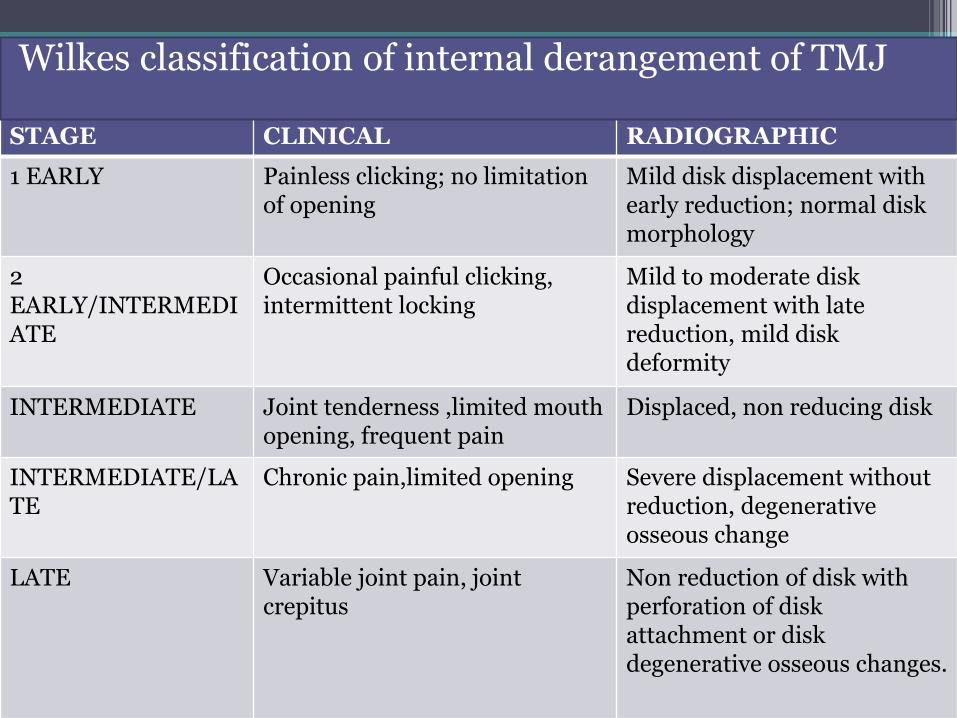
STAGE CLINICAL RADIOGRAPHIC
1 EARLY Painless clicking; no limitation of opening
Mild disk displacement with early reduction; normal disk morphology
2 EARLY/INTERMEDIATE
Occasional painful clicking, intermittent locking
Mild to moderate disk displacement with late reduction, mild disk deformity
INTERMEDIATE Joint tenderness ,limited mouth opening, frequent pain
Displaced, non reducing disk
INTERMEDIATE/LATE
Chronic pain,limited opening Severe displacement without reduction, degenerative osseous change
LATE Variable joint pain, joint crepitus
Non reduction of disk with perforation of disk attachment or disk degenerative osseous changes.
Wilkes classification of internal derangement of TMJ





• perforations between the superior and inferior joint spaces most commonly occur in the retrodiskal tissue, just behind the posterior band of the disk
• Not detected with MRI
Perforation and Deformities:
Fibrous Adhesions and Effusion:
- Fibrous adhesions are masses of fibrous or scarred tissue that form in the joint space, particularly after TMJ surgery- Joint Effusion means fluid in the joint and is considered to be and early change that may precede degenerative joint disease - Both can be detected by MRI

Remodeling and Arthritic condition
• Remodeling: • - Adaptive response of cartilage and osseous tissue
to forces applied to the joint that maybe excessive, resulting in alteration of the shape of the condyle and articular eminence
• - no destruction or degeneration of articular soft tissue occurs
• - occurs throughout adult life• - considered abnormal only if it is accompanied by
clinical signs and symptoms of pain or dysfunction

• - Radiographic Features:• - flattening • - cortical thickening of articulating surfaces• - subchondral sclerosis
A- The right temporal component shows subchondral sclerosis and flattening (arrow)B- The right condyle shows mild flattening of the lateral aspect and subchondralsclerosis of the medial aspect (arrow) C- Cadaver specimen. Note the flattening of the temporal component (black arrows) and large perforation posterior to a residual deformed disk (white arrow)

• 2- Degenerative joint disease (osteoarthritis):
• - non inflammatory disorder of the joints characterized by joint deterioration and proliferation
• - can occur at any age (increases with age)
• - female predominance
• - asymptomatic or pts may complain of signs + symptoms of TMJ dysfunction
• - Radiographic features:
• - more accurately seen in CT but gross osseous changes maybe evident in MRI studies
• At the maximum intercuspation joint space may be narrow or absent
• Loss of cortex or erosions of the articulating surfaces of the condyle or temporal component are characteristics of this disease
Deterioration: characterized by loss of articular cartilage and bone erosion Proliferation: proliferative component is characterized by new bone formation at the articular surface and in the subchondral region
ELY cyst: small round radiolucent area with irregular margins surrounded by broad zone 0f sclerosis

Bilateral destruction of condylesanterior open biteChin appears receded
• 3- Rheumatoid Arthritis:• - Synovial membrane inflammation• Female with increase age• - Patients with TMJ involvement complain
of swelling, pain, tenderness, stiffness on opening, limited range or motion, and crepitus
• - Radiographic Features:• - Osteopenia (decreased density) of the
condyle and temporal component• The pannus may destroy the disk, resulting
in diminished width of the joint space. • Bone erosions by the pannus most often
involve the articular eminence and the anterior aspect of the condylar head, which permits anterosuperior positioning of the condyle when the teeth are in maximal intercuspation and results in an anterior open bite.
• Erosion of the anterior and posterior condylar surfaces at the attachment of the synovial lining may result in a “ sharpened pencil ” appearance of the condyle. Erosive changes may be so severe that the entire condylar head is destroyed.
Result of synovitis which lead to formation of synovial granulomatous tissu(pannus) that grows into fibrocartilage & bone reliasing enzymes that destroy articular surface & underlying bone
4- Juvenile Arthritis:
• - Inflammatory disease that is characterized by chronic, intermittent synovial inflammationresults in: synovial hypertrophy, joint effusion, and swollen, painful joints
• Before the age of 16 years (mean age 5 years)• -pain and tenderness of affected joint or joints• - can be asymptomatic• - unilateral is common• - facial appearance known as “bird face”• - possible mandibular asymmetry if one side is more
severely affected with chin deviated toward affected side
• Radiographic features:
• - Osteopenia (decreased density) maybe only an initial radiographic finding
• - Impaired mandibular growth
• - Severe cases: only pencil shaped small condyle remains
• - Abnormal disk shape is often observed in patients with TMJ involvement

Trauma
1- Effusion: - Influx of fluid into the joint as a result of trauma
(hemorrhage or inflammation)- Swelling over affected joint• Pain in TMJ, preauricular region, and limited
range of motion• Radiographic Features:- Commonly seen in conjunction with internal
derangements- Joint space is widened

2- Dislocation:
- Abnormal positioning of the condyle out of the mandibular fossa but within the joint capsule
- Unable to close mandible to maximal intercuspation
* Radiographic Features:
- In bilateral cases, both condyles are located anterior and superior to summits of articular eminentia
3- Fracture:
- Usually occur at condylar neck and often are accompanied by dislocation of the condylar head
- Unilateral fractures more common
- May be accompanied by parasymphyseal or mandibular body fracture on contralateral side
- Swelling over TMJ
- Limited range of motion

• Radiographic features:
- Radiolucent line limited to the outline of the neck is visible
- If bone fragments overlap, an area of increase in radiopacitymay be seen
- Town’s view panorama is taken to view fractures

4- Neonatal Fracture:
- Use of forceps during delivery of neonates may result in fracture and displacement of the rudimentary condyle
- Severe mandibular hypoplasia
comminuted displaced left subcondylarneck fracture

5- Ankylosis:
- Condition in which condylar movement is limited by a mechanical problem in the joint or by a cause not related to joint components
- Restricted jaw opening or limited jaw opening
* Radiographic Features:
- In fibrous ankylosis articulating surfaces are usually irregular because of erosions
- In bony ankylosis joint space may be partly or completely obliterated by the osseous bridge
- Coronal CT images are the best
to evaluate ankylosis
Bony ankylosis (CT coronal image slice) right condyle and ramus are markedly enlarged. Articular surface irregular and central and lateral aspect fused to the roof of glenoid fossa, lack of joint space

1- Benign Tumors:
- Osteoma, osteochondroma, Langerhans histocytosisand osteoblastomas
- Chondroblastomas, fibromyxomas, benign giant cell lesions and anneurysmal bone cysts also occur
- Benign tumors and cysts of the mandible (ameloblastoma, OKC) may involve the entire ramus and condyle
- Grow slowly- TMJ swelling- Pain and decrease in range of motion- Tumors of coronoid process are painless but may
complain of progressive limitation of motion

Radiographic Features:
- Condylar tumors condylar enlargement with irregular outline
- Osteoma and osteochondroma appear as abnormal, pedunculated mass attached to the condyle
Axial bone algorithm. CT image of an osteochondroma extending from the anterior surface of the left condylar head (arrow)

2- Malignant Tumors:
A- Primary (rare): - Intrinsic
- Extrinsic
Intrinsic: Chondrosarcoma
Osteogenic sarcoma
Synovial sarcoma
Fibrosarcoma
Extrinsic: Direct extension of adjacent parotid salivary gland malignancies
rhabdomyosarcoma

1- chondrosarcoma (CT axial section bone algorithm) radiolucent destructive lesion present in the left condylar head and faint radiopacities (soft tissue calcifications) are visible anterior to the condylar head (arrows)2- Axial soft tissue algorithm CT image of a metastatic lesion from a carcinoma of the thyroid gland that has destroyed all of the left mandibular condyle.

TMJ ARTHROGRAPHYIndications:
Position and function of disk -pain and
dysfunction-long standing
History of locking-persistent
Perforations of the disk and retrodiskal
tissue.
Joint dynamics
Disc displacement-ant/anteromedial

Contraindications:Infections in the preauricular region.Patients allergic to contrast media.Patients with bleeding disorders and on anticoagulant therapy
Therapeutic :
Diagnostic aspiration of joint fluid.Intraarticular injections of steroids

Techniques
Single contrast – lower compartment arthrographyis most commonly done
Double contrast – contrast medium into the lower compartment and injection of air into the upper compartment.

STEPS
• Contrast media – non ionic agents such as iopamidol-370,iodohexol-350
• Fluoroscopy aids in accurate positioning of needle• Primary record-video-allows imaging of joint compartments as
they move• Only lateral parts seen
• Medial aspect of joint-thin section multidirectional hypocycloidal
tomography
• 5-6 slides ,2-3 mm apart, patient mouth open and closed
• If further info-contrast –upper joint space-repeat investigation

ARTHROSCOPY
ContraindicationsAbsolute
Bony ankylosis.Advanced resorption of the glenoid fossa.Infection around the joint area.Malignant tumors.
Relative Patients at increased risk of hemorrhage.Patients at increased risk for infection.

References
• White & Pharoah(6th Edition)
• Eric Whaites( 3rd Edition)
• Karjodkar (2nd Edition)
• Grey`s Anatomy (38th Edition)
• Anatomy Of Head & Neck By B.D Chaursia
• Textook Of Oral & Maxillofacial Surgery By NeelimaMalik.

THANK YOU