Embed Size (px)
Citation preview

THYROID EYE THYROID EYE DISEASEDISEASE
DR K HARIPRIYASSSIHMS

Also known as TRO / Graves’ orbitopathySelf-limiting auto-immune processMild to severe irreversible sight threatening
diseaseGraves' disease is the most common thyroid
abnormality Other associations include Hashimoto's
thyroiditis, thyroid carcinoma, primary hyperthyroidism, and neck irradiation

EPIDEMIOLOGY EPIDEMIOLOGY Most common disease affecting the orbitFemale to Male ratio 9.3:1 (mild cases) 1.4:1 (severe cases)Severe cases more frequent in >50 yr age
groupCigarette smoking is the strongest modifiable
risk factorMyasthenia gravis is 50 times more common in
patients with TAO

ETIOLOGYETIOLOGY80% are clinically hyperthyroid and 10% are
clinically euthyroid◦ Associated with normal to abnormal thyroid
function In patients who are hyperthyroid, eye signs
of TAO usually develop within 18 months

Smokers have a 5 time higher risk of developing TAO
Cawood and colleagues have established that orbital fibroblasts when exposed to cigarette extract showed an increased production of Glycosaminoglycans
There is evidence that cessation of smoking reduces the risk of progression of orbitopathy

A 6.4 times risk for development of orbitopathy in Europeans compared to Asians *
Genetic predisposition 20-60% - positive family history of thyroid
disease Concordance level is 50% in identical twins
* Tellez et al.Clin Endocrinol 1992

• Increased prevalence of HLA B8, DR-3 may increase susceptibility to TAO• Higher frequency of HLA-DRB1-16 allele in TRO patients with severe extra ocular muscle involvement ** **Akaishi et al. Thyroid
2008

PATHOGENESISPATHOGENESIS


PATHOGENESIS PATHOGENESIS Immune mediated inflammatory reaction Circulating auto antibodies like TRAb, TSI are
thought to be mediators of orbitopathy also IGF-IR ( Insulin like growth factor I receptor ) is
an auto antigen expressed by fibroblastsCOX-2 ( Cyclo oxygenase -2 )Expressed at
higher levels in fibro adipose tissue of TRO patients

PATHOPHYSIOLOGYPATHOPHYSIOLOGYFibroblasts are the target cells in TAOThey are extremely sensitive to stimulation
by cytokines and immunoglobulinsStimulated fibroblasts secrete Hyaluronic
acid which is hydrophilic and causes edema in extraocular muscles
Doubling of Hyaluronic acid content causes a 5 fold increase in tissue osmotic load

COURSE OF THE DISEASECOURSE OF THE DISEASETRO has an active inflammatory phase and
a stable post inflammatory phase Duration of active phase 6-18 monthsManagement of active phase is aimed at
modulating the immune response and reducing the inflammation
Reactivation of disease occurs in less than 5 percent of individuals

STAGINGSTAGINGWERNER´S CLASSIFICATION - NOSPECS
0 Nil (no symptoms or signs)
1 Only signs of: a) stare
b) lid lag
2 Soft tissue involvement: 0) absent
a) minimal
b) moderate
c) marked

3 Proptosis of 3mm or more: 0) absent
a) 3-4 mm
b) 5-7 mm
c) 8 or more mm
4 Extra ocular muscle involvement: 0) absent
a) limitation at extremes of gaze
b) evident restriction of motion
c) fixation of globe

5 Corneal involvement: 0) absent
a) SPE
b) corneal ulceration,
c) necrosis or perforation
6 Sight loss (due to optic neuropathy): 0) absent
a) 20/20-20/60
b) 20/70-20/200
c)Worse than 20/200.

MOURITS CLASSIFICATIONClinical Activity Score ( CAS ) to grade the
inflammatory phase of the diseaseThe CAS consists of two conjunctival,
eyelid and two orbital signsA score of 4 /> - active diseaseSubjective in nature with very large
interobserver variation

Clinical Activity ScoreFor initial CAS, only score items 1-71. Spontaneous orbital pain.2. Gaze evoked orbital pain.3. Eyelid swelling that is considered to
be due to active inflammatory phase.4. Eyelid erythema.5. Conjunctival redness that is
considered to be due to active inflammatory phase.

6. Chemosis.7. Inflammation of caruncle OR plica.Patients assessed after follow-up can
be scored out of 10 by including items 8-10.
8. Increase of > 2mm in proptosis.9. Decrease in uniocular ocular
excursion in any one direction of > 8º.10. Decrease of acuity equivalent to 1
Snellen line.

THE VISA CLASSIFICATIONTHE VISA CLASSIFICATIONDevised by Peter Dolman and Jack RootmanBased on four disease pointsBasic form consists of 4 sections recording
symptoms on the left and signs on the rightEach disease activity is gradedObjective and reproducibleAppropriate management for patients in a
logical sequence


VISA INFLAMMATORY SCOREVISA INFLAMMATORY SCORE

Clinical signs in TEDClinical signs in TEDFacial signs
joffroy’s sign-absent creases in the forehead on superior gaze.
Eyelid signsKocher’s sign-staring appearanceVigouroux sign-eyelid fullnessRosenbach’s sign-tremors of eyelidsRiesman’s sign-Bruit over the eyelids

Upper eye lid signsVon graefe’s sign-lid lag on downgazeDalrymple’s sign-lid retractionStellwag’s sign-incomplete & infrequent
blinkingGrove sign-resistance to pulling the
retracted upper lidBoston sign-jerky movements of lid on down
gazeGellineck’s sign-abnormal pigmentation of
upper lidGifford’s sign-difficulty in everting the upper
lidMeans sign-increase superior scleral show
on upgaze

Lower eye lid signs
Enroth ’s sign-edema of lower lidGriffith’s sign-lid lag on upgaze
Conjunctival signs
Goldzeiher’s sign-conjunctival injection

Extraocular movement signsMoebius sign-unable to converge eyes Ballet’s sign-restriction of one or more EOMSuker’s sign-poor fixation on abduction Jendrassik’s sign-paralysis of all EOM
Pupillary signs
Knies sign-uneven pupillary dilatation in dim lightCowen’s sign-jerky contraction of pupil to light

CLINICAL FEATURESCLINICAL FEATURES1. Eyelid Retraction2. Soft Tissue Involvement3. Proptosis4. Optic Neuropathy / Exposure
Keratopathy5. Strabismus

LID LID RETRACTIONRETRACTION

Eyelid RetractionEyelid Retraction Retraction of both upper and lower eyelids
occur in 50% of patients Normally, upper eyelid rests about 2mm
below limbus, with lower eyelid resting at the inferior limbus
When retraction occurs, the sclera (white) can be seen
Causes cosmetic problem May be due to contraction of the levator
muscle by fibrosis, or be chemically induced by high thyroid hormone levels
If persists when disease is inactive, can be helped by eye lid surgery

Eyelid Retraction – Clinical Eyelid Retraction – Clinical FeaturesFeaturesClinical signs:
◦Lid retraction in 1º (front) gaze
◦Lid lag i.e. delayed descent of upper lid in downgaze
◦Staring appearance of the eyes

SOFT TISSUE SOFT TISSUE INVOLVEMENTINVOLVEMENT

Soft Tissue Involvement - Soft Tissue Involvement - SymptomsSymptomsVariable grittinessPhotophobiaLacrimation - watery eyes

Soft Tissue Involvement - Soft Tissue Involvement - SignsSignsPeriorbital and lid swellingConjunctival hyperaemia
Sensitive sign of disease activityChemosis (edema of the
conjunctiva) Severe cases: conjunctiva prolapses over lower
eyelid

PROPTOSISPROPTOSIS

Proptosis(exophthalmos)Proptosis(exophthalmos) Proptosis is axial TED is the most common
cause of both bilateral and unilateral proptosis in adults
Proptosis is uninfluenced by Rx of hyperthyroidism and is permanent in 70% of cases
Severe proptosis prevents adequate lid closure, and may lead to severe exposure keratopathy and corneal ulceration

OPTIC NEUROPATHYOPTIC NEUROPATHY
Serious complication affecting about 5% of patients
Caused mainly through direct compression of the optic nerve or its blood supply by enlarged and congested rectus muscles at the orbital apex
May occur in the absence of proptosisCan cause severe but preventable visual
impairment

An early sign is decreased colour visionSlow progressive impairment of visual acuity
6/6 to 6/9 Va in 18% of cases Relative afferent pupillary defect -35%Visual defects, especially central scotomas –
66% Swollen or pale disc - 52%

CORNEAL CORNEAL INVOLVEMENTINVOLVEMENT
Exposure keratitis may result from proptosis, upper eyelid retraction, lower eyelid retraction, lagophthalmos, or a combination of these

OCULAR MOTILITY OCULAR MOTILITY PROBLEMSPROBLEMS
30% - 50% A defect in elevation
is most common due to fibrosis of inferior rectus muscle
IR>MR>SR>LR

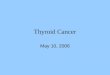
CT SCAN

MRI SCAN

VISUAL FIELDVISUAL FIELD
Characteristically a central scotoma / an inferior altitudinal defect is seen in cases of compressive optic neuropathy
Other visual field defects include an enlarged blind spot, para central scotoma, nerve fibre bundle defect, or generalized constriction

TREATMENTTREATMENT
Compressive optic neuropathy Inflammation Motility disordersEyelid abnormalities

COMPRESSIVE OPTIC COMPRESSIVE OPTIC NEUROPATHYNEUROPATHYThe treatment possibilities include high doses
of corticosteroids, irradiation,immunosupressants and orbital decompression.
Some patients require only one of these modalities, while other patients need combined therapies.

CORTICOSTEROIDSCORTICOSTEROIDSIntra-venous Methyl Prednisolone 1 gm
alternate days for 3-6 cyclesCumulative dose not to exceed 6-8 gmEffective in 63-77% *No response in 48 hours - Steroids probably
will not work * Rajendran et. al, CIRTED trial

RADIATION THERAPYRADIATION THERAPYLymphocytes infiltrating the orbit are highly
sensitive to Radiation. The glycosaminoglycan production by fibroblasts is reduced
Dose =1500- 2000 cGy per eye fractioned over a period of 2 weeks
Co coverage with steroidsA relative contraindication in diabetics

Although congestive findings improve most consistently, significant improvement in proptosis and extra ocular muscle function has been reported.
Radiation therapy is most effective within the first year, when significant fibrotic changes have not yet occurred.

ORBITAL DECOMPRESSIONORBITAL DECOMPRESSION
Indicated for compressive optic neuropathy when there has been failure of or contraindication for corticosteroids or radiation therapy
Gross proptosis with exposure keratitis and corneal ulceration
Cosmesis for disfiguring exophthalmos.

ORBITAL DECOMPRESSIONORBITAL DECOMPRESSION
The swinging lower lid approach to inferior and medial wall decompression is the most common approach used by ophthalmologists.
Medial wall decompression to extend posteriorly for compressive optic neuropathy

Medial wall removal not to extend above the fronto ethmoidal suturePreservation of a strut of bone between ethmoid
and maxillary bonesLateral wall removal has little effect on apical
compressionFour wall decompression requires a neurosurgical
approachOrbital fat decompression for reducing proptosis

AFTER 3-WALL DECOMPRESSION & AFTER 3-WALL DECOMPRESSION & FAT EXCISIONFAT EXCISION


ACTIVE INFLAMMATIONACTIVE INFLAMMATION
Treatment depends on inflammatory scoreScore <4 - conservative managementScore > 5 – more aggressive therapy Oral/IV steroids Radiotherapy Immunosuppressive agents

Soft Tissue Involvement - Soft Tissue Involvement - RRxxFrequently unsatisfactory, may be of
some benefit Topical Rx – lubricants (artificial tears &
ointment) reduce irritation caused by conjunctival inflammation and mild corneal exposure
Elevating the head end of bed during sleep may decrease periorbital oedema. Diuretics given at night may also reduce the morning accumulation
Taping of eyelids at night may be useful for mild exposure keratopathy

MOTILITY DISORDERSMOTILITY DISORDERS A major source of morbidity in thyroid
orbitopathy, and the most frequent problem associated with orbital decompression surgery
Minimal degrees of ocular misalignment - compensatory head posture, Fresnel plastic press-on prisms, or temporary occlusion
If there is marked asymmetry in ocular deviation in different fields of gaze, prisms are less effective

Surgery is usually considered if there is diplopia in primary gaze or reading position
Diplopia must have been stable for about 6 months
Rx is by muscle surgery, with the aim of producing binocular vision when looking forward, and good cosmetic result
Botulinum toxin injection (Botox) to relax muscles may be useful in selected cases

EYELID ABNORMALITIESEYELID ABNORMALITIESMild eyelid retraction does not require Rx, in
50% of cases, there is spontaneous improvement
Rx of associated hyperthyroidism may also improve lid retraction
Main indications are exposure keratopathy and poor cosmesis

A graded Muller’s and levator aponeurosis weakening abnormalities(recession of lower lid retractors,mullertomy)
Blepharoplasty is the final surgical procedure in the rehabilitation of TRO patient
Orbital decompression is performed initially followed by strabismus surgery and then eyelid surgery


No effective means of preventing the disease or reliably altering it’s course
Current therapeutic options aimed at reducing the inflammation during active stage and correction of residual abnormalities secondary to fibrosis in the inactive stage
Intervention not targeting the cause because the precise pathogenesis is still elusive
TO CONCLUDE...

TRO is a self limiting diseasePatient educationStopping smoking
Newer medical therapies like anti CD 20 (Rituximab) to deplete B- cell lymphocytes, anti TNF drugs, Pentoxyfylline and nicotinamide which inhibit cytokine induced glycosaminoglycan synthesis ,intravenous immunoglobulin are being tried

More studies are required to determine the risk benefit ratio of these new modalities
Recent advances in molecular biology, identification of multiple genes and auto antigens with a possible role in thyroid orbitopathy may pave a way in preventing this common yet poorly understood disease