Embed Size (px)
Citation preview

The use of bisphosphonate for patients
on glucocorticoid therapy for the
prevention of osteoporosis
Prepared by: Sara AbudahabSupervised by: Dr. Amal AkourDepartment of Clinical PharmacyUniversity of Jordan

Identifying the question
PICOT• Population: adult patients who take long term glucocorticoid
therapy (for 3 months or more)
• Intervention: bisphosphonate as a prophylaxis therapy for prevention of osteoporosis
• Comparison : patients on placebo or on VitD and Calcium therapy
• Outcome: Bone mineral density (BMD)and prevention of Fractures
• Time: up to 12-24 months follow-up

Introduction
• Glucocorticoids may effectively be used in the management of many inflammatory conditions but their use is associated with significant morbidity and mortality.
• Osteoporosis, with resultant fractures, constitutes one of these morbid complications and is associated with significant pain and disability.
• A rapid decline in bone mineral density (BMD) begins within the first 3 months of glucocorticoid use and peaks at 6 months, followed by a slower steady loss with continued use.
Introduction
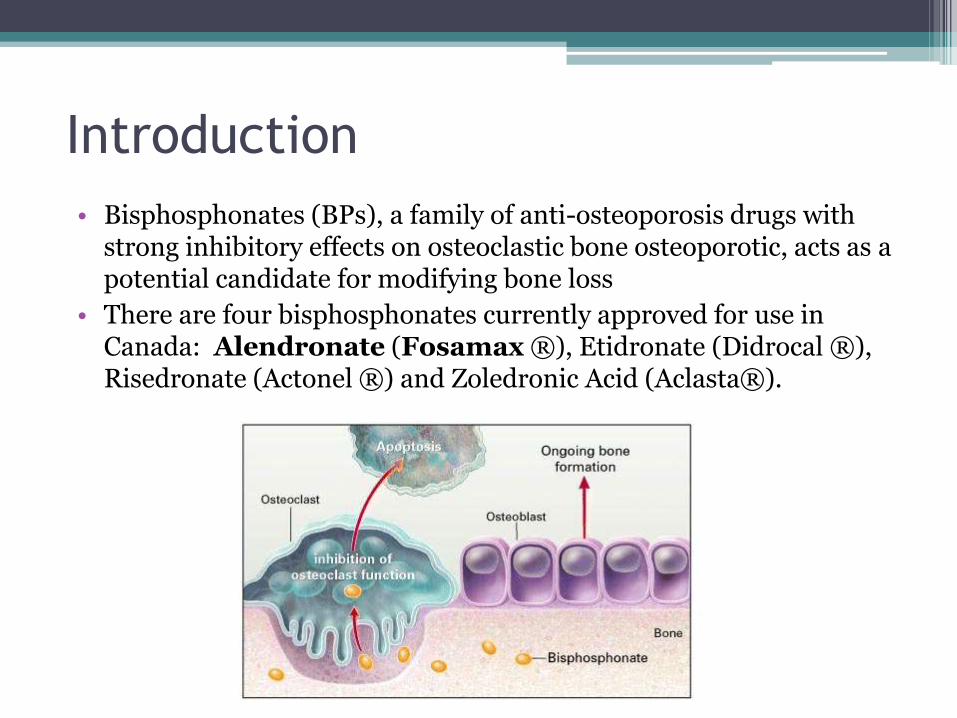
• Bisphosphonates (BPs), a family of anti-osteoporosis drugs with strong inhibitory effects on osteoclastic bone osteoporotic, acts as a potential candidate for modifying bone loss
• There are four bisphosphonates currently approved for use in Canada: Alendronate (Fosamax ®), Etidronate (Didrocal ®), Risedronate (Actonel ®) and Zoledronic Acid (Aclasta®).
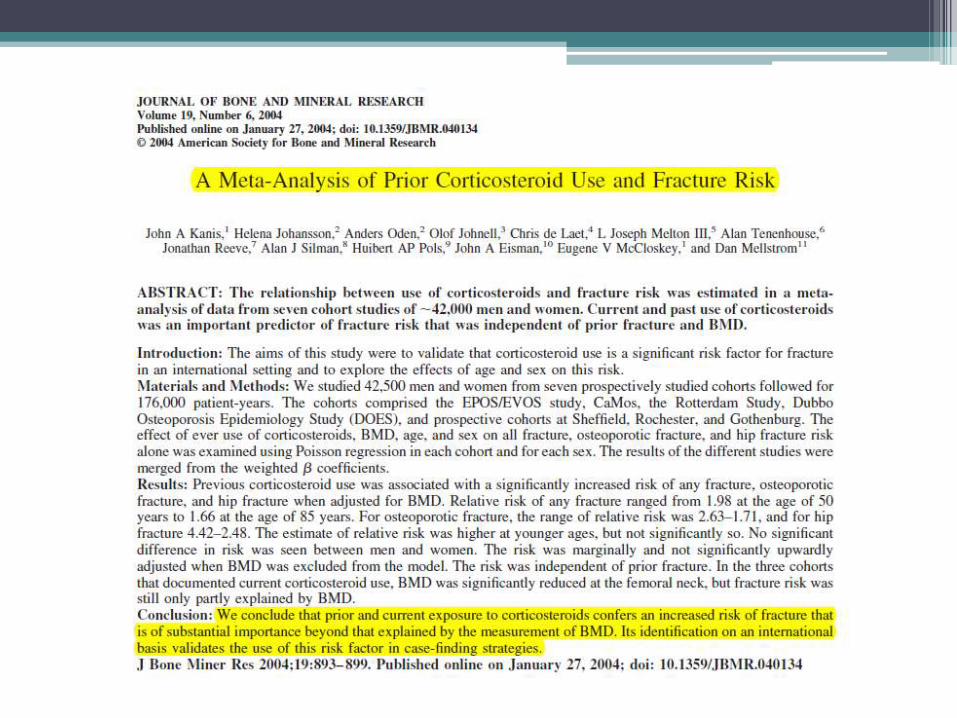

A Meta-Analysis of Prior Corticosteroid
Use and Fracture RiskMaterials and Methods: We studied 42,500 men and women from seven prospectively studied cohorts followed for 176,000 patient-years.
The effect of ever use of corticosteroids, BMD, age, and sex on all fracture, osteoporotic fracture, and hip fracture risk alone was examined using Poisson regression in each cohort and for each sex.
Conclusion: We conclude that prior and current exposure to corticosteroids confers an increased risk of fracture that is of substantial importance beyond that explained by the measurement of BMD. Its identification on an international basis validates the use of this risk factor in case-finding strategies.
Source: Journal of Bone and Mineral ResearchImpact Factor: 5.622
Evidence used:
1- Z Feng, et al “Bisphosphonates for the Prevention and Treatment of Osteoporosis in Patients with Rheumatic Diseases” (December 2013), Plos One : 8 (12)
2- Allen CS, et al “Bisphosphonates for steroid-induced osteoporosis”, (October 2016), Cochrane Library, Issue 10. Art. No.: CD001347

A meta analysis 2013

Study characteristics
Methodology:
We searched PubMed, EmBase, and the Cochrane Central Register of Controlled Trials for relevant literatures with a time limit of Jan. 6, 2012.
All randomized clinical trials of BPs for adult rheumatic patients with a follow-up of 6 months or more were included.
Total of 2o trials
Doses and route of administration used:
• Intervention: The intervention was the use of any generation of BPs, alone or together with calcium and/or vitamin D, irrespective of administered approach. The intervention in control group was placebo, alone or together with calcium, vitamin D, and calcitonin.
• Eight trials were prevention trials, defined as starting BPs treatment in the first three months of GC therapy
• Eleven trials were classified as treatment trials because BPs was given for long-term GC user. ▫ Of these 11 treatment trials, the mean dosage of GC
consumption was greater than 7.5 mg/day (prednisone equivalent) in 6 trials,
▫ less than 7.5 mg/day in 5 trials • No GC usage in 1 trial

Principal Findings: • The RR in rheumatic patients treated with
BPs was 0.61 (95%CI [0.44, 0.83], P = 0.002) for vertebral fractures, and 0.49 (95%CI [0.23, 1.02], P = 0.06) for non-vertebral fractures.
• The WMD of BMD change in the lumbar spine was
3.72% (95%CI [2.72, 4.72], P,0.001) at 6 months,
3.67% (95%CI [2.84, 4.50], P,0.001) at 12 months,
3.64% (95%CI [2.59, 4.69], P,0.001) at 24 months,
and 5.87% (95%CI [4.59, 7.15], P,0.001) at 36 months in patients using BPs, as compared with those treated with calcium, vitamin D or calcitonin.
In subgroup analyses, rheumatic patients using BPs for osteoporosis prevention had greater WMD than those using BPs for treating osteoporosis at 6 months (4.53% vs. 2.73%, P = 0.05) and 12 months (4.93% vs. 2.91%, P = 0.01).

Biophosphonates for vertebral fracture of rheumatic patients. Pooled estimate for the relative risk of vertebral fractures (a) and relative risk of vertebral fractures at 12 months (b)
Forest Plot for vertebral fracture

Forest Plot for vertebral fractures cont.
relative risk of vertebral fractures 24 months (c), and 36 months (d)

Forest Plot for non-vertebral fractures

Conclusions/Significance:
BPs can preserve bone mass and reduce the incidence of vertebral fractures in rheumatic patients, mainly for those who have GC consumption.
The efficacy of BPs is better when using BPs to prevent rather than to treat osteoporosis in rheumatic patients.
• Journal name: PLOS ONE
• Impact factor: 3.234

A meta analysis 2016
Study characteristics
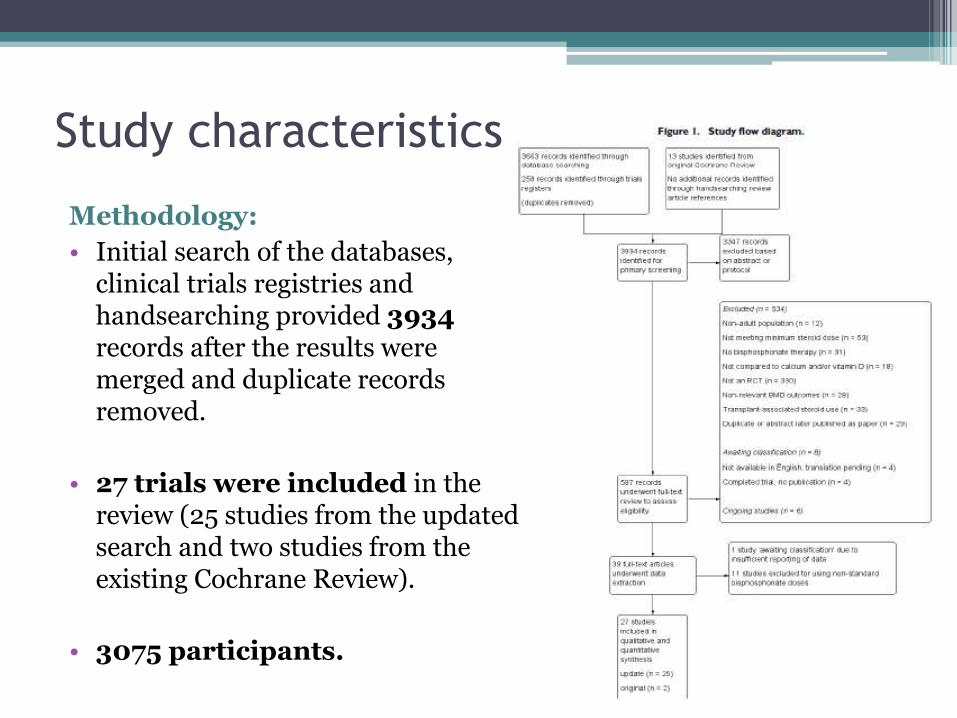
Methodology:
• Initial search of the databases, clinical trials registries and handsearching provided 3934records after the results were merged and duplicate records removed.
• 27 trials were included in the review (25 studies from the updated search and two studies from the existing Cochrane Review).
• 3075 participants.

Principal Findings:
1. Analysis: benefits - fractures (Incident radiographic vertebral fractures)
2. Analysis: benefits - fractures (Incident radiographic non-vertebral fractures)
3. Analysis: benefits - bone mineral density (BMD) at lumbar spine (LS)
4. Analysis: benefits - bone mineral density (BMD) at femoral neck (FN)
5. Analysis: harms (Serious adverse events)

Dose and route of administration used:
• We included randomized controlled trials (RCTs) satisfying the following criteria:
1) prevention or treatment of GIOP; 2) adults taking a mean steroid dose of 5.0 mg/day or more; 3) active treatment including bisphosphonates of any type alone or in combination with calcium or vitamin D; 4) comparator treatment including a control of calcium or vitamin D, or both, alone or with placebo; and 4) reporting relevant outcomes. We excluded trials that included people with transplant-associated steroid use.
Route used: IV and Oral (please check the next slide)

•Dose and route of administration used:


Principal Findings (vertebral fractures):
• Pooled analysis for incident vertebral fractures included 12 trials (1343 participants) with high-certainty evidence and low risk of bias.
• In this analysis 46/597 (or 77 per 1000) people experienced new vertebral fractures in the control group compared with 31/746 in the bisphosphonate group ▫ relative improvement of 43% (9% to 65% better) with
bisphosphonates▫ absolute increased benefit of 2% fewer people sustaining
fractures with bisphosphonates (5% fewer to 1% more)▫ number needed to treat for an additional beneficial
outcome (NNTB) was 31 (20 to 145) meaning that approximately 31 people would need to be treated with bisphosphonates to prevent new vertebral fractures in one person.
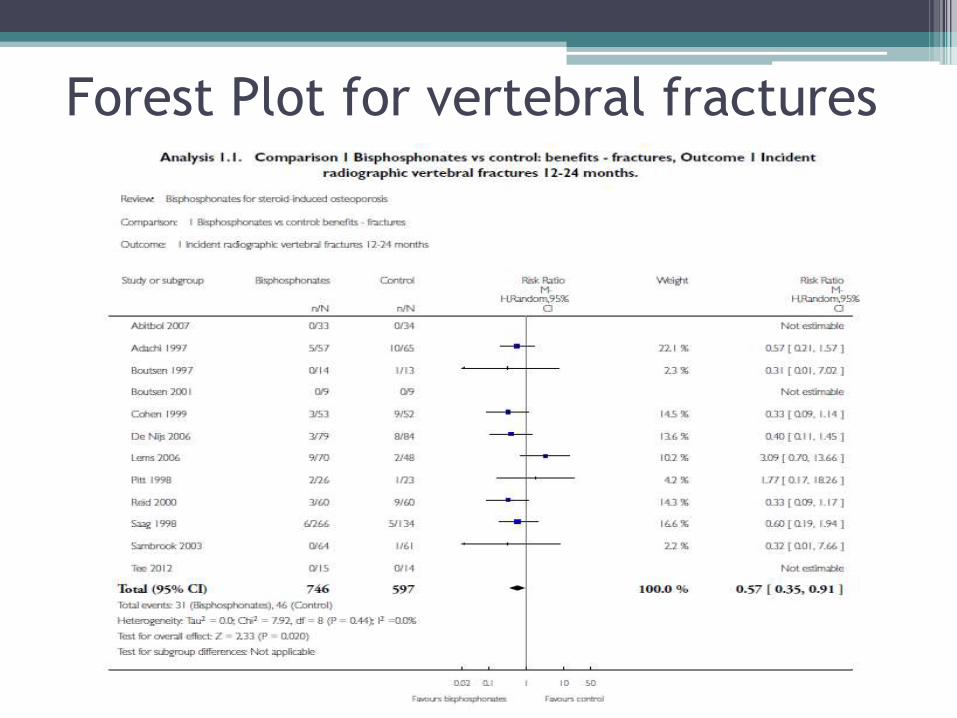
Forest Plot for vertebral fractures

• Pooled analysis for incident non-vertebral fractures included nine trials with 1245 participants with low-certainty evidence (downgraded for imprecision and serious risk of bias as a patient-reported outcome).
• In this analysis 30/546 (or 55 per 1000) people experienced new nonvertebral fracture in the control group compared with 29/699 (or 42 per 1000; range 25 to 69) in the bisphosphonate group;
• relative improvement of 21% with bisphosphonates (33% worse to 53% better);
• absolute increased benefit of 1% fewer people with fractures with bisphosphonates (4% fewer to 1% more).
Principal Findings (non-vertebral fractures):

Forest Plot for non-vertebral fractures

Principal Findings (BMD):
• Pooled analysis on BMD change at the lumbar spine after 12 months included 23 trials with 2042 patients.
▫ Evidence for both outcomes was moderate-certainty (downgraded for indirectness as a surrogate marker for osteoporosis) with low risk of bias.
• Overall, the bisphosphonate groups reported stabilization or increase in BMD, while the control groups showed decreased BMD over the study period.

Forest Plot for BMDLumbar Spine Femoral Neck

Serious adverse events
• Pooled analysis on serious adverse events included 15 trials (1703 participants) with low-certainty evidence (downgraded for imprecision and risk of bias).
• In this analysis 131/811 (or 162 per 1000) people experienced serious adverse events in the control group compared
• to 136/892 (or 147 per 1000; range 120 to 181) in the bisphosphonate group;
• absolute increased harm of 0% more serious adverse events (2% fewer to 2% more);
• a relative per cent change with 9% improvement (12% worse to 26% better).

Forest Plot for serious adverse events

Conclusions/Significance:• There was high-certainty evidence that bisphosphonates
are beneficial in reducing the risk of vertebral fractures with data extending to 24 months of use.
• There was low-certainty evidence that bisphosphonates may make little or no difference in preventing nonvertebralfractures.
• There was moderate-certainty evidence that bisphosphonates are beneficial in preventing corticosteroid-induced bone loss at both the lumbar spine and femoral neck.
• Regarding harm, there was low-certainty evidence that bisphosphonates may make little or no difference in the occurrence of serious adverse events or withdrawals due to adverse events.

Conclusions/Significance:
• Overall, our review supports the use of bisphosphonates to reduce the risk of vertebral fractures and the prevention and treatment of steroid-induced bone loss.
• Journal Name: Cochrane Database of Systematic Reviews (CDSR)
• Impact factor: 6.103



















![CHAPTER 11 BONE MARROW ADIPOGENESIS IN OSTEOPOROSIS chapters... · with conditions that lead to bone loss or osteoporosis, such as aging [1, 2], disuse [3, 4], long-term glucocorticoid](https://img.dokumen.tips/doc/110x75/601eb5077a3fcb54d13dccf1/chapter-11-bone-marrow-adipogenesis-in-chapters-with-conditions-that-lead-to.jpg)









