Embed Size (px)
DESCRIPTION
My Talk for emergency nurses on resuscitating the upper GI bleeder in the emergency department!
Citation preview

The Upper GI Bleeder
By Kane Guthrie FCENA

Upper GI Bleeds
• Understand the causes• Goals of resuscitation• Pharmacological resuscitation• Procedural resuscitation

Upper GI Bleeds in ED
• Its challenging• Effective Mx = good PT outcomes• Underlying comorbidities ∧ complexities• Team approach• Pharmacology & procedural approach

Upper Vs Lower
• Consider upper first– More life threatening
• Haematemisis = Upper GI source• Bright red blood not always = LOWER GI

Case Study
• 52 Male• Chronic ETOH abuse• Known varices
C/O – Vomiting blood post binge

What to Look for!

His Vitals

The Upper GI Bleeder
Multi Team Approach:• ED, ICU – resuscitate• Gastro – scope• Interventional Radiologist – therapeutic Ix• Surgeons – surgical intervention

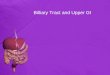
The Source
• Duodenal ulcers- 28%• Gastric ulcers- 26%• Gastritis- 13%• Varices - 12%• Esophagitis - 8%
• “Massive GI Bleed Mortality rate 20-39%”

The DDx!
• Intranasal• Intrapulmonary

Remember!
Early Interventioncan mean
difference between
Life & Death

The 3 Goals of Resuscitation
1 Provide Intravascular Volume Resuscitation
2 Optimise Oxygen-Carrying Capacity
3 Reverse Coagulopathy

Initial Resuscitating
• Start with ABCDE• x2 Large bore IVC – Bloods• Full monitoring• Get specialties involved• Arrange blood products• Consider limitations of care!

Intravascular Volume Resuscitation
• Limit crystalloid fluid –to early phase
Prepare for transfusion:• HB <80• Coagulopathy• Persistent hypotension

Intravascular Volume Resuscitation
• PRBC’s not enough• Replace clotting factors• Consider massive transfusion protocol• “PRBC:FFP:platelet ratio 1:1:1”
• Tranexamic Acid?

Optimise Oxygenation
Signs of decreased O2 delivery:– Decreased LOC– Evidence of cardiac ischaemia– Increased lactate– Cold peripheries

Optimise Oxygenation
• Give blood so oxygen can get to the tissue
Initially:– Provide High Flow 02
Crashing:• Intubate early
Stablised:• Titrate oxygen to need• Considered humidified

Intubating Isn’t Easy!
1. Intubate early2. Empty stomach (NGT)3. Intubate with HOB at 45°4. Preoxygenation5. Limit BVM6. Use experience7. Prepare for vomit


Reverse Coagulopathy
• Tailor to etiology.
Causes:• Anticoagulation• Shock– Metabolic acidosis –tissue hypoperfusion
• Chronic disorders– ETOH abusers

Pharmacological Interventions
• Proton Pump Inhibitors• Somatostatin• Vasopressin

Proton Pump Inhibitors
• Suppress gastric acid production• Potential reduction haemorrhage during scope
The evidence though:

Somatostatin
• (Octreotide)Reduces:• Portal venous blood flow• Splachinic vasoconstriction
=decrease GI Bleeding
Use• Variceal GI bleeds• Limited evidence – low side effect profile

Vasopressin
(Telipressin)• Reduces portal hypertension• Splachnic vasoconstrictor• Can cause ischaemia
• Last ditch effort in bleeding varices

Antibiotics
• Infection on varices– Causes bleeding
• Give antibiotics (broad spectrum)

Procedural Interventions
• Endoscopy• Balloon Tamponade

Endoscopy
• Diagnostic & therapeutic tool
Interventions:• Clips• Banding• Thermocoagulation• Sclerosant injection % adrenaline

Balloon Tamponade


Balloon Tamponade
• Temporising rescue device
Indicated:– Endoscopy not available– Endoscopy not successful
• Need to secure airway prior

Questions

Take Home Points
• Early recognition• Team approach is needed• Resuscitate with blood products• Advocate for early intervention