Embed Size (px)
Citation preview

Jozef Kesecioglu
How should an ideal Intensive Care Unit
and Team be?
Florence Nightingale
keep critically ill patients together in one separate place for special nursing care
1852
First Intensive Care Units
many years later
■ specialized
personnel
■ mainly focused on
improvement of
illness
■ patients together in
special wards

New Intensive Care Units
developments
■ well being of
personnel and
safety procedures
documented
■ insight on mental
stress of patient
and family


modify procedures and
choose equipments
build upon needs of
patient and family
developments

First step in new design
define a vision
create the best
environment for
critically ill patients and
their relatives
environment allows
personnel to focus
on patient
Tools for improvements
interview former patients and their family members
create a mock-up room to test optimal functioning

Where to begin?
different approach
patient centered care
dictates architecture
and interior
functionality and safety
defines concepts


Patient
centered
care

Patient needs - private rooms
privacy
quiet
decrease infection
decrease medication
errors
improve family support
improve communication
increase satisfaction

Patient needs - natural light
day & night
reduce agitation
decrease stay
decrease pain
medication
reduce depression
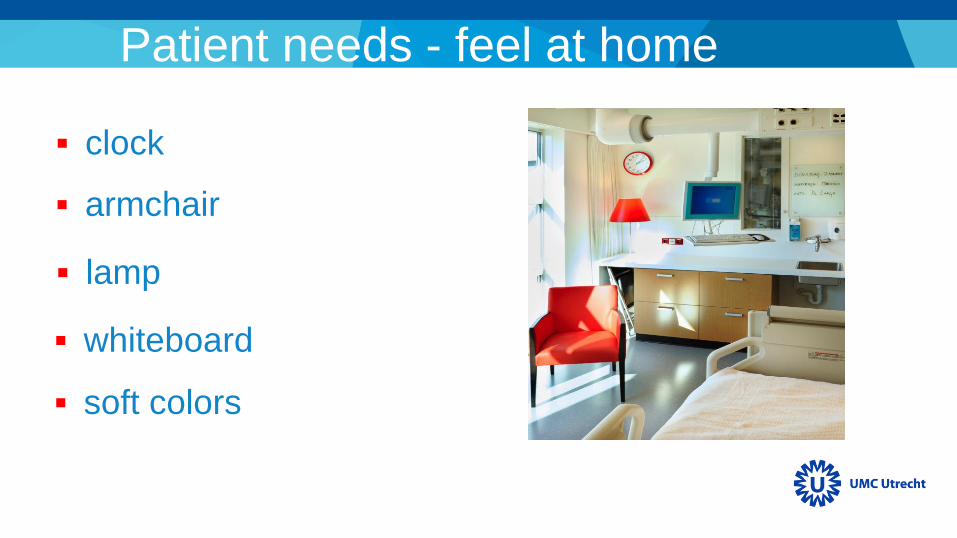
Patient needs - feel at home
clock
armchair
lamp
whiteboard
soft colors


Needs of
the family
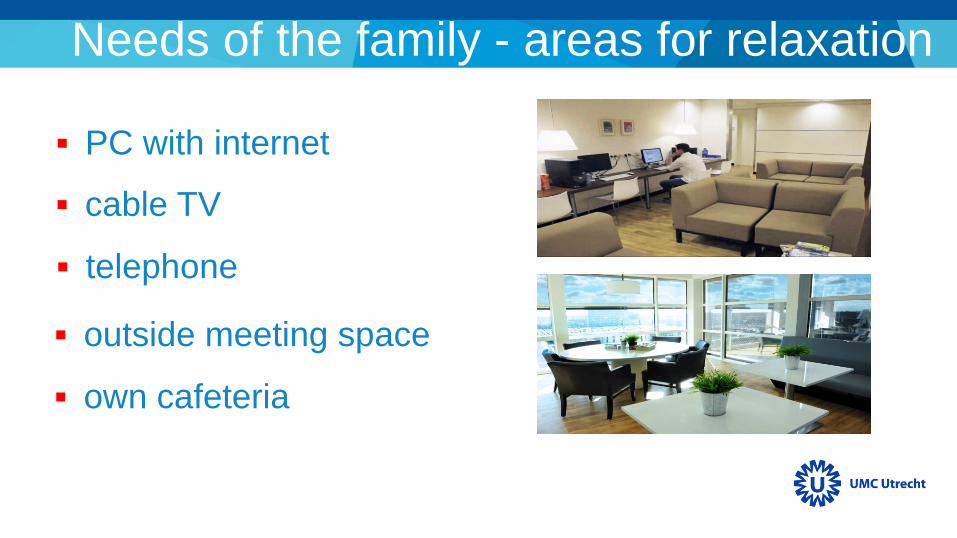
Needs of the family - areas for relaxation
PC with internet
cable TV
telephone
outside meeting space
own cafeteria

Needs of the family - signage/way finding
patient room numbers
directional signage
multilingual signage
way finding techniques
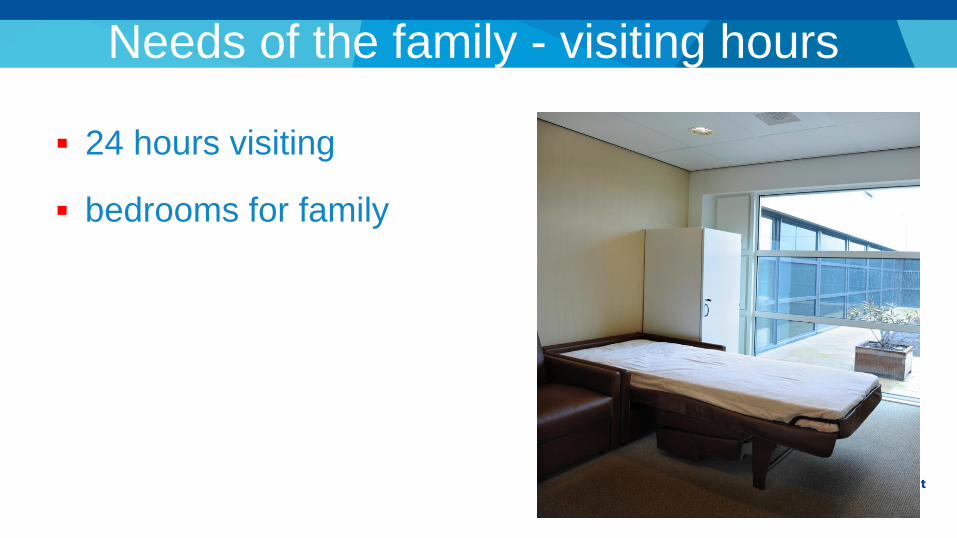
Needs of the family - visiting hours
24 hours visiting
bedrooms for family

Functionality
and safety

Functionality and safety - develop concepts
physician/nurse at
bedside or nearby
ergonomics
safety

Physician/nurse at bedside or nearby
“race track” configuration
with zones single room on periphery
of common corridor
decentralize care
outside view and natural
lightning workstation and window
between 2 rooms
Pysician/nurse at bedside or nearby
simple with minimal
alarms remote monitor at each
desk
selection equipment
evenly spreading of
personnel doors closed for quiet
atmosphere
Equipment according to concepts
select equipment that fits to the concepts developed
develop concepts after selection of equipment
NOT
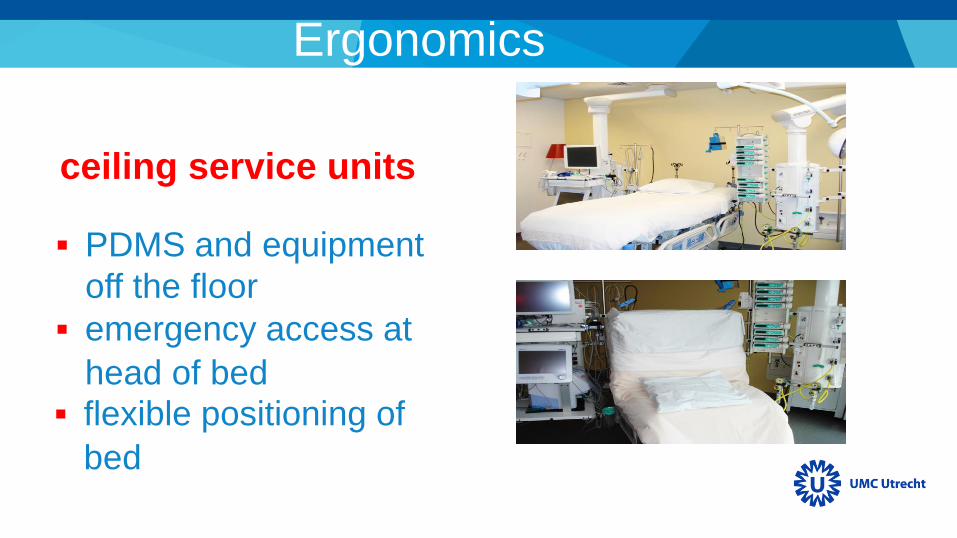
Ergonomics
PDMS and equipment
off the floor
emergency access at
head of bed
ceiling service units
flexible positioning of
bed

Safety
patient alarms
logistics
pharmacy
Patient alarms and logistics
bleeper and smart
phone
24 hours supplies and
brought daily
daily change of drawers
Medication errors/adverse drug events
satellite pharmacy in
ICU
automated dispensing
devices
barcode medication
medication checked by
pharmacist
medication ready to use

Jongerden I.P. et al. Intensive Care Med. 2013; 39: 1626–1634

• Daylight
• Privacy
• Quiet atmosphere
• Family facilities
• Visiting hours
Jongerden I.P. et al.
Intensive Care Med.
2013; 39: 1626–1634
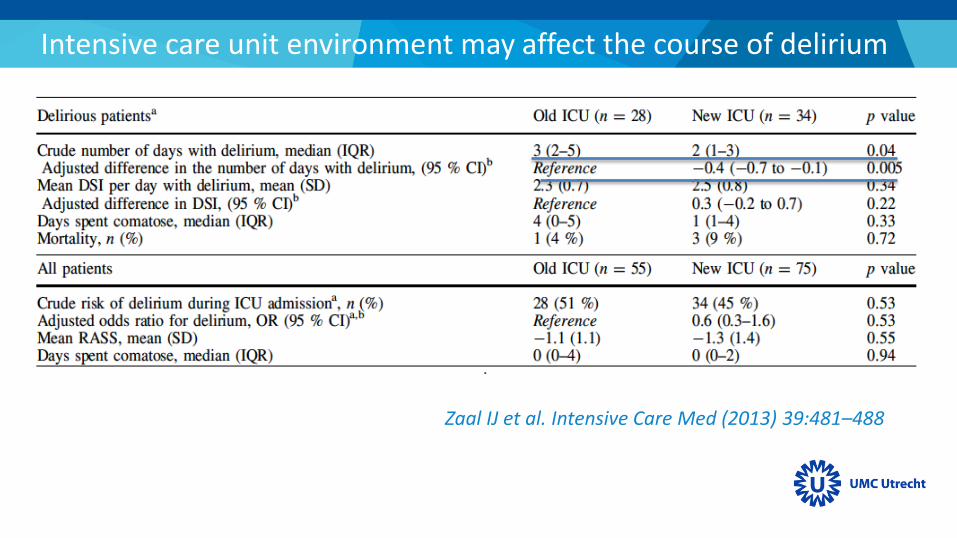
Intensive care unit environment may affect the course of delirium
Zaal IJ et al. Intensive Care Med (2013) 39:481–488
Conclusion
organization structured on needs of patient and
family is mandatory
develop concepts leading to architecture and
medical equipments
concepts as daylight, quiet surrounding, privacy,
ergonomics and safety will always be the future
materials, apparatus and building can get outdated
BUT
environment is an important factor in family and patient
satisfaction
single-room design improves satisfaction as compared
with an ICU with multiple beds on a ward
family and patient satisfaction with ICU experience
increases in an ICU environment consisting of noise-
reduced, single rooms with daylight, adapted coloring
and improved family facilities
Conclusion
Team
Open vs Closed format
Specialized vs Multidisciplinary
Workload
Nurses
Physicians
Background of physicians
Team
The risk of death was increased by:
3.5 (95% CI, 1.3–9.1) when the patient-to-nurse
ratio was greater than 2.5
2.0 (95% CI, 1.3–3.2) when the patient-to-physician
ratio exceeded 14
Neuraz A et al. Crit Care Med 2015; 43:1587–1594
Team
Open vs Closed format
Specialized vs Multidisciplinary
Workload
Nurses
Physicians
Background of physicians

© ESICM – Confidential document 48
TOPIC:
THE ART OF TRAUMA
RESUSCITATION

© ESICM – Confidential document 49
ESICM 28th Annual Congress