Embed Size (px)
DESCRIPTION
This presentation was given at the 2008 AFAO HIV Educators conference.
Citation preview

Conceptualising StigmaSkills WorkshopPresented by Daniel Reeders Campaign Coordinator, PLWHA Victoria
NAPWA Health Promotion & Education Network

Discrimination
Status Loss Separation
Stereotyping
Labelling
STIGMA
Component Model (Link & Phelan 2001)
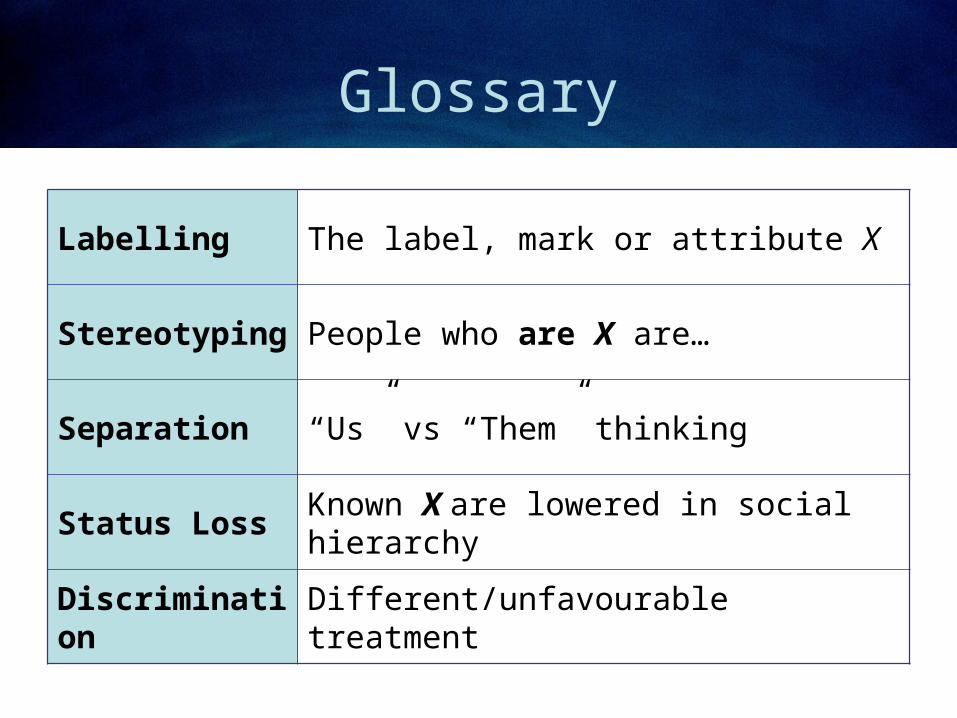
Glossary
Labelling The label, mark or attribute X
Stereotyping People who are X are…
Separation “Us” vs “Them” thinking
Status Loss Known X are lowered in social hierarchy
Discrimination Different/unfavourable treatment

Labelling Separation Stereotyping Status Loss Discrim
Do the components have to occur IN SEQUENCE?
1 2 3 4 5
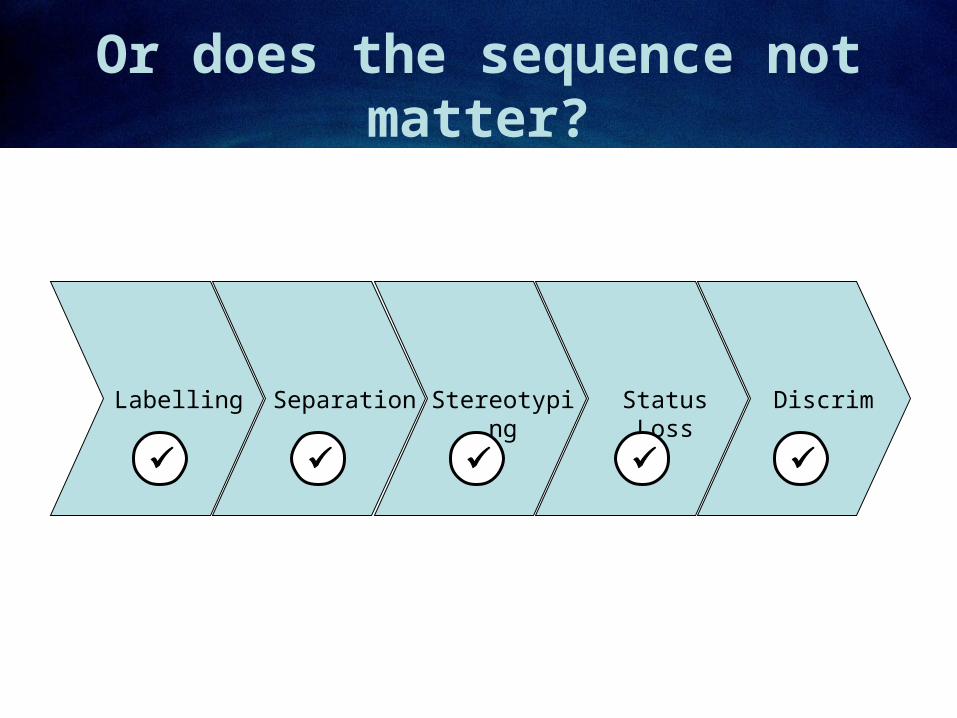
Labelling Separation Stereotyping Status Loss Discrim
Or does the sequence not matter?

Discrimination
Status Loss Separation
Stereotyping
Labelling
STIGMA
Exclusive Definition – if one component is missing, there is NO STIGMA (but possibly something else)

Discrimination
Status Loss Separation
Stereotyping
Labelling
STIGMA
Language choice – people who inject drugs are “junkies”
“Junkies” are violent criminals
“Junkies” are not people like us
“Junkies” are the lowest of the low
But on a talkback radio show there’s no individual who’s being treated differently – it’s a social process of generating & sustaining the meaning of the term “Junkie” and the related stereotype, which may later enable stigmatisation – but isn’t currently an example of it.
Nonetheless it’s something we might want to target in a stigma campaign!
Example – Social Regulation via Stereotypes

Discrimination
Status Loss Separation
Stereotyping
Labelling
STIGMA
“…because I only do it bareback…”
“…because I really like you and I need some time to think about what that means…”
Example – Sexual Rejection might not be stigma
Disclosure – “I’m HIV-positive”
Everyone has prior expectations about PLWHA
Thinks – “Okay, but I’m negative…”
Says – “I’d rather not have sex with you tonight…”

Stereotyping
• Stigma is not the same as stereotyping• Stereotypes are not “incorrect images” that
we can “correct” with “increased visibility”• They persist because they have social
meaning and utility – allow generalisation and judgment
• For example, imagine landing in a foreign country and treating every single new fact as particular and individual – exhausting!

Judgment
• Who can I safely have bareback sex with?• Who can I safely disclose my status to?• Who can I ask about the nearest NSP?• Who can I pay for sex?• Who can sell me half a gram of crystal?• Who will help me when I’m about to drop?
How do you know who to ask? Consequences of asking wrong?

Elaboration
Pre-Encounter
Totally relies on stereotype for judgment
Encounter
Challenges stereotype and initial judgment
Engagement
Development of a rich and individualised understanding over time – complex judgments

Social Research
Stigma in Australia and Overseas

Male Call
Sexual Rejection
• 70% of negative men wanted positive men to disclose their status before sex
• 80% would then reject the positive man

Male Call
However, remember…
• 80% of 70% is 56% overall
• The survey was conducted in 1999

Common Threads
Positive Pregnancy
• Respondents often reported having a really negative experience for their first pregnancy, followed by a much better experience the second time around

Futures
Disclosure Patterns• Steadily declining in all categories since
the first study in 1999• As a proxy measure for the prevalence of
stigma, does this mean more, or less?• Could mean more fear about disclosing
(Gorbach et al, 2004)• But stigma requires labelling and less
disclosure might prevent possible stigma

(Public Discourse)
• The past five years have seen a strong shift towards attributing blame for HIV infection to the people infected with it, driven by images of barebacking and bugchasing (Reeders, 2006)
• Attribution of blame is a proxy attitude for measuring stigma (Herek, ???)
• Disclosure is less safe in this environment• But it may reflect PLWHA taking more control of
public knowledge of their status: Sean Slavin.

American ResearchGregory Herek
Telephone cross-sectional 1991-99• Previous research has shown that AIDS stigma is expressed in a
variety of ways. Accordingly, the survey protocol assessed multiple facets of it. Questions were included about support for stigmatizing AIDS policies (quarantine, publicly identifying PWAs), support for mandatory testing (of pregnant women, immigrants, and people perceived to be at high risk), attributions of responsibility and blame to PWAs (the belief that PWAs are responsible for their disease, that they deserve it), beliefs about PWAs (that they do not care about infecting others), affective responses to PWAs (anger, fear, disgust), and discomfort with and avoidance of PWAs in hypothetical situations (having one’s child attend school with a PWA, working in an office with a PWA, patronizing a neighborhood grocer who has AIDS). (2002)

Herek1. “Stigma is more often attached to a disease whose causes is
perceived to be the bearer’s responsibility.”2. “Greater stigma is associated with illnesses and conditions that are
unalterable or degenerative… Being diagnoses with such a disease is often regarded as equivalent to dying and those who are diagnosed may represent a reminder – or even the personification – of death and mortality.”
3. “Greater stigma is associated with conditions that are perceived to be contagious or to place others in harm’s way.” This may be expressed in “continuing [ie persistent] overestimation of the risks posed by casual contact” and “the passage of laws that criminalize acts that might transmit HIV, such as unprotected casual intercourse”.
4. “Finally, a condition tends to be more stigmatised when it is readily apparent to others.”

Herek
• Instrumental Fear (of infection) vs Symbolic Associations (with risk groups)
Herek (1999)

Herek
• Stronger attributions of blame seen when infection fed into group stereotype
• In that study, Black participants attributed more blame if the PLWHA in a given scenario was Black rather than White
Implications for… Gay community? CALD communities? CALD+Gay? PLWHA (“In this day and age!”)

Perspective
Consider both sides of the stigma equation –
the STIGMATISED individualthe STIGMATISING individual
Victim vs Perpetrator?

Psychology, Briefly
The sides and different functional areas of the brain are frequently mutually inhibitory.
For example, we have two nervous systems related to fight/flight – one to make us anxious and one to calm us back down.
Language functions (neocortex) and strong emotions (archaecortex) work the same.
Rational thought <> Strong emotion

“Perpetrator”
• “Condoms are not enough protection”
• Clearly non-rational – temptation is to conclude ‘this person is really prejudiced’
• Alternatively, they may know the reasons why condoms are enough protection, but thinking about sex with an HIV+ person causes them great anxiety
• Result is fear management (rejection)
(aside)
• Fear management is another reason why really vivid fear campaigns can backfire

Perpetrator/Victim
It may not make sense to use blame to label our stigmatising individuals –
• they also suffer harm from the stereotype,
• temperament (emotional make-up) is probably inborn – they didn’t choose it;
• blame is a lousy educational premise.

Overcoming Stigma
• There are few research-validated programmatic solutions to stigma;
• Most evaluated projects have been short-term in nature and individually-focused;
• Australian campaigns have focused very heavily on ‘visibility’ campaigns;
• I’m interested in the learning process but my evidence in its support is anecdotal.

Dean’s Story
“As I looked over to the dancefloor, silhouetted against the laserlights were these amazing shoulders, this sexy vision, and I threw my arms around him and just draped myself over his shoulders. He thought it was his friend, and when he turned to look he went “who the fuck are you!?” If you’d said to me at the time ‘you are going to meet an HIV+ man who is 11 years your senior and fall in love with him’, I would have said, ‘you’re mad’.”
Staying Negative (2005)
VAC/GMHC

Elaboration
Pre-Encounter
Totally relies on stereotype for judgment
Encounter
Challenges stereotype and initial judgment
Engagement
Development of a rich and individualised understanding over time – complex judgments

Elaboration Likelihood Model
Petty & Cacioppo (1978)
• “Attitudes formed under high elaboration are stronger (more predictive of behavior and information processing, more stable over time, more resistant to persuasion) than those formed under low elaboration.”
• Factors promoting elaboration are motivation and ability to process

Educational Responses

Discrimination
Status Loss Separation
Stereotyping
Labelling
STIGMA
Campaigns“You can’t tell who’s +ve”“Use positive language”
Campaigns“Would you wear it?”“Think Again”“One Community +/-”
Campaigns“Are you positive about negatives?”
Campaigns“Sexual Racism Sux”
Campaigns“Sexual Racism Sux”
Campaigns

Campaigns
• Scenario – research indicates a slight majority of men (56%) may reject a known-positive partner, while men who express strongly negative opinions about PLWHA score lower on measures of confidence in condom use as protection against HIV/AIDS.
• Task – use the stigma model to identify opportunities and possible strategies for a campaign targeting men who reject PLWHA

Policy/Advocacy
• Scenario – recently the government of Viet Nam has pursued a “social evils” campaign to publicly identify HIV/AIDS as an epidemic prevalent among Gay Men, Injecting Drug Users and Sex Workers.
• Task – using the five-stage model, explain to the VN government why this approach may be counterproductive.

Policy/Advocacy
• Scenario – residents of an inner city suburb where street sex workers meet clients call a public meeting to demand police arrest sex workers on sight. They say street sex work is unnecessary when brothels/escort services are legal.
• Task – use the stigma model and psychology of discrimination material to plan a response at the meeting.

Case Work
Scenario – John is a 23yo HCV+ former injecting drug user from an outer western suburb who is currently on oral substitute therapy. He needs a safe home environment while he undergoes treatment for Hep C but his family has disowned him.
Task – using the stigma model, formulate a case management plan to help John re-engage and negotiate with his family.

Professional Education
Scenario – one of your members describes a terrible experience with a dentist who insists on double-gloving and disinfecting everything during appointments. You make contact and the dentist says “You just can’t be too safe with these people.”
Task – using the stigma model, plan an educational workshop & resource for clinical professionals including this dentist.

International Work
Scenario – you have been invited to work for a small NGO on a project to protect children from HIV/AIDS in Malaysia. Their children’s parents are injecting drug users, and the project coordinator is thinking of an after-school program for the kids.
Task – show how you might use the stigma model in your first task on the job, a needs analysis.

Policy/Advocacy
Scenario – prompted by a high-profile public prosecution of an HIV+ sex worker, the health department identifies onward transmission of HIV by sex workers in brothels/escort agencies as a priority issue and offers your organisation funding to conduct Condom Skills 101 workshops.
Task – use the stigma model to frame a response (that still results in funding).

Instructions
Suggestions
• Remember to consider
both perspectives
(stigmatised/stigmatising)
• Consider the different
levels (individual, social,
cultural);
• Don’t treat stigma as an
attribute of the person
who is stigmatised.
…Discrimination
…Status loss
…Separation
…Stereotyping
strategiesLabelling
THEN…FIRST

Reportback

References• Gorbach, Galea, Amani et al (2004) “Don’t ask, don’t tell: patterns of HIV disclosure among
positive men” Sex Transm Infect 80:512–517.
• Please see the Discussion Paper in your conference bags for other references.





























