Embed Size (px)
Citation preview


WHAT SAY NEW GUIDELINES ?
Many alternatives for treating angina : How to choose ?


A new name for the Guidelines that can be applied to a wider and more realistic range of patients
“Stable angina pectoris”
2006“Stable Coronary Artery Disease”
2013
This much broader term intended to include both symptomatic
and asymptomatic patients with a previous or present history of confirmed or suspected stable CAD.

(i) Those having stable angina pectoris or other symptoms felt to be related to CAD such as dyspnoea
(ii) Those previously symptomatic with known obstructive or non-obstructive CAD, who have become asymptomatic with treatment and need regular follow-up
(iii) Those who report symptoms for the first time and are judged to already be in a chronic stable condition (for instance because history-taking reveals that similar symptoms were already present for several months).
Stable coronary artery disease


Meets all three of the following characteristics:
• substernal chest discomfort of characteristicquality and duration;• provoked by exertion or emotional stress;• relieved by rest and/or nitrates within minutes.
Typical angina
Meets two of these characteristicsAtypical angina(probable)
Lacks or meets only one or none of thecharacteristics
Non-anginalchest pain
(Definite)
Traditional clinical classification of chest pain

Ordinary activity does not cause angina such as walking and climbing stairs. Angina with strenuous or rapid or prolonged exertion at work or recreation.
Class I
Slight limitation of ordinary activity. Angina on walking or climbing stairs rapidly, walking or stair climbing after meals, or in cold, wind or under emotional stress, or only during the first few hours after awakening. Walking more than two blocks on the level and climbing more than one flight of ordinary stairs at a normal pace and in normal conditions.
Class II
Marked limitation of ordinary physical activity. Angina on walking one to two blocks (~100–200 m)on the level or one flight of stairs in normal conditions and at a normal pace.
Class III
Inability to carry on any physical activity without discomfort' –angina syndrome may be present at rest'.
Class IV
Classification of angina severity according to the Canadian Cardiovascular Society

Antianginal Drug
Relief of symptoms Improving prognosis
(Prevent cardiovascular events)
Feel better Live longer

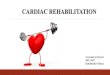
Medical management of SCAD patients
“We recommend the old drugs as first line treatment because they are cheap, effective and available everywhere.”
“We have roughly the same level of evidence for all of the second line drugs and we recommend that physicians also choose according to what is available in their country.”
Angina relief Event prevention
• β-blockers and/or CCB
Ivabradine Long-acting nitrates Nicorandil Ranolazine Trimetazidine
• Lifestyle management• Control of risk factors
• Aspirin (if intolerance, consider clopidogrel)
• Statins• Consider ACE inhibitors or ARBs
+ consider angio → PCI-stenting or CABG
Short-acting nitrates, plus
1st line
2nd line

Medical management of SCAD patients
Angina relief Event prevention
• β-blockers and/or CCB
IvabradineLong-acting nitratesNicorandilRanolazineTrimetazidine
• Lifestyle management• Control of risk factors
• Aspirin (if intolerance, consider clopidogrel)
• Statins• Consider ACE inhibitors or ARBs
+ consider angio → PCI-stenting or CABG
Short-acting nitrates, plus
1st line
2nd line
About revascularization, chairmen hopes that “guidelines will shift physicians’ practice so that they consider optimal medical treatment as their first course of action in stable CAD patients”.

Stable coronary artery disease
Old and New Anti-anginalDrugs

Old ( traditional ) anti-anginals
Drug class Vasodilation Heart rate Myocardial
contractility
Short acting
nitrate -
sublingual
Beta-blockers
Long-acting
nitrates
Calcium channel
blockers
DHP Amlodipine Non-DHP Diltiazem and Verapamil

NitratesCalcium channel blockers
Beta blockersCalcium channel blockers

New mechanistic approaches to myocardial ischemia
Metabolic modulation (trimetazidine)
Sinus node inhibition (ivabradine)
Late Na+ current inhibition (ranolazine)
Preconditioning (nicorandil)

Metabolic modulation (pFOX ) : trimetazidine
Trimetazidine : pFOX (partial fatty acid oxidation ) inhibitor


Ischemic Preconditioning
Myocardial Protection
There is general consensus that
Mito K+ATP channels
play a key role

Focus on ATP-sensitive K+ channels

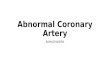
MYOCARDIAL ISCHAEMIC PRE-CONDITIONING
“Phenomenon by which a brief episode (s) of myocardial ischaemia increases the ability of the heart to tolerate a sbsequent prolonged period of ischaemia”

IPC concept
Murry CE. Circulation 1986;74:1124-36
infarct surface
ControlGroup
PreconditioningGroup
ischemia
brief ischemia
ischemia
reperfusioninduction
prolonged occlusion

Adenosine subtype 1 (A1) receptor
Ischemic stimulus
G protein and protein kinase C (PKC).
Opening of Mito K+ATP channel
Cardio-protective effect
IPC involves a complex cascade of intracellular events
amplified
effector
?

Cardioprotective effect
Opening Mitochondrial ATP-K+ channels:
Mimic the cardioprotective effect of IPC without inducing ischemia
Pharmacological preconditioning agents
Nicorandil mimics IPC

Preconditioning: Nicorandil
Nitrate-associated effects
• Vasodilation of coronary epicardial arteries
Activation of ATP-sensitive K+ channels
• Ischemic preconditioning
• Dilation of coronary resistance arterioles
N O
O NO2
HN

Nicorandil :dual effects
The ATP-sensitive K+ channels are composed of subunit proteins: *an inwardly rectifying K+ channel (KIR) *a sulphonylureareceptor (SUR)
Activation of ATP-sensitive K+ channels causes K+ efflux and hyperpolarisation of the smooth muscle cell membrane and closure of voltage-gated Ca2+ channels.Closure of Ca2+ channels reduces intracellular levels of Ca2+, resulting in relaxation of vascular smooth muscle and dilation of systemic and coronary arterioles
The nitrate moiety produces relaxation of vascular smooth muscle with dilation of systemic venous circulation and epicardial coronary arteries.

EFFECT OF MEDICATION
Preconditioning Preconditioning
KATP channel blockersKATP channel openers
Sulfonylurea drugs:
Glibenclamide , gliclazide , glimepiride
NICORANDIL

Cardioprotective effects of nicorandil


Adverse effects
Blood pressure and heart rate
Comorbidities & Contraindications
Drug costs & Drug-drug interactions
The ESC common strategy might be adjusted according to:-

Anti-anginal drugs.

Anti-anginal drugs.

Short-Acting NitratesSL Nitroglycerin & SL Isosorbide dinitrate
• Relief of pain, hemodynamic effect (10 mm Hg drop, ↑HR)
• Onset: 1-3 min, duration:10-30 min
• Prevention of attack: To be taken 5-10 min before the exertion that possibly precipitate angina(activity after a meal, emotional stress, sexual activity and in colder weather)
• Instructions to Patient:
o Sit immediately, place NTG/ISDN tablet under tongue
(standing promotes syncope, lying down enhances venous return and heart work)
o Max three tablets over 15 min
o If pain persists >30 min →suspected ACS

Nitrate Tolerance Minimization
• Nitrate-free interval of 10-12 hours minimize tolerance to therapeutic activity
• Lowest effective nitrate dose lower tolerance
• ß-blocker or CCB is given to provide anginalprotection during nitrate-free period
• Long-acting nitrates have no evidence of causing tolerance to SL nitrates’ use

ISOSORBIDE DINITRATE & MONONITRATE (ISDN & ISMN)
• ISDN oral formulation is used usually three times a day especially in severe angina
Usually ISDN is taken at 7 AM, Noon & 5 PM to allow 12 hr nitrate-free period
ISDN can be given twice/day in moderate severity angina
• ISMN can be given once or twice/day
(early morning & 7 hrs later)
ISMN has better patient compliance

Sexual activity may trigger ischaemia, and nitroglycerin prior to sexual intercourse may be helpful as in other physical activity.
Sexual activity
Erectile dysfunction (ED)
Pharmacological therapy with PDE5 inhibitors (sildenafil, tadalafil and vardenafil) are effective,safe and well tolerated in men with stable CAD

All of the preparations of nitroglycerin as well as isosorbide mononitrate and isosorbide dinitrate, are absolute contra-indications to the use of PDE5 inhibitors because of the risk of synergistic effects on vasodilation, causing hypotension and haemodynamic collapse.
If a patient on a PDE5 inhibitor develops chest pain, nitrates should not be administered in the first 24 hours (sildenafil “viagra”, vardenafil “levitra”) to 48 hours (tadalafil “cialis”).

Prostatic problems
Erectile dysfunction
Angina
α-adrenergic blockers
PDE5 inhibitorsNitrates

β-Adrenergic Blockers
ß-blockers abrupt withdrawal can be serious in severe CAD → ACS
*β - Blockers can be combined with CCBs ( DHPs:amlodipine ) to control angina.*Combination therapy of β -blockers with verapamil and diltiazem(non-DHPs) should be avoided because of the risk of bradycardia or AV block
Nevibolol and bisoprolol are partly secreted by the kidney, whereas carvedilol and metoprolol are
metabolized by the liver, hence being safer in patients with renal compromise.

Anti-anginal drugs should be started at very low doses, with preferential use of drugs with
no- or limited impact on BP, such as ivabradine (in patients with sinus rhythm),
ranolazine or trimetazidine.

Although lowering the heart rate ,60 b.p.m. is an important goal in the treatment of SCAD, patients presenting with low heart rate should be treated differently.
Heart rate lowering drugs (β-blockers, ivabradine,heartrate lowering CCBs) should be avoided or used with caution and, if needed, started at very low doses.
Anti-anginal drugs without heart lowering effects should preferably be given.

Non-steroidal anti-inflammatory drugs (NSAIDs) has been associated with an increased risk for CV events
In patients at increased CV risk in need of pain relief, it is therefore recommended to commence with acetaminophen or aspirin at the lowest efficacious dose, especially for short-term needs.
If adequate pain relief requires the use of NSAIDs, these agentsshould be used in the lowest effective doses and for the shortest possible duration.


BIShort-acting nitrates are recommended
AIFirst-line treatment is indicated with ß-blockers and/or calcium channel blockers to control heart rate and symptoms.
BIIaFor second-line treatment it is recommended to add long-acting nitrates or ivabradine or nicorandil or ranolazine,according to heart rate, blood pressure and tolerance.
BIIbFor second-line treatment, trimetazidine may be considered
CIAccording to comorbidities/tolerance it is indicated to use second-line therapies as first-line treatment in selected patients
Angina/ischaemia relief Class Level
2013 ESC guidelines on the management of SCAD

AILow-dose aspirin daily is recommended in all SCAD patients.
BIClopidogrel is indicated as an alternative in case of aspirin intolerance.
AIStatins are recommended in all SCAD patients.
AIIt is recommended to use ACE inhibitors (or ARBs) if presence of other conditions (e.g. heart failure, hypertension or diabetes).
Event prevention Class Level
2013 ESC guidelines on the management of SCAD