Embed Size (px)
Citation preview

Sandro Esteves, MD, PhDSandro Esteves, MD, PhD
Director, ANDROFERTDirector, ANDROFERT
Center for Male Reproduction and InfertilityCenter for Male Reproduction and Infertility
Campinas, BRAZILCampinas, BRAZIL
Training Program in Assisted Reproductive Technology 2011 Training Program in Assisted Reproductive Technology 2011 Cleveland Clinic Reproductive Research CenterCleveland Clinic Reproductive Research Center

Esteves, 2
Learning ObjectivesLearning Objectives

AzoospermiaAzoospermia
• It is not a synonymous of sterility It is not a synonymous of sterility

Technique Acronym IndicationsPercutaneous epididymal sperm aspiration
PESA OA cases only
Microsurgical epididymal sperm aspiration
MESA OA cases only
Testicular sperm aspiration TESA; TEFNA1 Failed PESA in OAEpididymal agenesis in CAVD casesFavorable testicular histopathology2 in NOA Previous successful TESA attempt in NOA
Testicular sperm extraction (single or multiple biopsies)
TESE Failed PESA or TESA in OANOA cases
Microsurgical testicular sperm extraction
Micro-TESE NOA cases only
Sperm Retrieval TechniquesSperm Retrieval Techniques
Esteves SC et al. Sperm Retrieval Techniques for Assisted Reproduction.Esteves SC et al. Sperm Retrieval Techniques for Assisted Reproduction. Int Braz J Urol 2011, Int Braz J Urol 2011, in press. in press.
Esteves, 4

Obstructive AzoospermiaObstructive Azoospermia
• Epididymis• Testicle• Simple and
effective
Sperm Retrieval for
ART
Esteves SC & Agarwal A. Sperm Retrieval Techniques; In: Gardner D et al (Eds.), Esteves SC & Agarwal A. Sperm Retrieval Techniques; In: Gardner D et al (Eds.), Human Assisted Reproductive Technology. Cambridge University Press, pp. 41-53, Human Assisted Reproductive Technology. Cambridge University Press, pp. 41-53,
2011.2011.Esteves, 5

Please visit Please visit http://androfert.com.br/videos http://androfert.com.br/videos to see the videoto see the video

Laboratory Sperm Processing Laboratory Sperm Processing
Verza Jr & Esteves, Atlas of Human Reproduction, Verza Jr & Esteves, Atlas of Human Reproduction, in pressin press

PERCUTANEOUS RETRIEVAL PERCUTANEOUS RETRIEVAL
Esteves SC, Verza S, Prudencio C, Seol B. Success of percutaneous sperm Esteves SC, Verza S, Prudencio C, Seol B. Success of percutaneous sperm retrieval and intracytoplasmic sperm injection (ICSI) in obstructive azoospermic (OA) retrieval and intracytoplasmic sperm injection (ICSI) in obstructive azoospermic (OA) men according to the cause of obstruction. Fertil Steril. 2010;94 (Suppl):S233.men according to the cause of obstruction. Fertil Steril. 2010;94 (Suppl):S233.

Non-obstructive AzoospermiaNon-obstructive Azoospermia
10-20% of infertile men attending ART Clinics10-20% of infertile men attending ART Clinics
60-70% of azoospermic men60-70% of azoospermic men
Causes are: Causes are: • Pre-testicular: HH Pre-testicular: HH • Testicular causesTesticular causes
• GeneticGenetic
Y chromosome microdeletion Y chromosome microdeletion Klinefelter syndrome Klinefelter syndrome
VaricoceleVaricocele Cryptorchidism Cryptorchidism Chemotherapy/RadiationChemotherapy/Radiation Infection Infection Idiopathic Idiopathic
Source: ANDROFERT, BrazilSource: ANDROFERT, Brazil

Non-obstructive AzoospermiaNon-obstructive Azoospermia
• Sperm production reduced or absent
• Geographic location unpredictable
Sperm Retrieval for ART
Untreatable condition
TESATESA
TESETESE

Controlled studies for NOA men
Needle Aspiration
Open Biopsy
Friedler et al., Human Reprod 12:1488, 1997
4/37 (11%) 16/37 (43%)
Ezeh et al. Human Reprod 13:3075, 1998
5/35 (14%) 22/35 (63%)
Non-obstructive AzoospermiaNon-obstructive Azoospermia
TESA vs. TESETESA vs. TESE

Conventional TESE (open biopsy) in NOAConventional TESE (open biopsy) in NOA
Ostad et al., Urology 52:692, 1998.Ostad et al., Urology 52:692, 1998.
Esteves, 12

Non-obstructive AzoospermiaNon-obstructive AzoospermiaTesticular microdissection - micro-TESETesticular microdissection - micro-TESE
• Method to identify site(s) of Method to identify site(s) of productionproduction– Based on the diameter of Based on the diameter of
seminiferous tubulesseminiferous tubules
• Microsurgical approachMicrosurgical approach– Identify site of productionIdentify site of production– Preserve vasculature of testisPreserve vasculature of testis– Small quantity of tissue excisedSmall quantity of tissue excised
Schlegel PN. Testicular sperm extraction: microdissection improves sperm yield with Schlegel PN. Testicular sperm extraction: microdissection improves sperm yield with minimal tissue excision. Hum Reprod. 1999;14:131-135.minimal tissue excision. Hum Reprod. 1999;14:131-135.

Please visit Please visit http://androfert.com.br/videos http://androfert.com.br/videos to see the videoto see the video

TESE/TESA Sperm Processing TESE/TESA Sperm Processing
Verza Jr & Esteves, Atlas of Human Reproduction, Verza Jr & Esteves, Atlas of Human Reproduction, in pressin press
Esteves, 15

Micro-TESEMicro-TESE
RESULTSRESULTS

Micro-TESE vs TESEMicro-TESE vs TESESuccess Rates in Controlled SeriesSuccess Rates in Controlled Series

Can We Predict Sperm Retrieval Can We Predict Sperm Retrieval Success in NOA?Success in NOA?
Important because:Important because:
2.2.Can minimize emotional and financial cost of IVF Can minimize emotional and financial cost of IVF cycles.cycles.
3.3.Can minimize trauma/ damage to testis during sperm Can minimize trauma/ damage to testis during sperm harvesting.harvesting.
Esteves, 18

Predictive Values of Noninvasive Tests for Predictive Values of Noninvasive Tests for Sperm Retrieval in NOASperm Retrieval in NOA
Carpi. Controversies in nonobstructive azoospermia. Fertil Steril 2009.
Marker Sensitivity % Specificity % Overall Predictive Value %
Testicular Volume 7.6-50 6.7-71
FSH 9-71 40-90
Inhibin B 44.6 63.4
FSH, Testosterone, Inhibin B
71 71.4
Testicular Volume + Hormones
80.8
Doppler US 47.3 89

Predictive Values of Noninvasive Tests for Predictive Values of Noninvasive Tests for Sperm Retrieval in NOASperm Retrieval in NOA
Esteves, Miyaoka & Agarwal: An update on the initial assessment of the infertile male. Esteves, Miyaoka & Agarwal: An update on the initial assessment of the infertile male. CLINICS 2011; 66:1-10. CLINICS 2011; 66:1-10.

Chance of Sperm Retrieval by NOA Chance of Sperm Retrieval by NOA DiagnosisDiagnosis
CryptorchidismCryptorchidism 52-74%52-74%
VaricoceleVaricocele 63-68%63-68%
Post-infection (mumps, etc.)Post-infection (mumps, etc.) 67%67%
TorsionTorsion >50%>50%
Post-radiation/chemotherapyPost-radiation/chemotherapy 55-75%55-75%
Genetic (Klinefelter, Y microdeletion)Genetic (Klinefelter, Y microdeletion) 0-75%0-75%
IdiopathicIdiopathic 50-60%50-60%
Esteves et al., Fertil Steril 94; 2010; Raman and Schlegel. J Urol.170; 2003; Esteves et al., Fertil Steril 94; 2010; Raman and Schlegel. J Urol.170; 2003; Hopps et al. Hum Reprod. 180, 2003; Damani et al. JCO. 15; 2002 Hopps et al. Hum Reprod. 180, 2003; Damani et al. JCO. 15; 2002

Esteves SC & Agarwal A. Novel concepts in male infertility. Esteves SC & Agarwal A. Novel concepts in male infertility. Int Braz J Urol 2011; 37:5-15. Int Braz J Urol 2011; 37:5-15.
Predictive Values of Noninvasive Tests for Predictive Values of Noninvasive Tests for Sperm Retrieval in NOASperm Retrieval in NOA
Y Chromosome MicrodeletionY Chromosome Microdeletion
Esteves, 22

Testicular HistopathologyTesticular Histopathology
Predictive Values of Invasive Tests for Predictive Values of Invasive Tests for Sperm Retrieval in NOASperm Retrieval in NOA
Esteves, Miyaoka & Agarwal. Surgical Treatment of Male Infertility in the ICSI Era. Esteves, Miyaoka & Agarwal. Surgical Treatment of Male Infertility in the ICSI Era. CLINICS 2011; 66:1463-77. CLINICS 2011; 66:1463-77.
Esteves, 23

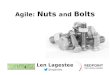
Microsurgical vs Single-Biopsy TESE in NOA: a Microsurgical vs Single-Biopsy TESE in NOA: a prospective controlled studyprospective controlled study
Verza Jr S & Esteves SC; ASRM 2011 (O-178)Verza Jr S & Esteves SC; ASRM 2011 (O-178)
Esteves, 24

Microsurgical vs Single-Biopsy TESE in Microsurgical vs Single-Biopsy TESE in Non-obstructive AzoospermiaNon-obstructive Azoospermia
Verza Jr & Esteves, O-178, ASRM 2011Verza Jr & Esteves, O-178, ASRM 2011
P=0.02
• Controlled series of 60 patients

Sperm Retrieval TechniquesSperm Retrieval Techniques Advantages DisadvantagesPESA Fast and low cost; No surgery
Minimal morbidity, repeatableFew sperm retrieved; Cryopreservation limitedFibrosis and obstruction at aspiration siteRisk of hematoma/spermatocele
MESA Large number of sperm retrievedSperm cryopreservationReduced risk of hematoma
Increased cost and time-demandingMicrosurgical instruments and expertise Postoperative discomfort
TESA Fast and low cost; No surgeryRepeatable Minimal/mild postop discomfort
Low success rate/few sperm retrieved in NOACryopreservation limitedRisk of hematoma/testicular atrophy
TESE No microsurgical expertise Fast and repeatable
Low success rate/few sperm retrieved in NOARisk of testicular atrophy (multiple biopsies)Postoperative discomfort
Micro-TESE Higher success rates in NOALarger number of sperm retrieved
Increased cost and time-demandingMicrosurgical instruments and expertise Postoperative discomfort
Esteves, Miyaoka & Agarwal. Sperm Retrieval Techniques for Assisted Conception. Esteves, Miyaoka & Agarwal. Sperm Retrieval Techniques for Assisted Conception. Int Braz J Urol Int Braz J Urol in pressin press

Reproductive Reproductive Potential of Potential of
Azoospermic Men Azoospermic Men undergoing ARTundergoing ART
Esteves, 27

Epididymis Testicle p
Female Age (years)Female Age (years) 31.5 ± 7.7 36.3 ± 5.1
Mature Oocytes Injected (n)Mature Oocytes Injected (n) 9.4 ± 5.8 9.4 ± 4.9
NS
Embryo Transfer (n)Embryo Transfer (n) 3.3 ± 1.3 3.7 ± 1.5
2PN Fertilization (%)2PN Fertilization (%) 74.7% ± 21.2% 69.1% ± 19.6%
TQE day 3 (%) TQE day 3 (%) 44.6% ± 30.5% 52.7% ± 29.6%
Clinical Pregnancy (%) Clinical Pregnancy (%) 51.6% 50.0%
Miscarriage (%)Miscarriage (%) 18.8% 25.0%
Verza Jr S & Esteves SC. Sperm defect severity rather than sperm source is associated with lower fertilization rates after intracytoplasmic sperm injection.
Int Braz J Urol 2008;34:49-56. Esteves, 28
Intracytoplasmic Sperm Injection Outcomes Using Intracytoplasmic Sperm Injection Outcomes Using Surgically-retrieved Sperm from Obstructive Surgically-retrieved Sperm from Obstructive
Azoospermic MenAzoospermic Men

Verza Jr S & Esteves SC. Sperm defect severity rather than sperm source is associated with lower fertilization rates after intracytoplasmic sperm injection.
Int Braz J Urol 2008; 34:49-56.
NS
Intracytoplasmic Sperm Injection Outcomes Using Intracytoplasmic Sperm Injection Outcomes Using Ejaculates vs. Surgically-retrieved Sperm from Ejaculates vs. Surgically-retrieved Sperm from
Obstructive Azoospermic MenObstructive Azoospermic Men

Obstructive Azoospermia
Non-obstructiveAzoospermia
2PN Fertilization Rate2PN Fertilization Rate 73.6% 52.2%*
TQE transfer dayTQE transfer day 46.3% 35.7%*
Clinical Pregnancy RateClinical Pregnancy Rate 51.3% 25.9%*
Miscarriage RateMiscarriage Rate 20.0% 14.3%
Verza Jr S & Esteves SC. Sperm defect severity rather than sperm source is associated with lower fertilization rates after intracytoplasmic sperm injection.
Int Braz J Urol 2008; 34:49-56.
Intracytoplasmic Sperm Injection Outcomes Using Intracytoplasmic Sperm Injection Outcomes Using Surgically-retrieved SpermSurgically-retrieved Sperm
Esteves, 30

ICSI Ejaculated Sperm (n=220)
Sperm Defect
Testicular/Epididymal Sperm
(n=93)
Normal Single Double Triple OA NOA
2PN Fertilization (%) 71.3 73.2 72.1 63.4* 73.6 52.2*
TQE on Day 3 (%) 48.4 50.5 46.9 48.3 46.3 35.7*
Clinical Pregnancy (%) 40.9 36.6 44.4 51.0 51.3 25.9*
Miscarriage (%) 14.9 9.1 12.5 12.0 20.0 14.3
* P<0.05
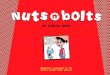
Sperm Defect Severity Rather Than Sperm Source Is Sperm Defect Severity Rather Than Sperm Source Is Associated With Lower Fertilization Rates After Associated With Lower Fertilization Rates After
Intracytoplasmic Sperm InjectionIntracytoplasmic Sperm InjectionVerza Jr S & Esteves SC; Int Braz J Urol 2008; 34
Esteves, Androfert

Odds-ratio 43.0 1.86
95% CI 10.3 – 179.5 1.03 – 2.89
p <0.01 0.03
Prudencio C, Seoul B, Esteves SC. Reproductive potential of azoospermic men Prudencio C, Seoul B, Esteves SC. Reproductive potential of azoospermic men undergoing intracytoplasmic sperm injection is dependent on the type of azoospermia.undergoing intracytoplasmic sperm injection is dependent on the type of azoospermia.
Fertil Steril 2010; 94(4):S232-3.Fertil Steril 2010; 94(4):S232-3.
Sperm Retrieval Rates and Reproductive Sperm Retrieval Rates and Reproductive Potential of Azoospermic Men undergoing Potential of Azoospermic Men undergoing
ICSIICSI

• Sperm retrieval and lab processing simple
• Sperm obtained in virtually all cases
• Chance of Retrieval and ICSI Outcomes: • Independent on obstruction etiology• Independent on retrieval technique• Independent on sperm source• Results similar or better than ejaculated sperm
Obstructive Azoospermia

•Sperm production deficient or absent
•Overall, retrieval rates ~50%
•Labor-intensive lab sperm processing•Retrieval rates dependent on technique
• Micro-TESE yields better SRR • Predictive factors: testis histology & Y-chromosome
•Reproductive potential by ICSI lower than OA and non-azoospermic men
Non-obstructive Azoospermia

MCQ 1
Azoospermic males presenting with:
a) obstructive azoospermia (OA) have normal spermatogenesis and a mechanical block somewhere between the epididymis and the ejaculatory duct. Common causes of OA include vasectomy, post-infectious diseases and congenital conditions.
b) nonobstructive azoospermia (NOA) have extremely deficient or absent sperm production within the testicles. Common causes of NOA include cryptorchidism, orquitis, radio/chemotherapy, use of gonadotoxic medication and steroids, and genetic origin.
c) nonobstructive azoospermia have retrieval rates dependent on the method of collection. Testicular histopathology results and Y-chromosome microdeletion testing are useful tools to predict the likelihood of sperm retrieval.
d) obstructive azoospermia have virtually 100% successful retrievals. Retrieval rates and ICSI outcomes are neither dependent on the method of collection nor on the origin of sperm for ICSI (epididymal or testicular).

MCQ 2
The following techniques can be used to retrieve sperm in men with nonobstructive azoospermia:
a) PESA (percutaneous epididymal sperm aspiration).
b) Micro-TESE (microdissection testicular sperm extraction).
c) TESA (testicular sperm aspiration).
d) Conventional TESE (testicular sperm extraction) using single or multiple biopsies.

MCQ 3
The following statements apply to sperm retrieval techniques:
a) Micro-TESE yields higher sperm retrieval success rates than conventional TESE or TESA.
b) PESA is a fast, effective and safe method to retrieve sperm in obstructive azoospermia. Expertise in microsurgery is required for PESA.
c) TESA is safe and effective in cases of failed PESA. No expertise in microsurgery is required for TESA.
d) MESA is indicated in obstructive azoospermia. Sperm retrieval rates are comparable to PESA although higher sperm number is obtained.

MCQ 4
Overall, sperm retrieval success and pregnancy rates by ICSI (using retrieved sperm) in men with obstructive (OA) and nonobstructive (NOA) azoospermia are:
a) 50% and 30%, 70% and 25%, respectively.
b) >90% and 50%, 40% and 25%, respectively.
c) 50% and 30%, respectively, and rates are not dependent on the type of azoospermia being obstructive or nonobstructive.
d) 100% and 50% in OA men with vasectomy, and 0% in NOA men with testicular histology showing germ cell aplasia (Sertoli cell-only).