Embed Size (px)
Citation preview

PBL 3 – hd - Severe combined immunodeficiencySCIDAsem shadid

• How your family history is used• By tracking the health of your blood relatives,
specialists may be able to identify some risk factors that could affect your current or future health. Risk factors raise your chances of developing certain conditions.
• The importance of knowing your family history• Knowing your potential risks of ill health can help
you to make better decisions about prevention and screening. It can encourage your family to live healthier lives too. And in some cases, it can also allow you to get involved in research aimed at understanding, preventing and curing the particular condition.
Severe combined immunodeficiencySCID• a genetic disorder characterized by the disturbed development
of functional T cells and B cells caused by numerous genetic mutations .
• SCID involves defective antibody response due to either direct involvement with B lymphocytes or through improper B lymphocyte activation due to non-functional T-helper cells.
• It is also known as the bubble baby disease and bubble boy disease .
• SCID patients are usually affected by severe bacterial, viral, or fungal infections early in life and often present with interstitial lung disease, chronic diarrhea, and failure to thrive.
• These babies, if untreated, usually die within 1 year due to severe, recurrent infections unless they have undergone successful hematopoietic stem cell transplantation.

Classification• X-linked - Most cases of SCID are due to mutations in the
gene encoding the common gamma chain (γc), a protein that is shared by the receptors for interleukins IL-2, IL-4, IL-7, IL-9, IL-15 and IL-21.
• These interleukins and their receptors are involved in the development and differentiation of T and B cells.
• The result is a near complete failure of the immune system to develop and function, with low or absent T cells and NK cells and non-functional B cells.
• The condition is inherited in an X-linked recessive pattern.

Classification
• Adenosine deaminase deficiency - caused by a defective enzyme, adenosine deaminase (ADA), necessary for the breakdown of purines.
• Lack of ADA causes accumulation of dATP. This metabolite will inhibit the activity of ribonucleotide reductase .
• Without functional ribonucleotide reductase, lymphocyte proliferation is inhibited and the immune system is compromised.

Classification• Purine nucleoside phosphorylase deficiency - An
autosomal recessive disorder involving mutations of the purine nucleoside phosphorylase (PNP) gene.
• Impairment of this enzyme causes elevated dGTP levels resulting in T-cell toxicity and deficiency.
• Omenn syndrome - mutations of the RAG-1 or RAG-2 genes prevent V(D)J recombination, causing SCID.
• V(D)J recombination, less commonly known as somatic recombination, is the unique mechanism of genetic recombination that occurs only in developing lymphocytes during the early stages of T and B cell maturation.
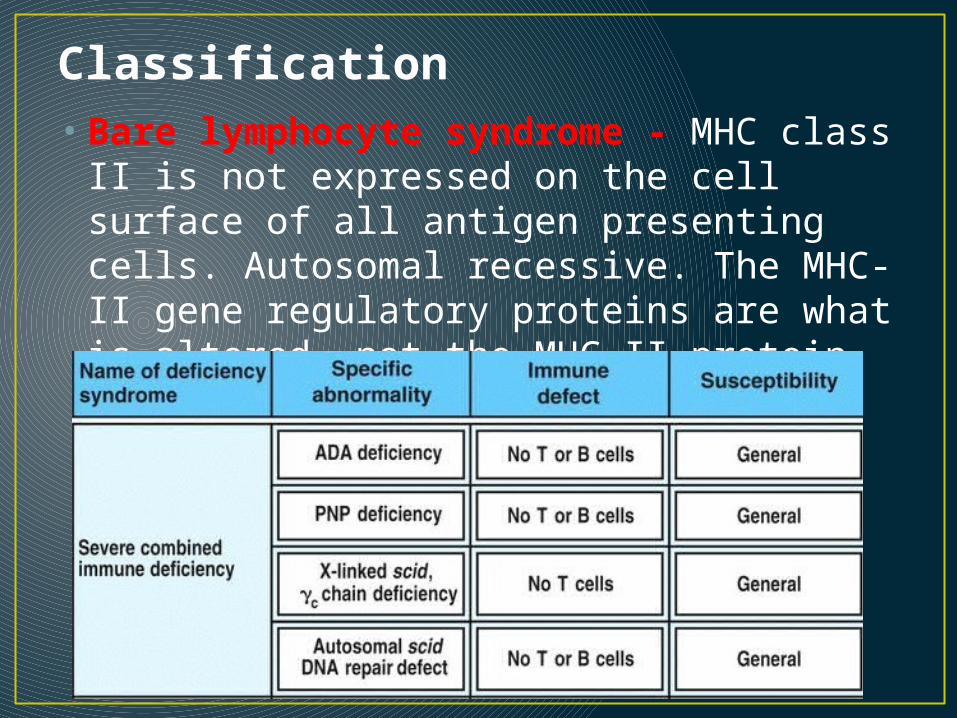
Classification• Bare lymphocyte syndrome - MHC class
II is not expressed on the cell surface of all antigen presenting cells. Autosomal recessive. The MHC-II gene regulatory proteins are what is altered, not the MHC-II protein itself.
LABORATORY ABNORMALITIES• The typical laboratory abnormalities
observed in SCID include low to absent T cell numbers and function, as measured by T cell enumeration by flow cytometry and T cell proliferation to mitogens such as phytohemagglutinin (PHA) and concanavalin A (ConA).
• Other immunologic abnormalities are seen, but are not critical to the initial evaluation.

Laboratory studies necessary to confirm the diagnosis are reviewed below. • There is usually a low absolute lymphocyte count (<2500
cells/microL). The thymus is generally small and devoid of lymphocytes. Occasionally, the absolute lymphocyte count is normal. This can be due to a high number of B cells or to engraftment of transplacentally transferred maternal T cells.
• ●Abnormalities of lymphocyte subpopulations as determined by flow cytometry may vary depending upon the specific molecular defect (table 1). Autologous T cells are <300 cells/microL. However, the autologous T cell count may be normal or high in some cases due to the presence of maternal T cells in the peripheral circulation or abnormal expansion of a few clones (eg, Omenn syndrome). (See 'Diagnosis' below.)
Laboratory studies necessary to confirm the diagnosis are reviewed below.
• ●T cell mitogen responses are absent or extremely low, and this is one of the most important tests to perform early. Absence of T cell mitogen response is a crucial element in the diagnosis of SCID. (See 'Diagnosis' below.)
• ●Cutaneous anergy to recall antigens is universal, but this test is not reliable under one year of age. In vitro tests of T cell antigen response may be used after the infant has been immunized, but the diagnosis of SCID rests largely upon the absence of T cell mitogen response. Thus, testing for antigen response is not usually required in the context of evaluation for SCID.
• ●Hypogammaglobulinemia is often found, but may be obscured due to the presence of maternal immunoglobulin G (IgG) in the blood in early infancy. Serum levels of immunoglobulin M (IgM), immunoglobulin A (IgA), and immunoglobulin E (IgE) are usually very low.

DIAGNOSIS — The diagnosis of SCID should be suspected in children with any of the following
• Unexplained lymphopenia
• ●Recurrent fevers
• ●Failure to thrive (FTT)
• ●Chronic diarrhea
• ●Recurrence of severe episodes of thrush, mouth ulcers, respiratory syncytial virus (RSV), herpes simplex virus (HSV), varicella zoster virus (VZV), measles, influenza, or parainfluenza 3
• ●Adverse reactions (infections) caused by live vaccines, such as Bacillus Calmette-Guerin (BCG), rotavirus vaccine, or varicella vaccine

An infant has a diagnosis of SCID if• The absolute autologous T cell count is
<300 cells/microL and the proliferative response to mitogens such as phytohemagglutinin (PHA) is less than 10 percent of the normal control.
• OR• ●There are maternal T cells in the
circulation.

B and T cell screen• A B and T cell screen is a laboratory test to determine
the amount of T and B cells (lymphocytes) in the blood.• After the blood is drawn it goes through a two-step
process.
• First, the lymphocytes are separated from other blood parts. Once the cells are separated, identifiers are added to distinguish between T and B cells.
• The E-rosetting test identifies T cells and direct immunofluorescence is used to identify B cells.
• Alternative Names• Direct immunofluorescence; E-rosetting; T and B
lymphocyte assays; B and T lymphocyte assays

Treatment
• ●The most common, widely available curative therapy for most forms of SCID is hematopoietic cell transplantation (HCT).
• An exception is adenosine deaminase (ADA) deficiency, which may be treated with enzyme replacement therapy (eg, polyethylene glycol-adenosine deaminase [PEG-ADA]).
• Gene therapy is another possible alternative in some forms of SCID.

How Vaccines Work • Vaccines help develop immunity by imitating an infection.
This type of infection, however, does not cause illness, but it does cause the immune system to produce T-lymphocytes and antibodies. Sometimes, after getting a vaccine, the imitation infection can cause minor symptoms, such as fever. Such minor symptoms are normal and should be expected as the body builds immunity.
• Once the imitation infection goes away, the body is left with a supply of “memory” T-lymphocytes, as well as B-lymphocytes that will remember how to fight that disease in the future. However, it typically takes a few weeks for the body to produce T-lymphocytes and B-lymphocytes after vaccination. Therefore, it is possible that a person who was infected with a disease just before or just after vaccination could develop symptoms and get a disease, because the vaccine has not had enough time to provide protection.

• Thank you





























