Embed Size (px)
Citation preview

Current Concepts ReviewAdvances in 3D-Printed Pediatric
Prosthesesfor Upper Extremity Differences
Kara S. Tanaka, MFA, and Nina Lightdale-Miric, MDInvestigation performed at Children’s Hospital Los Angeles, Los Angeles, California
A Journal Club presentation by
Dr. Libin Thomas Manathara

Introduction
• Advances in 3-dimensional (3D) printing are transforming the accessibility,customization, and distribution of upper extremity prostheses
• It is estimated that by 2050 “the prevalence of limb loss [in the United Statesalone] will more than double from 1.6 to 3.6million people”
• The steep cost of functional prostheses, limited access to skilled prosthetists, andthe time needed to create and learn how to use a new device often precludeindividuals with a limb difference from obtaining them

Introduction
• Recent advances in the fields of robotic, myoelectric, bionic, and neuromotor
prosthetic technology have had limited distribution and have focused primarily on
adult patients
• Children, most notably, may benefit from new cost-effective, lightweight
alternatives to traditional, professionally produced prostheses
• Developments in 3D printing technology are quickly moving access to the
consumer and prosumer (production by consumer) levels, and a strong network of
volunteers is currently soliciting orders, printing, and dispensing hand and arm
assistive devices around the world

Introduction
• There are notable benefits to 3D-printed prostheses
• First, open-source files for the designs are easy to download and include a wide
variety of designs that are increasing daily
• Second, the components necessary to create a “helper hand” are available at a
fraction of the cost and weight of those used in even the most basic traditional
prosthesis
• As children grow and develop interests in instruments and sports, 3D printing can
meet the challenge to create affordable, customized, easily repaired, well-fitting
devices specific for each activity, interest, and size

Background
• The additive manufacturing technology of 3D printing is in its fourth decade; 3D
printers, however, just recently became available for home-use consumers
• Common uses of 3D printers are rapid prototyping and direct digital
manufacturing
• The recent influx of 3D printers into the household, and subsequent abundance of
“makers”—prosumers and do-it yourself hobbyists—has led to the creation of
online communities where people desiring 3D-printed objects, including
prostheses, can find someone with a printer who is willing to print one for them

Background
• Current desktop 3D printer models are best suited, in terms of print time and scale,
for child-sized prostheses
• Print-on-demand technology benefits prosthetic devices by making them
customizable, affordable, and lightweight
• This combination of qualities is sparking a resurgence of interest in children’s
prostheses and orthoses


Background
• Robohand (robohand.net), the first open-source 3D printed hand device, was
developed in 2012 via the online collaboration of puppet-maker Ivan Owen in the
U.S. and carpenter Richard van As in South Africa
• The simple body powered device operates using reverse tenodesis—the
mechanical fingers close with flexion of the wrist axis and open with extension
• All 5 fingers are connected to the wrist piece through a tensioning system and
move in unison


Background
• The group currently sells do-it-yourself kits ranging from $54 to $500 and fully
customized Robohands and Roboarms from $2,000 to $3,500
• Magic Arms (magicarms.org), created in 2012, uses 3D printing to address
neuromuscular weakness in children with diseases such as arthrogryposis
• Three-dimensional-printed plastics are lightweight, and by replacing traditionally
weighty metal components of a body-powered Wilmington Robotic EXoskeleton
(WREX) orthosis (JAECO Orthopedic), the device is now functional for very
young children and allows freedom of movement in all directions
Background
• A primary focus for companies and individuals who are making 3D-printed
assistive devices is expanding accessibility to children around the world by
creating ways of remote measuring and fitting
• Magic Arms is developing a “fit kit” that can be sent directly to the family for
customization of the upper extremity orthosis

Background
• In 2013, Jon Schull, a research scientist from the Rochester Institute of
Technology, founded e-NABLE (enablingthefuture.org), now the nonprofit Enable
Community Foundation, to connect a global network of volunteers and recipients,
forming what is one of the most widely known organizations associated with
experimental open-source 3D-printed hand devices
• The Johns Hopkins Hospital presented the first e-NABLE conference in 2014,
sparking interest and support from around the globe
• With the advent of plug-and-play desktop 3D printers, available at consumer price
points, anyone with access to the Internet can download the open-source design
files and begin printing these hand devices

Background
• The material cost of a printed and assembled hand is between $25 and $50
• This affordability in prosthetic development is broadening access to prostheses
around the world
• Myoelectric devices have always been considered too expensive and heavy to
benefit a growing child, and the option for early introduction of myoelectric
device use has not gained popularity
• The nonprofit group Limbitless Solutions (limbitlesssolutions.org) has created
3D-printed myoelectric robotic arms since 2014

Background
• A team of engineering students at the University of Central Florida developed an arm
prosthesis with fingers that contract and release using muscular stimulation from the
upper extremity
• The Limbitless Arm is a modification of the Flexy Hand, and the material cost of the
myoelectric prosthesis is $350
• Open-source robotic and myoelectric technology for hand and arm prostheses is also
being developed by Open Bionics (openbionics.org) in the United Kingdom

Background• The child sized device was released in October 2015 and features customfit
attachment sockets, created by 3D scanning of the recipient’s arm, and tiny
lightweight electronics in the palm
• Two channels of electromyographic (EMG) data, placed on the flexor and
extensor muscle groups, create a simple open-and-close input that allows a child to
flex and extend the wrist or flex and extend the fingers
• Patients can also hold open a signal for a prolonged period of time to perform a
grip-change

Background
• The system is currently idealized for mid-forearm transverse deficiencies in an 8
to 10-year-old child
• For more distal prostheses, development of smaller component technology and
precision models with individual finger movement are being developed

Prosthetic Design and Production
Downloading, Sizing, and Customizing
• Printing a prosthesis starts by downloading an open-source design file from the
Internet and scaling the model to fit the recipient
• Many prosthetic models require measurements from the unaffected hand and arm,
such as the width across the palm or the circumference of the forearm, to approximate
the best fit
• For a patient with bilateral upper extremity amputations, the maker may choose to
scale the forearm portion—often called the gauntlet—to fit the existing arm, and then
scale the remaining components to the same size

Downloading, Sizing, and Customizing
• This may require printing several test components to find the correct fit for arecipient
• Customization can be done using computer-aided design (CAD) software such asAutoCAD (Autodesk) or SOLIDWORKS (Dassault Syst`emes)
• Scaling and layout of parts is easily done with the programs provided by theprinter companies or with independent programs such as Slic3r (slic3r.org)
• Parts can be printed in a wide spectrum of colored filament feedstocks that can betransparent, opaque, fluorescent, glow in the dark, or metallic

Printing
• Three-dimensional printing utilizes the fundamentals of inkjet printing; however,
in lieu of ink, the print head extrudes melted thermoplastic filament in a layering
process to create a 3D object
• This additive process is referred to as molten polymer deposition or MPD
• Common feedstocks include PLA (polylactic acid) thermo-bioplastic or a more
durable ABS (acrylonitrile butadiene styrene) thermoplastic
Printing
• These plastic filaments are readily available online from many manufacturers or
through suppliers such as Home Depot and Staples
• Currently, the process of printing a complete lightweight child-sized hand on a
consumer level 3D printer may take 20 to 30 hours

Assembly
• Assembly, often completed by watching instructional online video tutorials, adds a
few additional hours and requires non printable parts such as nylon string, elastic,
and medical-grade foam
• Hand parts snap together like Legos and can be assembled similar to a toy
• Three-dimensional-printed prostheses are typically composed of 12 main modular
pieces—5 distal phalanges, 5 proximal phalanges, 1 palm, and 1 wrist piece—as
well as printable hardware, tensioner pins, and attachments
• Prostheses can be assembled with household tools such as pliers, screwdrivers,
and scissors
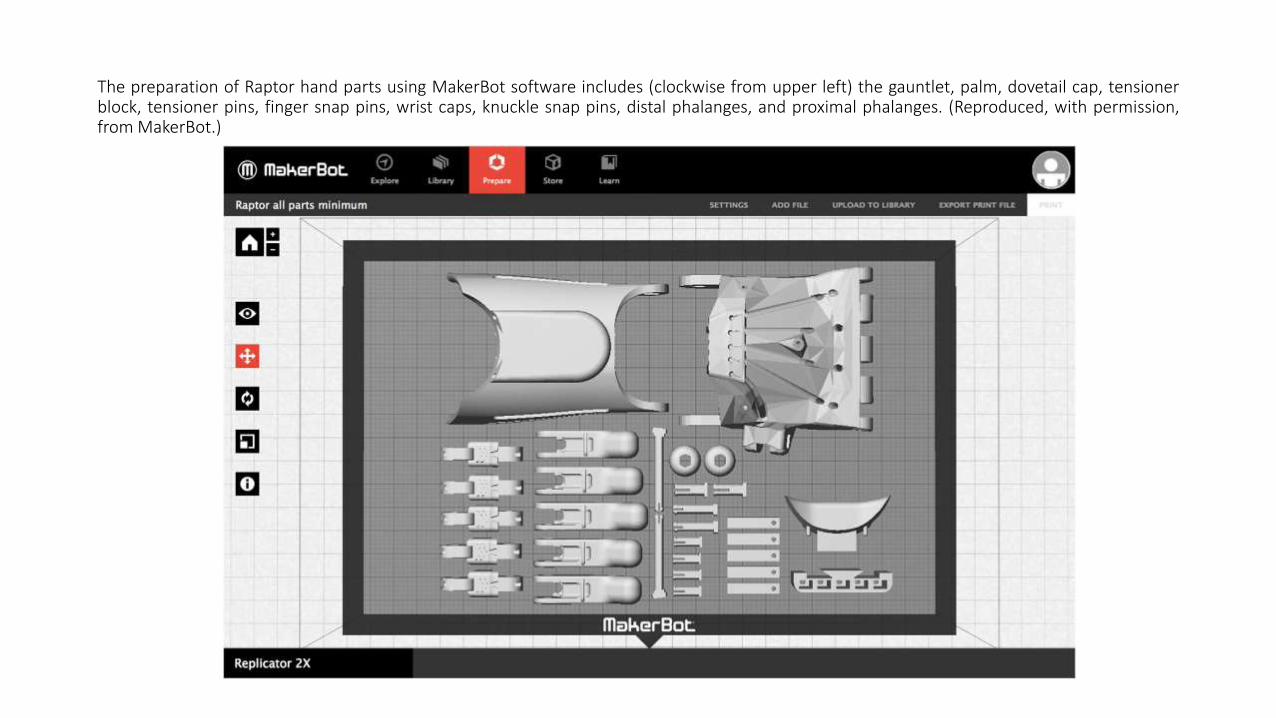
The preparation of Raptor hand parts using MakerBot software includes (clockwise from upper left) the gauntlet, palm, dovetail cap, tensionerblock, tensioner pins, finger snap pins, wrist caps, knuckle snap pins, distal phalanges, and proximal phalanges. (Reproduced, with permission,from MakerBot.)

Fitting
• Tailoring a 3D-printed prosthesis to the recipient may require modifying the
medical-grade foam padding and Velcro straps, adjusting the tensioning system to
an appropriate level for the recipient’s muscular development, and
thermoforming—gently heating plastic forms to take the contour of the recipient’s
hand or wrist
• While creation of a 3D-printed prosthesis may require only one individual, the
process of utilizing such a device and ensuring a proper fit ultimately involves the
medical care team, including the child’s physician and occupational therapist
Safety
• While PLA and ABS in their solid forms are generally considered inert,
individuals utilizing 3Dprinters should consider the fumes emitted during the
molten polymer deposition phase
• Stephens et al. conducted research on the ultrafine particle emissions of consumer-
level 3D printers and found that both PLA and ABS thermoplastics emit high
levels of ultrafine particles
• To avoid health complications, the authors advised that these machines should be
used with adequate ventilation
• Prosthetic breakage does occur and poses the same potential threats as broken
rigid plastic toys. Parts can be dangerous if swallowed, if aspirated, or if the parts
cause abrasion

Cost and Availability
• Material costs for 3D printing of a body-powered hand device may be between
$20 and $50, and an arm device may cost between $50 and $150
• These costs are compared with the current estimate for a professionally made,
body-powered prosthesis that ranges from $4,000 to $10,000
• Three-dimensional printers currently range from $500 to $4,000

Cost and Availability
• Because of the nature of open-source files and the increased availability of 3D
printers at local public libraries and schools, it is possible for an individual to print
his or her own prosthetic hand for the cost of materials alone
• Sites like MakerBot’s Thingiverse (thingiverse.com) and the National Institutes of
Health (NIH) 3D Print Exchange (3dprint.nih.gov) host many prosthetic designs
• For those not inclined to produce their own device, a global network of volunteers
is available to supply the hand devices

Cost and Availability
• At the time of writing, the e-NABLE network numbered 6,000 volunteers and had
produced >1,500 free hand devices for recipients in 40 countries
• Close approximations for sizing can be calculated by the maker or entered into a
calculating program, such as e-NABLE’s Hand-o-matic software application, from
a few simple measurements provided by the recipient
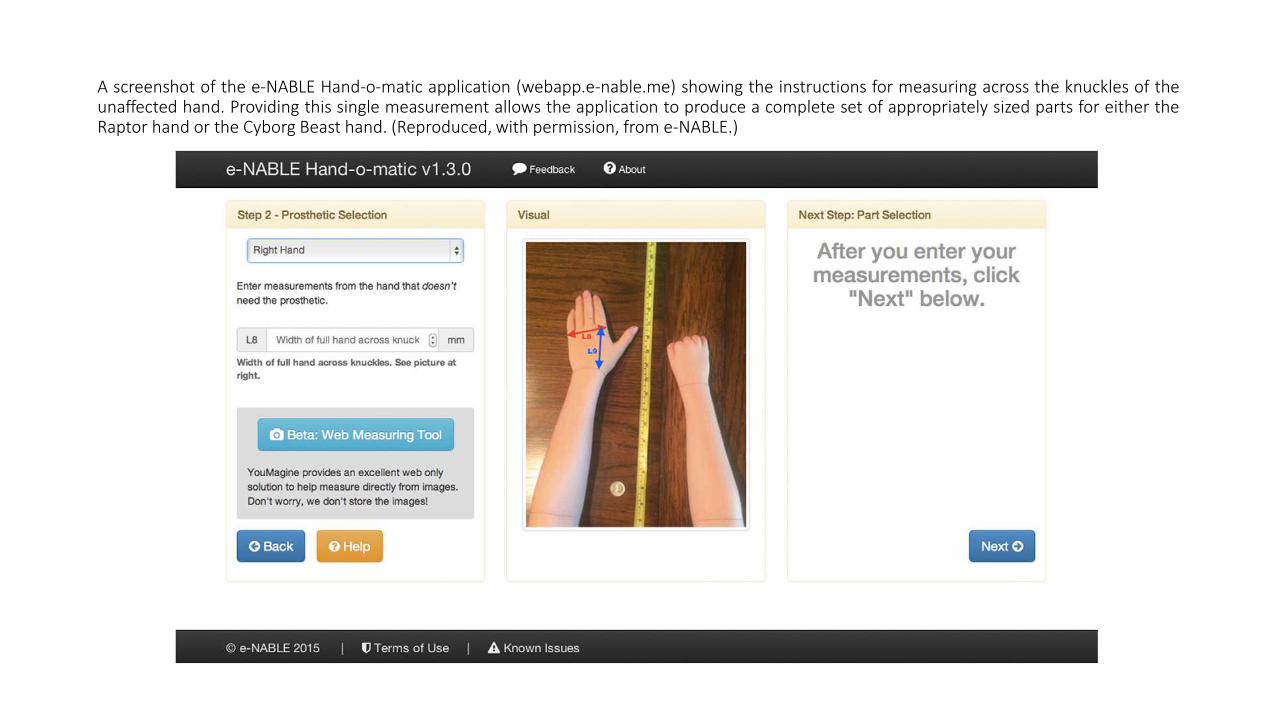
A screenshot of the e-NABLE Hand-o-matic application (webapp.e-nable.me) showing the instructions for measuring across the knuckles of theunaffected hand. Providing this single measurement allows the application to produce a complete set of appropriately sized parts for either theRaptor hand or the Cyborg Beast hand. (Reproduced, with permission, from e-NABLE.)

Patient Selection
• Children with upper limb differences are ideal candidates for currently available 3D-
printed devices because they quickly outgrow prostheses, and the low cost of 3D printing
makes repairs and upgrades affordable
• Zuniga et al. described the development technique of the Cyborg Beast 3D-printed device
and suggested that the “prosthetic hand and the proposed distance-fitting procedure
represent a possible low-cost alternative for children in developing countries and those
with little or no access to health-care providers”
• It is recommended that the children receive proper fitting, training, and follow-up with a
multidisciplinary team to ensure success

Patient Selection
• Although Davids et al. documented the benefits of fitting children with upper
extremity prostheses before the age of 3 years, many 3D-printed devices are not
recommended for children under 4 years old because of their often-limited ability
to express discomfort and the fact that free distribution of these devices is often
not monitored by a health-care professional
• Prostheses for very young children, with smaller parts and hardware, may also be
limited by the print resolution of the 3D printer

Patient Selection
• Socket creation is the art and science of a well-trained and experienced prosthetist
• The 3D-printed prostheses currently available replaced the socket with a wrist
piece that attaches with Velcro straps to allow for an adjustable, if less precise, fit
• An uncomfortable prosthesis will never be worn, so training with an occupational
therapist is recommended for the most successful outcome
• Caregiver vigilance is important to ensure that devices fit properly and are not
causing distress or fatigue

Patient Selection
• A 3D-printed prosthesis can be lightweight, making it advantageous for children
and appropriate for upper limb prostheses
• When 3D printing technology is evaluated for adult-sized prostheses, several
challenges arise, including the physical limitations of the printer bed platform size;
the considerable print times of larger parts, which are more apt to incur print
failures; and the toy-like appearance of the majority of viable models
• Print-on-demand lower limb prostheses face similar challenges and are not
currently available because of the load-bearing challenges and limited strength of
available thermoplastic materials

Clinical Guidelines
• Clinical guidelines to determine which 3D-printed device a child or an adultshould receive do not currently exist
• There are dozens of hand and arm models available to address amultitude of upperextremity congenital absences, from single digit replacements to full hand andwrist models
• Typical congenital or acquired upper limb differences include amputations,transverse deficiencies (forearm, wrist, and hand), symbrachydactyly, ulnarlongitudinal deficiency, and amniotic band syndrome

Examples of available open-source hand models include (from left to right, top down) Robohand, Cyborg Beast, Flexy Hand, K-1 Hand, RaptorReloaded, Second Degree Hand, Osprey Hand, Limbitless Arm, and RIT Arm. These models are available through web sites such as Thingiverse(thingiverse.com) and the NIH 3D Print Exchange (3dprint.nih.gov).
Clinical Guidelines
• Generally, the minimum requirement to operate the muscle-assisted devices is wrist
flexion of 30 or, in the absence of a wrist, elbow flexion of 30
• The complexity of natural finger articulation is reduced in 3D-printed hand devices to
a binary operation in which all 5 fingers contract or release in unison
• This is true for most currently available hand designs, even those with myogenic
options for movement

Clinical Guidelines
• Three-dimensional printed hand and arm designs are still in their infancy and are
often physically bulky, toy-like, and well received by children
• While not ideal for all daily tasks, the 3D printed hands are useful among children
for activity-specific applications such as sports or bike riding
• As with any plastic device, physical activity can be rough on the material, and
breakages will most likely occur

Clinical Guidelines
• Broken parts can be reprinted and replaced
• Maintenance of the devices currently falls on the caregivers
• The designs and color schemes are commonly tailored to the child’s desires, and
many children anecdotally report an increased social confidence and a “superhero-
like feeling” of having a personalized 3D-printed hand that is colorful and fun

Clinical Guidelines
• According to the findings of James et al., the quality of life for children withcongenital upper limb deficiencies was not substantially improved, and noimprovement in functionality was observed, by the addition of conventionalprosthetic devices
• Wagner et al. reported that for pediatric patients who rejected conventionalprostheses, the preeminent reason given was a lack of function, commonlyfollowed by dismissal of the device
• The introduction of a prosthetic device may then be thought of as a supplementalelective tool conducive to particular activities, such as social gatherings or sportsfunctions, as it may not be necessary or appropriate for all-day use
Outcomes
• Multiple validated pediatric and adult measures are available to evaluate patients who
use upper limb prostheses with respect to function, quality of life, and adoption of the
prosthesis into activities of daily living
• For example, the International Classification of Functioning, Disability and Health
(ICF), created by the World Health Organization, reports on overall health measures
for users of upper extremity prostheses and includes pediatric metrics for participation
and activity outcomes as well as adult emotional and psychosocial metrics
• Lindner et al. suggested that several tests for hand function can be utilized as metrics
for users of upper extremity prostheses

Outcomes
• These include the Assisting Hand Assessment (AHA), Box and Blocks test,
Jebsen-Taylor Hand Function Test, and Southampton Hand Assessment Procedure
(SHAP)
• The same metrics can be applied to 3D-printed prostheses, althoughwe know of no
current research that has examined 3D-printed prostheses with a quantified or
qualified metric

Outcomes
• Currently, no data exist to demonstrate how 3D-printed prostheses affect pediatric
usage
• Household 3D printers are increasing the number of prostheses available, and
studies are needed to assess the advantages and disadvantages of non-
commercially produced 3D-printed prostheses
• There are many reasons for an individual with an amputation or a child with a
limb congenital absence to discontinue the use of prostheses
• Three-dimensional printing may provide a less expensive way to explore a child’s
interest in prostheses

Overview
• On an Internet-connected world stage of engineers and volunteers, 3D-printedupper extremity prostheses are emerging as a disruptive technology that calls for areevaluation of the current model of manufacturing and distribution of prostheses
• It is important to understand that there is no current approval of these open-sourcedevices by the U.S. Food and Drug Administration and no regulation on theirdistribution, despite a daily increase in the production of these devices bynonclinical participants
• Members of multidisciplinary health-care teams should be aware that recipients ofthese hand and arm devices may be prompted to contact their physicians andmedical providers to determine a course of training and therapy, effectivelydefaulting the health impact responsibility from the makers to the health-care team

Overview
• As the crowd-sourced innovation movement of 3D printing of prostheses surges
forward, it may prove useful for surgeons and physicians to provide feedback or
medical perspective to online maker communities to help guide their development
• Participation in Internet communities may also provide the most current
information from developers and creative engineers regarding available hand and
arm devices
• Incorporation of a patient’s 3D-printed hand or arm into occupational therapy
sessions in an outpatient setting may help to ensure that the device fits properly
and that training is provided to deter harm and increase success

Overview
• Studies to evaluate function, adoption, and quality outcomes among different
design types or compare them with orthotist-produced prostheses are needed
• Parallel developments in brain-controlled prostheses and robotics will likely
merge with 3D-printed devices to keep costs lower and increase options for
growing children

THANK YOU