Embed Size (px)
Citation preview

Rickettsial Diseases

•Rocky Mountain spotted fever was first discovered in 1896 in the Snake River Valley of Idaho.
•Howard Taylor Ricketts first to identify the infectious organism.
•Also died from typhus

R. rickettsii
R. africae
R. conorii
R. conorii
R. slovaca
R. conorii Astrakhan
R. conorii Israël
R. australis
R. honei
Indian tick typhus Rickettsia
R. japonica
R. mongolotimonae
R. helvetica
R. mongolotimonae
R. sibirica
R. conorii
R. conorii Israël
« R. heilongjiangii »
R. helvetica

Characteristics of Rickettsia
• Gram (-), Aerobic, Coccobacilli
• Obligate intracellular parasite.
• Maintained in animal and arthropod reservoirs

Rickettsial Family
3 genera - obligate intracellular parasites:
– Rickettsia
– Coxiella
– Ehrlichia

Life Cycle of Rickettsia

Pathogenesis: Rickettsia
• Arthropod bite
• Invade endothelial cells/vascular : Have Phospholipase causing cell membrane injury…phagocytosis… cytokines (TNF, interleukines ..etc)
• Destroy endothelial cells
• Inflammatory cells accumulate/blood leakage: spots, rashes
• Released organisms reinfection.



Rickettsia as a Pathogen
• Transmitted and dependant on parasitic arthropod vectors: lice, fleas, and ticks.
R. prowazekii:
Epidemic typhus
human louse
R. typhi:
Murine typhus
flea
Rickettsia rickettsiae
RMSF
tick

Target Organs of Rickettsioses
Disseminated endothelial infection
of all organs with brain and lungs as
critically affected vital organs

Pathophysiology of Rickettsial Diseases
Increased vascular permeability
Edema (life threatening in brain and lungs)
Low blood volume
Hypotension
Decreased perfusion of organs
Organ dysfunction
(e.g., acute renal failure: prerenal azotemia)
Pathophysiology of Respiratory Failure
Intense infection of endothelium of pulmonary microcirculation
Interstitial pneumonia/edema
Non-cardiogenic pulmonary edema
Adult Respiratory Distress Syndrome
Hypoxemia


Types of Rickettsial Diseases
• R. rickettsii: Rocky mountain spotted fever
– Spread by tick bite; rodents are the reservoir
• R. prowazekii: epidemic typhus
– Humans primary host; vector is the louse
– Disease spread in crowded, unhygienic conditions
• R. typhi: murine/endemic typhus
– present in rodent population, vector is the flea.

Signs of Infection
• Fever, chills
• Severe headache
• 4th-6th day later = skin rash = lasts throughout course of disease
• EXCEPTION: Q-fever = no rash
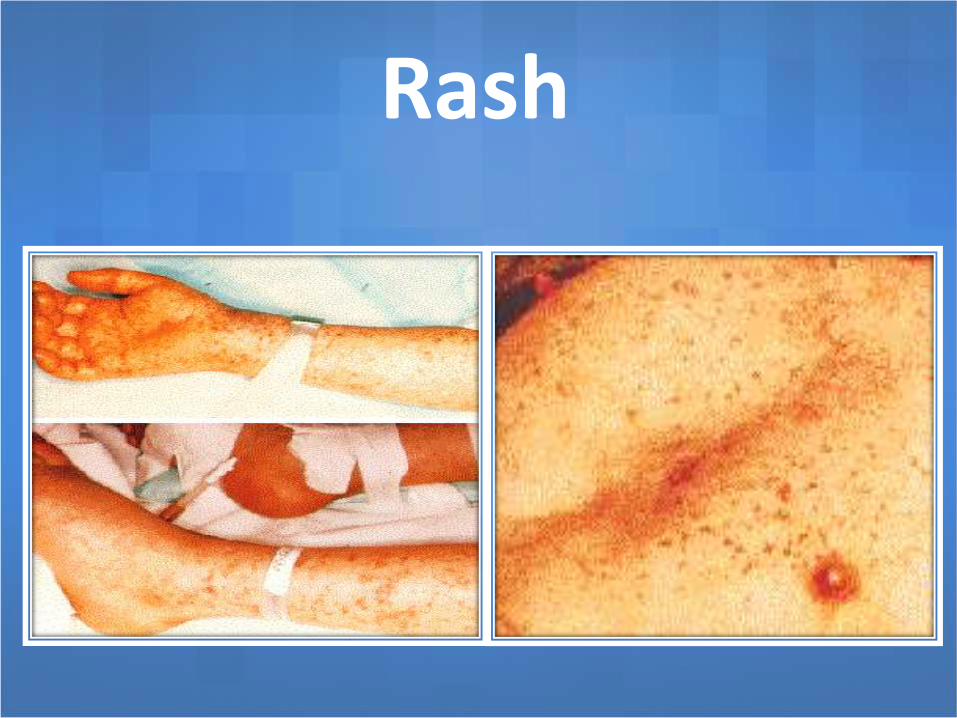
Rash

Important Clinical Diseases
• Spotted Fever Group– Rickettsia rickettsii = Rocky Mountain spotted fever
• tick bite
• fever/severe headache
• skin rash = wrists and ankles to trunk/palms of hands, soles of feet


Rickettsia rickettsii
• R. rickettsii causes 95% of all modern typhus.• If untreated mortality is ~20%.• Most cases occur in children during the spring or
summer.• It causes “tick typhus”, also known as Rocky Mountain
spotted fever. • The wood tick or dog tick is the insect vector.. • CNS symptoms include headache, delirium and coma.• Circulatory damage includes coagulation, edema and
collapse..

Important Clinical Diseases
• Typhus Group
–Rickettsia prowazekii = Epidemic typhus
• body louse = bite/feces
• fever/severe headache
• skin rash = trunk to extremities
Rickettsia prowazekii
• causes louse typhus, ie. epidemic typhus, or Brill-Zinsser disease (or these days “jail fever” ).
• This organism killed ~3 million people in WW1 .
• Transmission occurs human to human via lice vector, either directly in blood, or more likely as the contaminated louse feces is scratched into the bite wound.
• Symptoms can be acute and RMSF-like, or a milder sporadic / latent condition years after the initial infection.

Rickettsia typhi
• R. typhi causes Murine typhus or endemic typhus.
• cases occur commonly and a few at a time in endemic areas.
• reservoir is rodent (murine = rodent) and vector is the flea.
• scratching contaminated flea feces into the bite wound is the primary means of transmission.
• The rash is backwards here: trunk extremities.
• Murine typhus is milder, and will resolve untreated within 3 weeks.

Boutonneuse fever
– R.conori, tick vector, I.P: 6-10 days
– Generalized myalgia occurs, and even myositis can be demonstrated.
– A rash appears on days 3-5 of the illness. It spreads from the extremities to the trunk, neck, face, palms, and soles within 36 hours.
– The lesions progress from macular to maculopapular and may persist for 2-3 weeks.
– Eschar at site of tick bite is pathognomonic.
– Other manifestations and complications are similar to those seen in patients with RMSF.



Important Clinical Diseases
• Scrub Typhus Group
–Rickettsia tsutsugamushi =
Scrub typhus
• mite bite
• fever/severe headache
• skin rash = covers body/eschar
Important Clinical Diseases
• Q-Fever Group
–Coxiella burnetii - Q fever
• inhale contaminated aerosol; resist dessication = up to 3 years outside host
• intermittent fever/pneumonia
• NO skin rash
Diagnosis of Rickettsial Diseases
• No rapid laboratory tests are available to diagnose rickettsial diseases early in the course of illness.
• Rise in serum antibody/often do not develop in early stages

Diagnosis of Rickettsial Diseases
o Serologic assays that demonstrate antibodies to rickettsial antigens (eg, indirect immunofluorescence, complement fixation, indirect hemagglutination, latex fixation, enzyme immunoassay, microagglutination)
o They are preferable to the nonspecific and insensitive Weil-Felix test based on the cross-reactive antigens of Proteus vulgaris strains(OX19)
o It usually takes 10-12 days for serologic data to become positive..
Diagnosis of Rickettsial Diseases
o Polymerase chain reaction (PCR) to detect rickettsiae inblood or tissue provides promise for early diagnosis.
o PCR and fluorescent antibody testing of skin specimenobtained by biopsy may help confirm the clinicaldiagnosis in patients with rash .
o However, serology remains the mainstay of diagnosisbecause these other tests are expensive and lessavailable to clinicians.
o Rickettsial isolation in culture is unnecessary,laborious, and hazardous to laboratory personnel.

Disease Confirmatory testRMSF IFA, DFA, IHMediterranean SF IFA, DFA, IH, PCREpidemic Typhus IFA, PCRMurine Typhus IFA, DFA, PCR… LFT
IFA: Indirect fluorescent antibody assayDFA: Direct fluorescent antibody IH: Immunohistology

TREATMENT
• Rules :
– You will never make a definitive diagnosis before the patient recovers with treatment or dies
– High index of suspicion with good understanding of epidemiology is important for diagnosis
– Empiric therapy with doxycycline with a VERY rapid improvement after only a few doses
– Save acute and convalescent sera for testing if possible.

TREATMENT
Doxycycline is a drug of choice for treating suspected Rocky Mountain Spotted Fever in all patients
Dosage:Children: 2mg/kg PO q12 on day 1<45kg then
2-4mg/kg qd until afebrile for 2-3 days
Adults: 100mg PO q12 on day 1then
100mg qd until afebrile for 2-3 days

Tetracycline – In ChildrenPermanent Teeth Staining
• There is a dose dependent relationship between tetracycline and teeth color
• 5 courses of tetracycline are required to produce a perceptable difference in tooth color
• Doxycycline produces less tooth staining
Despite effective treatment and advances in medical care, approximately mortality is still 3- 5%

Prevention - Tick Removal

Tick collection: flagging
Rubber plantation

Tick collection on animals

Prevention - Deer BarriersLimiting exposure to ticks is currently the
most effective method of prevention.

Case Presentation
A.A.A.J is 5-year-old girl from Rafah, presented with 6 days complaint of fever, and 4 days history of generalized weakness, loss of appetite and skin rash.

History of present illness
• 6 days back she was perfectly well when she started tohave high grade fever which was progressivelyincreasing to which she received paracetamol withoutproper improvement.
• 2 days after she started to have skin rash more in lowerand upper limbs increasing with the spikes of feverduring that time she was refusing to eat so they soughtmedical advice where she was given cephalexin andparacetamol suppositories,
• after 3 days of treatment she came to E.R in ourhospital and admitted with the same complaint.
History
• There is past history of skin disease( Scabies) 6 months back and improved after receiving a skin lotion.
• She was born as preterm 35 weeks with birth weight of 2000 grams and admitted to SCBU because of mild RDS.
• Parents are first degree cousins, there is a history of death of one boy sibling at age of 15 months because of chest infection, the other 4 living siblings (boys) are normal.
• They live in a 5-rooms house, they have animal pets behind the rooms containing goats.
• She completed her vaccination schedule.• Her developmental history is within normal.
Examination
• Vital signs: Temp.: 39°C, Pulse: 115/m., B.P: 105/55, R.R: 22/min.
• Weight: 17.5 kg, Height: 102 cm (25th %).
• She looks ill, febrile, oriented in time and place, no signs of meningeal irritation.
• There is generalized rash including palms and soles.
• Throat is mildly congested.
• C.V.S: PPP, normal s1+s2, no murmur.
• Chest: fair A/E, no added sounds
• Abdomen: soft, no organomegaly.
• C.N.S: examination is normal.



Investigations
• CBC: WBC: 6.1, lymph:41%, Neut.:52%, Hb: 10.9gm, Plt:161,000.
• Urea:16, cr.:0.5, Na:130, k:3.9.
• LFT: mildly elevated
• PT, PTT : normal.
• Brucella: negative
• Widal: negative,
• OX19: 1:80 (sign.1:160)

Hospital Course
• On admission she was given:
Doxycycline tablets:
- first day: 50 mg BiD
- 2nd day onward: 50 mg daily
• Fever subsided on the 3rd day.
• Discharged after 5 days in good condition.






























