Embed Size (px)
Citation preview
RETROPERITONEAL FIBROSIS
Dr.Gaurav NaharDNB (Std.), Urology,M.M.H.R.C., Madurai
INTRODUCTION Uncommon condition.
A fibro-inflammatory mass envelops and potentially obstructs retroperitoneal structures, including either or both ureters.
Fibrous, whitish plaque encases aorta, IVC & their major branches, ureters, other retroperitoneal structures, at times intraperitoneal structures including GIT.
Centers around distal aorta at L4-L5 and wraps around the ureters, leading to hydronephrosis via extrinsic compression on the ureters or interference with ureteral peristalsis.
Extent:Longitudinal- from renal hilum to pelvic
brim(Aotic bifurcation); may extend into the pelvis, mediastinum and optic orbit.
Transverse-laterally to outer edge of psoas muscles.
AKA- Periureteritis fibrosa/plastica, Chronic periureteritis, fibrous retroperitonitis, sclerosing RP granuloma.
Ureteral obstruction in RPF appears minimal despite severe renal failure. This suggests that obstruction relates to impairment of normal ureteric peristalsis by fibrotic tissue rather than to mechanical obstruction.
EPIDEMIOLOGY
Peak age of incidence: 40-60 years.
Rarely in children.
Male predominance; M:F Ratio 2-3:1
Estimated annual incidence: 1 per 200,000-500,000 population.
No racial predilection.
ETIOLOGY Idiopathic-70%(Ormond’s disease): Inciting
etiology not defined.
Definitive etiology in 30%.
Suspected Causes of RPF Drugs
Methysergide
Hydralazine
Reserpine
Haloperidol
LSD
Methyldopa
β Blockers
Ergotamine alkaloids
Phenacetin
Amphetamines
Pergolide
Bromocriptine
Chemicals
Avitene
Methyl methacrylate
Talcum powder
Hemorrhage
Abdominal and pelvic surgery
Ruptured viscera
Henoch-Schönlein purpura with hemorrhage
Infection
Gonorrhea, Syphilis
Tuberculosis,Histoplasmosis,Actinomycosis
Chronic urinary tract infection
Inflammatory processes
Ascending lymphangitis
Chronic inflammatory bowel disease
Asbestosis
Amyloidosis
Erdheim-Chester disease
Sarcoidosis
Retroperitoneal tumors
Lymphoma
Sarcoma
Multiple myeloma
Metastases(breast, lung, stomach, colon, bladder, prostate, cervix)
Periarteritis
Aortic or iliac artery aneurysm
Inflammatory response to advanced atherosclerosis
Collagen vascular disease
Radiation injury
Other
Biliary tract disease
Endometriosis
PATHOGENESIS Exact pathogenesis- unclear.
Good evidence: an immunologic response to antigens within atherosclerotic plaques.
Vasculitis of adventitial vessels of aorta & perioaortic small vessels → release of antigens from atheromatous plaque such as ceroid, a complex lipoprotein → induces an autoimmune antigenic response → local inflammation & fibrosis.
Other immunologic events: CD3+ & CD20+ lymphocytes, IgG4-positive plasma cells identified.
Immune reaction to an external agent: Drugs/chemicals act as haptens-induce hypersensitivity or immune reaction.
In Carcinoid tumor: result of circulating serotonin or its metabolites.
Methysergide is a strong serotonin antagonist; Rebound serotonin release after prolonged intake may be an alternate mechanism.
Genetic influence- no major role, as no reports of familial clustering.
ASSOCIATION WITH OTHER AUTOIMMUNE DISORDERS:
HLA-DRB1*03 or HLA-B27 haplotype.
• Primary biliary cirrhosis• Sclerosing cholangitis• Autoimmune Pancreatitis• Fibrosing mediastinitis• Immune complex Membranous Glomerulonephritis• Panhypopituitarism• Rheumatoid arthritis• Ankylosing spondylitis• Polyarteritis nodosa• Systemic lupus erythematosus (SLE),Scleroderma• Hashimoto thyroiditis, Reidel’s thyroiditis.• Uveitis• Psoriasis• Amyloidosis

CLINICAL FEATURES Non-specific signs & symptoms.
Duration of symptoms prior to diagnosis: 4-6 months.
50% patients present with significant ureteric obstruction & uremia.
SYMPTOMS: M.C.symptom(92%)-dull, poorly localized,
noncolicky pain in flank, back, or lower abdomen. Unrelated to posture; relieved by aspirin.

In children, pain may be referred to ipsilateral hip or gluteal region, resulting in resistance to hip extension.
Fever
Lower-extremity edema Phlebitis Deep venous thrombosis
Weight loss, nausea, vomiting, anorexia, and malaise: Uncommon.
Raynaud phenomenon, ureteric colic, hematuria, claudication, and urinary frequency: Rare.
SIGNS: Hypertension: Present in 50% Presence of an abdominal mass
(occasionally) Ureteric obstruction with varying degree of
renal insufficiency: Earliest and M.C.organ involved.
Uncommon physical findings due to late complications:
Ascites Peripheral edema or thrombosis Hydrocele Jaundice Small- or large-bowel obstruction Spinal cord compression

Hypertension: results from many factors.
An increase in renin release secondary to obstructive uropathy.
In some patients, volume-dependent hypertension may result from obstructive nephropathy.
INVESTIGATIONS & DIAGNOSIS
Laboratory Studies Blood
Elevated ESR & CRP(acute phase reactants) Raised urea & creatinine(50%-75%) Normocytic normochromic anemia, Moderate
leukocytosis Polyclonal hypergammaglobulinemia Alkaline phosphatase Antinuclear antibodies (ANA;60%) rheumatoid
factor, and antibodies against smooth muscle, ds-DNA, extractable nuclear antigen and neutrophil cytoplasm
Urinalysis Usually normal.
Rarely, microscopic hematuria or pyuria.
IMAGING STUDIES:
PLAIN RADIOGRAPHY: Nonspecific findings. Obliteration of psoas shadow & an enlarged
renal outline due to hydronephrosis.
INTRAVENOUS UROGRAPHY (IVU): The classic triad (18-20%)1. U/L(20%) or B/L(68%) hydronephrosis,2. Medial deviation of middle third of ureters,3. Tapering of ureter at L4/L5 level.

IVU shows medial deviation of middle part of both ureters

RETROGRADE PYELOGRAPHY:
Demonstrates poor distensibility of ureter.
Delineates PCS anatomy; performed prior to stent insertion to decompress the kidneys.
Interestingly, very little resistance is encountered during ureteric catheterization despite extensive extrinsic fibrosis.
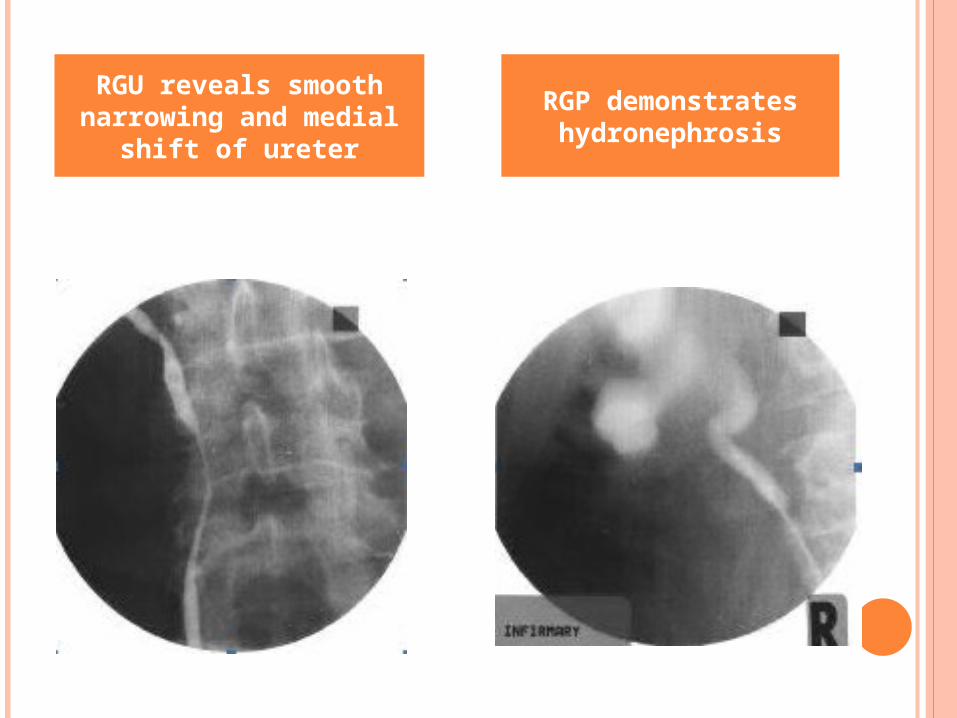
RGU reveals smooth narrowing and medial
shift of ureter
RGP demonstrates hydronephrosis

LYMPHANGIOGRAPHY:
Obstruction of lymphatic flow at L3/L4 level,
Opacification of collateral channels,
Nonvisualization of lymphatics above L4 vertebra,
Delay in passage of contrast through iliac and para-aortic lymphatics.
Obsolete nowadays.

ULTRASONOGRAPHY:
Simple noninvasive modality used to assess response to therapy.
RPF appears as a retroperitoneal, extensive, well-defined, hypoechoic mass centered over the sacral promontory.
Degree of hydronephrosis and hydroureter may vary.
Doppler ultrasonography has no role in differentiating benign from malignant RPF.
CT SCAN: Most frequently used imaging method for
diagnosis & follow-up of RPF.
Unenhanced CT: o RPF appears as a plaque that is isodense
with muscleo envelops aorta & IVC b/w the renal hila &
sacral promontoryo usually extends laterally to incorporate
ureters.o Obliteration of the fat plane between the
mass and the psoas muscle may be observed.
CECT:o Plaque may show a variable degree of
enhancement, depending on stage of the disease. Significant enhancement in the early active vascular stage, but poor in the late avascular stage.

NCCT scan: periaortic fibrotic reaction associated with an inflammatory aortic
aneurysm & bilateral ureteric stents
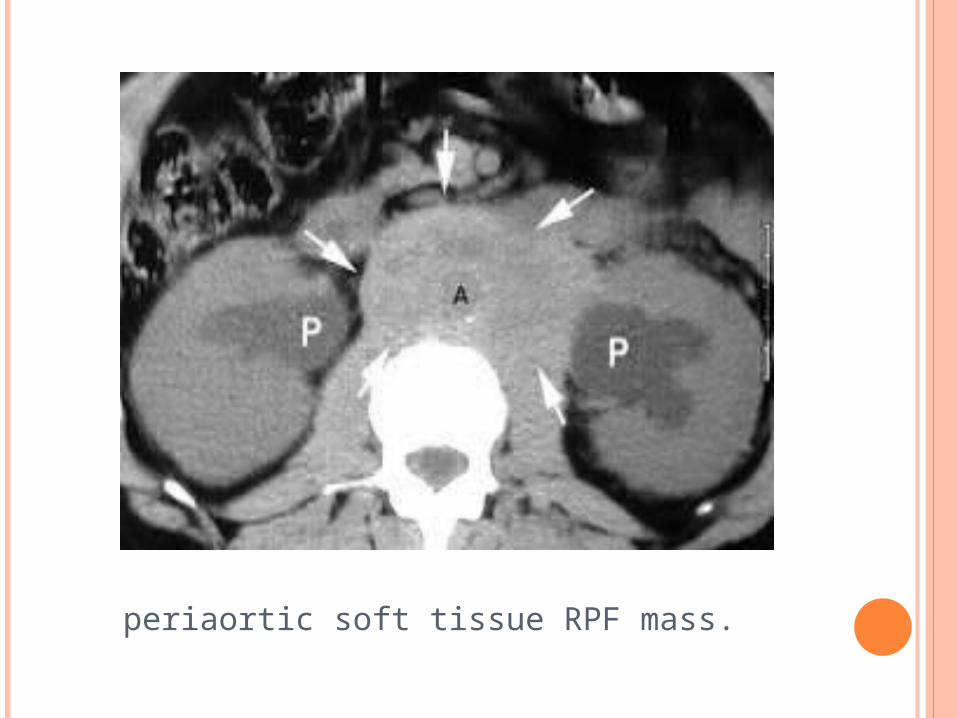
periaortic soft tissue RPF mass.
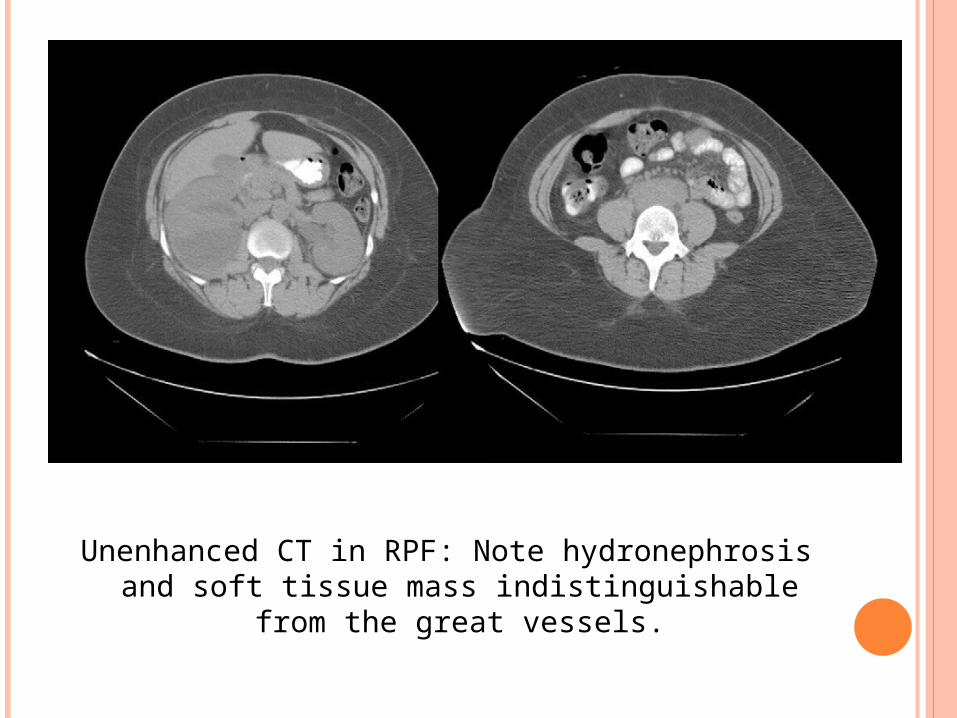
Unenhanced CT in RPF: Note hydronephrosis and soft tissue mass indistinguishable from
the great vessels.
MAGNETIC RESONANCE IMAGING:
o T1-weighted images: Both benign and malignant RPF have low-to-intermediate signal density density.
o T2-weighted images vary based on disease stage. Early stage- signal density is high because of high fluid content & hypercellularity.
o Late-stage disease has low T2 signal intensity as a result of avascular acellular fibrosis & decreased fluid content.(majority of plaque is composed of fibrosis)
WHY MRI IS SUPERIOR TO CT IN RPF:
Independent of patient’s renal functional status.
More accurately distinguishes the plaque from the great vessels than unenhanced CT.
The disease can be followed without radiation exposure of repeated CT.
Enhancement ratios can be calculated with dynamic gadolinium enhancement; can be used to assess disease activity & monitor treatment responses.
18-FDG PET SCAN:
o 18F-fluorodeoxyglucose positron emission tomography (F-18 FDG PET) detects glucose hypermetabolic activity.
o Degree of inflammation in the plaque, which may predict response to immunosuppressive therapy as well as its therapeutic response.
oCan also reveal other sites of disease (thyroid, thorax) and may help to identify the most appropriate sites for retroperitoneal biopsy.

Gallium-67 single photon emission–computed tomography (SPECT) scintigraphy
In the acute phase, RPF may take up gallium-67, due to binding of gallium-67 to lymphocytes.
Used for:o Evaluating responses to medical therapy of
RPF.o Detection of recurrent disease.o Demonstrates both the mass lesion and its
inflammatory component.
BIOPSY: Open, Laparoscopic,
Percutaneous(USG/CT/MRI guided). Core tissue biopsy (histologic confirmation)
is preferred over FNAC assessment.
RPF progresses through 2 clinical stages:(1) Early inflammatory phase: an inflammatory
infiltrate(both perivascular and diffuse) contains macrophages, lymphocytes, plasma cells, and occasional eosinophils; highly vascular & cellular.
(2) Late fibrotic phase: avascular & acellular with scattered calcification and fibrous scarring. consists of myofibroblasts and type-1 collagen.
Submucosal edema and lymphocytic infiltration may be observed in the ureter.
Malignant RPF: scattered nests of malignant cells within the inflammatory infiltrate.
TREATMENT
Goals of m/m:1. to preserve renal function.2. to prevent other organ involvement.3. to exclude malignancy, and4. to relieve symptoms.
Treatment of retroperitoneal fibrosis depends on disease stage at diagnosis, & patient’s clinical status.
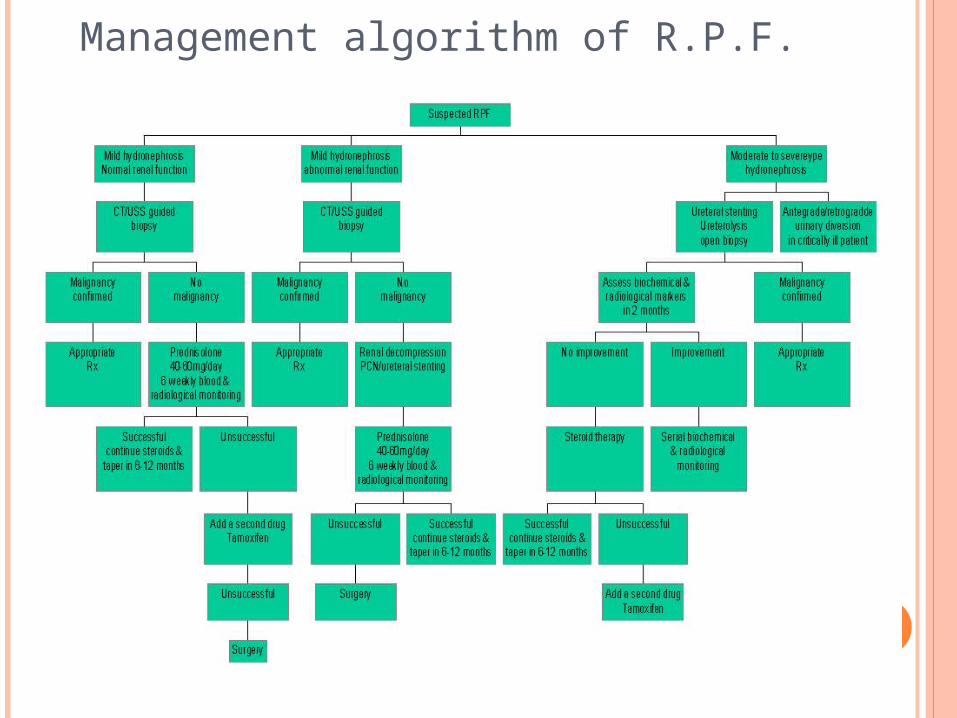
Management algorithm of R.P.F.
Patients with hydronephrosis and uremia- Emergency decompression by PCN or Indwelling DJ stent.
Close monitoring for post-obstructive diuresis(Urea diuresis, Sodium diuresis), renal function status, & appropriate fluid & electrolyte replacement.
Search for inciting cause; offending drugs discontinued.
Imaging & Biopsy to rule out malignancy.
Medical Management:
Empirical therapy includes corticosteroids, tamoxifen, and azathioprine;
Experimental therapy-azathioprine, cyclophosphamide, mycophenolate-mofetil, cyclosporin, medroxyprogesterone acetate, and progesterone.
Glucocorticoids and azathioprine: most useful in patients with signs of inflammation (eg, raised ESR and WBC count and positive ANA results)
CORTICOSTEROIDS: Beneficial effect: due to anti-inflammatory action &
ability to inhibit fibrotic tissue maturation.
A standard protocol is prednisolone at 40-60 mg/d tapered to 10 mg/d within 2-3 months and discontinued after 12-24 months.
Prednisolone oral 60 mg on alternate days for 2 months, tapered to 5 mg daily over next 2 months. The latter dose is continued for a total of 2 years.
Methylprednisolone pulse therapy (MPPT) at 1 g/d IV for 3 days along with azathioprine or penicillamine.
Steroids can be used in combination with surgery.
Characteristic clinical response to steroid therapy: resolution of pain and constitutional symptoms within days after treatment, a rapid fall of erythrocyte sedimentation rate, and diuresis.
TAMOXIFEN: Tamoxifen increases the synthesis and
secretion of transforming growth factor–beta (TGF-b), an inhibitory growth factor, by human fetal fibroblast in vitro.
Other possible mechanisms of action: inhibition of protein kinase C, reduction of epidermal growth factor production, inhibition of calmodulin, and blockage of growth-promoting histaminelike receptor.

Mycophenolate mofetil Blocks the proliferation of T cells and B cells.
Surgical Management: Open Ureterolysis
Midline, transperitoneal abdominal incision.
Preoperative RGC placement to facilitate identification & dissection.
Bilateral ureterolysis, even if single ureter invloved.

After B/L ureterolysis, repositioning of ureters & protection from fibrous entrapment.
Lateral retroperitonealisation: retract the ureters laterally and secure the overlying peritoneum medially to the psoas muscle to maintain the ureters in this location.
Intra-peritonealisation: close the peritoneum behind the ureters so that the ureters may be displaced anteriorly into the peritoneal cavity.
Omental wrap: In extensive RPF cases, surround the ureters with omentum and reposition them within the peritoneal cavity.
Ureteral wrap in PTFE vascular graft/Gore-tex graft.

Laparoscopic ureterolysis: Transperitoneal four-port approach. 3-4 ports placed along the midline1. Umbilicus2. B/w umbilicus & pubis3. B/w umbilicus & xiphoid
Advantages: Rapid recovery, shorter hospital stay & less morbidity.
POST-OP CARE: Removal of ureteric stents 6-8 weeks after
surgery .
Postop Steroid therapy may be considered to avoid recurrence.
OTHER OPTIONS: High-risk & elderly patients- long term
ureteral stents.
Ureterolysis not possible d/t extensive fibrosis & ureteric stricture:-
o Ileal substitutiono Appendix substitutiono Renal autotransplantation.
If lower ureter involved- Boari’s flap.
Poor Kidney function despite salvage decompression & N contralateral kidney- Nephrectomy.

Further Outpatient Care: Biochemical markers (CRP, ESR, renal
function) monitored every 4-8 weeks to assess response.
Radiologic assessment (CT, MRI) performed every 3 months; once disease stabilized, scanning can be repeated at 6 months.
Recurrence reported as late as 10 years; thus, long-term follow-up is necessary.
Renal failure patients- early Nephrology referral & continued follow-up.
COMPLICATIONS Renal failure Hypertension Scrotal edema Inferior vena cava thrombosis
PROGNOSIS
Non-malignant RPF- Good Malignant RPF- Poor.

THANK YOU