Embed Size (px)
Citation preview

- Large patient cohort prospective study with more than 500 patients and more than 5
years follow up have shown that CyberKnife is equally effective as long coures RT
- SBRT/ CyberKnife is now standard of care treatment for localized prostate cancer
- Outcome of CyberKnife treatment is similar to long course RT
- Side-effect after Cyberknife is less than 1% in prostate cancer
- CyberKnife is safe, out patient, short course treatment in both primary and metastatic
diseases.
- High dose radiation may be effective in many of the ‘radioresistant’ disease.
CyberKnife in prostate cancer

• Most prevalent malignancy in males in western community
• 2nd MC cause of mortality in the west
• Uncommon in Asians, probably shorter lifespan
• In TMH, constitutes 2.4% of all registered pts in 2000
• In recent years, more early prostate cancer patients are diagnosed
with prostate cancer
• Prostate cancer is slow growing tumour, risk of bone metastasis is
high in ‘high risk’ group patient
Prostate cancer

Risk stratification
RISK STRATIFICATION
LOW RISK INTERMEDIATE HIGH
T1,2a, PSA < 10 ng/ml,GS</=6
T2b, GS=7
T3,4,PSA>20ng/ml,GS>7
Wait & watchSurgeryRadiation therapyHTRadiosurgery
Combination
SurgeryRadiation therapyHTRadiosurgery
Combination
SurgeryRadiation therapyHTRadiosurgery
Combination

Radiotherapy Radiation techniques: 2D Planning Conformal Radiation therapy - 3D-CRT - IMRT - SBRT
Target volume: CTV – prostate with capsule + SVT1 & small T2 with less PSA less GS only prostate is
sufficient.PTV – 1 cm margin.
Inclusion of pelvic lymph nodes still controversial.

Ca prostate Incidence of pelvic LN metastasis at diagnosis
Study T1a,b T1c T2a T2b,c T3Pisansky 12/457
(2.6%)15/456(3.3%)
130/1206 (10.8%)
81/320(25%)
-
Petros & Catalona
2/61 (3.3%)
33/425(7.8%)
0
Sands 6/127 (5%) 41/243(16.9%)
95/199(47.7%)
Van Poppel
2/40(5%) 18/199(9%)
25/46(54%)
Hanks 1/21(5%) 38/135(28%) 48/95(50%)

Radiotherapy Radiation therapy schedules Conventional fractionation: - 70Gy/ 35# / 7 wk - 2Gy/# - Acute rectal & bladder toxicity
Hypofractionation schedule: - High dose per fraction, short course treatment - Equivalent loco-regional control
Ultra-hypofractionation schedule: - Very short course, high dose per fraction - Usual treatment duration 5 to 7 days

Conformal Radiation therapy reduces toxicity
• RCT• Royal Marsden Tait et al.
Gr 2 or more 5 Vs 15%.• Rotterdam trial Koper et al.
Grade 2 GI toxicity (32% vs. 19%, p = 0.02).
• M.D. Anderson Storey et al.No dif but Dose 78 vs 70.
• Nonrandomized trials• 15/27 improvement • Most pronounced when dose
escalation was not used.• When dose escalation was used, no
increased toxicity was demonstrated, except when the dose to the rectum >75 Gy.
• No article suggested increased toxicity with 3D-CRT for similar doses delivered compared withconventional RT.

WPRT VS PORT:RTOG trial 9413
• WP RT NCHT improves PFS compared with PO RT and NCHT or PO RT and AHT, and compared with WPRT + AHT in patients with a risk of LN involvement of 15%.
•Median follow-up : 59.5 mnths
• No OS advantage JCO 2003

Subset analysis of RTOG 9413
•Median PFS was 5.2, 3.7, and 2.9 years ( p 0.02). •7-year PFS was 40%, 35%, and 27%•RT field size has a major impact on PFS, and it is advised thatnodal treatment should be done in patients with a risk of LN inv >15% .
Roach IJROBP 2006

Dose escalation: improve LC

Author Study type Patient criteria Study details ResultsKurban et al Prospective
multi-institutional
N= 48391986-95T1-2 low risk prostate cancer
No neo-adj HTRT dose 60-78 Gy3DCRT planmingMedian FU 6.3 yrs
8-year PSA control rates were 72 to 93%. Dose >72 Gy had lower PSA relapse rate.
Zietman MDACCRandomized
N= 393T1-2 diseasePSA < 105ng/dl
Arm 1: Conv RT 70.2 GyArm 2: Conv RT 79.2 GyMedian FU: 5.5 yrs
5-yr PSA rFS higher with dose escalation (61% vs 80%). 49% risk reduction in biochemical failure.
Pollack et al MDACCRandomized
N=301Low risk prostate cancer
Arm 1 (n=150): Conv RT 70 GyArm 2 (151): 3DCRT 78 Gy
PSA rFS higher with dose escalation (70% versus 64%; p=0.03)
Peeters et al RandomizedNetherland
N=669T1-4
Arm 1 (n=150): Conv RT 68 GyArm 2 (151): Conv RT 78 GyMedian FU: 51 months
5-yr PSA relapse-free survival superior with high dose (64% vs. 54%; p = .02).
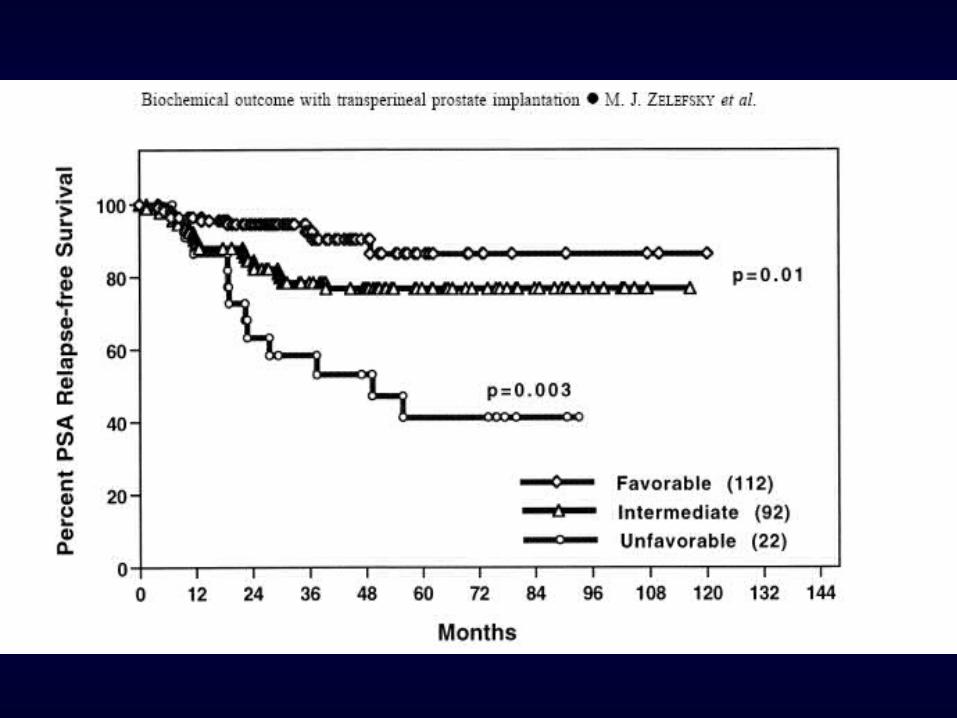
Zelefsky et al RandomizedMSKCC
N=11001988-98
RT dose systematically increased from 64.8 to 86.4 Gy by increments of 5.4 Gy in consecutive groups of pts.
5-yr PSA rFS was higher with dose escalation in favorable, intermediate and unfavourable groups.
Zelefsky et al Single arm N=5611996-2000
RT dose: 81 Gy to PTV 8-yr PSA rFS for favorable-, intermediate-, and unfavorable-risk groups were 85%, 76%, 72%
Prostate Cancer: Dose escalation studies

Intensity modulated radiation therapy
76- 81 Gy at 2 Gy/# dose delivered
Dose to target higher
Rectal & Bladder dose is high
High acute reactions
Dose escalation methodsIMRT/ 3DCRT

Toxicities after Radiation therapy
Rectal toxicity - Telengectasia - Bleeding - Bladder toxicity - Incontinence - Bleeding - Thimble bladder- Urethral stricture -Erectile dysfunction- Quality of life

Toxicity depends upon dose

Author Study Patient criteria Study details ResultsMartin Prospect
ivePMH
N= 92June 2001- Mar 2004
60 Gy /20 fr/ 4 wksIMRT, FU: 38 mo
3 yr PSA relapse free was 76%.RTOG Gr ≥3 GI toxicity in 1 patient
Kupelian Cleveland Clinic
N= 7701998-2005
70 Gy; 2.5-Gy/fr/ 5 wks.FU: 45 mo
5 yr PSA relapse free of low, intermediate and high-risk disease was 95%, 85%, and 68%, respectively.
Livsey RetrospectiveManchester
N= 705 men T1-T4 disease 1995 -1998
Conformal RT (50 Gy/16fr/ 22 days)Median FU: 48 months
Favourable, intermediate, poor prognostic groups biochemical control was 82%, 56%, and 39%. RTOG Gr ≥2 GI and bowel toxicity was 5% and 9%.
Lukka RandomizedNCI Canada
N= 936Mar 1995- Dec1998
Long arm: 66 Gy/33 fr 45 days Short arm: 52.5 Gy/20 fr 28 days
5 yrs, PSA relapse free survival was 52.95% in long and 59.95% in short arm.GI toxicity higher with short arm (11% vs 7%)
Tsuji Chiba Japan
N=201June 1995-Feb 2004
Three clinical trials RTOG Gr ≥2 GI toxicity. 5-yr PSA relapse-free survival 83.2% without any local recurrence.
Prostate Cancer: Hypofractionation studies
Author Study Patient criteria Study details Results
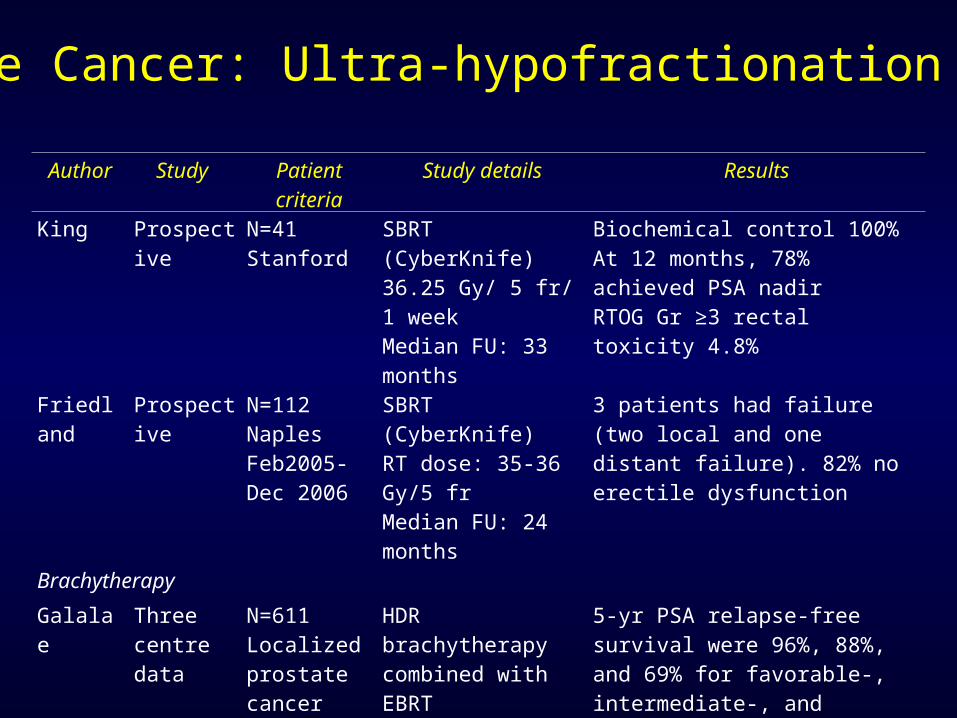
King Prospective N=41Stanford
SBRT (CyberKnife)36.25 Gy/ 5 fr/ 1 weekMedian FU: 33 months
Biochemical control 100%At 12 months, 78% achieved PSA nadirRTOG Gr ≥3 rectal toxicity 4.8%
Friedland Prospective N=112NaplesFeb2005-Dec 2006
SBRT (CyberKnife)RT dose: 35-36 Gy/5 frMedian FU: 24 months
3 patients had failure (two local and one distant failure). 82% no erectile dysfunction
Brachytherapy
Galalae Three centre data
N=611Localized prostate cancer
HDR brachytherapy combined with EBRT
5-yr PSA relapse-free survival were 96%, 88%, and 69% for favorable-, intermediate-, and unfavorable-risk patients
Prostate Cancer: Ultra-hypofractionation studies

Fullar et al, IJROBP 2008
Radiosurgery mimicking brachytherapy

Fullar et al, IJROBP 2008
Radiosurgery mimicking brachytherapy

Fullar et al, IJROBP 2008
Radiosurgery vs brachytherapy: Dosimetry

Radiosurgery vs brachytherapy: Dosimetry
Fullar et al, IJROBP 2008

Hossain et al, IJROBP 2010
SBRT vs IMRT : Dosimetry

Hossain et al, IJROBP 2010
SBRT vs IMRT : Dose distribution

Hossain et al, IJROBP 2010

Hossain et al, IJROBP 2010

Hossain et al, IJROBP 2010

SBRT: Early outcome of Ph II study (n=45)

SBRT: Early outcome of Ph II study (n=45)

SBRT: Clinical outcome (n=112)
Frieland et al, IJROBP 2009
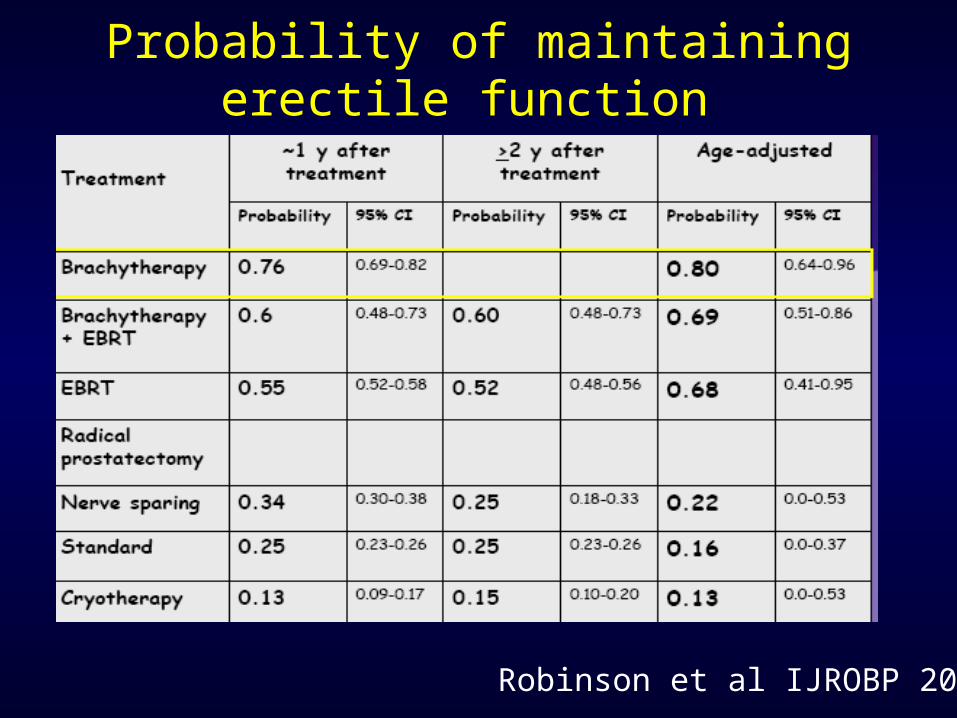
Probability of maintaining erectile function
Robinson et al IJROBP 2002

King et al. IJROBP 2010
QOL: Sexual function domains
5 yr FU data with biochemical control & QOL function
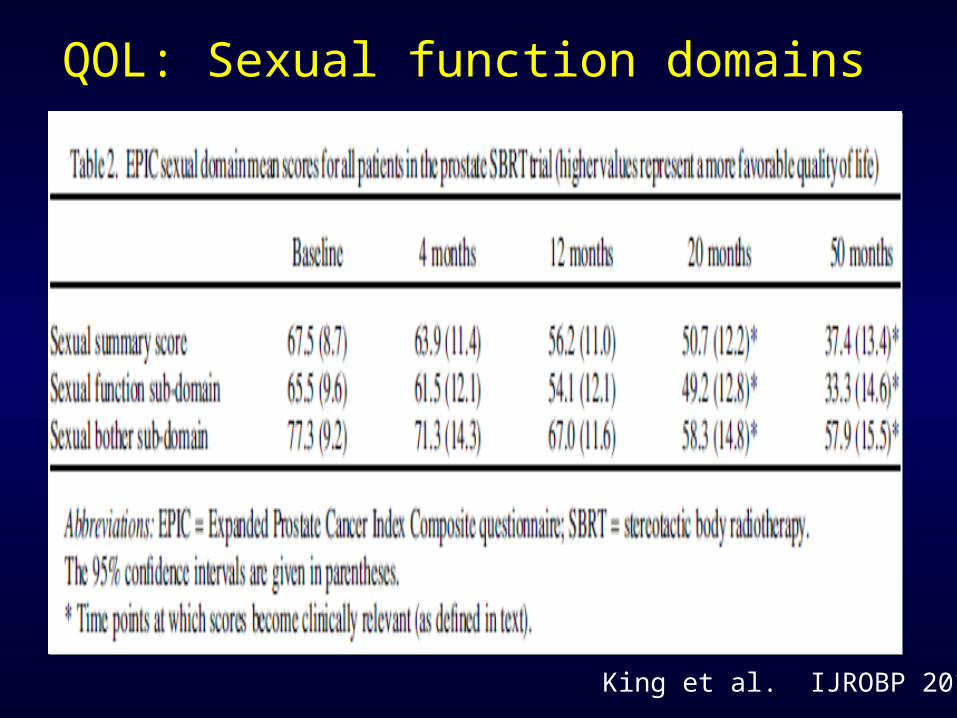
QOL: Sexual function domains
King et al. IJROBP 2010

Aluwin J of Endourology 2010
Experiences from new centres
Conclusions
- Large patient cohort prospective study with more than 500 patients and more than 5
years follow up have shown that CyberKnife is equally effective as long coures RT
- SBRT/ CyberKnife is now standard of care treatment for localized prostate cancer
- Outcome of CyberKnife treatment is similar to long course RT
- Side-effect after Cyberknife is less than 1% in prostate cancer
- CyberKnife is safe, out patient, short course treatment in both primary and metastatic
diseases.
- High dose radiation may be effective in many of the ‘radioresistant’ disease.

Thank you
Dr Debnarayan Dutta, MDCyberKnife Specialist





























