Embed Size (px)
Citation preview

Ye l lo x ® A p o w e r f u l t o o l f o r m a n a g in g p o s t -o p e r a t iv e in f la m m a t io n
Maart 2012

Contents
– Disease background: Prostaglandin (PG) production and their role in post-operative ocular inflammation
– Introducing Yellox® (bromfenac) − a new, unique and highly potent tool in managing PG-mediated post-operative inflammation
– Yellox® clinically proven efficacy and risk/benefit profile: Phase III efficacy data
– Yellox® safety and tolerability
– Summary

Mechanism of prostaglandin-mediated anterior chamber cell and flare, and CME
Post-surgical inflammatory complications produced by prostaglandins (PG)
PG
PG, prostaglandins; IOP, intraocular pressure.Adapted from Miyake K. J Cataract Refract Surg 1996; 22 Suppl 1:759-63.
PG
Vasodilation HyperaemiaMiosis
Cellular and protein flare in the anterior chamber
IOP
Rupture of the blood-aqueous barrier (BAB)
Accumulation of liquid in the macula forming large cystic
area = cystoid macular edema (CME)
Rupture of the blood-retinal barrier (BRB)
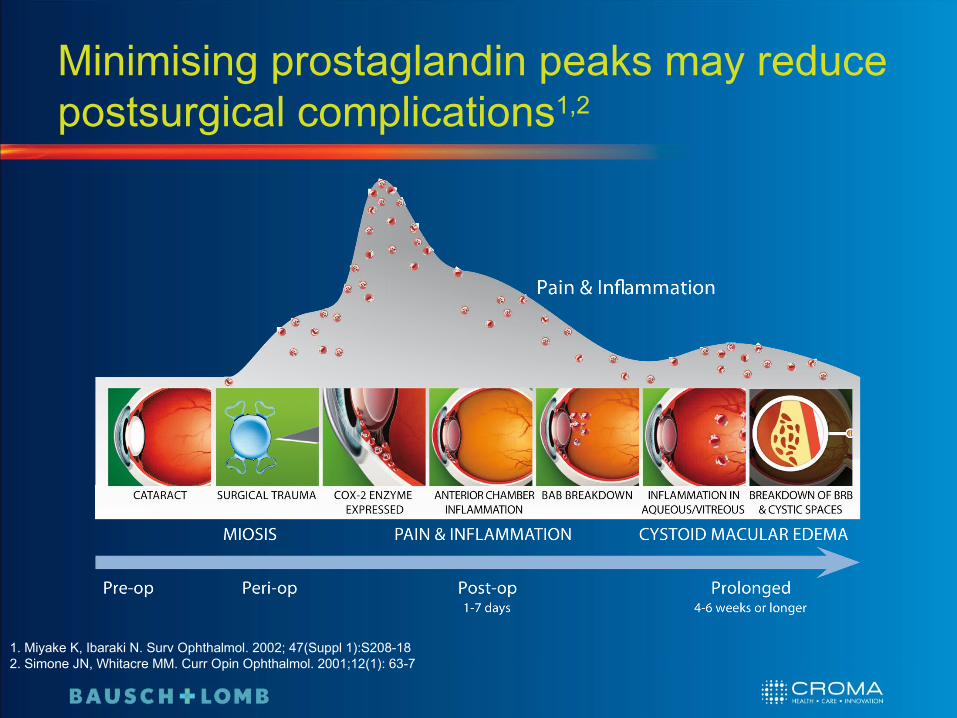
Minimising prostaglandin peaks may reduce postsurgical complications1,2
1. Miyake K, Ibaraki N. Surv Ophthalmol. 2002; 47(Suppl 1):S208-182. Simone JN, Whitacre MM. Curr Opin Ophthalmol. 2001;12(1): 63-7
Might induce cystoid macular edema
(CME)
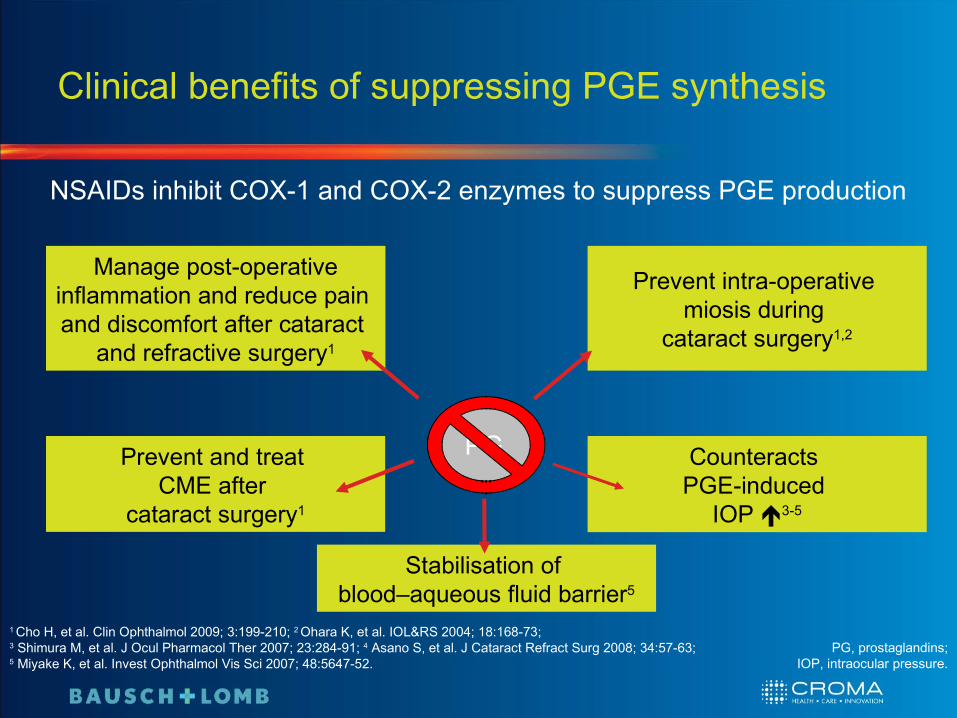
Clinical benefits of suppressing PGE synthesis
PG
Initiate and maintainocular inflammation
Produce miosis
Affect IOP
NSAIDs inhibit COX-1 and COX-2 enzymes to suppress PGE production
Increase permeability of blood-aqueous barrier
1 Cho H, et al. Clin Ophthalmol 2009; 3:199-210; 2 Ohara K, et al. IOL&RS 2004; 18:168-73; 3 Shimura M, et al. J Ocul Pharmacol Ther 2007; 23:284-91; 4 Asano S, et al. J Cataract Refract Surg 2008; 34:57-63; 5 Miyake K, et al. Invest Ophthalmol Vis Sci 2007; 48:5647-52.
PG, prostaglandins;IOP, intraocular pressure.
Manage post-operative inflammation and reduce pain and discomfort after cataract
and refractive surgery1
Prevent intra-operative miosis during
cataract surgery1,2
Counteracts PGE-induced
IOP 3-5
Stabilisation of blood–aqueous fluid barrier5
Prevent and treat CME after
cataract surgery1
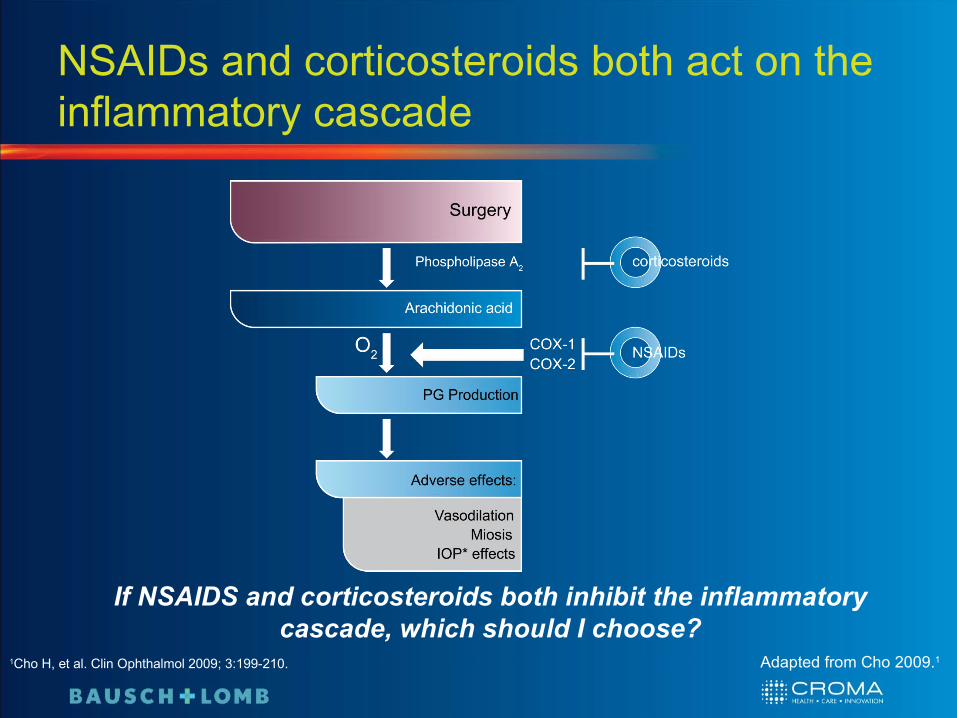
NSAIDs and corticosteroids both act on the inflammatory cascade
1Cho H, et al. Clin Ophthalmol 2009; 3:199-210.
If NSAIDS and corticosteroids both inhibit the inflammatory cascade, which should I choose?
Adapted from Cho 2009.1

Differences between NSAIDs and corticosteroids
Topical NSAIDs are notable for a definitive lack of corticosteroid-defined toxicity and have secured an important role in the treatment of ocular inflammatory disease2
1Cho H, et al. Clin Ophthalmol 2009;3:199-210 2Gaynes BI, Fiscella R. Drug Saf 2002;25:233-250 Adapted from Cho 2009.1
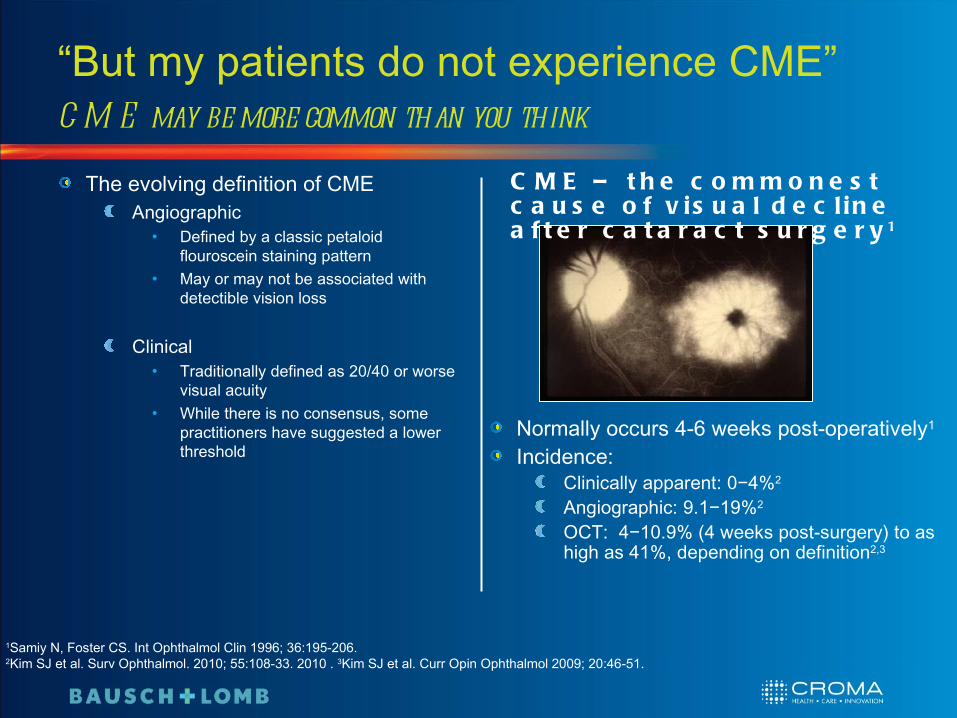
“But my patients do not experience CME”CM E may be more common than you think
The evolving definition of CMEAngiographic
• Defined by a classic petaloid flouroscein staining pattern
• May or may not be associated with detectible vision loss
Clinical• Traditionally defined as 20/40 or worse
visual acuity• While there is no consensus, some
practitioners have suggested a lower threshold
Normally occurs 4-6 weeks post-operatively1
Incidence:Clinically apparent: 0−4%2
Angiographic: 9.1−19%2
OCT: 4−10.9% (4 weeks post-surgery) to as high as 41%, depending on definition2,3
1Samiy N, Foster CS. Int Ophthalmol Clin 1996; 36:195-206. 2Kim SJ et al. Surv Ophthalmol. 2010; 55:108-33. 2010 . 3Kim SJ et al. Curr Opin Ophthalmol 2009; 20:46-51.
C M E – t h e c o m m o n e s t c a u s e o f v is u a l d e c l in e a f t e r c a t a r a c t s u r g e r y 1

The role of OCT in detecting occult CME
Optical coherence tomography (OCT) is sensitive to modest changes in retinal thickness, detecting increases as small as 10 μm 1
Increases >10 μm may correlate with poorer visual outcomes1
Increases of this size may escape routine clinical detection
1Wittpenn JR et al. Am J Ophthalmol 2008; 146: 554-560. 2Jamal KN, Goldenberg DT. Rev Ophthalmol. [http://www.revophth.com/index.asp?page=1_14257.htm]
Even mild macular thickening can result in a significant reduction in quality of vision and patient satisfaction2

In t r o d u c in g Ye l lo x ®
A new, unique and highly potent tool in managing PG-mediated post-operative
inflammation

Bromfenacbelongs to the chemical class of phenylacetic acids1
is the sodium salt (sesquihydrate) of [2-amino-3-(4-bromobenzoyl) phenyl] acetic acid
Bromfenac – a unique, brominated structure produces a highly potent NSAID
1Cho H, et al. Clin Ophthalmol 2009; 3:199-210; 2Baklayan GA, et al. J Ocul Pharmacol Ther 2008; 24:392-8; 3Ahuja M, et al. AAPS J 2008 10:229-41.
O NH2
OH
OBr
• The introduction of bromine into the NSAID structure:• Enhances lipophilicity of the molecule leading to improved ocular
penetration2
• Increases duration of analgesic and anti-inflammatory activity1,3
• May enhance inhibitory effect on COX-2 thus contributing to the molecule’s potency1,3
Cyclooxygenase: The importance of COX-2 inhibition
Activation of cyclooxygenase isoenzymes (COX-1 and -2) produce inflammation mediators1,2
Isoforms have very similar molecular structures but different actions and sites of action
COX-1 • Expressed constitutively in almost all tissues• Action on physiological regulations: coagulation (thromboxanes), gastric secretion,
etc.
COX-2 • Expressed in response to inflammation, injury and pain • Action on damaged tissues (production of prostaglandins)
COX-2 is thought to be the primary mediator of ocular inflammation through prostaglandin production3
1 Donnenfeld ED, Donnenfeld A. Int Ophthalmol Clin 2006; 46:21-40; 2 Polansky JR, Weinreb RN. In: Pharmacology of the Eye. 1984:460–538; 3Oka T et al. Curr Eye Res. 2004; 29(1)27-34
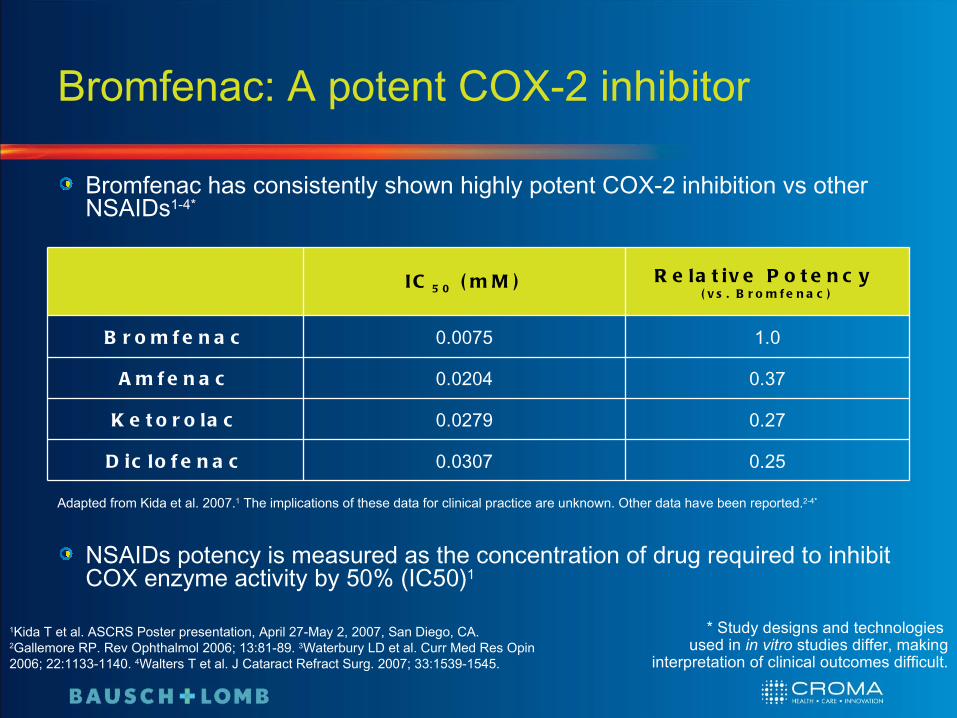
Bromfenac: A potent COX-2 inhibitor
Bromfenac has consistently shown highly potent COX-2 inhibition vs other NSAIDs1-4*
NSAIDs potency is measured as the concentration of drug required to inhibit COX enzyme activity by 50% (IC50)1
IC 5 0 ( m M ) R e la t iv e P o t e n c y ( v s . B r o m f e n a c )
B r o m f e n a c 0.0075 1.0
A m f e n a c 0.0204 0.37
K e t o r o la c 0.0279 0.27
D ic lo f e n a c 0.0307 0.25
Adapted from Kida et al. 2007.1 The implications of these data for clinical practice are unknown. Other data have been reported.2-4*
1Kida T et al. ASCRS Poster presentation, April 27-May 2, 2007, San Diego, CA. 2Gallemore RP. Rev Ophthalmol 2006; 13:81-89. 3Waterbury LD et al. Curr Med Res Opin 2006; 22:1133-1140. 4Walters T et al. J Cataract Refract Surg. 2007; 33:1539-1545.
* Study designs and technologies used in in vitro studies differ, making
interpretation of clinical outcomes difficult.

Bromfenac: Rapid and sustained penetrationBromination increases lipophilicity
Unique bromination of amfenac can increase lipophilicity, resulting in enhanced penetration of bromfenac through the cornea and ocular tissues below
0 6 12 18 24Time (h)
0.001
0.01
0.1
1
10
Co
nce
ntr
atio
n (
ug
eq
ulv
./g
)
14C-Bromfenac
Baklayan GA, et al. J Ocul Pharmacol Ther 2008; 24:392-8.
Aqueous humourCornea Iris-ciliary body RetinaChoroid
Retina notdetectable at 6
hours
0 6 12 18 24
1E-3
0.01
0.1
1
10
Time (h)
Con
cent
ratio
n (μ
g eq
ulv.
/g)
14C-Nepafenac
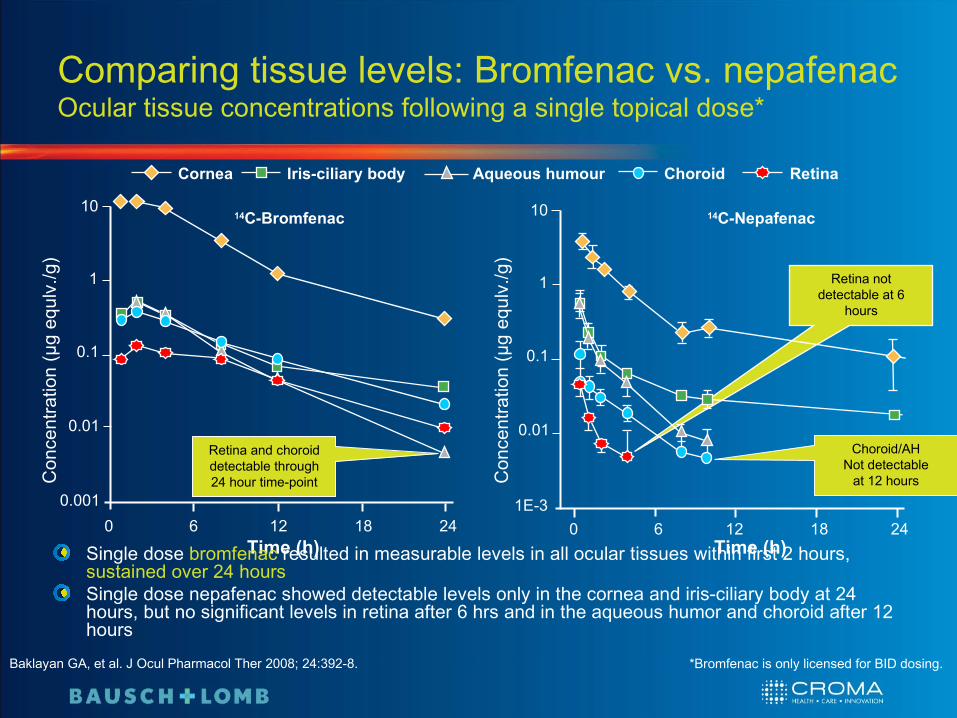
Comparing tissue levels: Bromfenac vs. nepafenacOcular tissue concentrations following a single topical dose*
0 6 12 18 24Time (h)
0.001
0.01
0.1
1
10
Con
cent
ratio
n (μ
g eq
ulv.
/g)
14C-Bromfenac
Baklayan GA, et al. J Ocul Pharmacol Ther 2008; 24:392-8. *Bromfenac is only licensed for BID dosing.
Aqueous humourCornea Iris-ciliary body RetinaChoroid
Retina and choroiddetectable through24 hour time-point
Choroid/AHNot detectable
at 12 hours
Single dose bromfenac resulted in measurable levels in all ocular tissues within first 2 hours, sustained over 24 hoursSingle dose nepafenac showed detectable levels only in the cornea and iris-ciliary body at 24 hours, but no significant levels in retina after 6 hrs and in the aqueous humor and choroid after 12 hours

Phase III trial program design
S t u d y N o .
D e s ig n a n d t r e a t m e n t r e g im e n D o s e B r o m f e
n a c
N
Donnenfeld et al, 2007
Two US phase III trials conducted to assess efficacy and safety of bromfenac in patients undergoing cataract surgery. Primary endpoint was the assessment of efficacy according to the Cell and Flare Score of 0 at Day 15.Secondary endpoint was the time to the resolution of ocular pain
0.1% b.i.d 527
Donnenfeld ED, et al. Ophthalmology 2007; 114:1653-62; Data on file

Yellox® vs placebo after cataract surgery Two phase III, multicenter, randomised, double-masked, parallel group studies
Data were pooled from two trials that had a common protocol
Endpoints:Primary: Cell and flare score (SOIS) = 0 at day 15Secondary: Time to resolution of ocular pain (days from baseline to time when pain was first scored “none” in diary)Safety
Scheduled study visits (for assessment of SOIS):days 1 (16-32 h after surgery), 3, 8, 15 (end of therapy), 22, 29 and at early discontinuation of test agent or upon early withdrawal from the study
Patients (age ≥ 18y)undergoing cataract surgery* with no pre-treatment (n=527)
R
One drop Bromfenac 0.09% BID (n=356)†‡
Placebo BID (n=171)†‡
continuing for 14 days
*Post-surgical Summed Ocular Inflammation Score (SOIS) ≥ 3
2:1
SA
FE
TY
EV
AL
UA
TIO
N
†Starting treatment 16-32 h after surgery; ‡ITT population.
Donnenfeld ED, et al. Ophthalmology 2007; 114:1653-62. ITT, Intention-to-treat; b.i.d., twice daily.
continuing for up to 14 days

Yellox®: Rapid results
8.4% of patients had clearance of ocular inflammation by day 3.
0
20
40
60
80
100
Day 3 Day 8 Day 15 Day 22 Day 22
Pa
tie
nts
wit
h S
OIS
0 (
%)
Placebo Bromfenac
*
* *
*
# p=0.0012, * p<0.0001 vs placebo
#
† Patients receiving Bromfenac or placebo alone‡ LOCF, last observation carried forward;
SOIS, summed ocular inflammation score.
Proportion of patients with SOIS 0 at each study visit†
N.B. Treatment duration was 14 days onlyAdapted from Donnenfeld ED, et al. Ophthalmology 2007; 114:1653-62.
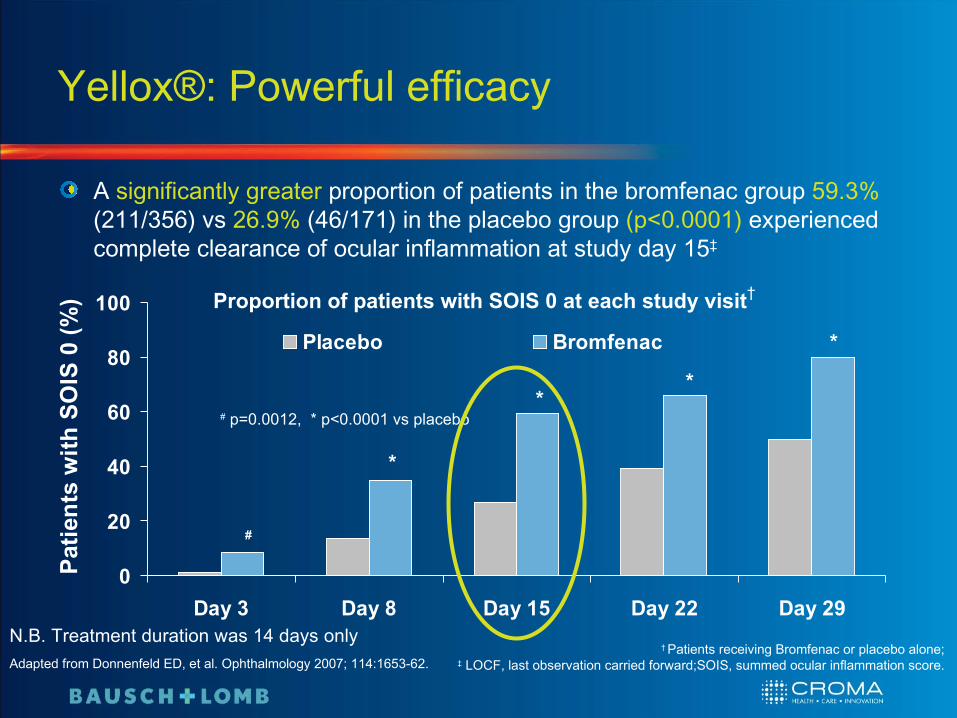
Yellox®: Powerful efficacy
A significantly greater proportion of patients in the bromfenac group 59.3% (211/356) vs 26.9% (46/171) in the placebo group (p<0.0001) experienced complete clearance of ocular inflammation at study day 15‡
Adapted from Donnenfeld ED, et al. Ophthalmology 2007; 114:1653-62.† Patients receiving Bromfenac or placebo alone;
‡ LOCF, last observation carried forward;SOIS, summed ocular inflammation score.
N.B. Treatment duration was 14 days only
*
* *
*
# p=0.0012, * p<0.0001 vs placebo
#
Proportion of patients with SOIS 0 at each study visit†
0
20
40
60
80
100
Day 3 Day 8 Day 15 Day 22 Day 29
Pat
ien
ts w
ith
SO
IS 0
(%
)
Placebo Bromfenac

Fewer adverse events in Yellox®-treated patients than placebo groupOccurrence of adverse events was lower for the bromfenac group than for the placebo group (33.7% vs 47.4%; p=0.0027)1,2
Adverse event*, %
Treatment groups
Yellox® (n=356) Placebo (n=171)Iritis 7.0 18.1
Abnormal sensation in eye 6.5 8.2
Eye pain 4.2 11.7
Eye pruritus 3.9 2.9
Posterior capsular opacification 3.9 4.1
Eye irritation (burning/stinging) 2.5 4.7
Eye redness 2.2 7.6
Conjunctival hyperaemia 2.2 11.1
Photophobia 2.0 11.1
Macular oedema 1.4 4.7
Adapted from Donnenfeld et al. 20071 and Donnenfeld et al. 2006.2
* MedDRA Preferred Term.1Donnenfeld ED, et al. Ophthalmology 2007; 114:1653-1662; 2Donnenfeld ED, Donnenfeld A. Int Ophthalmol Clin 2006; 46:21-40.

Patient comfort and compliance
A US survey (n = 589) demonstrated ophthalmologists’ satisfaction or their judgment of patient satisfaction in a number of key areasYellox® has two key benefits that may enhance patient compliance
Convenience of bid dosing frequency
42 39 38 2919
53
58 61 62 7081
46
100%
50%
0% Overall patient
satisfaction
Safety Comfort upon
instillation
Patient comp-liance
Ease of use by
patients
Control of inflam-mation
ISTA Pharmaceuticals, Inc. Data on file; Adapted from Donnenfeld ED, Donnenfeld A. Int Ophthalmol Clin 2006; 46:21-40.
Expectations exceeded
Met all expectations
Comfort and high tolerability

Proven in the clinic with extensive global ophthalmic usage
Over 9 years experience with more than 20 million patients treated with Bromfenac1,2
Japan as Bronuck® since 2000 for the treatment of:3
• Blepharitis• Conjunctivitis• Scleritis• Post-operative inflammation
US as Xibrom® since 2005 for the treatment of:4
• Post-operative inflammation• Reduction of ocular pain after cataract extraction
1Committee for Medicinal Products for Human Use (CHMP) Assessment Report, 17 March 2011. 2Bromfenac SPC. 3Bronuck® package insert. Senju Pharmaceutical Co,. Ltd., Osaka, Japan, 2003; 4Xibrom® package insert. ISTA Pharmaceuticals, Inc., Irvine, CA; 2006.

Very low incidence of corneal complications
More than 20 million patients worldwide over 9 years have now been treated with bromfenac.1 To date, there have been four reports of serious corneal damage2,3
It is important to note that in each of these four cases the cornea being treated had a pre-existing cause for compromise, or were associated with off-label use or polypharmacy3
Case 1: a 20-year-old woman with Stevens–Johnson syndrome had diffuse punctuate epithelial erosionsCase 2: a 58-year-old man with Fuch’s endothelial dystrophy had episcleritisCase 3: a patient treated with topical bromfenac for 40 days developed a 60% corneal melt in an area previously associated with a dellen (shallow excavation along the outer edge of the cornea)Case 4: A patient with a culture-proven bacterial ulcer was treated with bromfenac four times daily for 3 weeks
Corneal complications are not unique to bromfenac, and are inherent to the NSAID class2,3
1Committee for Medicinal Products for Human Use (CHMP) Assessment Report, 17 March 2011. 2Cho H et al. Clin Ophthalmol 2009; 3:199-210. 3Jones J, Francis P. Expert Opin Pharmacother 2009; 10(14):2379-2385.

No systemic events with Yellox®
No detectable plasma concentration was found at any time point (HPLC detection limit: 50 ng/ml) after ocular instillation of 1 dose of bromfenac1
Overall, low occurrence of systemic AEs were reported by bromfenac- and placebo-treated patients (10.7% and 10.5%; p=0.977)2
Upper respiratory tract infections (2.5% bromfenac and 0.6% placebo)Headache (2.0% bromfenac and 1.8% placebo)
Incidence of systemic AEs was comparable across both groups2
No treatment-related SAEs were reported in the bromfenac and placebo groups2
No clinically significant changes in liver chemistry were observed in either group2
1Data on file Senju G-01; 2Stewart RH, et al. J Ocul Pharmacol Ther 2007; 23:601-12. AE; adverse events,SAE; serious adverse events.

Yellox®: A potent tool in managing post-operative inflammation
Post-operative prostaglandin production leads to important inflammatory complications1
Yellox® has important benefits in the management of ocular inflammation:Potently inhibition of COX-2, a key enzyme in producing prostaglandin-mediated complications2,3
Rapid and sustained penetration of ocular tissues4,5
Potency and penetration that allow twice daily dosing5,6
Unique twice daily dosing and comfortable solution, which may enhance patient compliance4,6
Bromfenac’s efficacy and safety have been demonstrated in:Two large, multicenter phase III trials7
Extensive global experience8-10
1Miyake K. J Cataract Refract Surg 1996; 22 Suppl 1:759-63. 2Kida T et al. ASCRS Poster presentation, April 27-May 2, 2007, San Diego, CA. 3Oka T et al. Curr Eye Res. 2004; 29:27-34. 4Donnenfeld ED, Donnenfeld A. Int Ophthalmol Clin 2006; 46:21-40. 5Baklayan GA et al. J Ocul Pharmacol Ther 2008; 24:392-398. 6Yellox SPC. 7Donnenfeld ED et al. Ophthalmology 2007; 114:1653-1662. 8Committee for Medicinal Products for Human Use (CHMP) Assessment Report, 17 March 2011. 9Cho H et al. Clin Ophthalmol 2009; 3:199-210. 10Jones J, Francis P. Expert Opin Pharmacother 2009; 10:2379-2385.





























