Embed Size (px)
Citation preview
(50 marks seminar) Presented by:
S.S.D.SreejaM.Pharmacy I/II
Pharmacology
Under the guidance of:
Dr. R. PadmavathiAssoc. Professor
M.Pharm, PhD.

• INTRODUCTION
• PHARMACOKINETICS AND DRUG THERAPY IN GERIATRICS
• PHARMACOKINETICS AND DRUG THERAPY IN PEDIATRICS
• PHARMACOKINETICS AND DRUG THERAPY IN PREGNANCY AND LACTATION
Pharmacokinetics deals with the description of concentration changes of drugs in the body as a function of time. It is best defined as what the body does to the drug.
it includes:
Absorption
Distribution across body compartments
Metabolism
Excretion

Pharmacokinetic Parameter Age related changes
Absorption Nil
Distribution ofLipid soluble drugsWater soluble drugsAcidic drugsBasic drugs
IncreasedDecreasedIncreasedDecreased
Metabolism Phase IPhase II
DecreasedNil
Excretion Decreased

System Age related Physiological changes Consequences
General Increased body fatDecreased total body water
Vd of lipid soluble drugs is increased requiring higher dose; eg. Diazepam.Vd of water soluble drugs is decreased requiring low dose; eg. Digoxin.
Gastrointestinal tract
Decreased gastric acidityDecreased gastrointestinal motilityDecreased hepatic blood flow
Absorption of basic drugs is enhanced; eg. Propranolol.Absorption of acidic drugs is decreased; eg. Barbiturates.Decreased metabolism of drugs.
Renal Decreased renal blood flow, GFR and tubular secretion
Renal clearance is decreased and hence drugs excreted through kidney should be used cautiously. Eg. Digoxin, aminoglycosides.
Musculoskeletal Decreased muscle massDecreased bone density
Resulting in functional impairment and fracture requiring treatment and hospitalization, etc.
Cardiovascular system
Increased blood pressure Cardiovascular complications requiring treatment, hospitalization, etc.
Central nervous system
Brain atrophyDecreased dopaminergic synthesisDecreased sleep (stage 4)
Results in forgetfulness, depression, Parkinson’s, insomnia etc. requiring therapy.
Genitourinary Vaginal/ urethral mucosal atrophyProstate enlargement
Bacteriuria, increased residual urine volume requiring hormonal or drug therapy.
Endocrine Decreased basal metabolic rateVulnerable to stressGlucose intolerance
Resulting in diabetes mellitus which needs life long treatment.

Class or Category Decreased Hepatic Metabolism Decreased Renal Elimination
Analgesics and anti-
inflammatory drugs
Ibuprofen
Meperidine
Morphine
Naproxen
Meperidine
Morphine
Providing safe, effective drug therapy for the elderly is challenging for many reasons:
They use more drugs than any other age group, increasing risk of adverse effects and drug interactions, and making adherence more difficult.
They are more likely to have chronic disorders that may be worsened by the drug or affect drug response.
Their physiologic reserves are generally reduced and can be further reduced by acute and chronic disorders.
Aging can alter pharmacodynamics and pharmacokinetics
They may be less able to obtain or afford drugs.
There are 2 main approaches to optimizing drug therapy in the elderly:
Using appropriate drugs as indicated to maximize cost-effectiveness
Avoiding adverse drug effects

Category Definition
Drug interactions Use of a drug results in a drug-drug, drug-food, drug-supplement, or drug-
disease interaction, leading to adverse effects or decreased efficacy.
Inadequate monitoring A medical problem is being treated with the correct drug, but the patient is
not adequately monitored for complications, effectiveness, or both.
Inappropriate drug selection A medical problem that requires drug therapy is being treated with a less-
than-optimal drug.
Inappropriate treatment A patient is taking a drug for no medically valid reason.
Lack of patient adherence The correct drug for a medical problem is prescribed, but the patient is not
taking it.
Overdosage A medical problem is being treated with too much of the correct drug.
Poor communication Drugs are inappropriately continued or stopped when care is transitioned
between providers and/or facilities.
Underprescribing A medical problem is being treated with too little of the correct drug.
Untreated medical problem A medical problem requires drug therapy, but no drug is being used to
treat that problem.
Some drug categories (eg, analgesics, anticoagulants, anti hypertensives, antiparkinsonian drugs, diuretics, hypoglycemic drugs, psychoactive drugs) pose special risks for elderly patients. Some drugs, although reasonable for use in younger adults, are so risky they should be considered inappropriate for the elderly.
The Beers Criteria are most commonly used to identify such inappropriate drugs. The 2012 American Geriatrics Society updates to the Beers criteria further categorize potentially inappropriate drugs into 3 groups:
Inappropriate: Always to be avoided
Potentially inappropriate: To be avoided in certain diseases or syndromes
To be used with caution: Benefit may offset risk in some patients
Anticholinergics:
First-generation antihistamines, as single agents or in combination products (brompheniramine, carbinoxamine, chlorpheniramine, clemastine, cyproheptadine, dexbrompheniramine, dexchlorpheniramine, diphenhydramine [oral], doxylamine, hydroxyzine, promethazine, triprolidine)
Antiparkinson drugs (benztropine [oral],trihexyphenidyl)
Antispasmodics (belladonna alkaloids, clidinium-chlordiazepoxide, dicyclomine, hyoscyamine, propantheline

Anti-infectives: Nitrofurantoin
Antithrombotics: Dipyridamole, Ticlopidine
Cardiovascular drugs: Alpha-1 blockers (doxazosin, prazosin,terazosin) Alpha agonists, central (clonidine,
guanabenz, guanfacine, methyldopa, reserpine Antiarrhythmic drugs, classes Ia, Ic, and III
(amiodarone, dofetilide, dronedarone,flecainide, ibutilide, procainamide,propafenone, quinidine, sotalol)
Disopyramide†
Dronedarone Digoxin (> 0.125 mg/day) Nifedipine Spironolactone (> 25 mg/day)
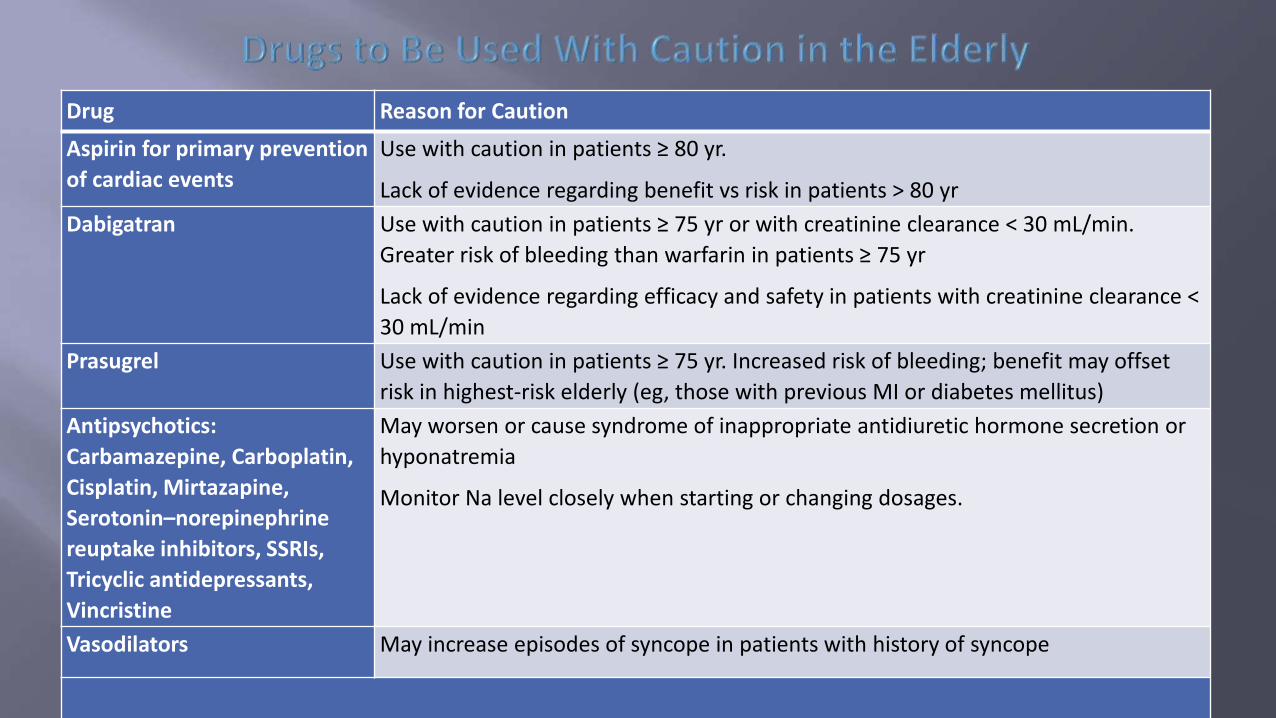
Drug Reason for Caution
Aspirin for primary prevention
of cardiac events
Use with caution in patients ≥ 80 yr.
Lack of evidence regarding benefit vs risk in patients > 80 yr
Dabigatran Use with caution in patients ≥ 75 yr or with creatinine clearance < 30 mL/min.
Greater risk of bleeding than warfarin in patients ≥ 75 yr
Lack of evidence regarding efficacy and safety in patients with creatinine clearance <
30 mL/min
Prasugrel Use with caution in patients ≥ 75 yr. Increased risk of bleeding; benefit may offset
risk in highest-risk elderly (eg, those with previous MI or diabetes mellitus)
Antipsychotics:
Carbamazepine, Carboplatin,
Cisplatin, Mirtazapine,
Serotonin–norepinephrine
reuptake inhibitors, SSRIs,
Tricyclic antidepressants,
Vincristine
May worsen or cause syndrome of inappropriate antidiuretic hormone secretion or
hyponatremia
Monitor Na level closely when starting or changing dosages.
Vasodilators May increase episodes of syncope in patients with history of syncope

Absorption: Absorption from the GI tract is affected by:
Gastric acid secretion: Reduced gastric acid secretion increases bioavailability of acid-labile drug and decreases bioavailability of weakly acidic drugs.
Bile salt formation: Reduced bile salt formation decreases bioavailability of lipophilic drugs (eg, diazepam).
Gastric emptying time and Intestinal motility: Reduced gastric emptying and intestinal motility increase the time it takes to reach therapeutic concentrations when enteral drugs are given to infants < 3 mo
Bowel length and effective absorptive surface: Infants with congenital atretic bowel or surgically removed bowel or who have jejunal feeding tubes may have specific absorptive defects depending on the length of bowel lost or bypassed and the location of the lost segment
Drug-metabolizing enzymes present in the intestines of young infants are another cause of reduced drug absorption.

• Injected drugs are often erratically absorbed because of: Variability in their chemical characteristics, Differences in absorption by site of injection (IM or sc), Variability in muscle mass among children, illness and Variability in depth of injection (too deep or too shallow)
• IM injections are generally avoided in children because of pain and the possibility of tissue damage, but, when needed, water-soluble drugs are best because they do not precipitate at the injection site.
• Transdermal absorption may be enhanced in neonates and young infants because the stratum corneum is thin and because the ratio of surface area to weight is much greater than for older children and adults. Skin disruptions (eg, abrasions, eczema, burns) increase absorption in children of any age.
• Transrectal drug therapy is generally appropriate only for emergencies when an IV route is not available
• Absorption of drugs from the lungs varies less by physiologic parameters and more by reliability of the delivery device and patient or caregiver technique.

The volume of distribution of drugs changes in children with aging. These age-related changes are due to changes in body composition (especially the extracellular and total body water spaces) and plasma protein binding.
Higher doses (per kg of body weight) of water-soluble drugs are required in younger children because a higher percentage of their body weight is water Conversely, lower doses are required to avoid toxicity as children grow older because of the decline in water as a percentage of body weight.
Drug metabolism and elimination vary with age and depend on the substrate or drug, but most drugs, and most notably phenytoin, barbiturates, analgesics, and cardiac glycosides, have plasma half-lives 2 to 3 times longer in neonates than in adults.
Phase I activity is reduced in neonates, increases progressively during the first 6 months of life, exceeds adult rates by the first few years for some drugs, slows during adolescence, and usually attains adult rates by late puberty. Phase II metabolism varies considerably by substrate

Drug metabolites are eliminated primarily through bile or the kidneys. Renal elimination depends on
Plasma protein binding
Renal blood flow
GFR
Tubular secretion
All of these factors are altered in the first 2 yr of life. Renal plasma flow is low at birth (12 mL/min) and reaches adult levels of 140 mL/min by age 1 yr. Similarly, GFR is 2 to 4 mL/min at birth, increases to 8 to 20 mL/min by 2 to 3 days, and reaches adult levels of 120 mL/min by 3 to 5 mo.

Drug treatment in children differs from that in adults, most obviously because it is usually based on weight or surface area. Doses (and dosing intervals) differ because of age-related variations in drug absorption, distribution, metabolism, and elimination. A child cannot safely receive an adult drug dose, nor can it be assumed that a child’s dose is proportional to an adult’s dose (ie, that a 7-kg child requires 1/10 the dose of a 70-kg adult).
Children are generally subject to the same adverse effects as adults but they have increased risk with certain drugs because of differences in pharmacokinetics or because of drug effects on growth and development

Drug Clinical Syndrome Mechanism Comments
Anesthetics, topical
(eg, benzocaine, mixture
oflidocaine and prilocaine)
Cyanosis Formation of methemoglobin (ferrous iron
oxidized to ferric iron)
Incidence rare
Ceftriaxone Jaundice
Kernicterus
Bilirubin displaced from albumin Affects only neonates
Codeine Respiratory depression
Death
Ultrarapid metabolization
of codeine tomorphine
Genetic variant
Deaths have occurred after surgery and in a
breastfed infant whose mother tookcodeine
Diphenoxylate Respiratory depression
Death
CNS depression (in immature CNS) Overdose syndrome, usually in children < 2 yr
Fluoroquinolones Cartilage toxicity Unknown Suspected based on animal studies, but adverse
effects in humans unproved—short-term use
may be safe
Lindane (topical) Seizures
CNS toxicity
Probably enhanced absorption in children Should not be used in children < 50 kg
(alternative should be used)
Prochlorperazine Altered CNS function
Extrapyramidal effects
Opisthotonus
Bulging fontanelles
Actions via multiple CNS receptors Febrile and dehydrated infants especially at risk
SSRIs Suicidal ideation Unknown Increased incidence of suicidal ideation in
children and adolescents
Tetracycline Discoloration and pitting of
tooth enamel
Chelation with Ca in growing teeth Not given to children < 8 yr

In pregnancy and labour the body becomes a complex physiological unit which consists of mother, placenta and fetus.
This unit is complicated not only because of integrated parts of the system are interrelated but also because considerable changes occur as pregnancy advances.
These changes may lead to important variations in the pharmacokinetic processes of absorption, distribution and elimination of drugs
Alterations in pharmacokinetic parameters in pregnancyAbsorption GI absorption: reduced intestinal motility; increased gastric and
intestinal emptying time; reduction in gastric acid secretion; increased mucus secretion; total perfusion is increased
Pulmonary absorption: haemodynamic and ventilatory factors
Hyperventilation: increased alveolar drug uptake
Intramuscular absorption: increased peripheral tissue perfusion due to vasodilation. In late pregnancy blood flow is decreased to lower limbs

Drug distribution
increased blood volume and cardiac output
Drug elimination
Renal Drug elimination – creatinine clearance and drug elimination.
Hepatic Drug elimination - increased rate of metabolism
decreased rate of metabolism - ethylmorphine

It is an index of the fetus to the drug taken by the mother.
It is the ratio of the total area under the drug concentration time curve for the fetus to that of the mother-from the time of drug administration to the mother to the time when all drug has been eliminated
Drugs that are intended to reach the fetus should have a high index of relative exposure, while that should preferably not reach the fetus but are intended for the mother then it should have a low index of relative exposure to the fetus.

category A- careful tests in humans have shown no harm.
Category B- animal studies have shown an adverse effect, but adequate and well controlled studies in pregnant women have failed to demonstrate any risk to the fetus.
Category C- animal studies show some harm and there are no good studies in humans.
Category D- adequate well controlled studies in pregnant women have demonstrated a risk to the fetus.
Category X- adequate well controlled studies in animals or in pregnant women have shown that the drug causes fetal abnormalities.

Stage Gestation period Main cellularprocess
Altered by:
Blastocyst formation
0 – 16 days Cell division Cytotoxic drugs
Organogenesis 17 – 60 days DivisionMigrationDifferentiation
Teratogens
Histogenesis, functional maturation
60 days to term (same as above) MiscellaneousAlcholnicotine

• A substance, organism, physical agents or deficiency state capable of inducing abnormal structure or function such as: – Gross structural abnormalities
– Functional deficiencies
– Intrauterine growth restriction
– Behavioral aberrations
– Demise

• Timing of exposure
• Developmental stage during exposure
• Maternal dose and duration
• Maternal pharmacokinetics
• Genetic factors/phenotypes
• Interactions between agents

• Placental transfer may occur by:
– Passive diffusion
– Facilitated diffusion
– Active transport
• Placental surface area
• Placental metabolism

• Diffusion from maternal plasma into
milk
• Higher maternal plasma levels mean
higher breast milk concentrations
• Equilibrium will be established with
most drugs between milk and plasma


ANTIEPILEPTICS: Uncontrolled epilepsy in a pregnant woman is a serious and potentially life threatening condition for both mother and child. But they have adverse effects such as:• Fetal abnormalities• CHF,• Neural tube defects,• Neuro genital defects.
CARBAMAZEPINE
Structural birth defects.
Compatible with breastfeeding
VALPROATE
Should be avoided in reproductive women.
Major malformations including spina bifida.
Compatible with breastfeeding.
LAMOTRIGINE
Plasma concentrations of lamotrigine fall early in pregnancy,so dose increases may be necessary to control seizures
At the post partum lamotrigine concentration rises with in a few days and dose reduction may be required to prevent toxicity.
Excreted in considerable amounts into breast milk.

PHENYTOIN
Less frequently used because of increased malformations.
Increased clearance, decreased plasma concentrations lead to loss of seizure control.
Post partum monitoring of plasma concentrations helps in preventing phenytoin toxicity.
CLONAZEPAM
No particular pregnancy risks.
Causes drowsiness in breast feeded neonate.
Withdrawal effects
PHENOBARBITONE
Marked increase in plasma clearance.
Neonatal drowsiness and apathy.

ANTIDEPRESSANTS
Harmful effects:
In pregnancy –Shorter gestational length and lower birth weight in new born.
Raised cortisol levels with the increased vulnerability to psychopathology
In lactation-women who develop post natal depression are most likely to stop breastfeeding.

SSRIs during pregnancy: First trimester-no teratogenic effects.
Paroxetine - Cardiovascular abnormalities. Second trimester-significant risk of shorter gestational length and
lower birth weight in infants. Third trimester-increased respiratory distress,irritability and feeding
problems. Persistent pulmonary hypertension in new born and possibly
intraventricular haemorrhage.
SSRIs during lactation:
Compatible with breastfeeding.
Highly protein bound so less drug is transferred from mother to the infant during lactation.


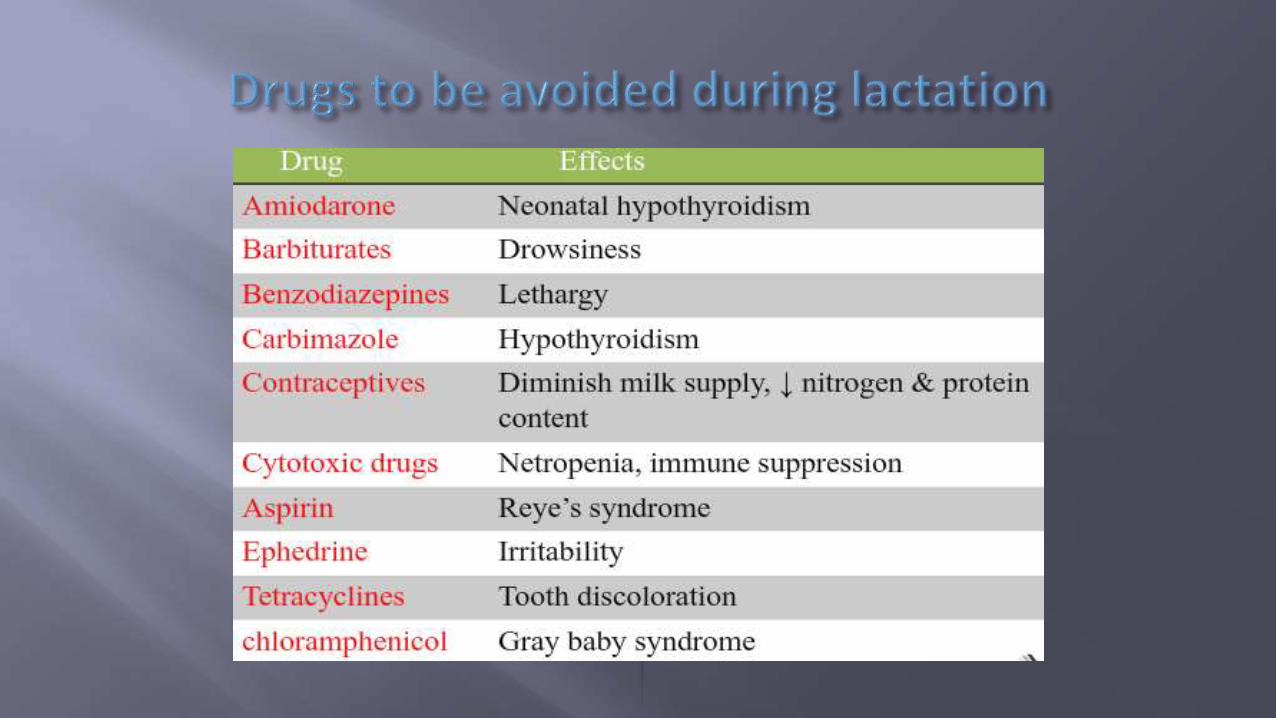

Anticancer drugs
Radio pharmaceuticals
Ergot & its derivatives
Lithium
Chloramphenicol
Phenyl butazone
Atropine
Thiouracil
Iodide
Mercurials
sulphonamides

Drugs which inhibit/suppress lactation:
• Bromocriptine
• Bendroflumethazide
• Estradiol
• Oral contraceptives
• Levodopa
• Trazodone
Drugs which are hazardous to the infant:
Large doses of Alcohol, caffeine, theophylline.
Hand book of clinical pharmacokinetics Milo Gibaldi and Prescott
Applied biopharmaceutics and pharmacokinetics ;Leon shargel,Susanna wu-pong,AndrewB.C.YU
Clinical pharmacokinetics ; Rowland and Tozer
Clinical pharmacology and pharmacotherapeutics; Roser walker
Pharmacological basis of therapeutics; Goodmann and Gilmann
www.spingerlink.com
www.wikipedia.org
www.pubmed.gov
www.pharmainfo.net
Last full review/revision June 2014 by J. Mark Ruscin, PharmD; Sunny A. Linnebur, PharmD, FCCP, BCPS, CGP

THANKYOU